Embed Size (px)
Citation preview
Responding to ACES at Monroe High School
Joe NeigelOctober 21, 2015
Our Goals This Morning
Review the Adverse Childhood Experiences Study and how early life trauma influences behavior, health outcomes and readiness to learn.
Discover how ACE impact students and educators at Monroe High School.
Consider simple, evidence-based strategies educators and counselors can adopt to mitigate the harm ACE cause to students and the learning environment.
Adverse Childhood Experiences Study (ACES)
ACES began as a weight-loss study at Kaiser-Permanente inSouthern California. It became the largest study evercompleted that examined the health and social effects oftraumatic childhood experiences over the lifespan.
Middle class, average age of 57
80% white, 10% black, 10% Asian
74% some college
44% graduated college
49.5% men
Examines three general forms of abuse and household dysfunction.
The Adverse Experiences
• Child physical abuse
• Child sexual abuse
• Child emotional abuse
• Neglect
• Mentally ill, depressed or suicidal person in the home
• Drug addicted or alcoholic family member
• Witnessing domestic violence against the mother
• Loss of a parent to death or abandonment, including abandonment by divorce
• Incarceration of any family member
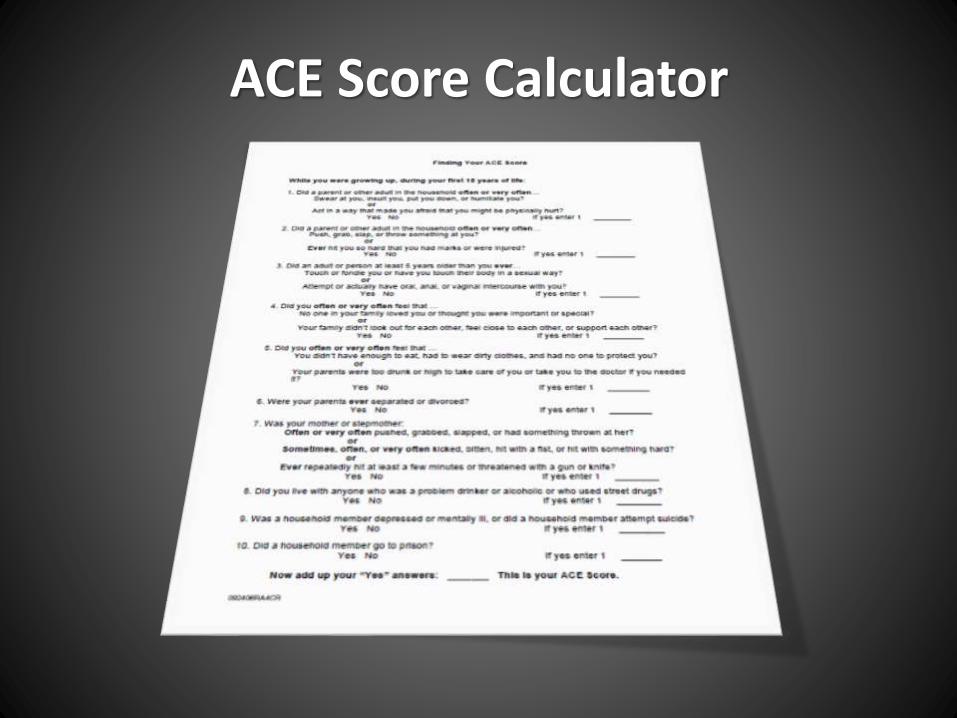
ACE Score Calculator
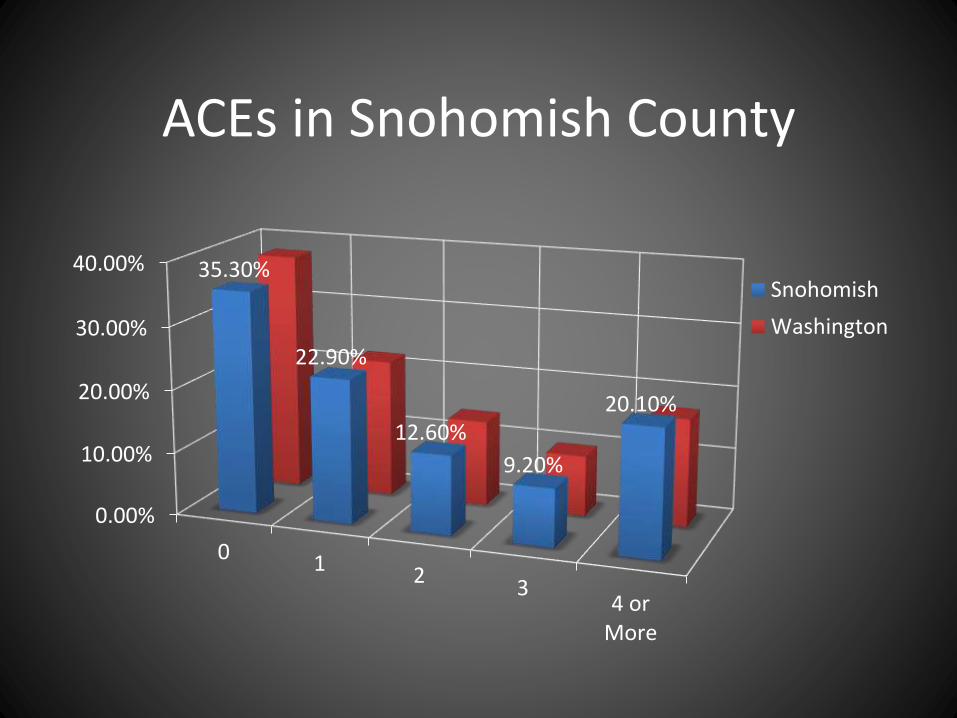
ACEs in Snohomish County
0.00%
10.00%
20.00%
30.00%
40.00%
0 12
34 or
More
35.30%
22.90%
12.60%
9.20%
20.10%
Snohomish
Washington
ACE Study Findings
ACEs are very common.
They are well-concealed.
The ACE Study found that the number of categories, not necessarily the frequency or severity of the experiences within a category, determine health outcomes across the population as a whole.
ACEs are strong indicators of what happens later in life, in terms of health risks, diseases and even premature death.
The Science Behind ACES
A child’s environment and experience
shapes their behavior and health.
Our brain is designed to prioritize
survival.
Cortisol is released when our “Fight,
Flight, or Freeze” response is triggered.
Toxic Stress
Toxic Stress
Prolonged exposure to Cortisol is toxic,
and makes permanent changes to the
brain.
This means you may have students
perfectly suited to survive in their home
environment, but who cannot turn-off
their stress response in the classroom or
other “normal” situations.
Do you recognize these signs of traumatic brain development?
Hypervigilance - “Always on the ready.”
Display of trauma induced ADHD symptoms, including an inability to stay on task or follow directions.
Early onset of sexualized behaviors and activity.
More impulsive, aggressive and disruptivebehaviors, including those leading to suspension.
Being less able to tolerate stress.
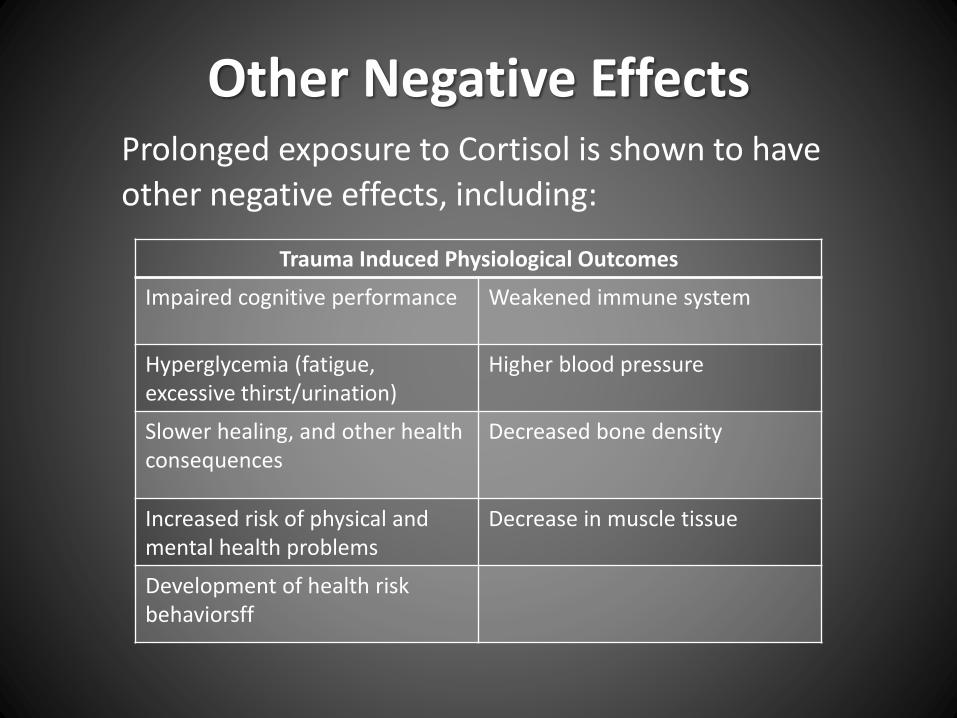
Other Negative EffectsProlonged exposure to Cortisol is shown to have
other negative effects, including:
Trauma Induced Physiological Outcomes
Impaired cognitive performance Weakened immune system
Hyperglycemia (fatigue, excessive thirst/urination)
Higher blood pressure
Slower healing, and other health consequences
Decreased bone density
Increased risk of physical and mental health problems
Decrease in muscle tissue
Development of health risk behaviorsff
Graded Relationships in Health Risk Behaviors
• There is a strong “dose/response” relationship between a person’s ACE score and the likelihoodthey will adopt personal solutions that lead to serious health problems.
• Dose/Response is a direct measure of “cause and effect.”
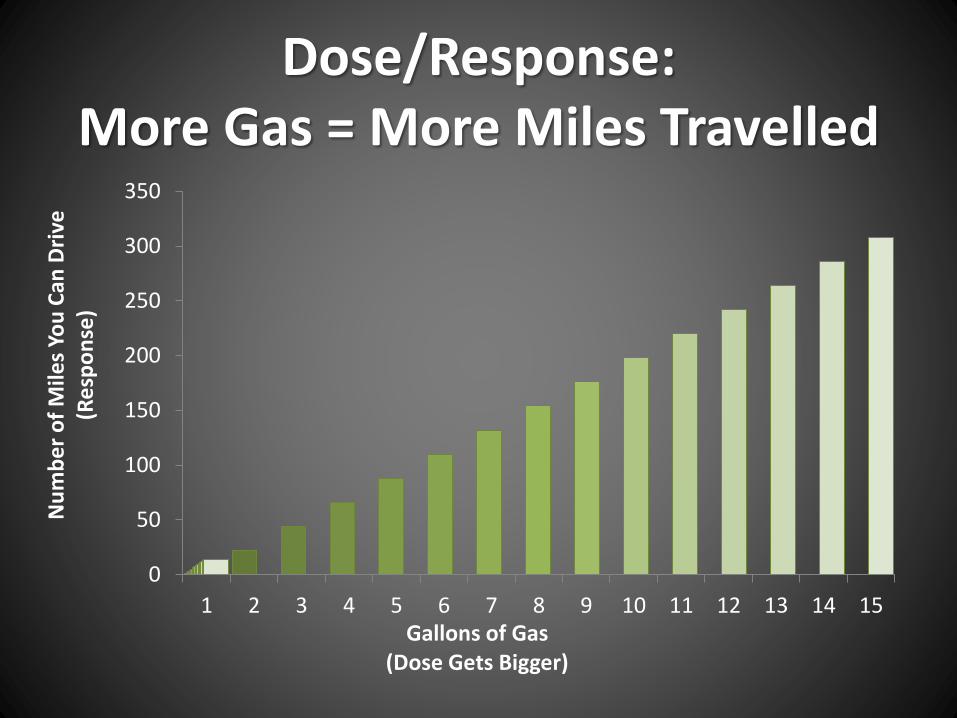
Dose/Response: More Gas = More Miles Travelled
0
50
100
150
200
250
300
350
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Nu
mb
er
of
Mile
s Yo
u C
an D
rive
(R
esp
on
se)
Gallons of Gas(Dose Gets Bigger)
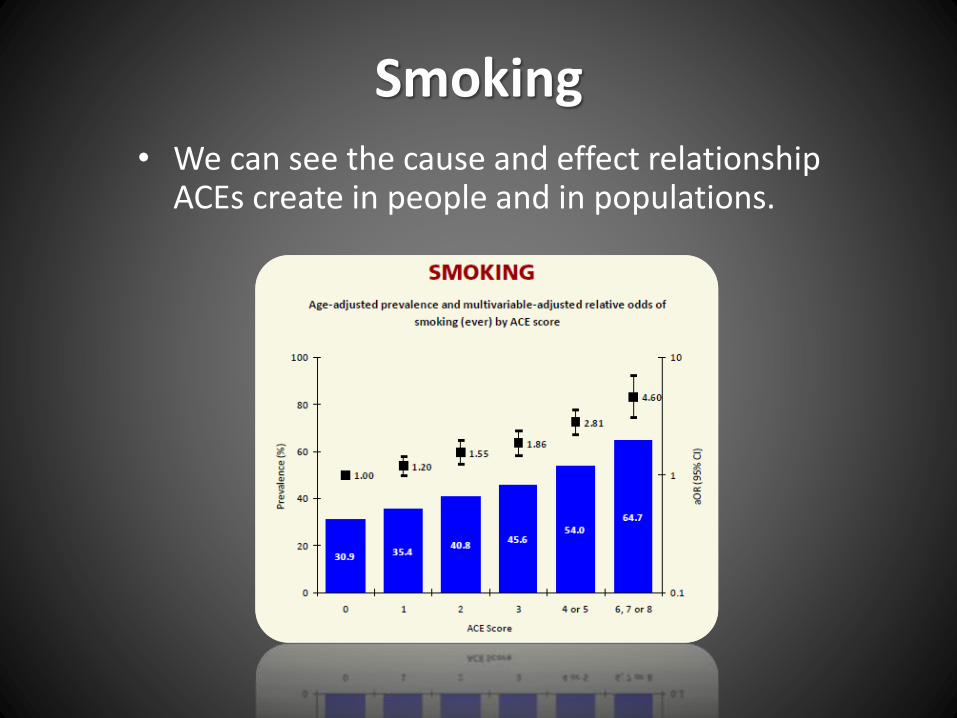
Smoking
• We can see the cause and effect relationship ACEs create in people and in populations.
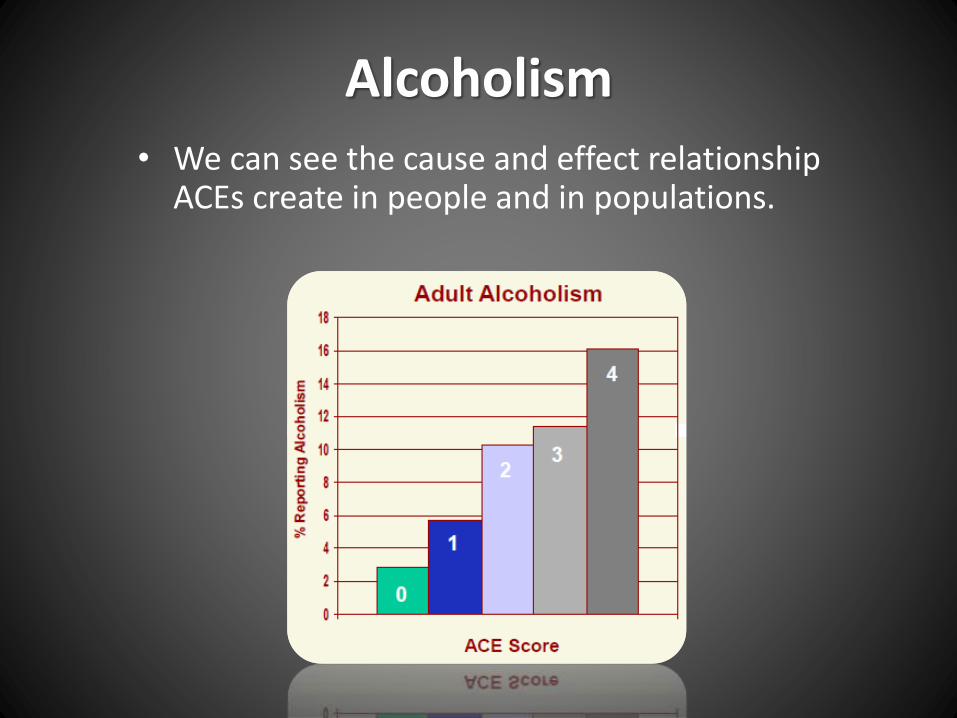
Alcoholism
• We can see the cause and effect relationship ACEs create in people and in populations.
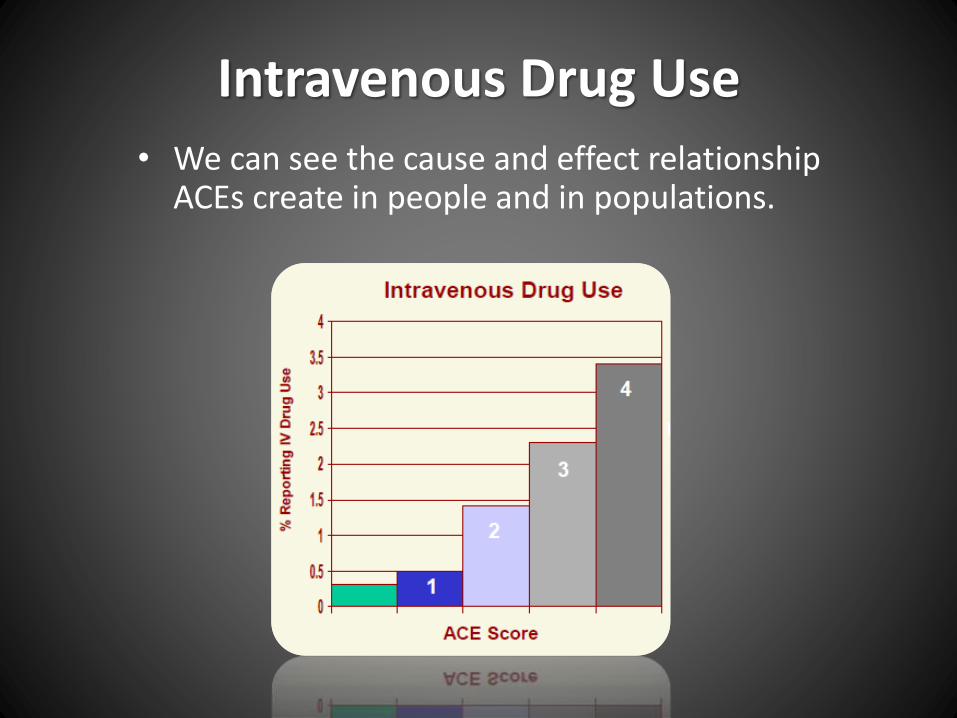
Intravenous Drug Use
• We can see the cause and effect relationship ACEs create in people and in populations.

