Embed Size (px)
Citation preview
MANDIBULAR SPACE INFECTIONS &
COMPLICATIONS
Submitted by
Geetha R
Final Year BDS part II
KANNUR DENTAL COLLEGE
Department of Oral & Maxillofacial Surgery
CONTENTS
INTRODUCTION
Odontogenic infections are among the most frequently encountered infections affecting humans. In majority of cases, these infections are minor and resolve either by spontaneous drainage through the gingival tissues of the tooth or by extraction of the offending tooth.
Chronic sinus tracts from the apex of the tooth to the surface mucosa or skin are not uncommon in populations who receive little or no dental care.
A great deal of pain and suffering accompany establishment of these draining sinus tracts. Removal of the offending tooth almost always results in rapid resolution of the infection, even with antibiotic therapy. Unfortunately, these minor tooth-related infections occasionally become serious and life-threatening. Aggressive surgical and medical care is necessary to prevent disastrous results.
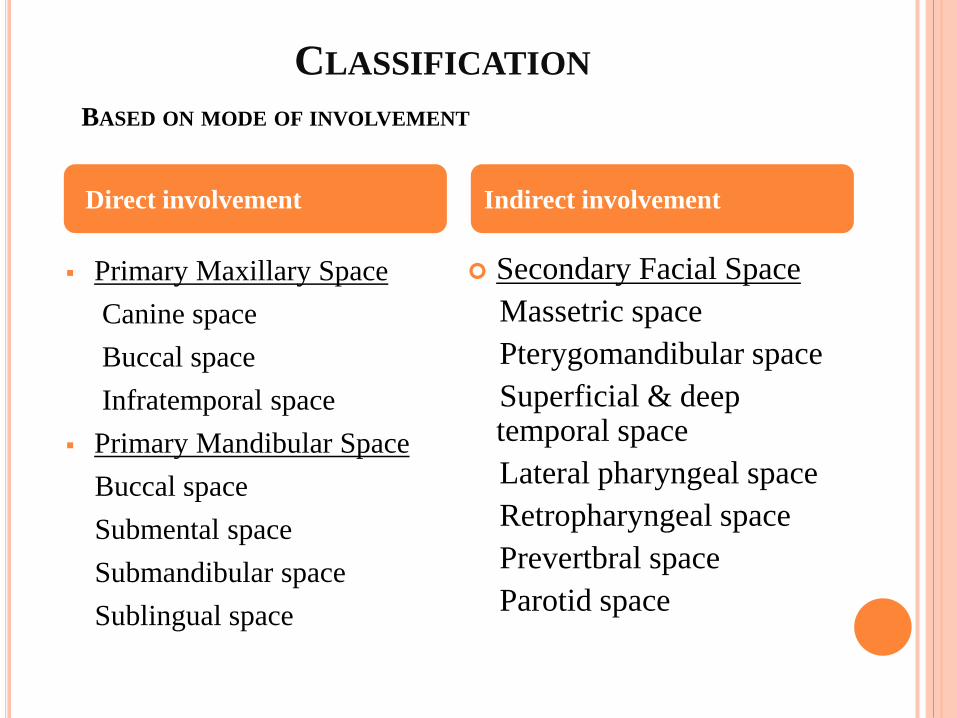
CLASSIFICATION
BASED ON MODE OF INVOLVEMENT
Primary Maxillary Space
Canine space
Buccal space
Infratemporal space
Primary Mandibular Space
Buccal space
Submental space
Submandibular space
Sublingual space
Secondary Facial Space
Massetric space
Pterygomandibular space
Superficial & deep temporal space
Lateral pharyngeal space
Retropharyngeal space
Prevertbral space
Parotid space
Direct involvement Indirect involvement
MANDIBULAR SPACES
Infection may erode from mandibular teeth into a variety
of spaces, in addition to the usual vestibular abscess.
The three primary spaces are the submental,
sublingual,and submandibular spaces; the three
secondary spaces are the pterygomandibular, masseteric,
and temporal spaces.
The primary spaces are those into which infection
spreads directly from the teeth and bone.
SUBMENTAL SPACE
Etiology
1. Infection from anterior mandibular teeth.
2. Spread of infections from lower lip, skin around
cheek, floor of mouth , tip of tongue & sublingual
tissues
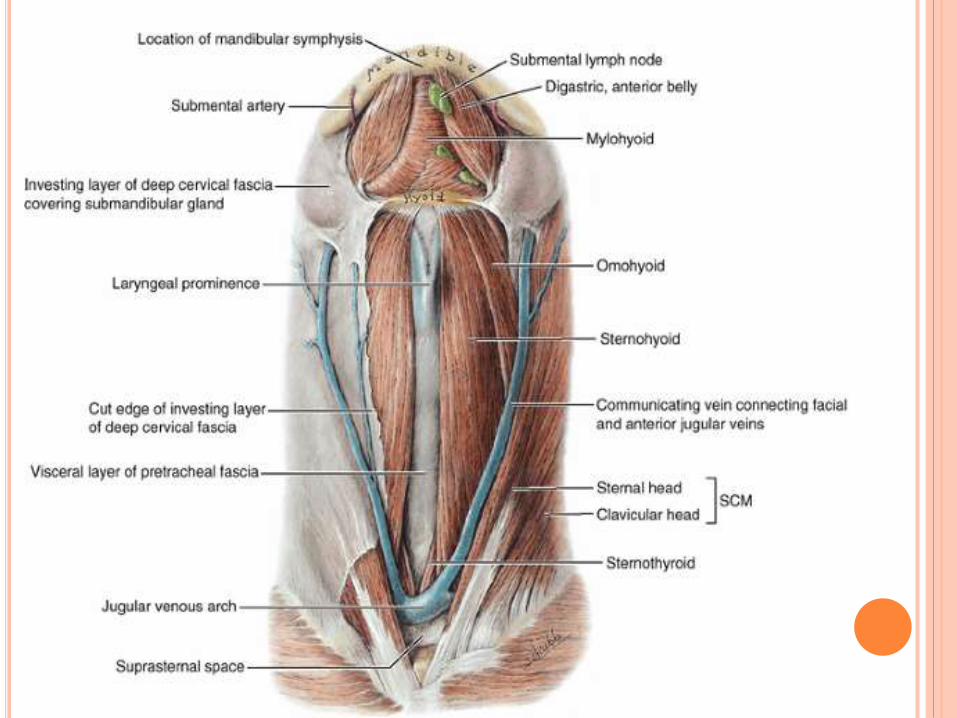
SURGICAL ANATOMY
Boundaries
Deep or Lateral : Anterior belly of digastric
Superficial or medial : Investing layer of deep
cervical fascia
Superior : Mylohyoid muscle
Inferior : Investing layer of deep cervical fascia
Anterior : Inferior border of mandible
Posterior : Hyoid bone
Contents
Submental lymph nodes & anterior juglar vein
CLINICAL FEATURES
Extraoral findings
Distinct, firm swelling in midline, beneath the chin. Skin
overlying the swelling is board like and taut. Fluctuation
may be present.
