Embed Size (px)
Citation preview

Sepsis and Septic Shock
Akram M Fayed, MD, ABIM
Lecturer, Department of Critical Care Medicine Faculty of Medicine
University of Alexandria
Pharmacotherapy 2008. S. LENA KANG-BIRKEN AND JOSEPH T. DIPIRO

Prevalence and Incidence
Sepsis represents a significant burden to the national health caresystem
In 2000, sepsis affected approximately 660,000 people, anincrease of 8.7 % per year since 1979
More than one-half of the patients were admitted to the ICU with amean length of stay of 15.7 days

Prevalence and Incidence
The total number of deaths increased from 21.9 per 100,000population in 1979 to 43.9 per 100,000 populations in 2000
With the annual cost of approximately $16.7 billion, there remains a vital need for clinicians to comprehend the pathophysiology and toappreciate the management options available for acutely ill patientswith sepsis or septic shock

Definition
The criteria for the new terms provide specific physiologic variablesthat can be used to categorize a patient as having:
-Bacteremia, - Systemic inflammatory response syndrome (SIRS), - sepsis, - severe sepsis, - septic shock, or - multiple-organ dysfunction syndrome (MODS),
Suggesting an important continuum of progressive physiologic decline

Definition

Definition
Introduction of the term SIRS reflects the knowledge that aphysiologically similar systemic inflammatory response can be seeneven in the absence of identifiable infection
Severe sepsis refers to patients with an acute organ dysfunction suchas acute renal failure or respiratory failure
These patients have a mortality rate of approximately 40%

Definition
Septic shock refers to sepsis patients with arterial hypotension thatis refractory to adequate fluid resuscitation, thus requiring vasopressoradministration
These patients usually require intensive care and ultimately die in 50% to 80% of cases
It is important to note that progression from sepsis to MODS can occur in the absence of an intervening period of septic shock

Definition

INFECTION SITES AND PATHOGENS
The leading primary sites of microbiologically documented infectionsthat led to sepsis were:- The respiratory tract (21%–68%), - Intraabdominal space (14%–22%), and - Urinary tract (14%–18%)
Although almost any microorganism can be associated with sepsisand septic shock, the most common etiologic pathogens are: - Gram-positive bacteria (40% of patients), followed by - Gram-negative bacteria (38%) and - Fungi (17%)
Certain viruses and rickettsiae can produce a similar syndrome

GRAM-POSITIVE BACTERIAL SEPSIS
Since 1987, gram-positive organisms are the predominant Pathogens in sepsis and septic shock, accounting for approximately40% to 50% of all cases
They are commonly caused by:- Staphylococcus aureus, - Streptococcus pneumoniae, - Coagulase-negative staphylococci,and - Enterococcus species.
Streptococcus pyogenes and viridans streptococci are lesscommonly involved

GRAM-NEGATIVE BACTERIAL SEPSIS
A greater proportion of patients with gram-negative bacteremiadevelop clinical sepsis, and gram-negative bacteria are also morelikely to produce septic shock in comparison to gram-positive organisms, 50% versus 25%, respectively
Gram-negative sepsis also results in a higher mortality rate compared with sepsis from any other groups of organisms
The major factor associated with the outcome of gram-negativesepsis appears to be the severity of any underlying condition

GRAM-NEGATIVE BACTERIAL SEPSIS
Patients with rapidly fatal conditions, such as acute leukemia, aplastic anemia, and >70% of the body’s surface burn injury, have asignificantly worse prognosis than do those patients with nonfatal underlying conditions, such as diabetes mellitus or chronic renal Insufficiency
Escherichia coli and Pseudomonas aeruginosa are the most Commonly isolated gram-negative microorganisms in sepsis

GRAM-NEGATIVE BACTERIAL SEPSIS
Other common gram-negative pathogens include:
- Klebsiella species, - Serratia species, - Enterobacter species, and - Proteus species
P. aeruginosa, although not considered a predominant endogenous flora, is found widely in the environment and is the most frequent causeof sepsis fatality

ANAEROBIC AND MISCELLANEOUS BACTERIAL SEPSIS
Anaerobes are usually considered low-risk organisms for the development of sepsis
If present, anaerobes are often found together with other pathogenicbacteria that are commonly found in sepsis
Epidemiology reports suggested that polymicrobial infections accounted for 5% to 39% of sepsis