Chronic Depression
• We can see the cause and effect relationship ACEs create in people and in populations.
0
10
20
30
40
50
60
70
80
0 1 2 3 >=4
% W
ith
a L
ifet
ime
His
tory
of
De
pre
ssio
n
ACE Score
Women
Men
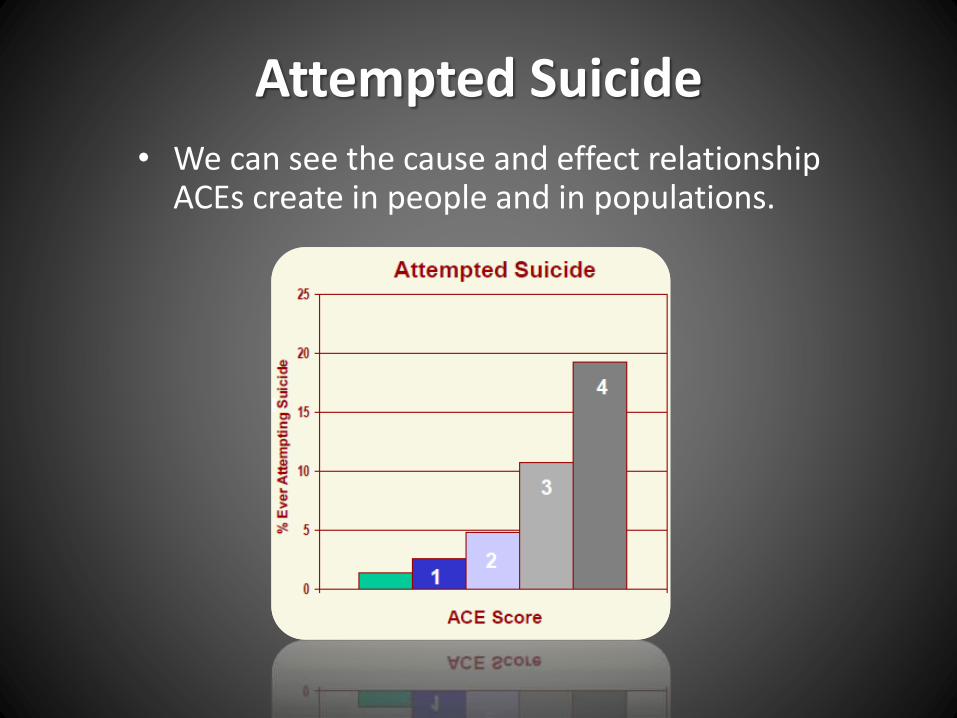
Attempted Suicide
• We can see the cause and effect relationship ACEs create in people and in populations.

ACE lead to risk factors for the 10 most common causes of early
death in the United States
Reframing Our Point of View
• With an ACE score of 0, the majority of adults have few, if any, risk factors for these diseases leading to early death.
• With an ACE score of 4 or more, the majority of adults have multiple risk factors for these diseases or the diseases themselves.
Much of what we see as problem behaviors should actually be viewed as a
personal solution to an unrecognized prior adversity.
ACE Impact Monroe High School
We also know ACE drive :
• Special education needs
• Grade repetition
• Problems at school
• Educator burnout

Meet Mallory

Getting to Know Mallory
• Mallory is in 10th grade at Monroe High School.
• Her counselor Tammy knows Mallory’s mother physically abused the girl in her past. As a result, Mallory’s known ACE Score is “1.”
• Keep in mind - ACEs travel in clusters: Among people exposed to physical abuse, 84% report at least 2 additional ACE.
Mallory’s Grades
Mallory appears to have trouble paying attention in class. She doesn’t turn in her homework and seems to have a hard time following directions -
her grades reflect this.
• Students like Mallory were nearly twice as likely (1.7x) to report getting C’s, D’s and F’s.