Intraoral findings
The anterior teeth, are either non-vital, fractured or
carious. The offending tooth may exhibit tenderness to
percussion and may show mobility. The patient may
experience considerable discomfort on swallowing.

INCISION & DRAINAGE
Transverse incision placed in skin below symphysis
of mandible.Blunt dissection done with kelly’s
forceps or sinus forceps

SPREAD
Infection can extend
a) Posteriorly, to submandibular space
b) Dicharge of contents in submental region in face
SUBLINGUAL AND SUBMANDIBULAR SPACES
The sublingual and submandibular spaces exit on
the medial aspect of the mandible.They are usually
involved by lingual perforation of infection from the
mandibular molars. The factor determining whether
the infection is in the sublingual or submandibular
space is the relationship between the area of the
infection's perforation and the location of the
mylohyoid muscle's attachment .
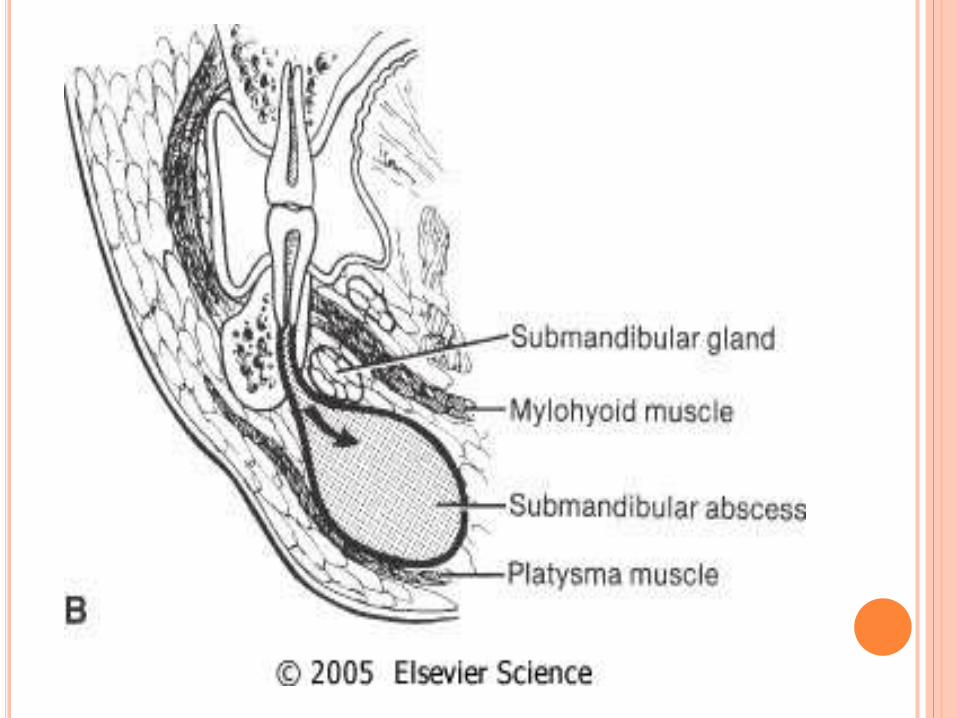
SUBMANDIBULAR SPACE
If the apex of the tooth is inferior to the muscle (third
molar) , the submandibular space is involved.
Etiology
1.Infection of mandibular molars
2.Infection from submandibular salivary gland
3.Infection from submental space
4.Infection from sublingual space
5.Infection from tongue , floor of mouth & cheek.
SURGICAL ANATOMY
Anteromedially :mylohyoid muscle
Posteromedially: hyoglossus muscle
Superolaterally : medial surface of mandible
Anteroinferiorly : anterior belly of digastric
Posteroinferiorly : posterior belly of digastric,
stylohyoid & stylopharyngeus muscle
Superficial: platysma & skin
Deep : Mylohyoid ,hyoglossus & superior
constrictor
Contents : superficial lobe of submandibular
salivary gland & lymph nodes , facial artery & vein
CLINICAL FEATURES
Extraoral
(i) Firm swelling in submandibular region, below the
inferior border of mandible.
(ii) Generalized constitutional symptoms
(iii) Some degree of tenderness
(iv) Redness of overlying skin.
Intraoral
(i) Teeth are sensitive to percussion
(ii) Mobile
(iii) Dysphagia
(vi) Trismus.

INCISION & DRAINAGE
Incision of about 1.5 to 2 cm in length is made 2 cm
below lower border of mandible. Skin & subcutaneous
tissue are incised .A sinus forceps is inserted through
incision superiorly & posteriorly on lingual side to
mandible to drain pus. Rubber drain is placed & secured
with sutures.

