Embed Size (px)
Citation preview

Lawrence Andrew “Drew” ShirleyOctober 14th, 2016
Surgical (or Non-Surgical) Management of Thyroid Cancer in the Era of “Over-
Diagnosis”
The Problem of Thyroid Cancer in the 21st Century
2
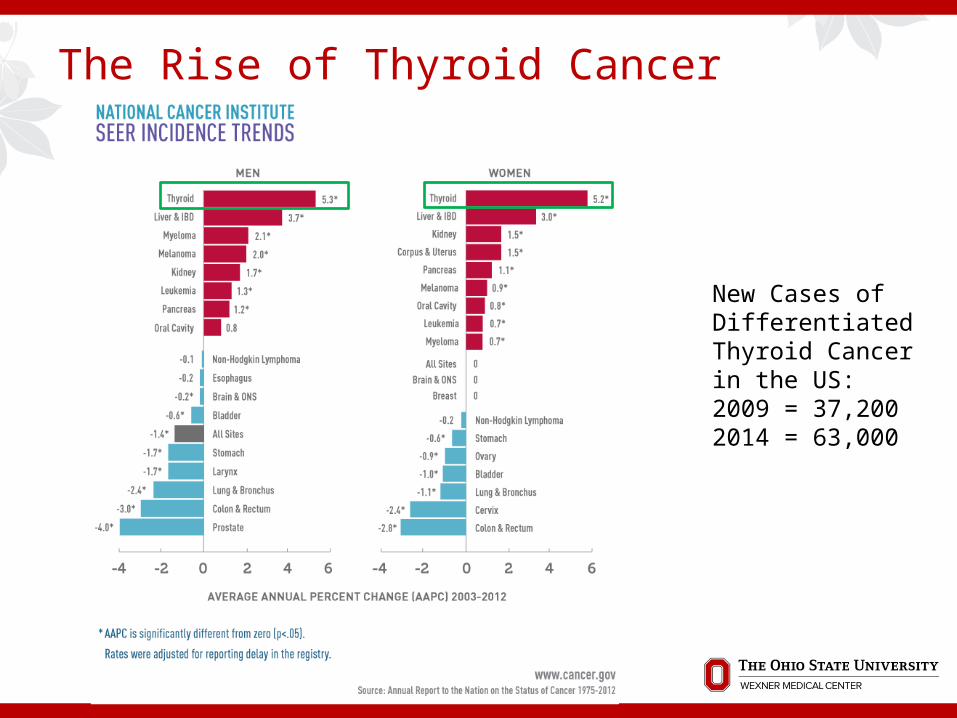
The Rise of Thyroid Cancer
New Cases of Differentiated Thyroid Cancer in the US: 2009 = 37,2002014 = 63,000

4
The Future of Thyroid Cancer
Lubitz, et al. Cancer. 2014 May 1;120(9):1345-52Rahib L, et al. Cancer Res. 2014 74:2913-21.

5
The Outcomes of Thyroid Cancer

6
The Cost of Thyroid Cancer
Estimated Cost of Care in 2013 in the US $1.6 BILLION
Projected Cost in 2030 $3.5 BILLION
2.5 x more likely to file for bankruptcy than those without cancer (highest incidence rate for any cancer)
Lubitz et al. Cancer. 2014 May 1;120(9):1345-52Ramsey et al. Health Affairs. 2013 6:1143-52.