Bullying and Safety at School
Mallory has trouble making lasting friendships and is frequently the target of bullying behavior.
• 10th graders like Mallory were:
Nearly twice as likely (1.9x) to report being the victims of bullying.
2.7x as likely to report missing days of school because they felt unsafe.
Mallory’s Mental Health
Mallory seems pretty disengaged in class and always looks tired. She can’t seem to remember facts from 10 minutes ago.
• Students who report being physically abused by an adult were nearly three times as likely* (2.9x) to report being depressed on the most recent HYS.
• They were also 4.6x as likely* to report contemplating suicide.
Mallory’s Personal Solutions
Mallory was caught bringing a flask of alcohol to school in 9th grade. She talked with Dave Ketchell and avoided most of her suspension, but she and her family really haven’t engaged with any helping adults since then.
• Students like Mallory are 2.2x more likely to report current alcohol use.
• They are 2.5x more likely to indicate any other type of current drug use, including Marijuana use.
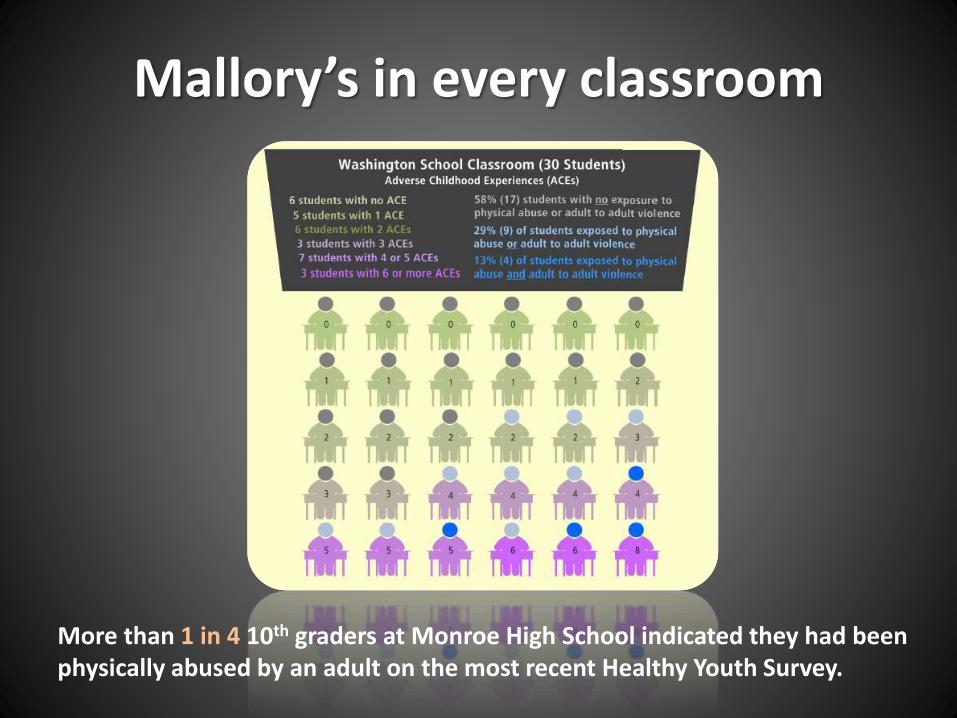
Mallory’s in every classroom
More than 1 in 4 10th graders at Monroe High School indicated they had been physically abused by an adult on the most recent Healthy Youth Survey.
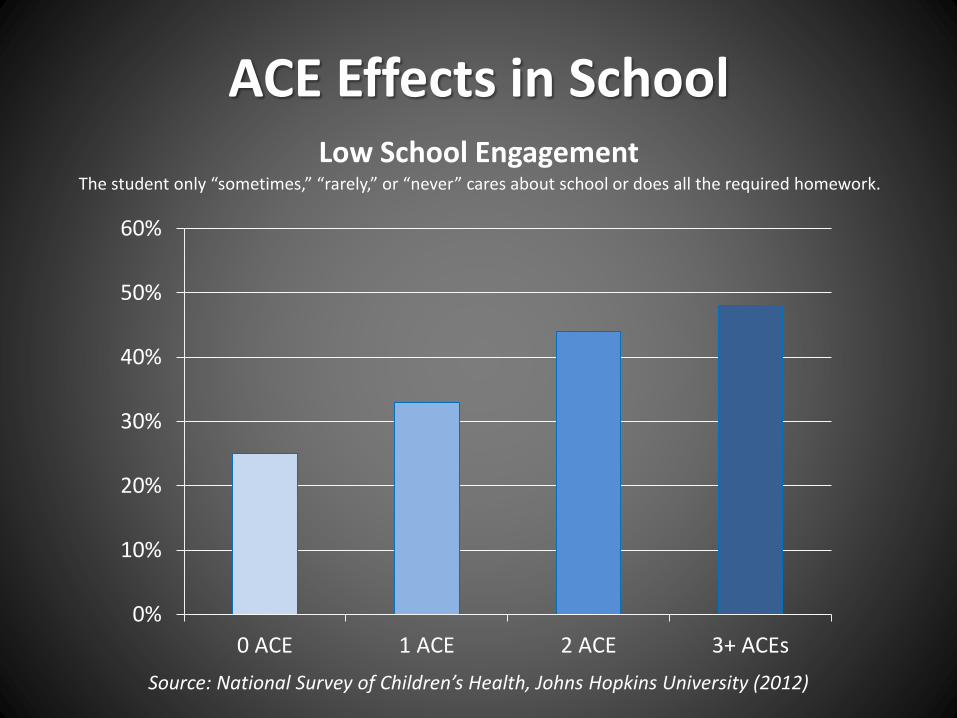
ACE Effects in SchoolLow School Engagement
Source: National Survey of Children’s Health, Johns Hopkins University (2012)
0%
10%
20%
30%
40%
50%
60%
0 ACE 1 ACE 2 ACE 3+ ACEs
The student only “sometimes,” “rarely,” or “never” cares about school or does all the required homework.
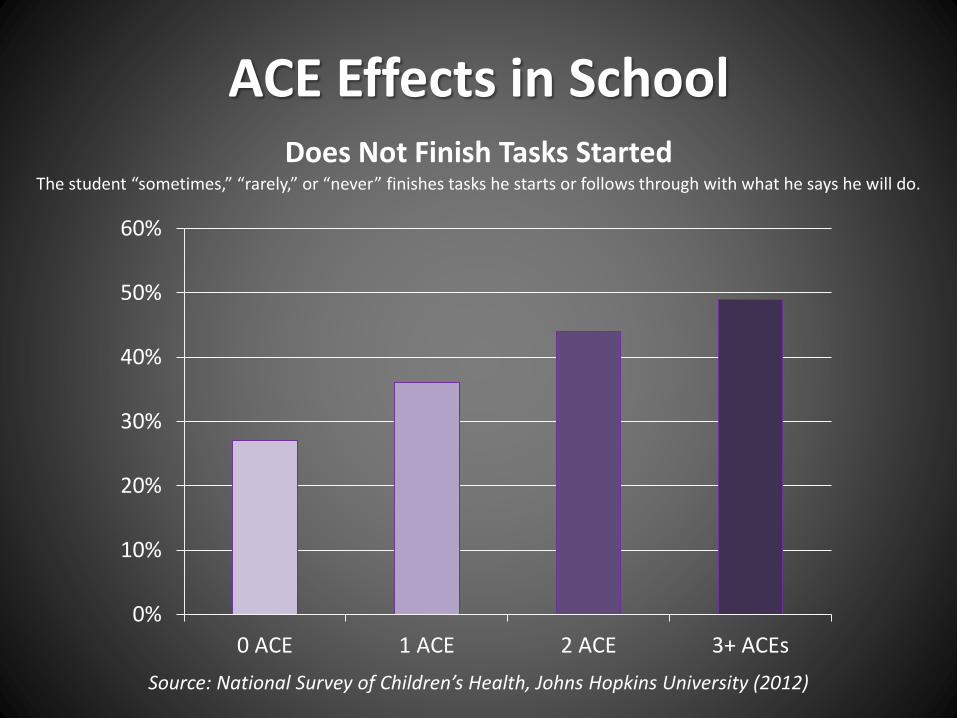
ACE Effects in SchoolDoes Not Finish Tasks Started
Source: National Survey of Children’s Health, Johns Hopkins University (2012)
0%
10%
20%
30%
40%
50%
60%
0 ACE 1 ACE 2 ACE 3+ ACEs
The student “sometimes,” “rarely,” or “never” finishes tasks he starts or follows through with what he says he will do.
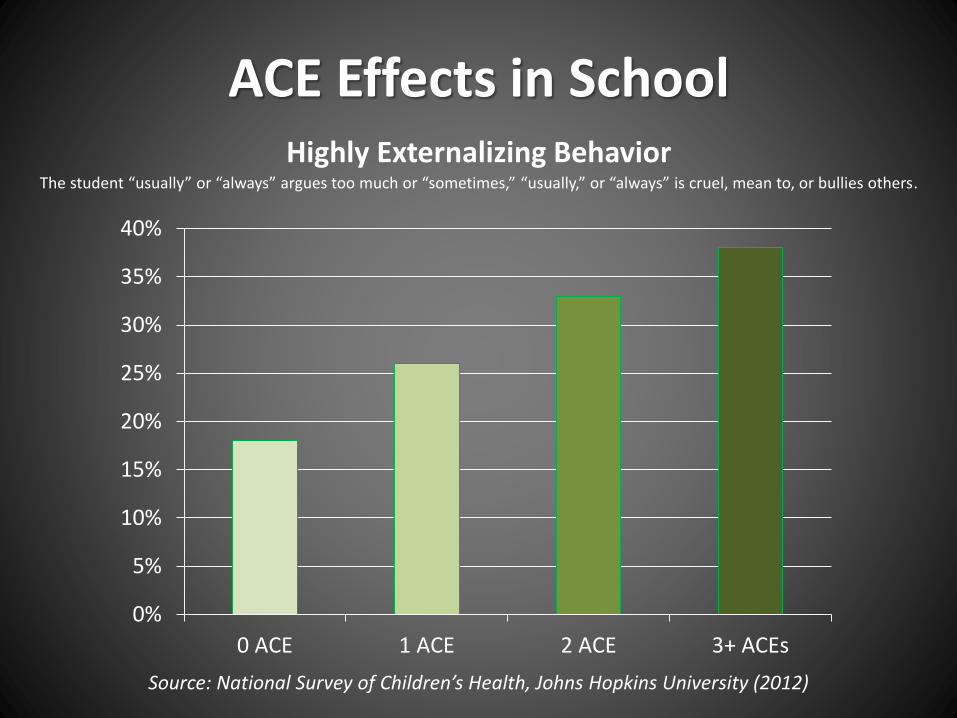
ACE Effects in SchoolHighly Externalizing Behavior
Source: National Survey of Children’s Health, Johns Hopkins University (2012)
0%
5%
10%
15%
20%
25%
30%
35%
40%
0 ACE 1 ACE 2 ACE 3+ ACEs
The student “usually” or “always” argues too much or “sometimes,” “usually,” or “always” is cruel, mean to, or bullies others.
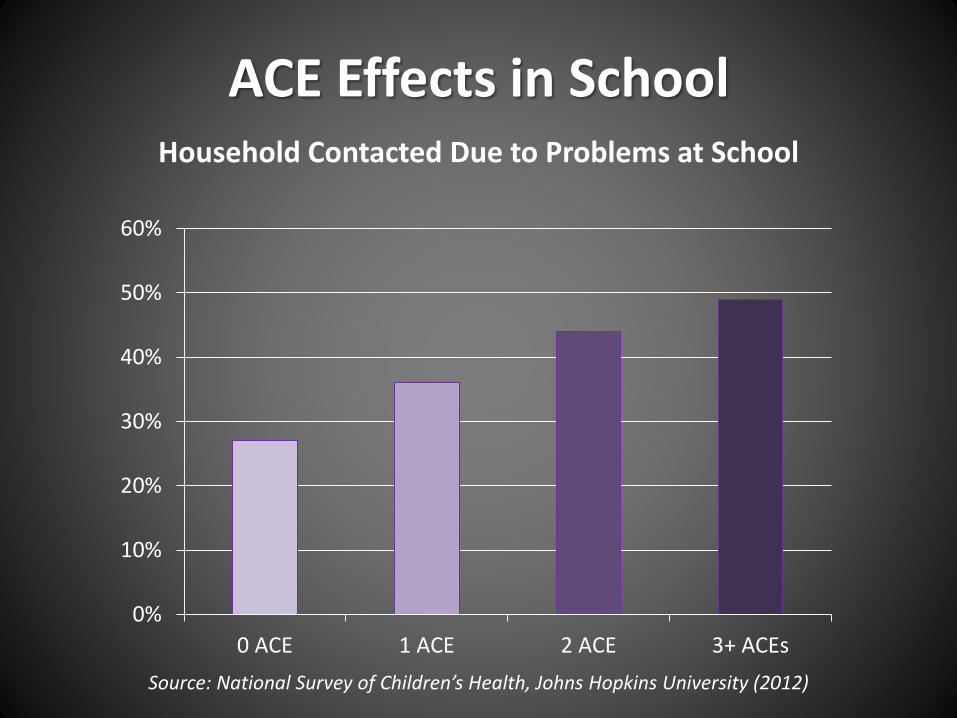
ACE Effects in SchoolHousehold Contacted Due to Problems at School
Source: National Survey of Children’s Health, Johns Hopkins University (2012)
0%
10%
20%
30%
40%
50%
60%
0 ACE 1 ACE 2 ACE 3+ ACEs
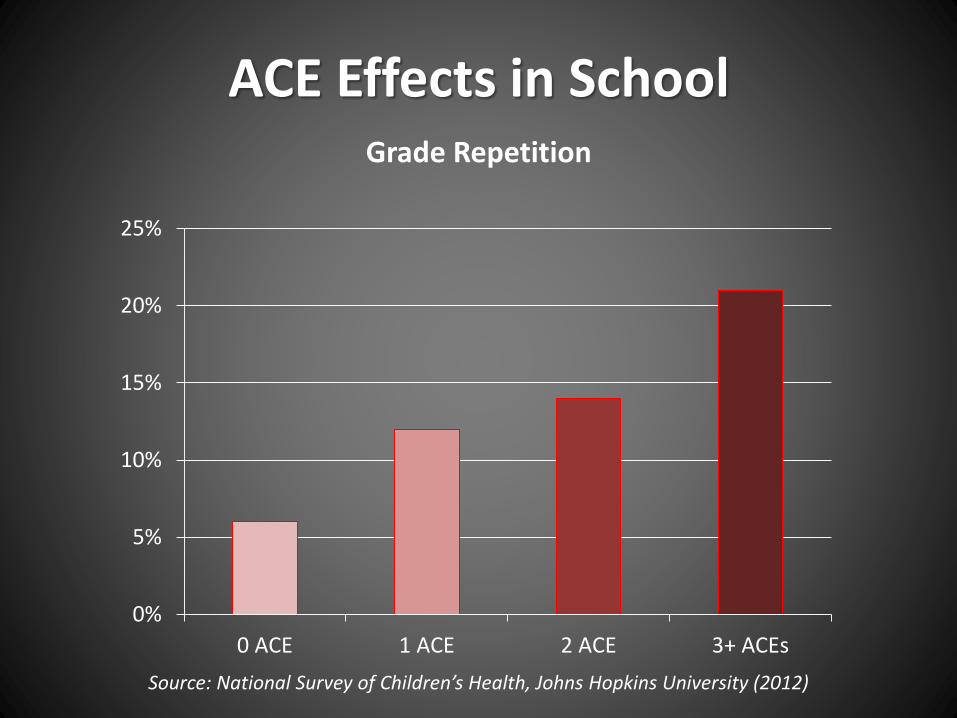
ACE Effects in SchoolGrade Repetition
Source: National Survey of Children’s Health, Johns Hopkins University (2012)
0%
5%
10%
15%
20%
25%
0 ACE 1 ACE 2 ACE 3+ ACEs
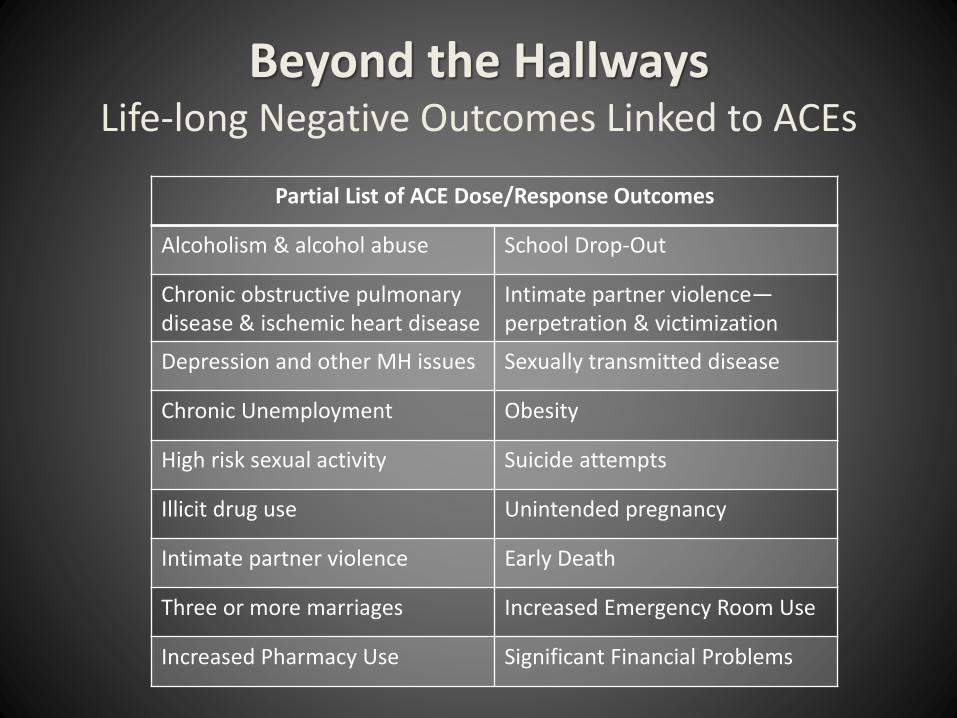
Beyond the HallwaysLife-long Negative Outcomes Linked to ACEs
Partial List of ACE Dose/Response Outcomes
Alcoholism & alcohol abuse School Drop-Out
Chronic obstructive pulmonary disease & ischemic heart disease
Intimate partner violence—perpetration & victimization
Depression and other MH issues Sexually transmitted disease
Chronic Unemployment Obesity
High risk sexual activity Suicide attempts
Illicit drug use Unintended pregnancy
Intimate partner violence Early Death
Three or more marriages Increased Emergency Room Use
Increased Pharmacy Use Significant Financial Problems
What Are the Implications?To put it simply, childhood experiences are the most
powerful determinants of who we become as adults.
Population Attributable Risk
PAR = The difference in rate of a condition
between an exposed population and an
unexposed population.
In this case, it is a calculation used by the
CDC to estimate the proportion of a health
outcome caused by ACE.
Takes into account:
The increased risk due to each level of ACE
The prevalence of the number of ACE categories
Population Attributable Risk
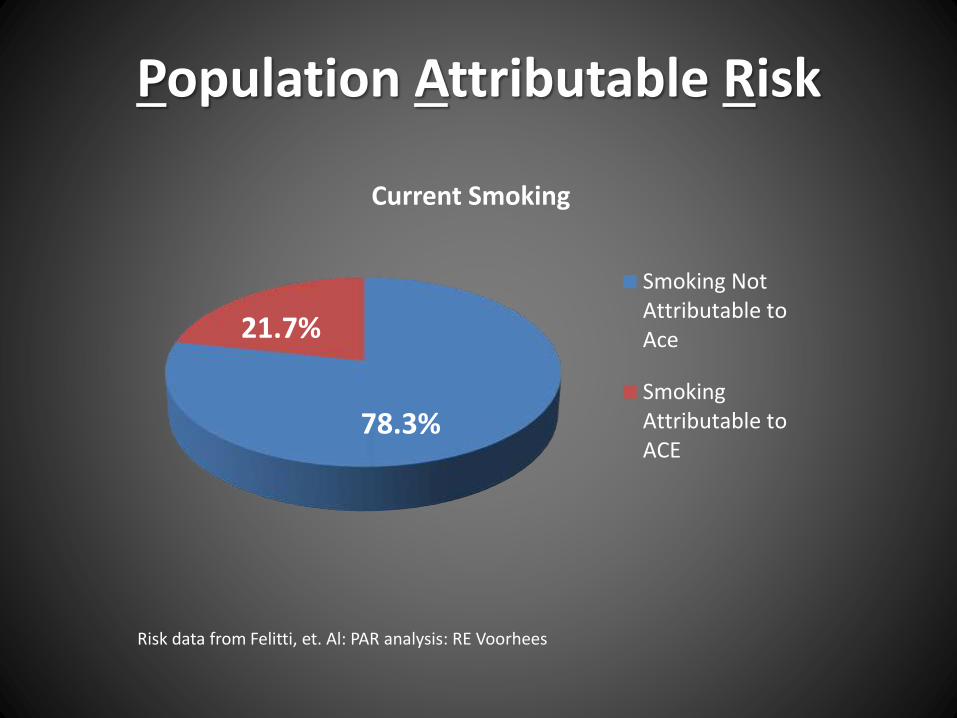
Current Smoking
Smoking NotAttributable toAce
SmokingAttributable toACE
78.3%
21.7%
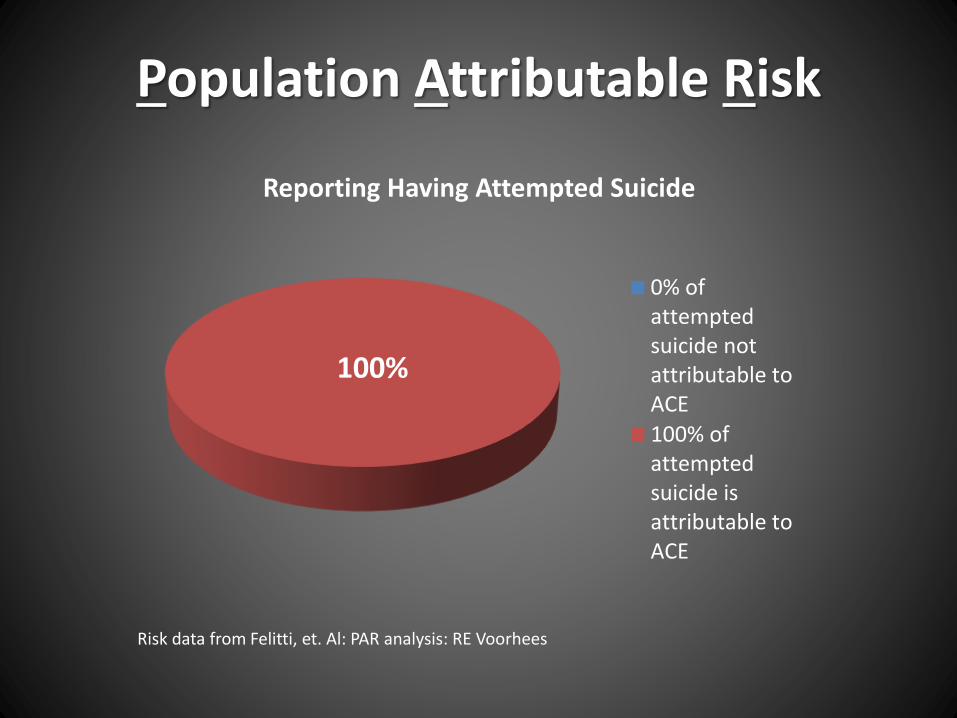
Risk data from Felitti, et. Al: PAR analysis: RE Voorhees
Population Attributable Risk
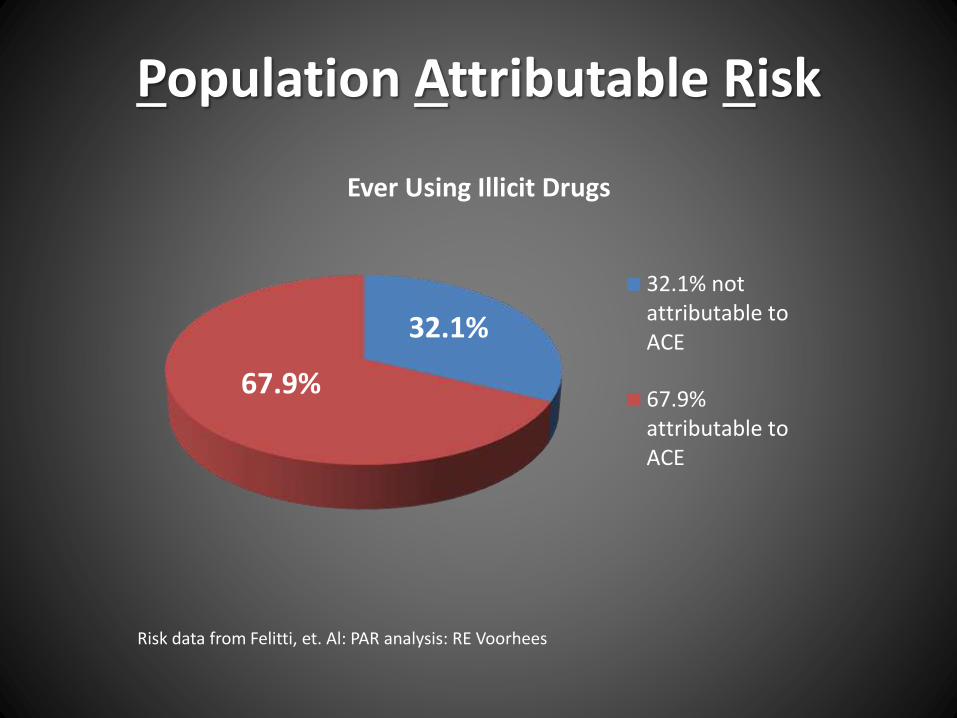
Ever Using Illicit Drugs
32.1% notattributable toACE
67.9%attributable toACE
Risk data from Felitti, et. Al: PAR analysis: RE Voorhees
67.9%
32.1%