SPREAD
Involve contralateral submandibular space
Involve submental space
Involve sublingual space
Involve parapharyngeal space
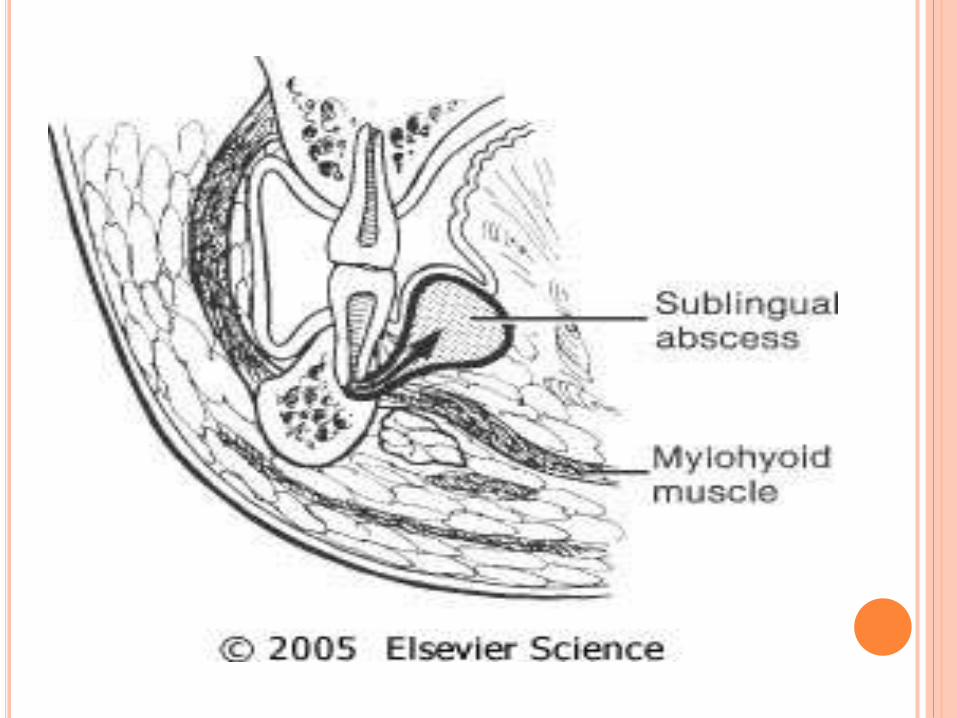
SUBLINGUAL SPACE
Submandibular and sublingual spaces surgically distinct, but
should be considered as surgical unit due to proximity and
frequent dual involvement in odontogenic infections.
Etiology
1. Infected premolar and 1st molar teeth frequently drain into this space due to their root apices existing superior to the mylohyoid muscle
SURGICAL ANATOMY
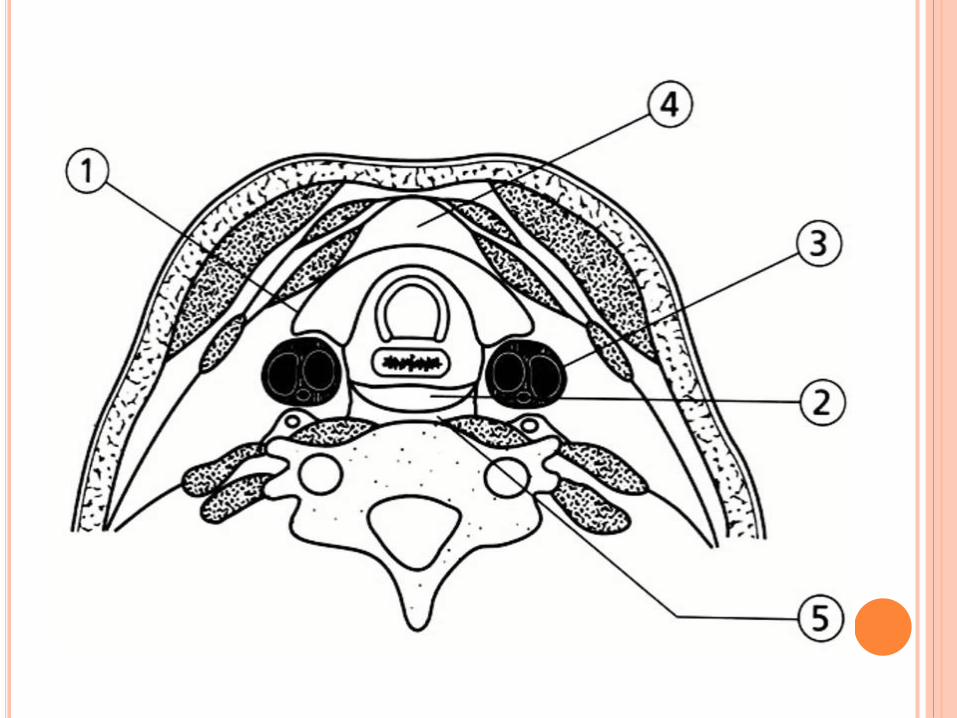
Boundaries
1. Inferiorly : Mylohyoid muscle
2. Laterally : Medial surface of mandible
3. Medially : Hyolglossus, genioglossus & geniohyoid
4. Posteriorly : Submandibular space
5. Laterally & inferiorly : Mylohyoid muscle & lingual side of mandible
Contents
Geniohyoid & genioglossus muscle , hyoglossusmuscle ,submandibular & sublingual salivary gland,
lingual & hypoglossal nerve.
CLINICAL FEATURES
Extraoral : There is little or no swelling. The lymph
nodes may be enlarged and tender. Pain and discomfort
on deglutition. Speech may be affected.
Intraoral : Firm, painful swelling seen in the floor of the
mouth on the affected side. The floor of the mouth is
raised. The tongue may be pushed superiorly.

INCISION AND DRAINAGE
Intraorally : an incision is made close to the ligual
cortical plate lateral to the sublingual plica, as the
important structure at this site is the sublingual nerve.
Extraorally : When both the submental and sublingual
spaces contain pus, they can be drained via a skin
incision placed in the submental region, pushing a closed
sinus forceps through the mylohyoid muscle.
SPREAD
Infection can spread to contralateral side
Infection can spread to submandibular,
pterygomandibular & parapharyngeal space
Infection can spread to submental or
submandibular lymph nodes
Infection spread through aperatures of perforating
arteries into submental space
SECONDARY SPACES
The three secondary spaces of the mandible are
posterior to the tooth-bearing portion of the
mandible in the angle-ramus area. They are called
secondary spaces because they become infected
by secondary spread of infection from other anterior
spaces. The primary spaces feeding them are the
buccal, sublingual, and submandibular spaces.