7
Summary of The Problem
Increasing Incidence Increasing Costs Stable, Excellent Outcomes OVER-TREATMENT

8
How to Slow Over-Treatment of Differentiated Thyroid Cancer
Watch It Rename It Stop Looking for It

9
Watch It(Extent of Surgery)
10
Sosa, et al. 2014 National Cancer Database Review
PTC 1-4cm 1998-2006 54,926 total thyroidectomies 6849 lobectomies Assessed for differences in overall survival

11
No Significant Difference in Survival

12
Wang, et al. 2014 Papillary Thyroid Microcarcinoma Treatment
Review of 29,512 patients with PTCs <1cm in SEER 73.4% had total thyroidectomy Radioactive Iodine given to 31.3% No sig diff in DSS for extent of surgery 5 and 10 y DSS 99.6, 99.3%
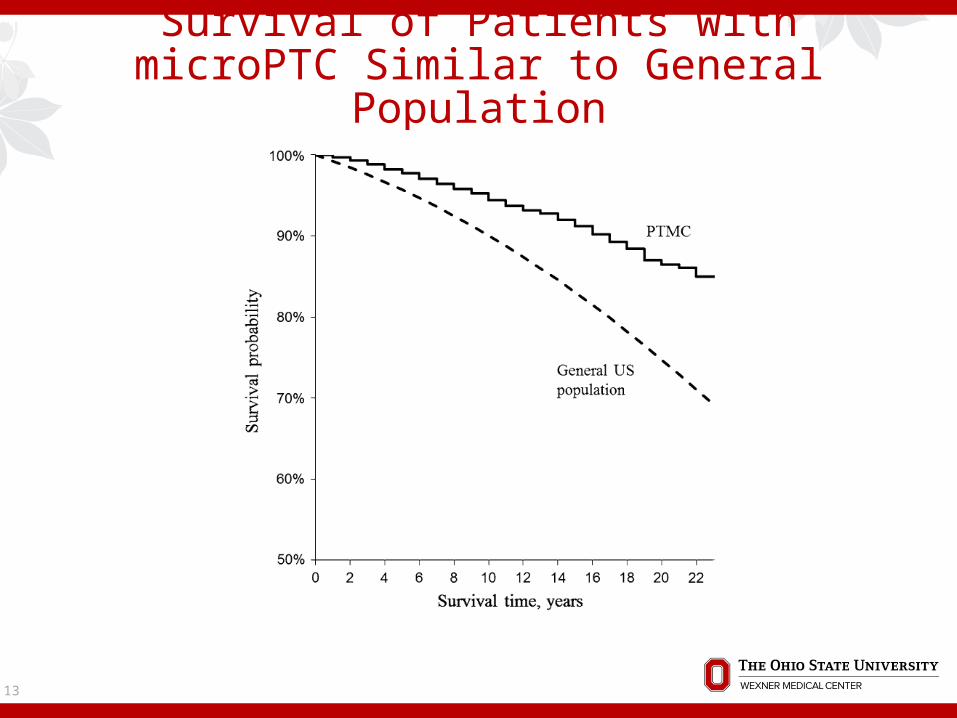
13
Survival of Patients with microPTC Similar to General Population
14
2015 ATA Guidelines - Let’s Take it Down a Notch
For Low-risk Differentiated Thyroid Cancers 1-4cm “Initial surgical procedure can be either a bilateral
procedure (near total or total thyroidectomy) or a unilateral procedure (lobectomy)”
For Microcarcinomas (<1cm) “If surgery is chosen”, lobectomy alone is sufficient

Ito et al. 2010 – Observation Trial
1395 pts with microPTC (<1cm) 340 observation 1055 immediate surgery
Mean observation period 74 months 109 (32%) observed -> surgery
15

16
Ito, et al. – 5 and 10 Year Data
At 10 years, 15.9% tumor grew >3mm and 3.4% with new LN mets
% Tumor Enlargement % Developed Lymph Node Mets

17
Concurrent Observation Studies
Sugitani et al, 2010, Japan 230 patients 5 year 4.6% tumor growth, 1.5% LN mets 15.5% surgery
Pace et al, 2013 - Memorial Sloan Kettering Group Ongoing 71 patients 15 months – 1.4% tumor growth and 1.4% LN mets 8.5% surgery

18
When Papillary Microcarcinomas are Still Dangerous… Clinical presentation, especially vocal cord paralysis Present with clinically apparent lymphadenopathy Present with distant mets (very rare) Present with tall cell variant or poorly differentiated
on FNA (very rare as well)