Population Attributable Risk
Risk data from Felitti, et. Al: PAR analysis: RE Voorhees
Alcoholism
3.2% of self-reportedalcoholism notattributable toACE
96.8% of self-reportedalcoholismattributable toACE
96.8%
3.2%
Population Attributable Risk
Risk data from Felitti, et. Al: PAR analysis: RE Voorhees
Reporting Having Attempted Suicide
0% ofattemptedsuicide notattributable toACE
100% ofattemptedsuicide isattributable toACE
100%
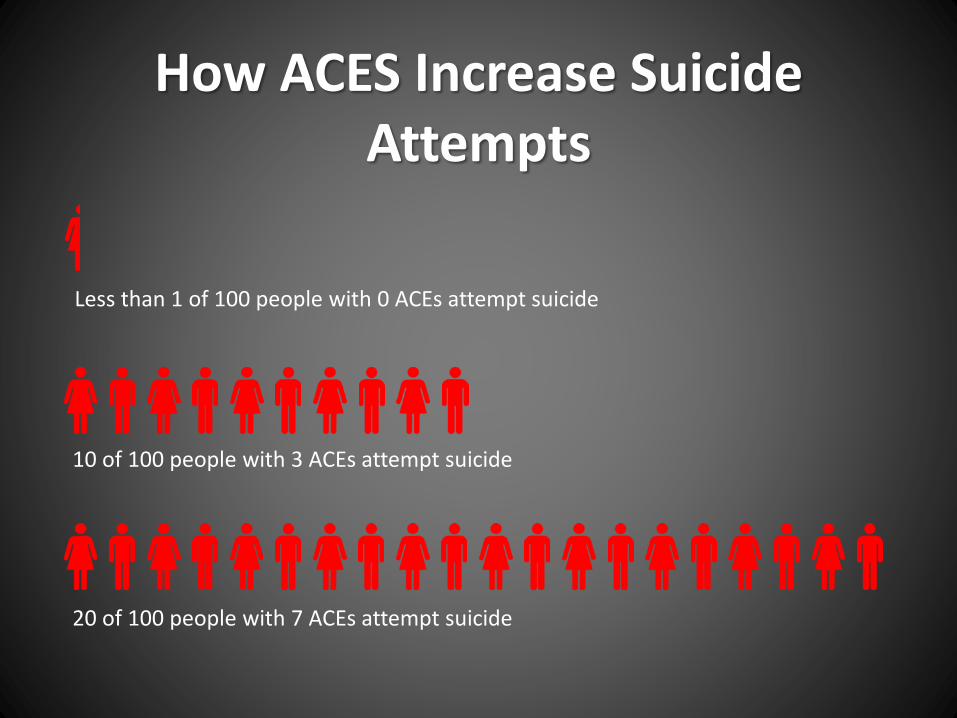
How ACES Increase Suicide Attempts
Less than 1 of 100 people with 0 ACEs attempt suicide
10 of 100 people with 3 ACEs attempt suicide
20 of 100 people with 7 ACEs attempt suicide
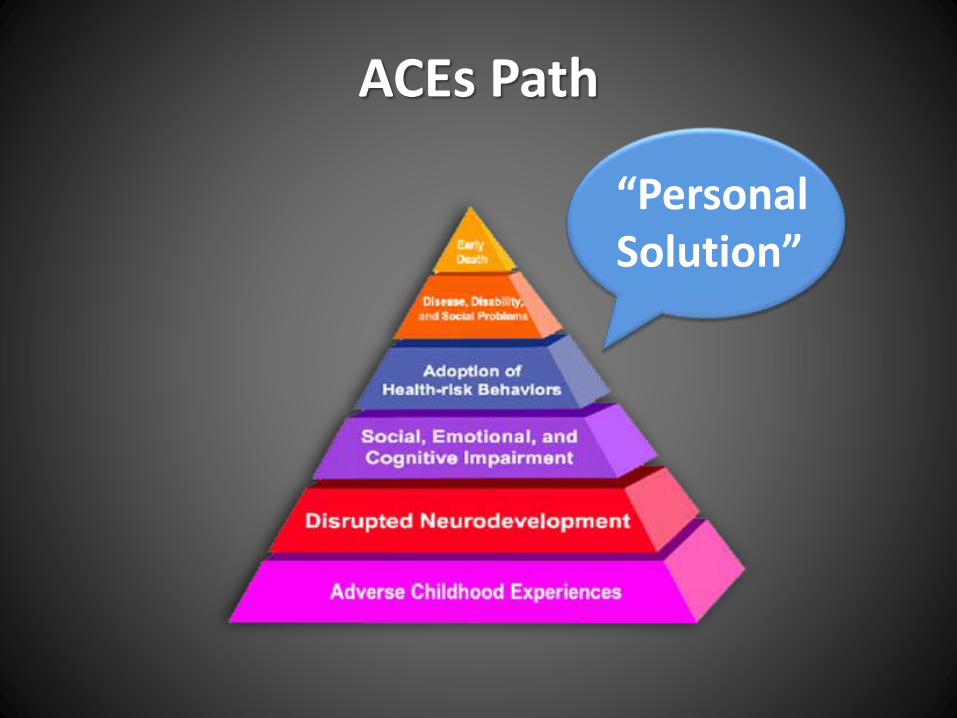
ACEs Path
“Personal Solution”
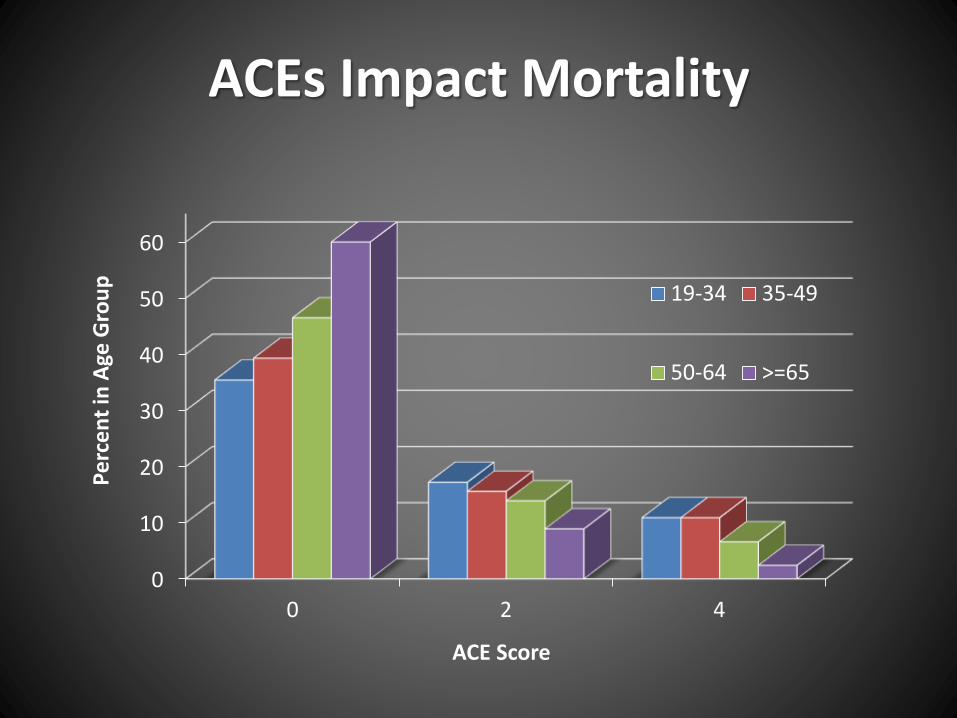
ACEs Impact Mortality
0
10
20
30
40
50
60
0 2 4
Pe
rce
nt
in A
ge G
rou
p
ACE Score
19-34 35-49
50-64 >=65
Psychological Depletion
• Whether you like it or not, counselors and educators at MHS are on the ACE frontline.
• The constant demand of caring for others as you manage your students and classrooms can lead to burnout:
• Illness
• Chronic fatigue
• Emotional exhaustion
• Indifference or detachment
• Isolation from colleagues
• A lack of personal satisfaction
• Trauma-informed schools and classrooms can create an environment where students with injured brains have the best opportunity to learn.
• Evidence-based Kernels can lead you from intuitive responses to intentional action.
• Mood is your internal emotional state.
• Affect is how you externalize your emotions through verbal and non-verbal cues.
• Research shows that trauma-impacted youth are particularly aware of changes in affect, which trigger the fight, flight, or freeze response and decreases the capacity to learn.
Attachment, Self-Regulation & CompetencyKinniburgh, Blaustein, Spinazzola & van der Kolk, 2005, Psychiatric Annals, pp. 424-430.
ARC - Managing Affect
• Traumatized students often have difficulty communicating, so their behaviors may become a “front” for conveying unmet needs or unregulated affect.
• Adults may respond to the most distressing symptom, rather than the underlying emotion or need.
• Ask - “What’s happening here?” rather than, “What’s wrong with this child?”
Attachment, Self-Regulation & CompetencyKinniburgh, Blaustein, Spinazzola & van der Kolk, 2005, Psychiatric Annals, pp. 424-430.
ARC - Attunement