MASSETERIC
The masseteric space exists between the lateral
aspect of the mandible and the masseter muscle.
This space is involved most often by spread from
the buccal space or from soft tissue infection
around the third molar. When it is involved, the
posteroinferior portion of the face swells.
In addition to the swelling, the patient has mild to
moderate trismus caused by inflammation of the
masseter muscle.
ETIOLOGY
Infection of third molar
Infection from fracture of angle of mandible
SURGICAL ANATOMY
Boundaries
Anterior : Anterior border of masseter & buccinator
Posterior : Parotid gland
Superior : Zygomatic arch
Inferior : Inferior border of mandible
Medial : Lateral surface of ramus
Lateral : Medial surface of masseter
Contents
Massetric nerve , superficial temporal artery &
transverse facial artery

CLINICAL FEATURES
INCISION & DRAINAGE
PTERYGOMANDIBULAR SPACE
The pterygomandibular space lies between the
medial aspect of the mandible and the medial
pterygoid muscle.
Etiology
1.This space becomes involved from spread from the
sublingual and submandibular spaces and from soft
tissue infection around the third molar(pericoronitis)
2.Use of contaminated needle for inferior alveolar
nerve block
3.Infection can arise from maxillary third molar from
posterior superior alveolar nerve block injection
SURGICAL ANATOMY
Boundaries
Lateral : Ramus of mandible.
Medial : Medial pterygoid muscle.
Posterior : Parotid gland
Anterior : Pterygomandibular raphae.
Contents : Lingual nerve,
Mandibular nerve,
Inferior alveolar,
Mandibular artery.
Mylohyoid nerve and vessels.
Loose areolar connective tissue.
CLINICAL FEATURES
Severe degree of limitation of mouth opening.
Tenderness over the area of swollen soft tissues medial to
anterior border of ramus.
Dysphagia is present.
Medial displacemnet of lateral wall of the pharynx.
Redness and edema of the area around the third molar.
Midline of the palate is displaced to the unaffected side.
Uvula is swollen.
Difficulty in breathing.

INCISION & DRAINAGE
Intraoral : A vertical incision, approximately 1.5 cm in length, is made on the anterior and medial aspect of the ramus of mandible. A sinus forceps in inserted in the abscess cavity, opened and closed & withdrawn. The pus is evacuated, a rubber drain is introduced and is secured in position with a suture.
Extraoral : An incision is taken in the skin below the angle of the mandible. A sinus forceps is inserted towards the medial side of the ramus in an upward and backward direction. Pus is evacuated and the drain inserted from an intraoral approach and sutured in position.
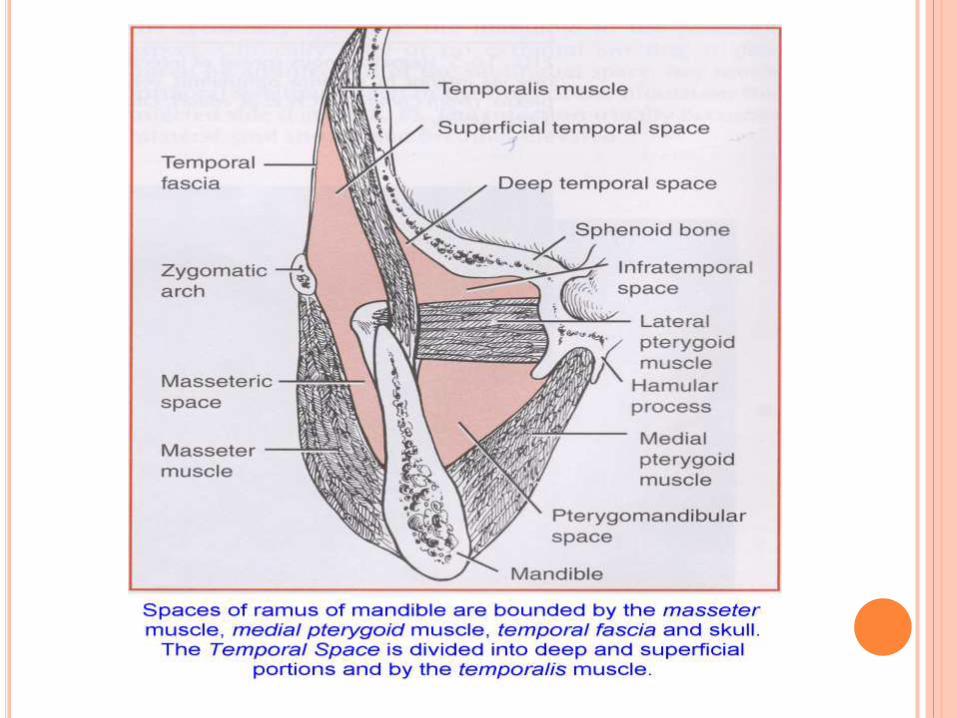
MASTICATOR SPACES
Masseteric, pterygomandibular, and temporal spaces
spaces are collectively known as the masticator space,
since they are bounded by the muscles of mastication:
masseter, medial pterygoid, and temporalis.
The three individual spaces communicate freely with one
another and are simultaneously involved
.If all three of the primary mandibular spaces become involved with the infection, the infection is known as Ludwig's angina. Ludwig's angina, described in 1936, was a relatively common occurrence until the antibiotic era. It is a rapid, bilaterally spreading, gangrenous cellulitis of the submandibular, sublingual, and submental spaces. It usually spreads posteriorly to the secondary spaces as well. It produces gross swelling, elevation and displacement of the tongue, and tense, brawny induration of the submandibular region superior to the hyoid bone. There is usually little or no fluctuance (Finch et al, 1980; Patterson et al, 1982). The patient experiences severe trismus, drooling of saliva, tachypnea, and dyspnea. Impending compromise of the airway produces marked anxiety. The cellulitis can progress with alarming speed, producing an upper airway obstruction that may lead to death. The usual cause of Ludwig's angina is an odontogenicinfection, usually from the mandibular second or third molar. The microbes involved are usually Streptococcus, oral anaerobes, or both.