19
Patients and the “C” Word

20
WAR!
21
Rename It
22
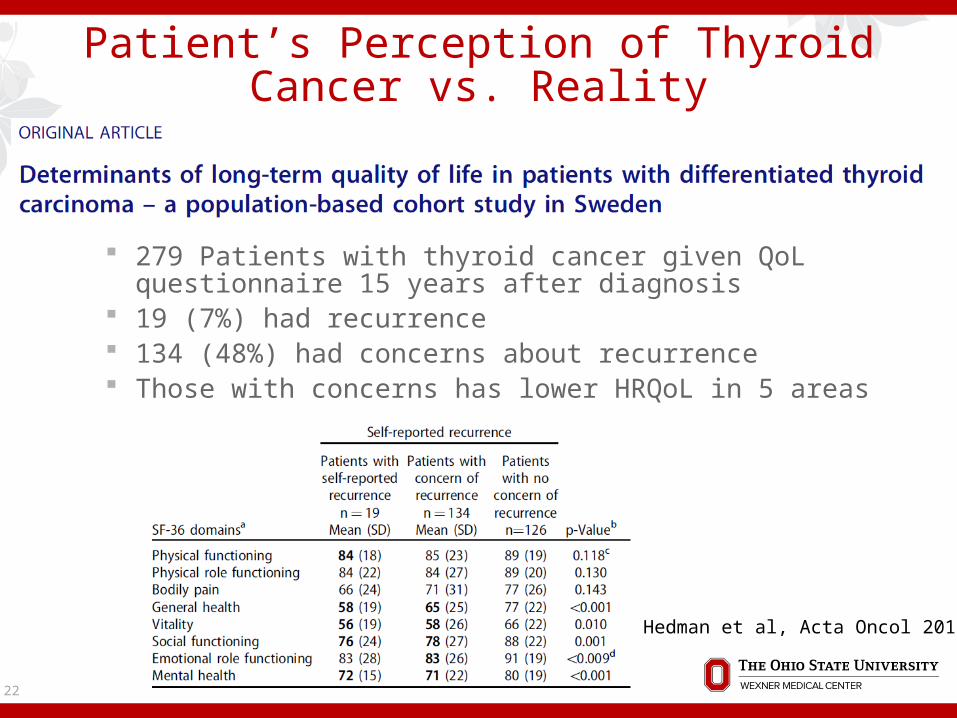
Patient’s Perception of Thyroid Cancer vs. Reality
279 Patients with thyroid cancer given QoL questionnaire 15 years after diagnosis
19 (7%) had recurrence 134 (48%) had concerns about recurrence Those with concerns has lower HRQoL in 5 areas
Hedman et al, Acta Oncol 2015

23
Thyroid Nodules in the Mainstream Media

24
How Common is EFVPTC?
Encapsulated follicular variant of papillary thyroid cancer
Incidence increased 2-3 fold over 2-3 decades Currently, 10-20% of all thyroid cancers
25
Nikiforov, et al. 2016
24 pathologists reviewed specimens from 109 patients with noninvasive encapsulated follicular variant of papillary thyroid cancer (EFVPTC)
Also 101 with invasive EFVPTC Assessed for outcomes
Nikiforov et al, JAMA Oncology 2016

26
No Adverse Events for Noninvasive EFVPTC
Nikiforov et al, JAMA Oncology 2016

27
No More “Cancer”
Noninvasive encapsulated follicular variant papillary thyroid cancer has now become…
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features or…
NIFT-P
28
Renaming MicroPTCs?
5-10% Adults Per Mayo Group (Brito, et al), for cancers:
<2cm No family history No radiation exposure
They should now be called… Micropapillary lesions of indolent course, or… MicroPLICs
Brito et al, 2014 Future Oncol. 2014 10:1-4
29
Stop Looking For It
The Prevalence of Thyroid Pathology
Thyroid nodules Physical Exam – 4-7% Imaging – 30-67% Autopsy study (1955) – 50% had nodules Up to 20% of excised nodules cancer
Thyroid Cancer Autopsy study (1985) – ~ 33% with thyroid cancer
2-3mm cuts – if 1mm cuts, could approach 50%
30
Mortensen 1955 JCEM Harach et al, 1985 Cancer 56:531-8