• Being predictable by having consistent responses to student behavior is vital to establishing safety and reducing a child’s need to exert control.
• An intentional focus on building success, rather than establishing limits – which may be associated with powerlessness or vulnerability – should be your priority.
• Traumatized children may initially react to both negative or positive responses.
Attachment, Self-Regulation & CompetencyKinniburgh, Blaustein, Spinazzola & van der Kolk, 2005, Psychiatric Annals, pp. 424-430.
ARC - Consistency
• Building routines and rituals, particularly around trouble areas, can make your classroom fun and predictable.
• Research shows that establishing routines enhances student:
Feelings of safety
Ability to build trust and feelings of reliability within a relationship
Anticipation of an event, which reduces stress
Attachment, Self-Regulation & CompetencyKinniburgh, Blaustein, Spinazzola & van der Kolk, 2005, Psychiatric Annals, pp. 424-430.
ARC - Routines & Rituals
• These four strategies come from the Attachment, Self-Regulation and Competency research conducted by Kinniburgh and Blaustein.
• You can learn more about ARC framework and training atwww.traumacenter.org
• The Compassionate Schools Initiative from OSPI also provides a framework for understanding the negative impacts of stress and trauma on learning.
ARC & Compassionate Schools
• Kernels are low or no-cost to implement.
• This means we can unleash access to strategies that support safety, relationship and skill building essential to our student’s readiness to learn.
• Kernels give us a way to implement evidence-based practices that will interrupt the ACES trajectory,move us from intuition tointention, and improve classroom outcomes.
• A kernel is the smallest unit of scientifically proven behavioral influence.
• Kernels produce quick easily measured change that can grow into much bigger change over time.
• They can be used alone OR combined with other kernels to create new programs, strategies or policies.
• Combinations of Kernels are considered “behavioral vaccines.”
• “Planted” Kernels create a culture.
What is a Kernel?
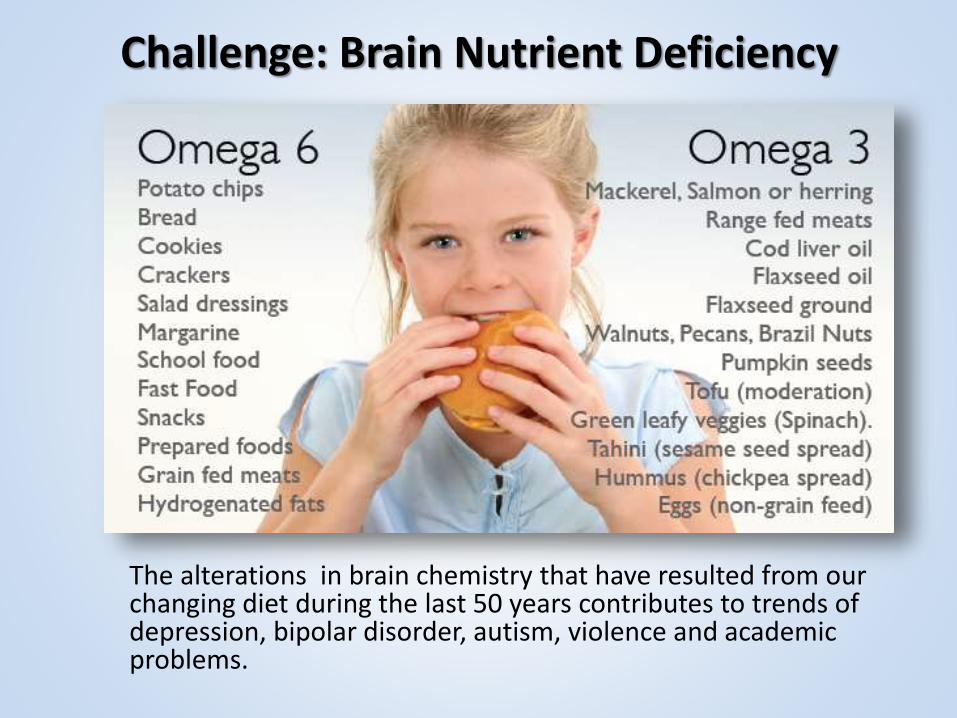
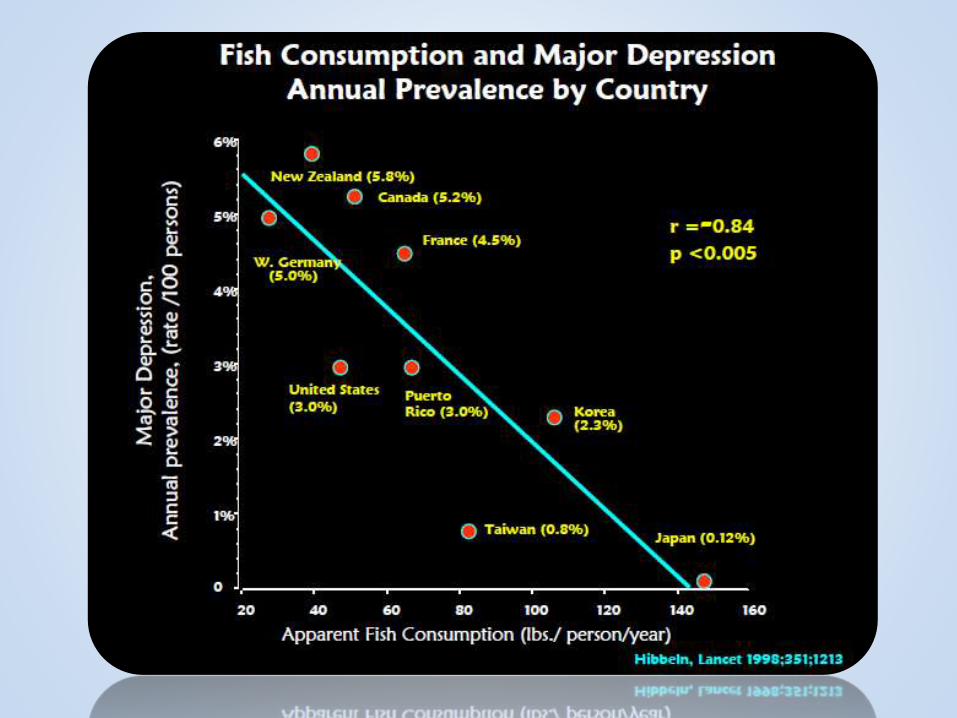
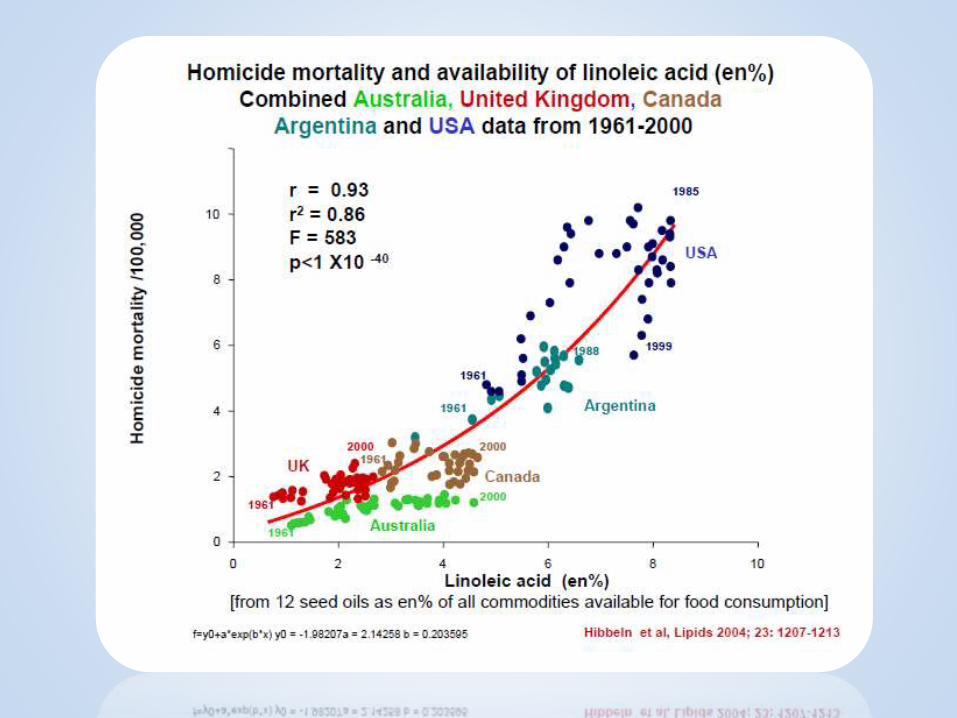
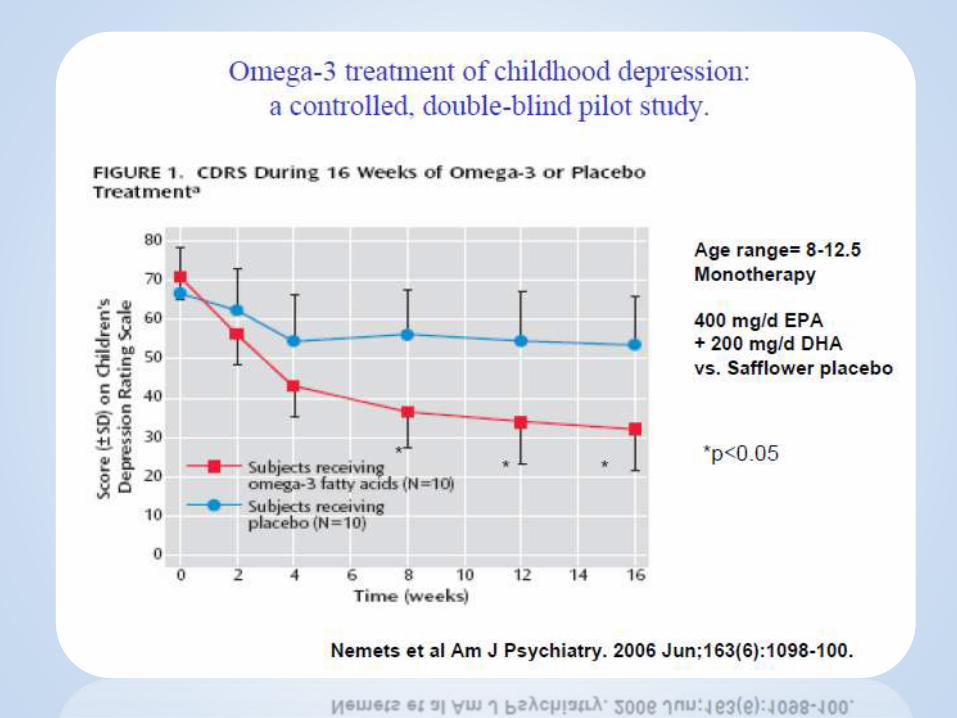
The alterations in brain chemistry that have resulted from our changing diet during the last 50 years contributes to trends of depression, bipolar disorder, autism, violence and academic problems.
Challenge: Brain Nutrient Deficiency
Omega-3 Supplementation
• Omega 3 has no harmful effects
• Well-documented evidence for Reducing aggression, depression, anxiety, bipolar disorder, post partum depression and borderline personality disorder
• 2002 Oxford University study and 2009 Dutch Corrections study of found Omega-3 supplementation achieved a 37% reduction in episodes of inmate aggression.
• In 2006, the American Psychiatric Association recommend that all psychiatric patients receive at least 1 gram of omega-3 per day to reduce symptoms of mental illness.