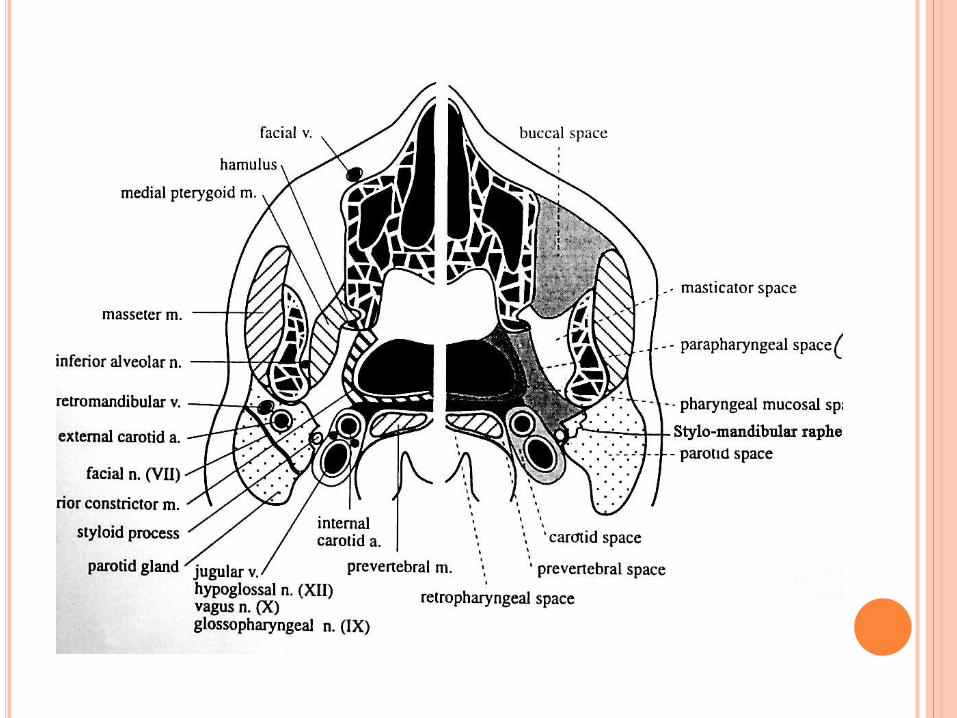
CERVICAL (DEEP NECK) SPACES
CERVICAL (DEEP NECK) SPACES
Extension of odontogenic infection beyond the mandibularspaces is an unusual event.
When it does occur, spread to the cervical or deep neck spaces from the submandibular, sublingual, or pterygomandibularspaces may have serious, life-threatening sequelae. These sequelae may result of complications, such as upper airway obstruction or mediastinitis.
Odontogenic infections cause as much as 30% of all deep neck infections (Virolainen et al, 1979).
The deep neck spaces have a variety of names and descriptions.Three are relatively consistent through the literature: the lateral pharyngeal space, the retropharyngeal space, and the prevertebral space, or danger space No, 4.
The layers of deep cervical fascia form and bind these three spaces.
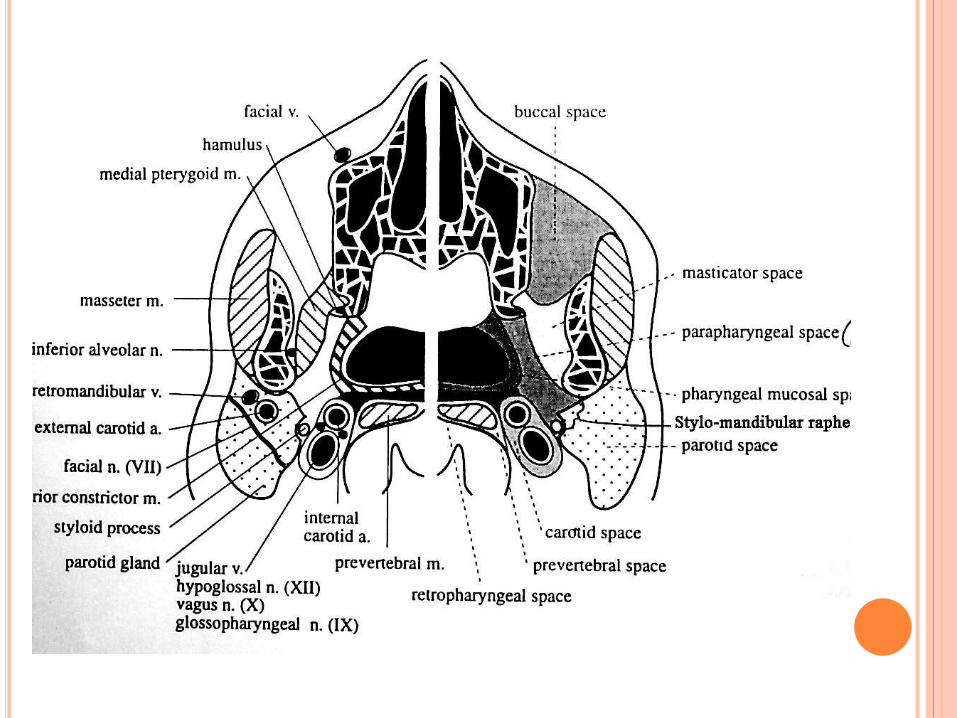
LATERAL PHARYNGEAL SPACE
The lateral pharyngeal space is classically described as having the shape of an inverted pyramid or funnel.
Etiology
Infection from third molars
Tonsillar infection in neighbouring spaces
Surgical Anatomy
Superior : Skull base at the sphenoid bone
Inferior : Hyoid bone.
Lateral : Medial pterygoid muscle
Medial : Superior & middle pharyngeal constrictor muscle
Anterior : Pterygomandibular raphe
Posterior : Carotid sheath & scalena fascia
Contents : Carotid artery , Internal juglar vein, Vagusnerve, Cervical sympathetic chain
LATERAL PHARYNGEAL SPACE
Around the boundary is pterygomandibular raphe, it
communicates with the spaces of the mandible.
Posteromedially it extends to and is bounded by the
prevertebral fascia and communicates freely with the
retropharyngeal space.