“Over-Diagnosis”
31

32
Diagnostic Tools vs. Incidence

33
Davies and Welch, 2014
Reviewed SEER data from 1975 – 2009 Incidence tripled 4.9 -> 14.3/100,000 PTC 3.5 -> 12.5/100,000 Mortality stable at 0.5/100,000 Increased incidence -> increased imaging
34
Exposure to Medical Care
Per Davies and Welch, 3 clinical pathways to address:
Opportunistic Screening Diagnostic Cascade Serendipitous Detection “Physicians’ thresholds to palpate, image, and
biopsy the thyroid have likely fallen too far.” “Clinicians…need to be asking themselves whether
they are looking too hard for thyroid cancer.”

35
Critics of Davies/Welch Conclusions
“Had it covered just the last 10 years, critics say, it would show that the death rate from thyroid disease is increasing faster than any other cancer except liver cancer.”
Large tumor incidence Incidence in poorer countries

36
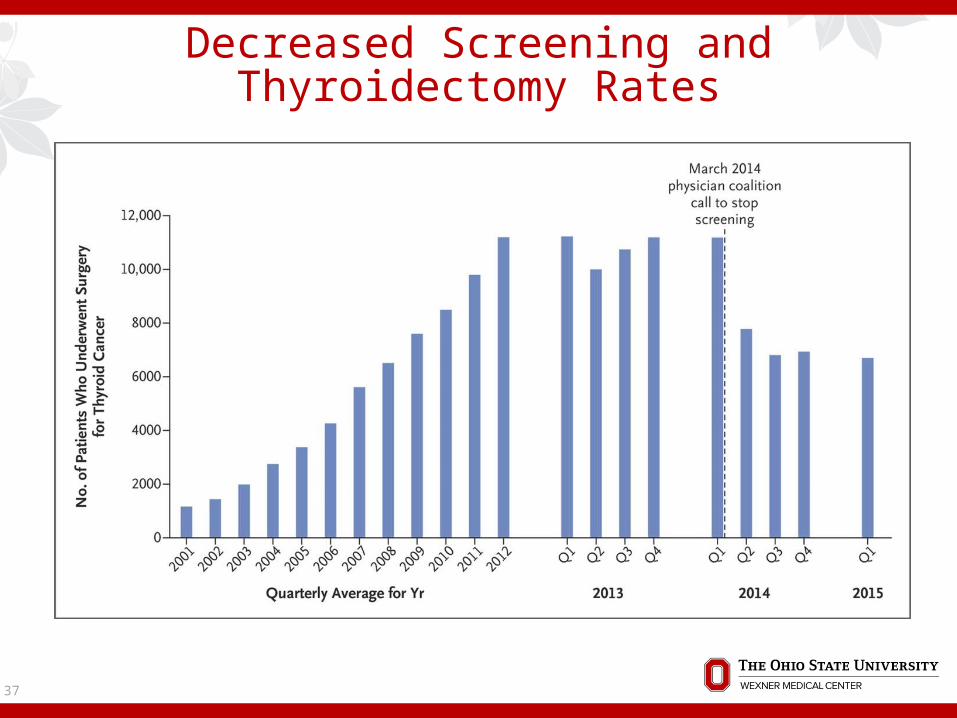
Effect of U/S Screening in South Korea
In 1999, Korean physicians began offering routine cancer screenings, including neck U/S
37
Decreased Screening and Thyroidectomy Rates
38
Mayo Clinic Cohort
Rochester Epidemiology Project Patient Cohort from 1935 Evaluate How Diagnosed
39
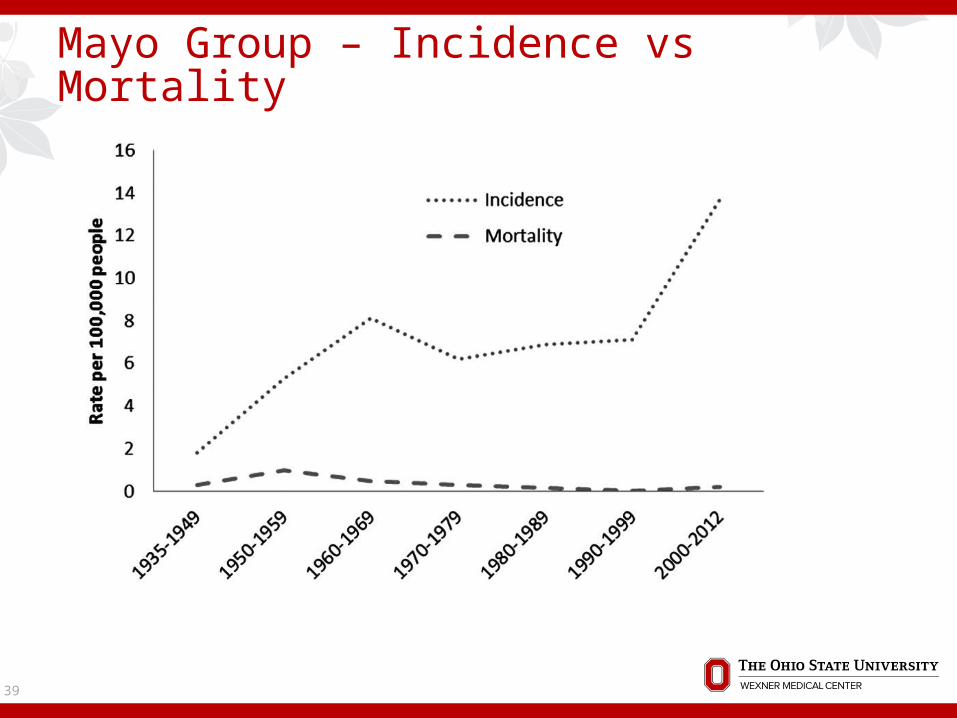
Mayo Group – Incidence vs Mortality