Why haven’t we heard this before?!
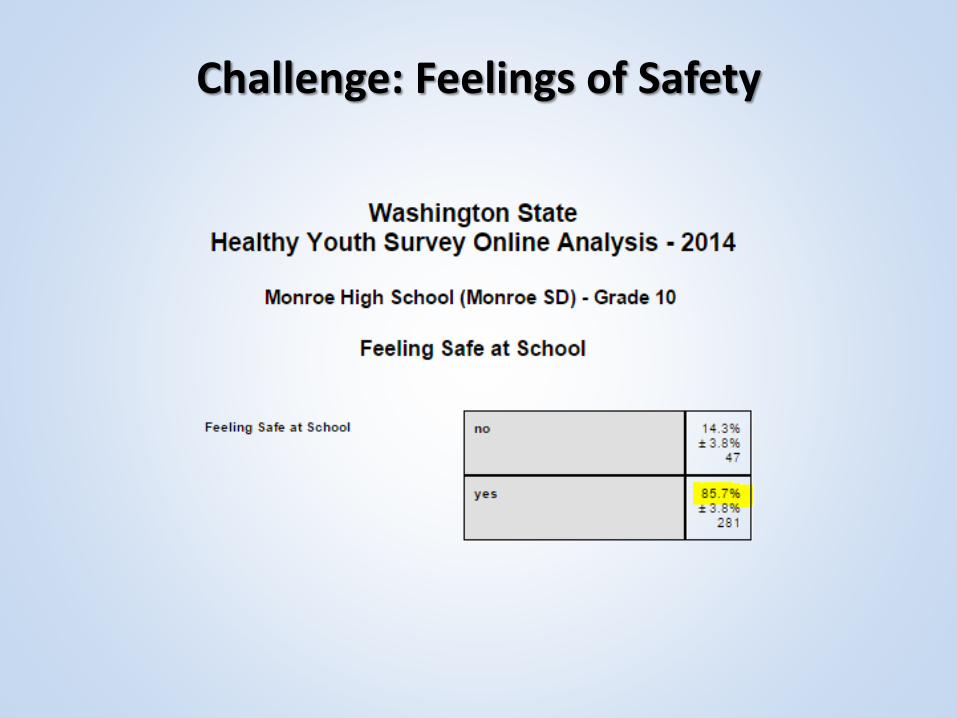
Challenge: Feelings of Safety

• Also known as “handshakes.”
• Frequent friendly physical and verbal greetings impact social status and perceptions of safety and harm.
• It also affects behavior streams of aggression, hostility and politeness.
Pleasant Greeting with Physical Touch
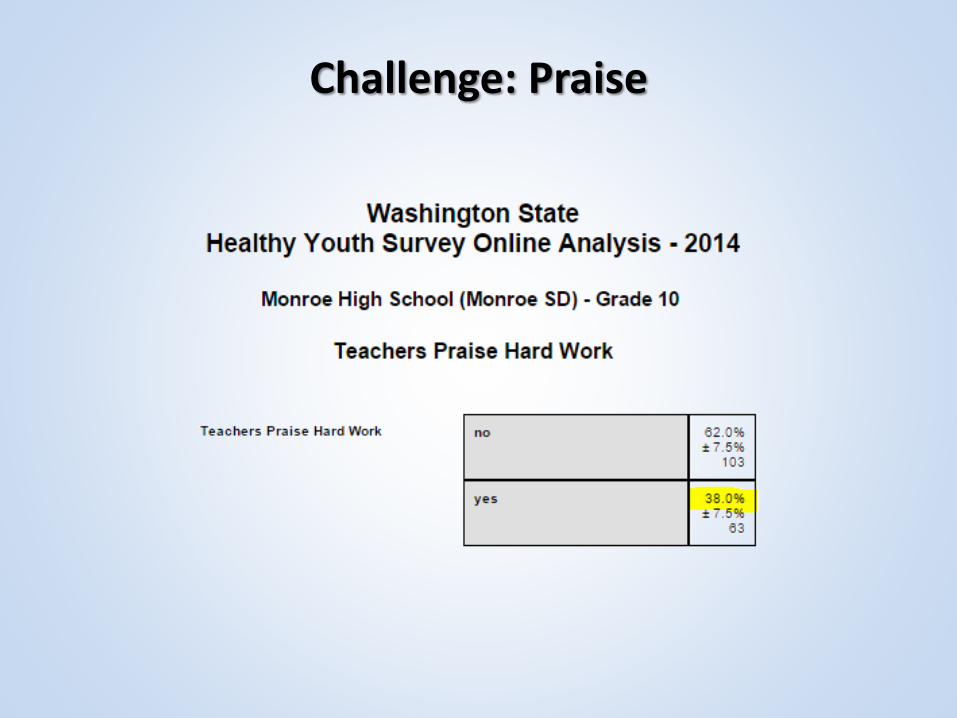
Challenge: Praise
When any person receives specific, spoken recognition for engagement in a target act or behavior, it is widely demonstrated to:
• Improve school performance
• Improve adult/child interactions
• Improve organizational functioning
• Increase engagement in thenoticed behavior
Verbal Praise
Verbal Praise As a Social Reinforcer
What are the social reinforcers in your classroom for this behavior?
Paying attention.
Verbal Praise As a Social Reinforcer
How about for this behavior?
Showing off.
Peer to Peer Notes
Notes of praise written from one peer to another, then read aloud or posted on a public display is widely shown to:
• Increase positive friendships
• Reduce neighborhood disorganization and crime
• Increase sense of safety
• Increase volunteerism
• Increase engagement in the noticed behavior
Adult to Child Notes
Notes from adults to children recognizing them for a specific action or behavior is demonstrated to help students of all ages to:
• Do better at school
• Be more socially competent
• Reduce ADHD, aggression and problem behaviors
• Increase engagement in thenoticed behavior
Beat the Timer
Beat the timer makes daily routines run smoother, reduces parent/child conflict and reduces accidental attention to negative behavior.
Research shows that this simple game:
• Increases compliance
• Increases accuracy and completion of homework
• Helps with chores
Copy Cat (Paragraph Shrinking)
• After talking with your student, ask him to repeat what was said in 8-10 words.
• Repeat if summary is poor.
• Praise if the summary is good.
• Helps with retention and understanding of what is said or read.
Random Calling
This kernel is sometimes referred to as “Ritalin on a Stick” and is proven effective by research.
Random calling results in:
• Equality in participation
• Increased attention to the lesson
• Increased academic performance
• Decreased disruptive behavior
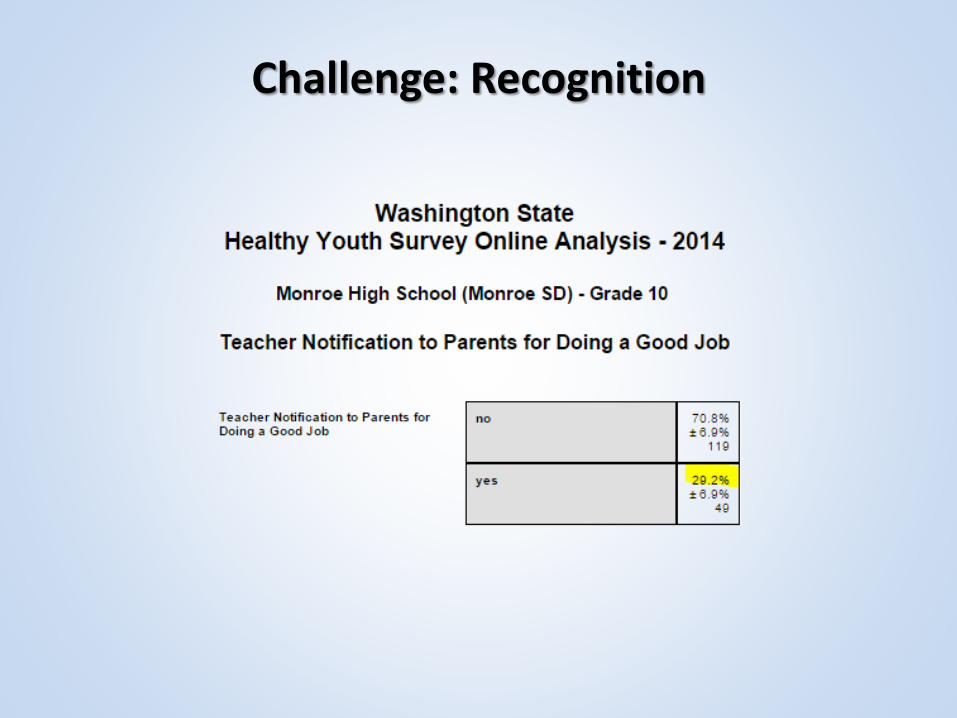
Challenge: Recognition
Positive Note Home for Inhibition
A positive note sent home with a student for inhibiting an otherwise disruptive behavior is show to:
• Reduce disruptive and aggressive behavior
• Reduce problems at home
• Increase engagement atschool
Principal Lottery
When a status figure sends a note home or calls a parent about a student’s positive behavior, research shows that action results in:
• Increases in academic achievement
• Reductions in disruptive behavior
• Reductions in aggression
Auditory/Visual Signal for Transition
The attention kernel works for students and adults. It results in:
• Immediate reduction in transition time
• Increased academic engagement
• Reduced disruptive behavior
• Reduced aggression and bullying
• Reduced trauma response in traumatized people.
Premack’s Principle
Also known as Contingency Management, the Mystery Motivator, Granny’s Wacky Prizes, Prize Bowl and the Game of Life. Results in:
• Reduction in deviant behavior across the lifespan
• Reduction in problem behaviors at school
• Increases desirable behavior in all age groups
• Reduces addiction.
• Motivates youth and adults to do their best and improve
• Promotes self-regulation instead of excitement
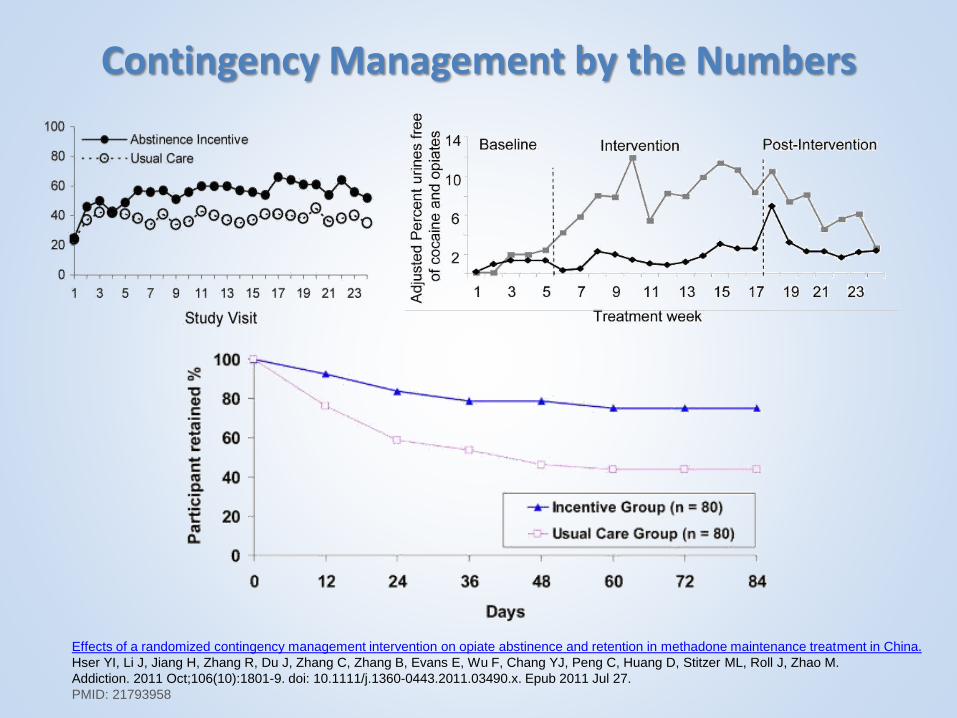
Contingency Management by the Numbers
Effects of a randomized contingency management intervention on opiate abstinence and retention in methadone maintenance treatment in China.
Hser YI, Li J, Jiang H, Zhang R, Du J, Zhang C, Zhang B, Evans E, Wu F, Chang YJ, Peng C, Huang D, Stitzer ML, Roll J, Zhao M.
Addiction. 2011 Oct;106(10):1801-9. doi: 10.1111/j.1360-0443.2011.03490.x. Epub 2011 Jul 27.
PMID: 21793958
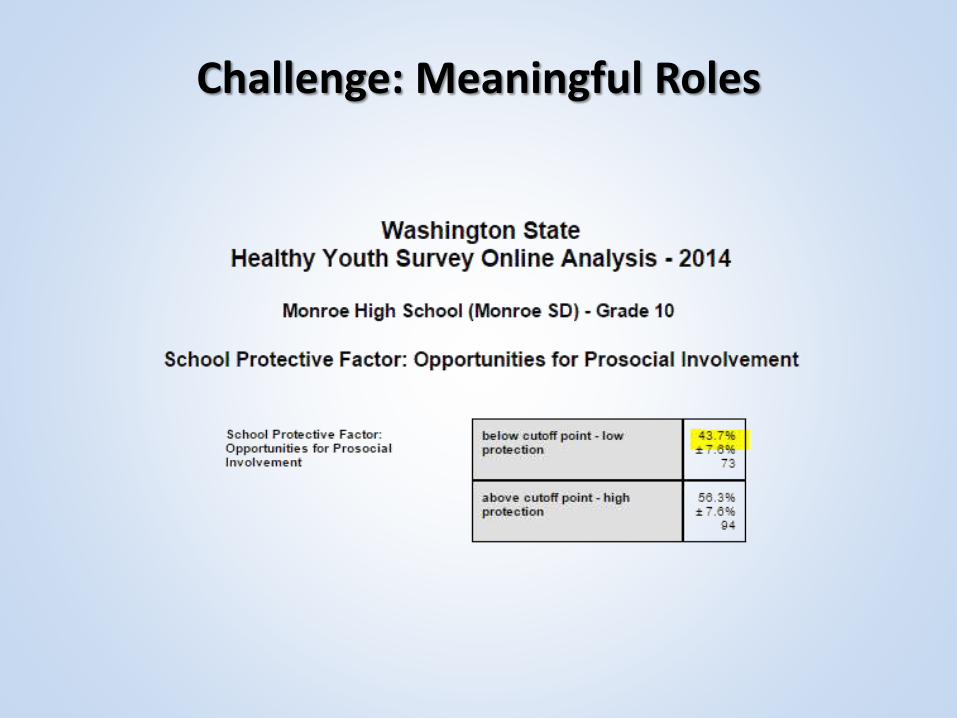
Challenge: Meaningful Roles

The Social Development Strategy
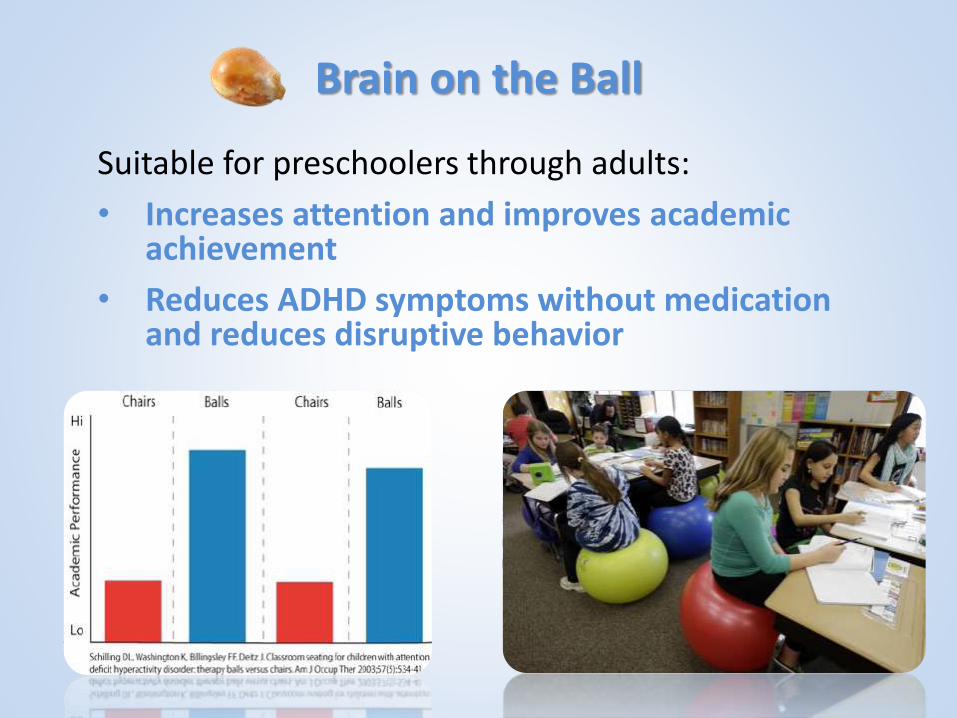
Brain on the Ball
Suitable for preschoolers through adults:
• Increases attention and improves academic achievement
• Reduces ADHD symptoms without medication and reduces disruptive behavior
3 C’s: Clarify, Consider, Choose
• Every student in middle school learns an evidence-based framework for making decisions.
• Step 1: Clarify what decision you need to make.
• Step 2: Consider the available alternatives.
• Step 3: Choose the best alternative for you.
LifeSkills Training In Middle Schools
• Our middle school science teachers are very quietly making a significant difference right under our noses!
• They have taught your students everything from decision making to stress management skills.
• Since renewing our focus on implementing with fidelity, we have achieved:
A 42% reduction in 8th grade perceived use of drugs
A 50% reduction in 8th grade binge drinking
A 29% reduction in 8th grade marijuana use
• How can we reinforce their incredible work?

