Embed Size (px)
Citation preview

Round window in Cochlear implant
10-4-201711.33 am

Helicotrema (at right angles to a line between the oval and round windows)

ROUND WINDOW MEMBRANE SO FAR NEGLECTED PART IN OTOLOGIC SURGERY
Surgeons, so far round window membrane is most neglected part in otological surgery endoscopic visualisation of RWM with 2.7 mm 45 degree scope gives more information
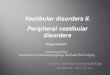
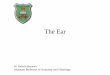
Dear surgeons,These are pictures of round window membrane RWM may be kidney shaped, round or triangular or oval or semilunar The thickness of membrane is 60 micro mm The length is 1.70 mm the width is 1.35 mm It contains all three layers like TMThe entrance of niche is 2.2 mm.

1 Round window membrane 2 Crista semilunaris 3 Fustis 4 Horizontal bar 5 cavum posterior 6 Cavum anterior 7 vertical
bar 8 Pars anterior 9 Pars posterior 10 Crista

1 Round window membrane 2 Crista semilunaris 3 Fustis 4 Horizontal bar 5 cavum posterior 6 Cavum anterior 7 vertical
bar 8 Pars anterior 9 Pars posterior 10 Crista

1 Round window membrane 2 Crista semilunaris 3 Fustis 4 Horizontal bar 5 cavum posterior 6 Cavum anterior 7 vertical
bar 8 Pars anterior 9 Pars posterior 10 Crista

1 Round window membrane 2 Crista semilunaris 3 Fustis 4 Horizontal bar 5 cavum posterior 6 Cavum anterior 7 vertical
bar 8 Pars anterior 9 Pars posterior 10 Crista

Surgical implications1) It is a outlet door of sound conduction through cochlea2) It acts as resonant chamber of sound3) Sono invertion - sound can be transported through the RWM and passing through cochlea and coming outfrom oval window gives rise to good hearing - reverse way4) It transports micromolecules to inner ear by eaither diffusion or pinocytosis5) For cochlear implant surgeons RWM is not directly posteroior to scala tympani So scala is present just antero superior to RWM hence surgeon has to remove crista to insert electrode directly in to scala tympani

• 6) Rwm is divided in to pars anterior and pars posterior by fibrous band arising from crista semilunaris The implant electrode shoud be introduced from pars anterior to enter the scala if electrode is introduced from pars posterior it touches osseous osseous spiral lamina and electrode does not go into scala.7) The floor of niche divided by horizontal bony bar and small vertical bar into cavum posterior and cavum anterior These bony cavums act like resonant spaces to outlet sound8) pars anterior always for sound vibration RWM vibration is evident at 1500 to 3000 hzs and at higher frequencies it vibrates irrigularly9) pars posterior is always tor micromolecules diffusion in to inner ear ant it contains more melanocytes so for gentamycin instillation it is better to place fluidIn posterior part of RWM for better diffusion10) Most of the round windows have false membranes hence it is better to remove those before instillation of gentamycin.

• 11) Micro molecules of 1mue easily passes through the RWM but micromolecules more than 3 mue can not pass through the membrane so surgeon during instillation of intratympanic gentamycin has to observe this point (not to add sodium bicarb in gentamycin solution )12) Rupture of RWM occur in pars anterior it looks like a slit with leak into cavum anticus and cavum posticus13) Cochlear aqueduct inner opening is present in scala tympani just anterior to crista semilunaris still inside is opening of cochlear vein so obstruction to cochlear vein causes sensory neural learing loss outer opening of cochlear aqueduct is present in pyramidal fossula14) Fustis gives strong support to RWM unnecessory excessive drilling of fustis in cholesteatoma surgery causes may accidentally rwm rupture.15) rupture of RWM is one of the causes for sudden SN loss

16)Fustis gives strong support to rwm unnecessory excessive drilling of fustis in cholesteatoma surgery causes may accidentally RWM rupture.17) Rupture of RWM is one of the causes for sudden sn loss18) Gentamycin trans tympanic instillation for menieres disease spreads from pars posterior of RWM to vestibule through the scala rather than diffusion through the helicotrema19) complete closure of round window is the good alternative treatment in SSCS (superior semicircularcanal fistula syndrome)20) The second most common site of otosclerosis is round window During stapes surgery it is better to visualise the round window for better results