The styloid process and associated muscles and fascia
divide the lateral pharyngeal space into an anterior
compartment, which contains muscles, and a posterior
compartment, which contains the carotid sheath and
cranial nerves
CLINICAL FEATURES
Severe trismus
Lateral swelling of the neck
Bulging of the lateral pharyngeal wall
Rapid progression of infection in this space is common
Posterior compartment involvement can result in thrombosis of the internal jugular vein, erosion of the carotid artery or its branches, and interference with cranial nerves IX to XII
INCISION & DRAINAGE
Extraoral approach
An incision is made along the anterior border of sternocleidomastoid muscle, extending from below the angle of the mandible, to the middle third of submandibular gland.
The fascia behind the gland is incised and a curved hemostat is inserted and carefully directed medially behind the mandible, as well as superiorly and slightly posteriorly until the abscess cavity is reached.
A rubber drain is inserted and secured to skin with suture
INCISION & DRAINAGE
Intraoral appraoch
A vertical incision is placed over the pterygomandibular raphe.
A sinus forcep or curved hemostat is passed through the pterygomandibular raphae along the medial surface of the mandible, medial to the medial pterygoid and just lateral to the superior constrictor is then divided posteriorly
SPREAD
Infection can spread upwards through foramina
such as f. ovale, f.lacerum & juglar foramen
resulting in brain abscess, meningitis or sinus
thrombosis
Infection can spread downward into carotid sheath
towards mediastinum ; a pathway Mosher called
the “Lincoln’s highway” of neck
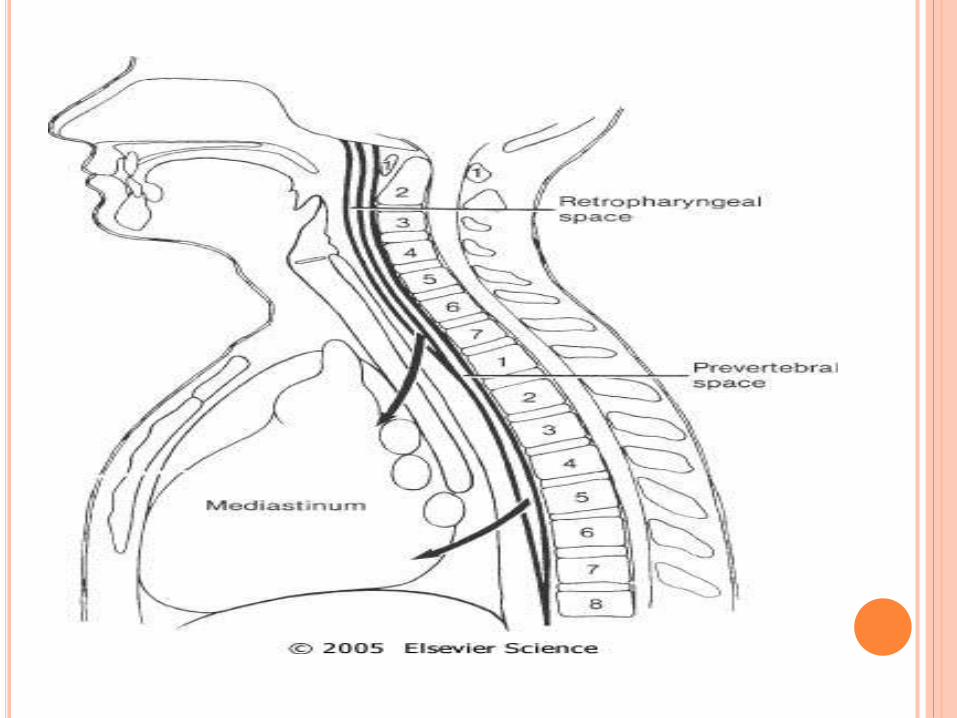
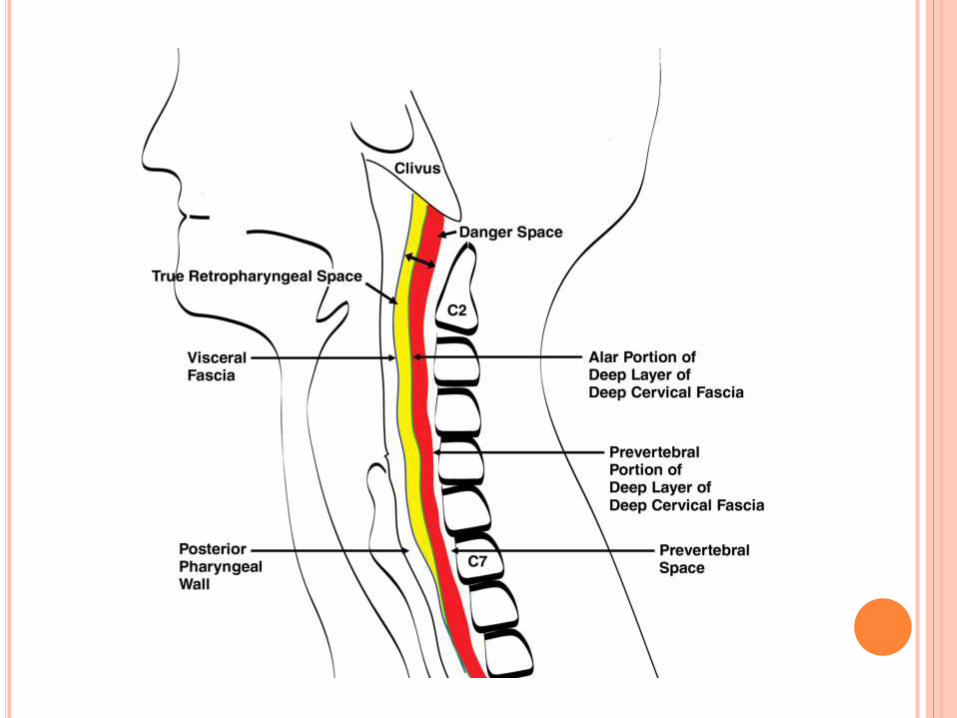
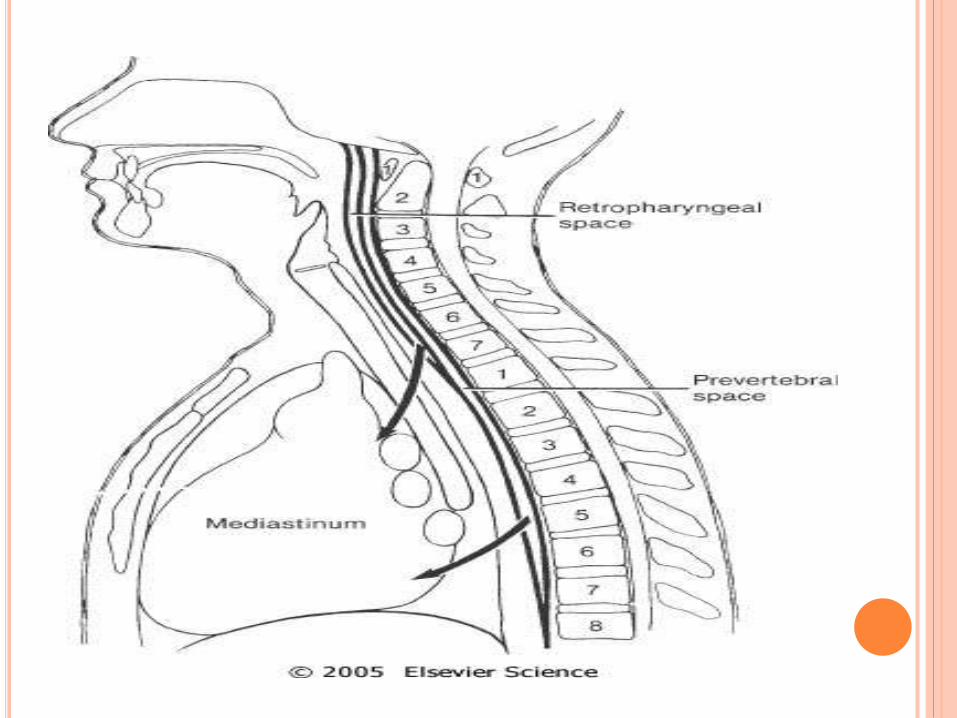
RETROPHARYNGEAL SPACE
The retropharyngeal space lies posteromedial to
the lateral pharyngeal space.
SURGICAL ANATOMY
Anterior : Superior pharyngeal muscle and its
investing fascia
Posterior : Alar layer of prevertebral fascia
Superior : Skull base at pharyngeal tubercle
Inferior : Fusion of alar & prevertebral fascia at C6
to T1.This level is at the posterosuperior
mediastinum.
Lateral : Carotid sheath & Lateral pharyngeal space
CLINICAL FEATURES
When the retropharyngeal space becomes involved
condition is always fatal.
Clinical signs and symptoms are those of a severe
infection.
Trismus is severe in essentially all patients at this
stage.
Evaluation of the retropharyngeal space is
performed with the greatest sucess by a lateral