Many Other Kernels
Graphic/Node Maps
Choral Responding
Peer to Peer Tutoring
Nasal Breathing
Private Reprimands
More!
The Bottom Line
• Understanding ACES gives you the power to significantly impact the trauma trajectory of youth in your classroom.
• Remember Kaiser Permanente’s diet and nutrition program dropouts? The researchers learned that their very successful intervention wasn’t just treating nutrition problems, it was treating personal solutions!
• If you take away a person’s solution before they discover a better one, and you’re just digging a hole for them to fall back into.
• Partner with me. If you need it, I give you my permission to do what’s in your heart.
Johnny

ResourcesPresenter: Joe Neigel
Monroe Community Coalition
200 E Fremont
Monroe, WA 98272
(360) 804-2594
Power Point: http://www.slideshare.net/jneigel/aces-and-kernels-parents-2013-04
Kernels: http://promiseneighborhoods.org/kernels/
Or
http://bit.ly/embry_kernels
ACES: http://www.cdc.gov/ace/index.htm
Or
http://www.acestudy.org/
Or
http://www.fpc.wa.gov/
Or
http://www.acestoohigh.com
ARC Training: http://www.traumacenter.org/research/ascot.php
OSPI Initiative: http://www.k12.wa.us/CompassionateSchools/
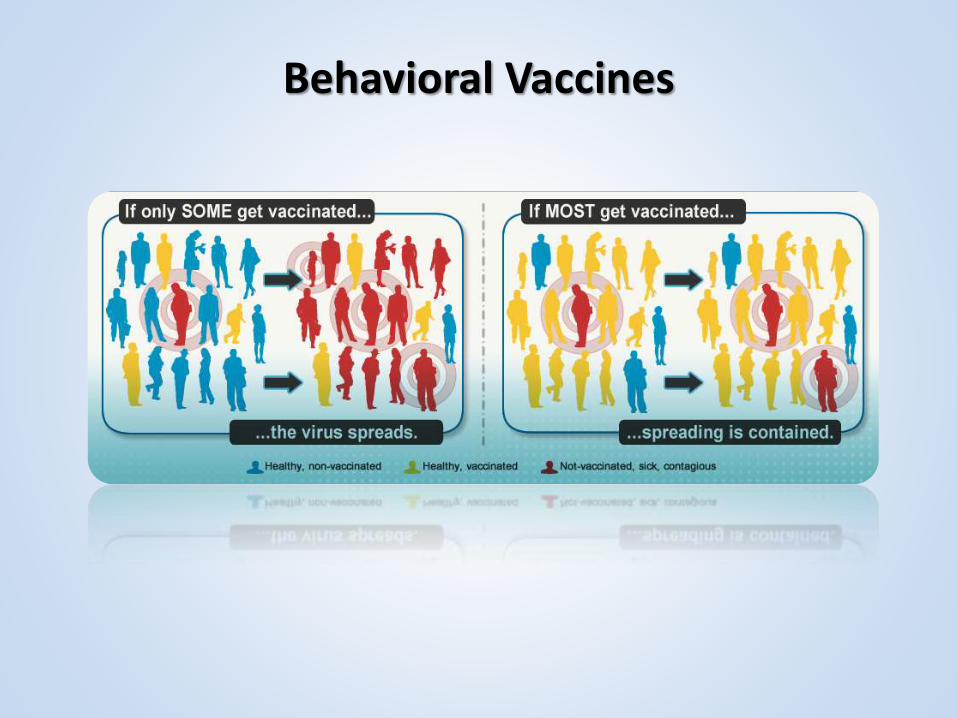
Behavioral Vaccines

Good Behavior Game Active Ingredients
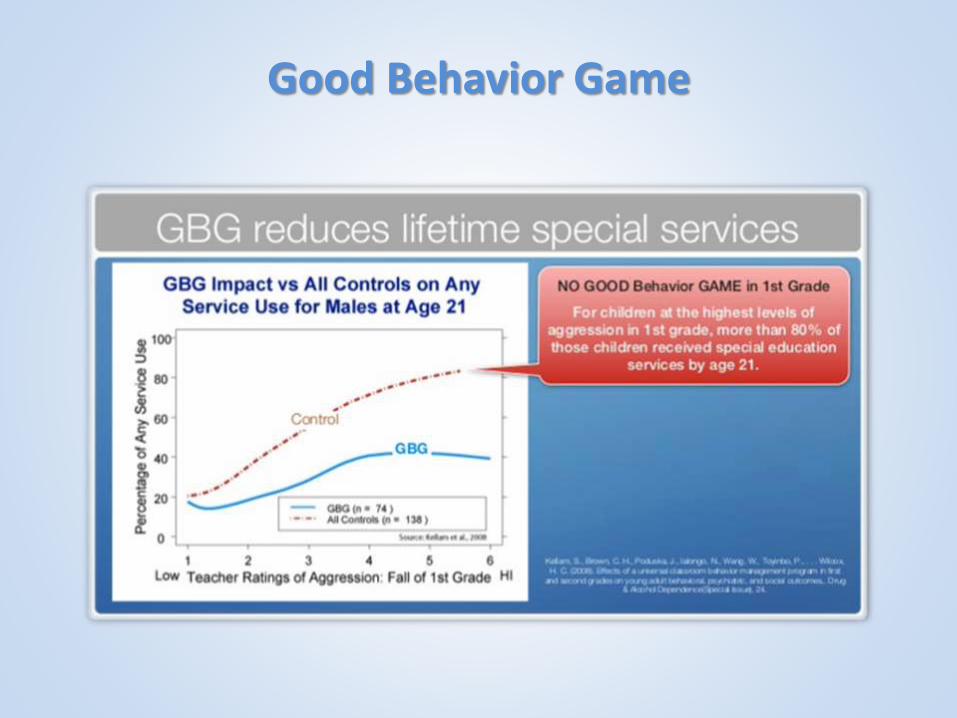
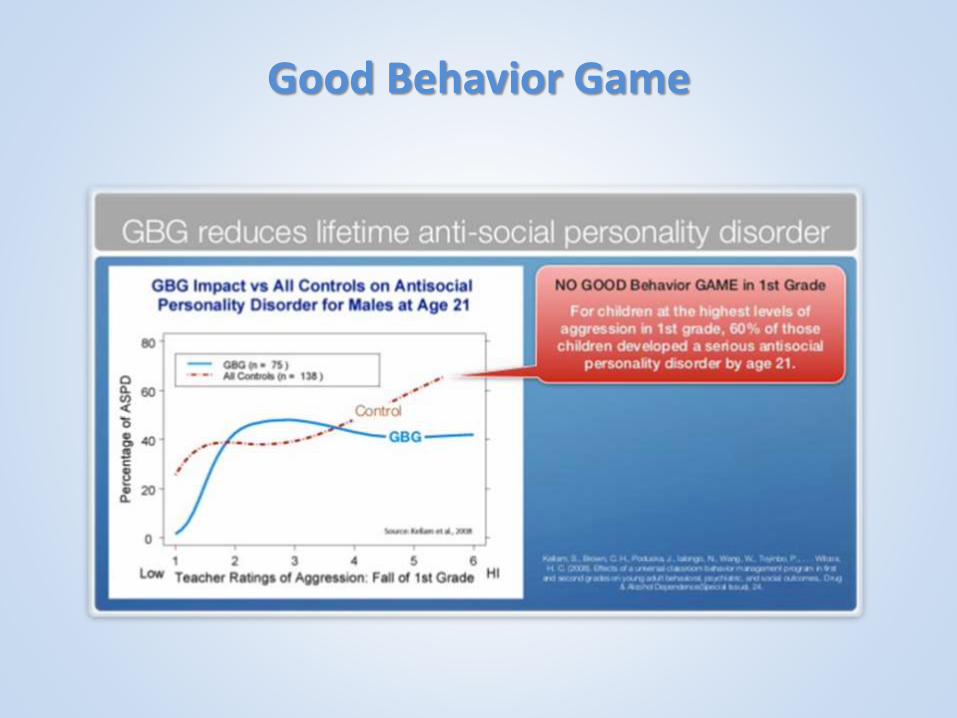
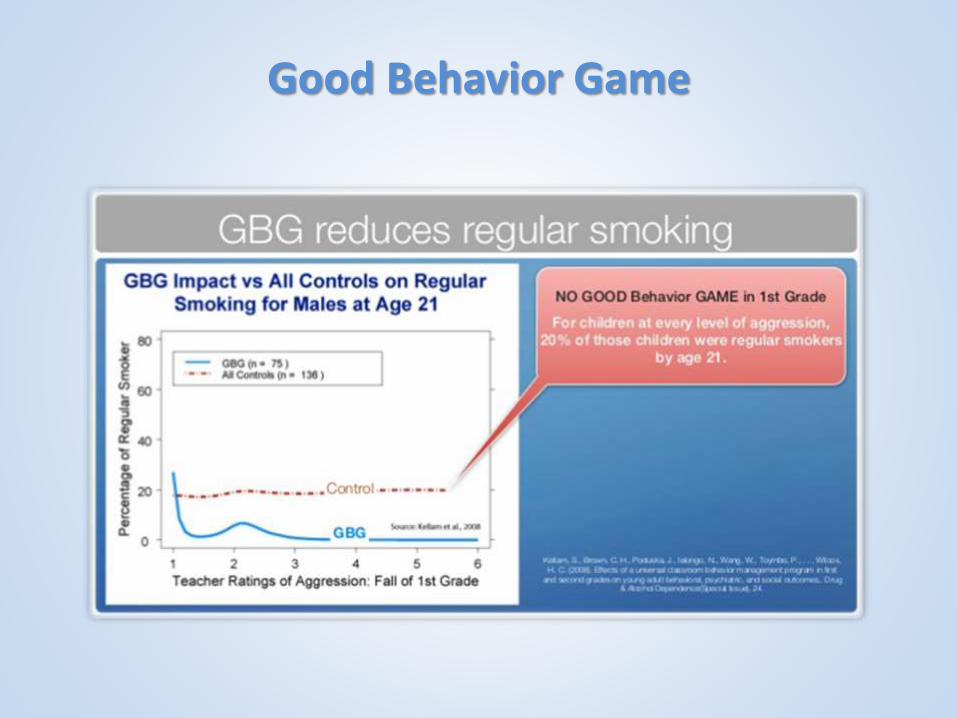
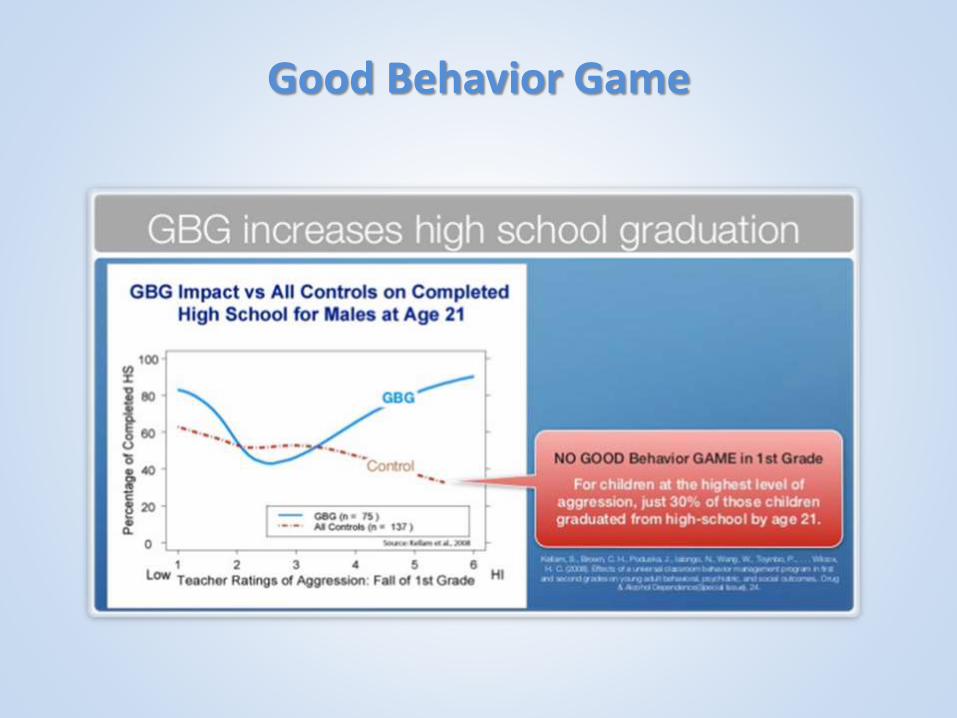
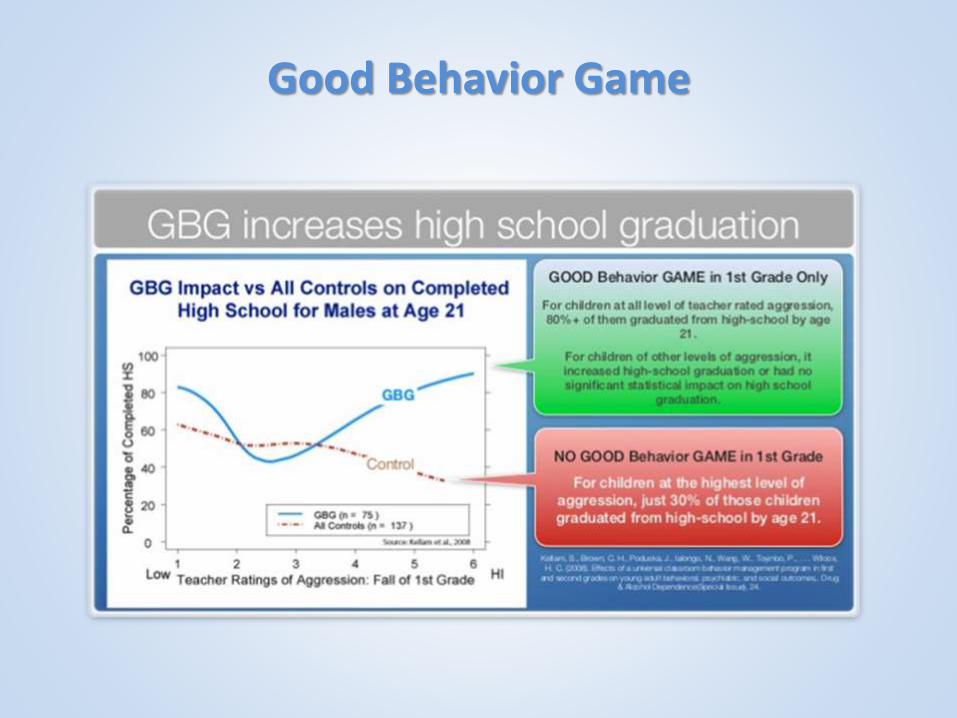
Good Behavior Game