40
Trends in Mayo Cohort – More Low Risk PTC

41
Mayo Group – How Diagnosed
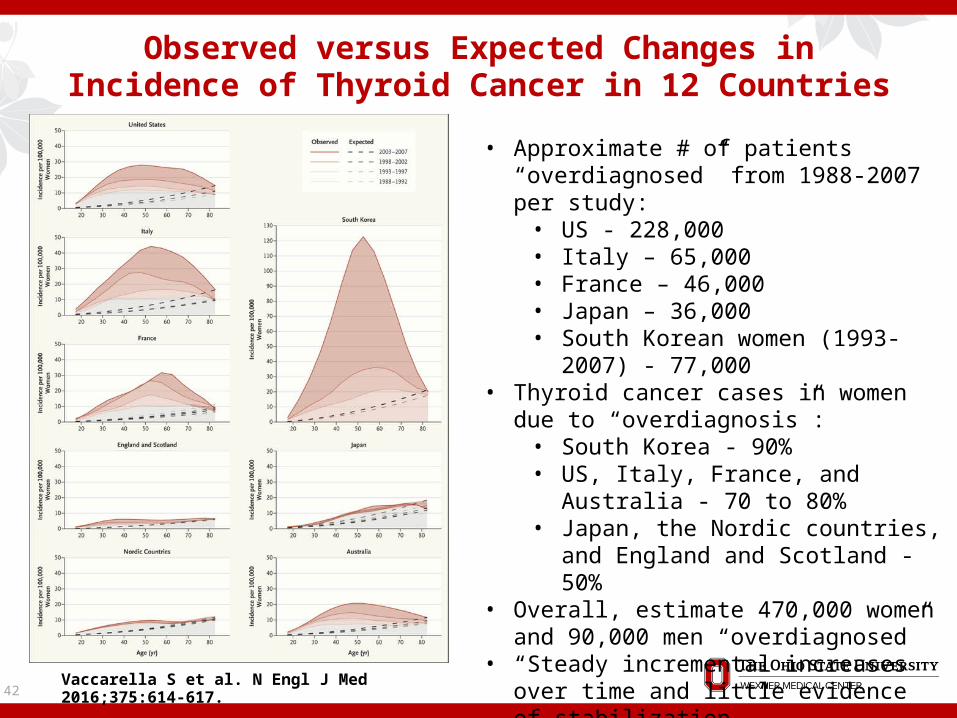
42 Vaccarella S et al. N Engl J Med 2016;375:614-617.
Observed versus Expected Changes in Incidence of Thyroid Cancer in 12 Countries
• Approximate # of patients “overdiagnosed” from 1988-2007 per study:
• US - 228,000 • Italy – 65,000 • France – 46,000• Japan – 36,000 • South Korean women (1993-2007) -
77,000 • Thyroid cancer cases in women due to
“overdiagnosis”: • South Korea - 90%• US, Italy, France, and Australia - 70 to
80% • Japan, the Nordic countries, and
England and Scotland - 50% • Overall, estimate 470,000 women and
90,000 men “overdiagnosed” • “Steady incremental increases over time
and little evidence of stabilization.”

43
New York Times on “Overdiagnosis”
44
Some Choice Quotes from the NYT Article 70-80 % of women “who were told they had thyroid
cancer…actually had tumors that should have been left alone”.
“led doctors to actively look for such minuscule lumps by screening healthy people”
“Once doctors find a tiny nodule, removing the thyroid is often the remedy”
“Some thyroid cancers, of course, really are dangerous, but they tend to be larger than the tiny ones found with scans.”
“But a rise in cancer cases while the death rate does not budge points to overdiagnosis.”
“And that, sadly enough, is what has happened”.

45
Is Incidence Plateauing?
Update of SEER Data From 2010-2012, incidence stabilized Attributed to more measured work-up and
treatment
Morris, Tuttle, Davies. JAMA Otolaryngol Head Neck Surg. 2016 Jul 1;142(7):709-11.

46
The Problem with the Solutions
Many patients will not accept “observation” Renaming small cancers will not completely fix, as
small cancers can still metastasize Avoiding imaging and further work-up of these
nodules can miss the opportunity to catch these cancers before they spread
“Progress, but no precision”

47
Next Steps

48
Separating Out the Bad Actors
Imaging PET scan/other metabolic imaging
Molecular testing Afirma and Thyroseq (but for cancers specifically) BRAF/RAS/TERT promoter mutations
Other biomarkers…
49
Conclusions
Thyroid cancer is increasing in incidence, on track to be 4th most common cancer by 2030
Majority of this increase in cancer incidence is due to small papillary thyroid cancers, but they are still treated aggressively
2015 ATA guidelines recommend more measured approach to work-up and surgical treatment (lobectomy, possibly observation)
Observation trials show slow rate of tumor growth and lymph node metastases – but not ZERO
Re-naming more indolent thyroid nodules to remove the word “cancer” may stem aggressive treatment (NEFVPTC -> NIFT-P)
Some groups advocate lessening imaging and biopsies of thyroid abnormalities to “decrease” cancer rates and treatment
Need biomarkers to determine which cancers will spread and which will remain indolent

50
Acknowledgements Department of Surgery:
Timothy Pawlik Steven Steinberg Raphael Pollock John Phay
Shirley Lab: Sam McCarty
Ringel Lab: Matthew Ringel Moto Saji
Department of Pathology: Ben Swanson

51
Questions?