Still experts opinion has to be taken regarding below line diagram - don’t take it granted – below line diagram is in the process of
developing
1. Round window membrane 2. Crista semilunaris3. Fibrous band
Crista semilunaris & fibrous band devides RWM into pars anterior & pars posterior
4. Horizontal bar5. Vertical bar
6. Cavum anterior 7. Cavum posterior
8. Fustis9. Opurculum or Crista











FUSTIS

FUSTIS•
it is fustis a solid bony column connecting the retrotympanum to round window niche. So far this structure is neglected Microscopically it may not be clearly visible, but endoscopically it is seen clearly The surgical implications of this structure are 1) its origin is pylogenically different from other parts of that area hence it behaves differently 2) It contains enzymes which are resistant to cholesteatoma destruction 3) it prevents sinus cholesteatoma extending downwards..4) This structure is directed towards round window, in narrow round window niche by following its upper border, we can identify the round window membrane 5) It divides upper part of subtympanic sinus, concomerata into medialis and lateralis. C medialis is site for posterior ampullary nerve section. 6) Fustis regulates smooth out flow of sound waves from round window membrane.

• 7) It helps in creation of pressure difference between round and oval windows encourages acoustic coupling. 8) It gives support round window niche because both postis anticus and postis posticus contains cochlea and subcochlear portion that are hollow structures. 9) This structure modulates according to round window niche i. e, "V" shaped, square shaped, triangular gothic shaped, like that, to have a relation with RW10) In absent sibiculum, the fustis gives support.11) Fustis narrows the round window niche there by protects the round window membrane (rupture)normally. 12) embryologically fustis develops between periosteal layer of the labyrinthine capsule and the thin smooth plate of Pavementum Pyramidalis and it is ontogenically important structure. So surgeons, fustis is very important structure at outflow gate of sound in middle ear. In 1968 Bruce Proctor mentioned, Recently prof Presutti, Prof Marchioni and Prof Joao F Nogueira described this part. so surgeons please look this important but poor part while performing surgeries because it is present in all middle ears..





Type A fustis. f fustis, sp styloid proeminence, st scala tympani, rw round
window

Type B fustis. f fustis, sp styloid proeminence, st scala tympani, rw round
window

Right ear. Endoscopic view of fustis type B. ow oval window, st scala tympani, fu fustis, pe pyramidal
eminence, rw round window

Right ear. The tool shows the scala tympani. ow oval window, st scala tympani, fu fustis, rw round window

A. Original round window. B. Basilar membrane. C. Osseous spiral lamina. D. Reflection of perilymphatic fluid. E. Darker area of first curve of the basal turn
of the scala tympani. F. Blood vessels. G. Modiolus. H. Removed bone of round window overhang.

SCC = Sub Cochlear Canaliculus,

Between the fustis and the finiculus a subcochlear canaliculus is often seen, which is a tunnel that connects the round window chamber with the petrous apex via a series of
pneumatized cells.
Right ear. Endoscopic anatomy of inferior retrotympanum. fu fustis, t tegmen, pp posterior pillar, f finiculus, j jacobson’s nerve

Right ear. Endoscopic anatomy of the retrotympanum during dissection for acustic neuroma surgery.
fu fustis, fn facial nerve, ow oval window, pr promontory, scc subcochlear canaliculus, et Eustachian tube

Right ear. Endoscopic dissection during surgery, after drilling the promontory. ow oval window, st scala tympani, scc subcochlear
canaliculus

Subcochlear canaliculus type A

Subcochlear canaliculus type B

Subcochlear canaliculus type C

Round window

• So far round window is neglected part in middle ear Now a days it is gaining popularity For type4 and 5 t plasties sono inversion techniques viroplasties gentamycin and other chemical perfusions cochlear implant insertions corticosteroid perfusions in s n d skullbase approaches round window is important There are so many verieties of shapes of r w s I have previously discussed 4 types of r w s