radiograph of the neck
Involvement of the retropharyngeal space may also
include the prevertebral space
INCISION & DRAINAGE
Suprahyoid portion : The space is approached through the
lateral pharyngeal space, hence the dissection is the same,
until the lateral pharyngeal space is further explored by blunt
finger dissection. the dissection is continued until the surgeon
is able to palpate the contralateral transverse processes of the
vertebrae, the endotracheal tube from its posterior aspect, and
if necessary the opposite carotid artery.
Infrahyoid portion : If the space is involved below the hyoid
bone, then the posterior end of the low submandibular incision
described above is extended inferiorly along the anterior
border of sternocleidomastoid muscle. As the dissection
passes deep to anterior layer of deep cervical fascia, the
sternocleidomastoid muscle is retracted posterolaterally to
expose the carotid sheath.
PREVERTEBRAL SPACE
A potential space between the two layers of prevertebral
fascia, the alar and prevertebral layers.
It extends from the skull base inferiorly to the
diaphragm.
The space is also known as the danger space No. 4 (Grodinsky and Holyoke, 1938).
Mediastinitis is concern with prevertebral space
infections similarly to retropharyngeal space infections
COMPLICATIONS
First, the upper airway is in danger of obstruction as a
result of anterior displacement of the posterior pharyngeal
wall into the oropharynx. Narrowing of the upper airway
as the retropharyngeal space swells.
Second, when the retropharyngeal spaces are filled with
pus, a danger exists of spontaneous rupture of the
abscess, resulting in aspiration, pneumonia, and
asphyxiation. Rupture may also be caused by attempts at
insertion of an endotracheal tube to secure the airway.
Third, once the infection has gained access to the
retropharyngeal spaces, the posterosuperior mediastinum
or the entire posterior mediastinum may become infected
also.
LUDWIG’S ANGINA
DEFINITION
Ludwig's angina is a bacterial infection of the floor of the
mouth.
ALTERNATE NAMES
PATHOLOGY
MICROBIOLOGY
ETIOLOGY
Ludwig's angina is a type of cellulitis that involves
inflammation of the tissues of the floor of the mouth,
under the tongue. It often occurs after an infection of the
roots of the teeth (such as tooth abscess) or a mouth
injury.
This condition is uncommon in children.
ETIOLOGY
CLINICAL FEATURES
Swelling of the tissues occurs rapidly and may block the airway or prevent swallowing of saliva.