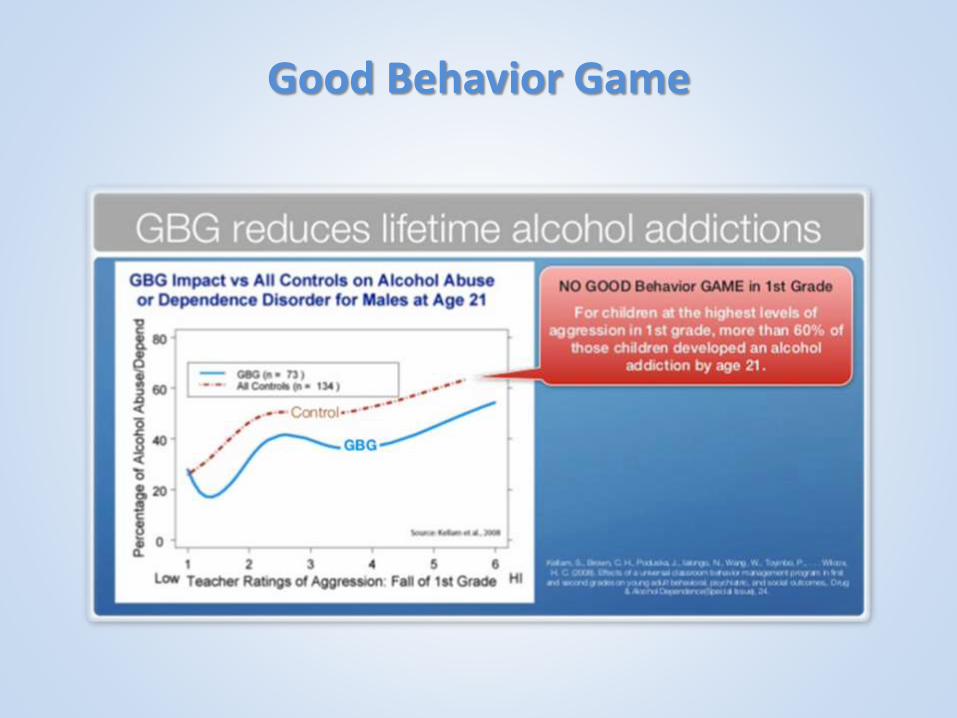
Good Behavior Game
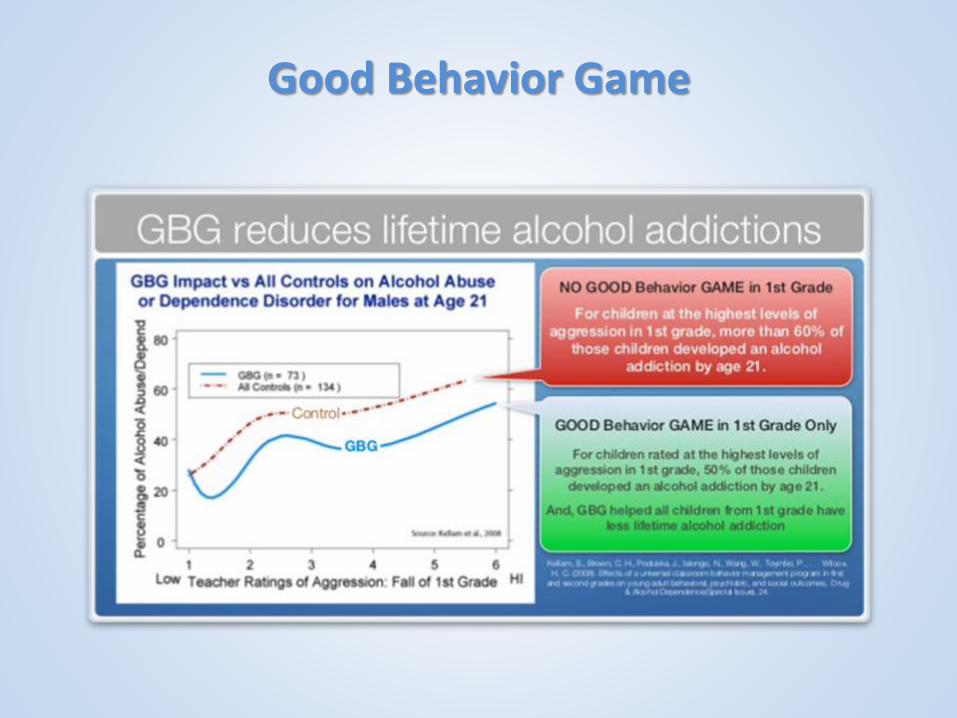
Good Behavior Game
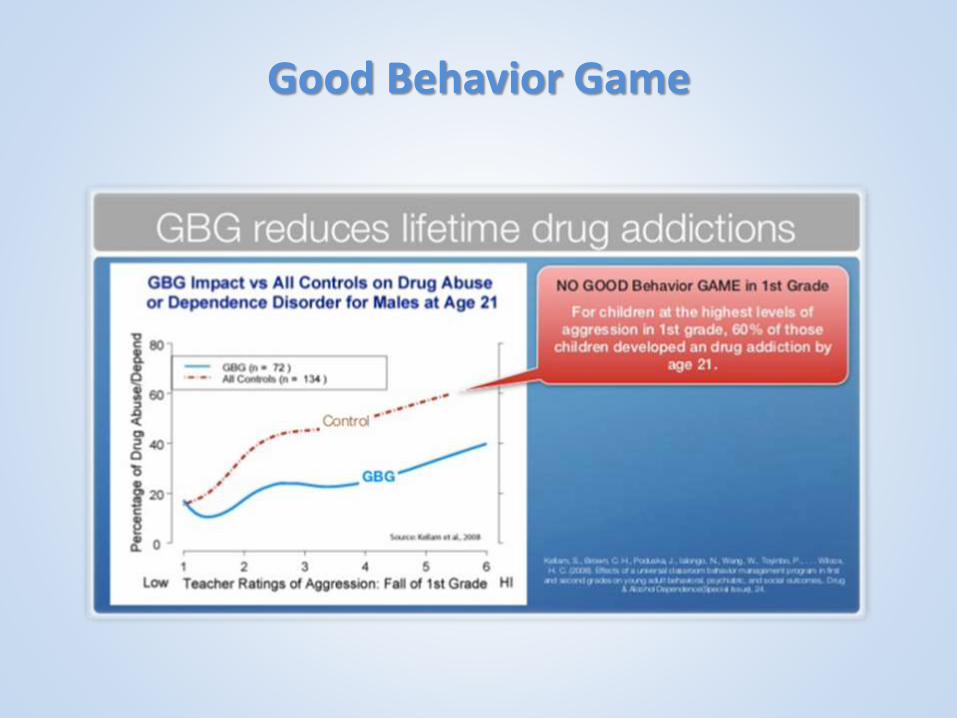
Good Behavior Game
Good Behavior Game

Good Behavior Game
Good Behavior Game

Good Behavior Game
Good Behavior Game

Good Behavior Game
Good Behavior Game
Good Behavior Game
Good Behavior Game
1. The class defines the “good” to be achieved = PAX
2. The class defines the “bad” to be reduced = Spleems
3. The teachers use kernels, like transitions, Beat the Timer and Prize Bowl to create a daily “game.”
4. Teacher forms 3-5 teams in the class (based on a formula).
5. A Spleem (a disturbing, disruptive, destructive or inattentive behavior) is counted against the team.
6. A game is played three (3) times per day for increasing number of minutes as successful. The games are played during demanding times for instruction.
7. Teams have a Win if the score three (3) or fewer Spleems.
8. The wins are reinforced by silly activities for a few seconds or minutes at most, based on Premack’s Principle
The Darrington Experience
• After seeing a presentation like this, a champion emerged at Darrington Elementary School. With her help, we identified the Good Behavior Game and Brain on the Ball as strategies that were a good fit for her classroom.
• Research shows the Good Behavior Game implemented in a 1st grade classroom for one school year produces:
• 60-90 minutes more time to teach and learn each day.
• 75-125 fewer disruptions per hour in classes.
• 20%-30% reduction in need for special education
The Darrington Experience
• The effects are even more profound over the lifetime of a Good Behavior Game participant:
• 50% - 70% reduction in mental health difficulties (e.g., ADHD and conduct symptoms).
• A 10% to 30% reduction injuries or stress related complaints.
• Reduction in directly observable symptoms of ADHD such as inattention and fidgeting, even for children not on medication.
• 30% to 60% reduction in referrals, suspensions or expulsions
• At age 13, reduced initiation of smoking by 26% and of hard drugs by more than 50%.
• At age 19, increased the likelihood of high school graduation by 21% and of college attendance by 62%.

Our Investment
• The County invested approximately $450 in Good Behavior Game manuals and materials.
• Teachers noticed immediate reductions in disruptions and increases in teaching time.
• Teachers implemented the Good Behavior Game in combination with another kernel – alternative seating strategy.
• They replaced all chairs in 1st – 3rd grade with therapy balls.
Our Investment
• Therapy balls were ordered to each student’s measurement, and had feet to prevent rolling or tip-overs.
Our Investment
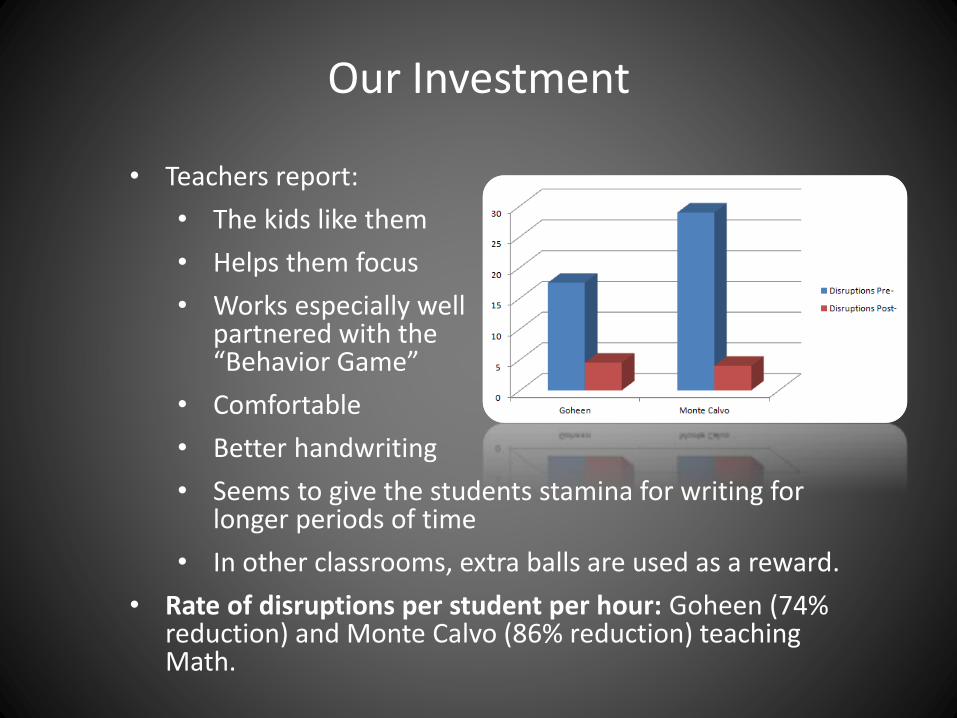
• Teachers report:
• The kids like them
• Helps them focus
• Works especially well partnered with the “Behavior Game”
• Comfortable
• Better handwriting
• Seems to give the students stamina for writing for longer periods of time
• In other classrooms, extra balls are used as a reward.
• Rate of disruptions per student per hour: Goheen (74% reduction) and Monte Calvo (86% reduction) teaching Math.




• Do we routinely screen for trauma exposure and related symptoms?
• Do we make resources available to youth, families, and providers on trauma exposure, its impact, and treatment?
• Do we engage in efforts to strengthen the resilience and protective factors of youth and families impacted by and vulnerable to trauma (think Kernels)?
• Do we address parent and caregiver trauma and its impact on the family system?
• Do we maintain an environment of care for staff that addresses, minimizes, and treats secondary traumatic stress, and that increases staff resilience?
Policy Discussion Questions