" High arched" round window

" High arched" round window• Dear surgeons it is" High arched" round window it is
present 1-3%of cases you can compare this window to normal r w which is shown here The arched round window associated with1 compressed cochlear capsule in caratico facial angle2 Deep hypotympanum3 long trabiculae including trabicula longa4 wide concomerata lateralis and absent concomireta medialisWide postis posticus with subcochlear tunnel5 wide sinus tympani



"PARABOLIC" round window

"PARABOLIC" round window
• Dear surgeons it is "PARABOLIC" round window in shape present 1% of cases characterised by 1 two vertical limbs longer than tegmen2 wide niche3 Third limb is formed by styloid complex4 s shaped cochlea including sub vestibular portion5 wide finiculus with high pavementum pyramidalis6 deep carotid recess7 3rd part of facial nerve is nearer to middle ear

• Surgical implications1 wide angle cochlea hence cochlear implant electrode insertion is easy2 narrow vestbular window stapes surgery is difficult3 endoscopic endomeatal f n decompression is easy in these cases4 vibroplasty is easy5 infracochlear approach to petrous apex is not possible in this type of round windows6 endoscopic endomeatal approach to IAC is easy in this type of cases7 s shaped cochlea here allows wide transcochlear approach to clivus





Middle turn cochleostomy

PARISIER'S TRIANGLE (DANGEROUS TRIANGLE)

PARISIER'S TRIANGLE (DANGEROUS TRIANGLE)
Perisier's triangle is very important triangle in endoscopic ear surgery1) Superior limb is formed by inferior part of HFN 2) The apex is formed by the geniculate ganglion
3) The base is formed by the anterior commissure (end) of oval window 4) Inferior limb is formed by tunning point of jocobson's nerve to the the
geniculate ganglion.

• The surgical implications are
1) This triangle contains labyrinthine part of FN. 2) During transotic or transcochlear approaches surgeon should respect this triangle and drill carefully to avoid injury to FN. 3) Clinically labyrinthine part consists of two segments a meatal segment of nerve, labyrinthine part of nerve. total length of this nerve is 3 to 5 mm. Anteriorly we can see these parts clearly through this triangle. 4) 1st part of FN passes close to lower border of precochlear HFN towards anterior end of oval window in this triangle. 5) Irregular drilling of cochlea in this triangle damages FN That is why it is called DANGERS TRIANGLE. 6) During trans meatal endoscopic dissection of IAC, this triangle important for identification of nerves7) Translabyrinthine approach visualises posterior surface of 1st part of FN, in transcochlear approaches the anterior surface of the nerve is exposed. In transottic approaches 270 to 320 degrees of 1 st part of FN is exposed. 8)Observe closely the labyrinthine part of FN there is a constriction of labyrinthine segment and meatal segment. Facial nerve key points1) Facial nerve changes direction 5 times during its course from brain stem to styloid foramen. 2) No other nerve in body covers such a long distance in bony canal3) facial nerve contains 10000 axons that are responsible for the innervation of the face musculature and also for the communications with other nerves human body4) work with injured facial nerve requires lot of patience.

• RULE OF 2 IN TEMPORAL BONES1) The diameter of geniculate fossa is 2 mm2) The distance between between geniculate fossa to anterior wall of vestibule is 2 mm3) The thickness of geniculate crest is 2 mm4 ) The diameter of horizontal facial nerve in that area is 2 mmHence while drilling the bone or curetting the bone at perigeniculate area it is not advisable to use bigger burs more than 2mm diameter5) The meatal segment of facial nerve is usually 2 mm anterior and superior to superior vestibular nerve.My special thanks to prof Livio presuitti, prof Daniele Marchioni and prof Jao Flavio Nogueira who taught me this Anatomy






While making middle turn cochleostomy we shouldn’t injure the labyrinthine part of facial nerve present in
perisier’s triangle

Notch 2 to 3 mm anterior to OW & below the processes cochleriformis leads to middle turn


For middle turn cochleostomy also we need to drill a lot . Not opening that much easily

Still not opened .

Still not opened .

Still not opened .

Now opened .
In middle & apical turns SV is more than ST ……I don't know why

See how depth the middle turn cochleostomy

See how depth the middle turn cochleostomy

All opening from above 1. OW 2. Middle turn cochleostomy 3. SV cochleostomy 4.Superior cochleostomy 5. RW 6.INFERIOR
cochleostomy