ANAEROBIC AND MISCELLANEOUS BACTERIAL SEPSIS
Mortality rates associated with polymicrobial infections are similar to sepsis caused by a single organism
Although some clinicians believe the particular combination oforganisms present in polymicrobial sepsis can provide clues to thesource of infection, no clear source for the infection can be identifiedin up to 25% of cases

FUNGAL SEPSIS
The rate of fungal infections increased more than 200% from1979 to 2000
Candida species are common causes of fungal sepsisin hospitalized patients
Although Candida albicans remains the most dominant species, non-albicans Candida species, particularly Candida glabrata, Candida parapsilosis, Candida tropicalis, and Candida krusei, have graduallyemerged from 24% in the 1980s to 46% during 1997 to 2000

CELLULAR COMPONENTS FOR INITIATING THE INFLAMMATORY PROCESS

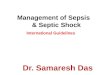
PRO- AND ANTIINFLAMMATORY MEDIATORS
The balance between pro- and antiinflammatory mediators
(CARS, compensatory antiinflammatory response syndrome; IL, interleukin; IL-1RA, interleukin-1 receptor antagonist; SIRS, systemic inflammatory response syndrome; TNF-α , tumor necrosisfactor-α.)

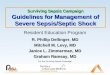
PRO- AND ANTIINFLAMMATORY MEDIATORS
Cascades of sepsis

COMPLICATIONS
DISSEMINATED INTRAVASCULAR COAGULATION
ACUTE RESPIRATORY DISTRESS SYNDROME
HEMODYNAMIC EFFECTS
ACUTE RENAL FAILURE

CLINICAL PRESENTATION

PROGNOSIS
As the patient progresses from SIRS to sepsis to severe sepsis toseptic shock, mortality increases in a stepwise fashion
Mortality rates are higher for patients with advanced age, preexistingdisease including chronic obstructive pulmonary disease, neoplasm, and human immunodeficiency virus (HIV) disease, ICU care, more organfailure, positive blood cultures, and Pseudomonas species infection
Mortality increased with age from 10% in children to 38.4% in those ≥85 years

PROGNOSIS
ICU admission was required in 51.1% of the patients with severe sepsis and of those patients, mortality was reported in 34.1%
Mortality from severe sepsis and MODS is most closely related to thenumber of dysfunctioning organs
As the number of failing organs increased from two to five, mortalityincreased from 54% to 100%
Duration of organ dysfunction can also affect the overall mortality rate

PROGNOSIS

PROGNOSIS
An elevated lactate concentration of >4 mmol/L in the presenceof the SIRS significantly increases intensive care unit admissionrates, and persistent elevations in lactate for more than 24 hoursare associated with a mortality rate as high as 89%
Inversely, patients with higher lactate clearance after 6 hours ofEmergency Department intervention have improved outcome compared with those lower lactate clearance
There was an approximately 11% decrease likelihood of mortality for each 10% increase in lactate clearance

TREATMENT

TREATMENT

EARLY GOAL-DIRECTED THERAPY
Initial resuscitation of a patient in severe sepsis or sepsis-inducedtissue hypoperfusion should begin as soon as the syndrome isrecognized
A randomized, controlled trial evaluated the timing of the goal-directed therapy involving adjustments of cardiac preload, afterload, and contractility to balance oxygen delivery with demandprior to admission to the ICU

EARLY GOAL-DIRECTED THERAPY
The goals during the first 6 hours included:
- Central venous pressure of 8 to 12 mm Hg, - Mean arterial pressure of ≥65 mm Hg, - Urine output of ≥0.5 mL/kg/h, and - A central venous or mixed venous oxygen saturation of ≥70%
During the first 6 hours of resuscitation, the early goal-directed therapygroup had a central venous catheter placed and received more fluidthan with traditional therapy (5 versus 3.5 L), dobutamine therapy toa maximum of 20 mcg/kg/min, and red blood cell transfusions

EARLY GOAL-DIRECTED THERAPY
The 28-day mortality rate was 30% in the early goal-directed therapygroup, in comparison to 46.5% in the traditional therapy groupconsisting of fluid resuscitation, followed by vasopressor therapy ifrequired
Increased oxygen delivery from the red blood cell transfusionsto achieve a hematocrit of ≥30% in the early goal-directed therapy group appeared to be the primary difference between the two groups

EARLY GOAL-DIRECTED THERAPY
One institution evaluated the impact of 6-hour sepsis care bundle and found the compliance rate to be 52%
The noncompliant group had a more than twofold increase in hospitalmortality in comparison to the compliant group (49% vs. 23%)

Thank You