Symptoms include:
Breathing difficulty
Confusion or other mental changes
Fever
Neck pain
Neck swelling
Redness of the neck
Weakness, fatigue, excessive tiredness
Additional symptoms that may be associated with this disease:
Drooling
Earache
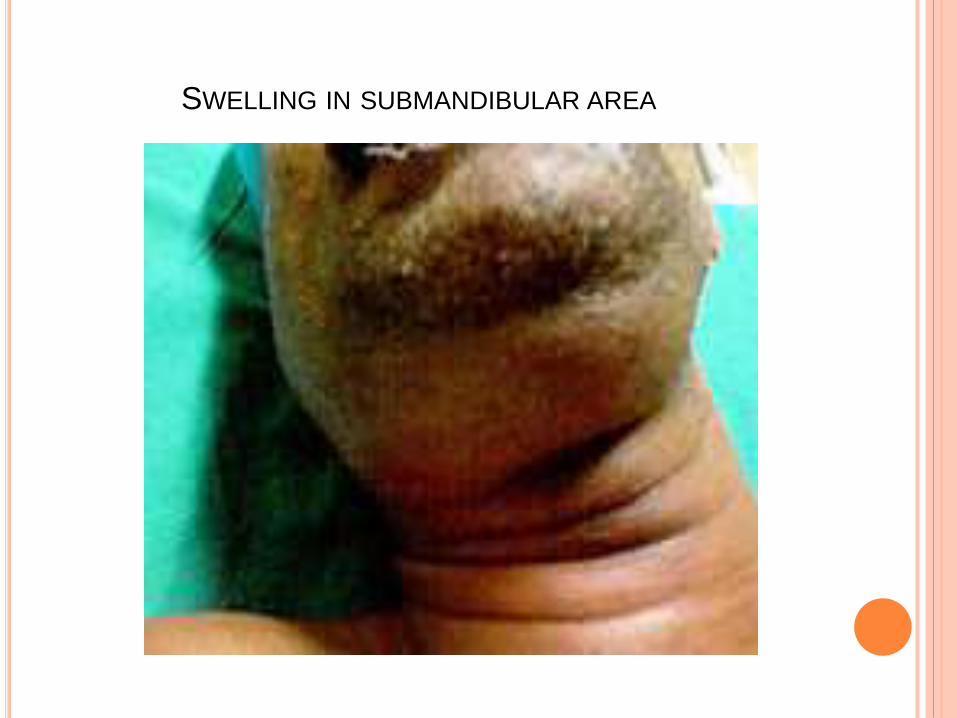
SWELLING IN SUBMANDIBULAR AREA
EXAMINATION & INVESTIGATION
An examination of the neck and head shows redness and
swelling of the upper neck, under the chin. The swelling
may reach to the floor of the mouth. The tongue may be
swollen or out of place.
A CT scan of the neck may be recommended.
Culture of fluid from the tissues may show bacteria
MANAGEMENT
If the swelling blocks the airway, emergency medical help is needed to maintain an open airway. This may involve placing a breathing tube through the mouth or nose and into the lungs, or surgery called a tracheostomy that creates an opening through the neck into the windpipe.
Antibiotics, usually penicillin or a penicillin-like medication, are given to fight the infection. They are usually given through a vein until symptoms go away. Antibiotics taken by mouth may be continued until tests show that the bacteria have gone away.
Dental treatment may be needed for tooth infections that cause Ludwig's angina.
Surgery may be needed to drain fluids that are causing the swelling.
PROGNOSIS
Ludwig's angina can be life threatening. However, it can
be cured with proper protection of the airways and
appropriate antibiotics
CAVERNOUS SINUS THROMBOSIS
Is the formation of a blood clot within the cavernous
sinus, a cavity at the base of the brain which drains
deoxygenated blood from the brain back to the heart.
The cause is usually from a spreading infection in the
sinuses, ears, or teeth.
Staphylococcus aureus and Streptococcus are often the
associated bacteria.
Cavernous sinus thrombosis causes decrease or loss of
vision, drooping or bulging eyes, headaches, and
paralysis of the cranial nerves which course through the
cavernous sinus.
This infection is life-threatening and requires immediate
treatment, which usually includes antibiotics and
sometimes surgical drainage
ETIOLOGY
CST most commonly results from contiguous spread of
infection from the sinuses (sphenoid, ethmoid, or frontal)
or middle third of the face.
Less common primary sites of infection include dental
abscess, nares, tonsils, soft palate, middle ear, or orbit
(orbital cellulitis).
The highly anastomotic and valveless venous system of
the paranasal sinuses allows retrograde spread of
infection to the cavernous sinus via the superior and
inferior ophthalmic veins.
Staphylococcus aureus is the most common infectious
microbe, found in 50% to 60% of the cases.
Streptococcus is the second leading cause.
Gram-negative rods and anaerobes may also lead to
cavernous sinus thrombosis.
Rarely, Aspergillus fumigatus and mucormycosis cause
CST.
CLINICAL FEATURES
The clinical presentation of CST can be varied.
Both acute, fulminant disease and indolent, subacute
presentations have been reported in the literature.
The most common signs of CST are related to
anatomical structures affected within the cavernous
sinus, notably cranial nerves III-VI, as well as symptoms
resulting from impaired venous drainage from the orbit
and eye.
Classic presentations are abrupt onset of unilateral
periorbital edema, headache, photophobia, and bulging
of the eye (proptosis).
Other common signs and symptoms include:
Ptosis, Chemosis, Cranial nerve palsies (III, IV, V, VI).
Sixth nerve palsy is the most common. Sensory deficits
of the ophthalmic and maxillary branch of the fifth nerve
are common.
Periorbital sensory loss and impaired corneal reflex may
be noted. Papilledema, retinal hemorrhages, and
decreased visual acuity and blindness may occur from
venous congestion within the retina.
Fever, tachycardia, sepsis may be present.
Headache with nuchal rigidity may occur.
Pupil may be dilated and sluggishly reactive.
Infection can spread to contralateral cavernous
sinus within 24–48 hr of initial presentation
DIAGNOSIS
The diagnosis of cavernous sinus thrombosis is made
clinically, with imaging studies to confirm the clinical
impression. Proptosis, ptosis, chemosis, and cranial
nerve palsy beginning in one eye and progressing to the
other eye establish the diagnosis.
DIFFERENTIAL DIAGNOSIS
Orbital cellulitis
Internal carotid artery aneurysm
CVA
Migraine headache
Allergic blepharitis
Thyroid exophthalmos
Brain tumor
Meningits
Mucormycosis
Trauma
CONCLUSION
Most odontogenic infections are caused by anaerobes
Identify possible complications of odontogenicinfections
Antibiotics may not sufficient and incision and drainage of these abscesses may be necessary for resolution
Extracting the causative tooth facilitates the resolution of the infection
Textbook of oral surgery by Neelima Malik.
Textbook of oral surgery by Peterson ,2 nd edition.