Embed Size (px)
Citation preview

Tuberculosis in Rroma communities in Europe
Traian Mihaescu

The Rroma population represents an ethnic group of 10 million individuals living in almost all European countries: “the most populous marginalised community in Europe having some of the greatest health needs”
Parekh N, Rose T. Cent Eur J Public Health 2011

The Economist, 2001

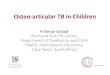
Linguistic, anthropological, historical and genetic evidences point out India* as the origin of the Rroma populations, which may have left the continent approximately between the 5th–10th centuries . After leaving India, the Rroma migration route passed through Persia, Armenia, Greece and the Balkans.
*the Punjab state, in North-western India
Mendizabal I et al. PLoS One. 2011


In UK and IrelandGypsies and Travellers report poorer health on standardised measures than comparable groups of residents from socially deprived inner city areas, other ethnic minorities and rural residents.
Poorer health status was reported in relation to long-term illness, health problems that limit daily activities or work, health-related quality of life, chest pain, respiratory problems, arthritis, miscarriage and premature death of offspring.
Parry G et al. J Epidemiol Community Health 2007

Incidence of TB, AIDS, imprisonment and injecting drug use in a Roma population.
Barcelona (1985–2008) Rate/100 000pyf (95% CI) Global
TB 90.9 (68.5–113.2) AIDS 104.1 (80.1–128.0) Imprisonment 642.0 (579.7–704.3) IDU 239.8 (203.0–276.6)
Casals M et al. Eur J Publ Health 2011

In 126 gypsy patients, aged over 15, registered with TB in two districts of Bucharest, Romania
• 83% of bacteriological confirmed cases were smear positive
• 48% succes rate• 66.7% associated diseases/comorbidities
Dediu I et al. Pneumologia 2000

A prospective study of detection of TB infection in the rroma community fom the west of Romania (July 2009-December 2010):• 1417 persons surveyed• 700 (49,40%) with positive TST • 73.42% no BCG scar • 51.43% positive TST - men• 71,20% had recently tb contact
Nini G et al. ERS Congress 2011

Active TB screening in Rroma population, Belgrade, Serbia:• 407 registered adults• 167 (41%) presented and id chest X-ray• 8 subjects suspects – no TB case M-/C-
• 224 children• 202 examined• 16 TST positive – none diagnosed with TB
Curcic RV et al. ERS Congress 2005

Active TB screening in Rroma population, Vojvodina, Serbia:
• 3958 registered adults• 870(22%) with suspect chest X-ray• 7 active cases confirmed (176.9/100000)
Pavlovic S et al. ERS Congress 2005

Tuberculosis in a gypsy community (rural, Romania) has an unpredictible course, primary tuberculosis is prevalent, and the illness develops in isolated foci requiring targeted and sustained surveillance.
Ionita M et al. ERS Congress 2001

Published research on the health needs of the Roma population is sparse!
Hajioff S . J Epidemiol Community Health 2000
A limitation .. which exists in all studies about the Rroma population, is that follow-up is hindered by the fact that subject information is found under different names, shared names and many do not appear in the registers.
Casals M. Eur J Publ Health 2011
Defining the Rroma population is quite difficult.Idzerda L.BMC International Health and Human Rights 2011

“The common trait of the Gypsies, one that gives them identity, is a way of life different from that of other ethnic communities, and most of all a different strategy of life that has survived to this day, even if in modern shapes.”
Achim V. The Gypsies in the histoy of Romania, Ed Enciclopedica, 1998

“Family was found to be an important factor influencing the survival rates..”
Casals M et al. Eur J Public Health 2011

The absence of data and comprehensive efforts addressing TB in the Rroma community is striking.
Schaaf M. Open Society Institute 2007

• real numbers – – migration,– ethnicity denial, – uptodate identification papers.
• socio economic status• education level• unemployment• overcrowding

Levels of CO and CO2 were higher in winter in both
countries as compared to summer. The limit value of 10 mg/m3 CO was exceeded in a few cases in both countries. In general, levels of CO, CO2 and PM were higher in Romania. Further environmental and behavioural hazards such as indoor smoking, pets inside or lack of ventilation were found. The reported self-perceived quality of the indoor environment was poor in many aspects.
Cent Eur J Public Health. 2012 Sep;20(3):199-207. Assessment of the indoor environment and implications for health in Roma villages in Slovakia and Romania. Majdan M, Coman A, Gallová E, Duricová J, Kállayová D, Kvaková M, Bosák L.

Roma scored poorly compared to non-Roma in psychological well-being, vital exhaustion and HRQL (p ≤ 0.001); however, these differences could be to a substantial extent explained by SES. With regard to personality traits, ethnicity and SES played a less significant role.
Skodova Z, van Dijk JP, Nagyova I, Rosenberger J, Ondusova D, Studencan M, et al. Psychosocial factors of coronary heart disease and quality of life among Roma coronary patients: a study matched by socioeconomic position. Int J Public Health. 2010 Oct;55(5):373–380.

CONCLUSIONS:The adverse quality of life among Roma coronary
patients may warrant additional care, which should target their low SES but also other factors related to their ethnic background, such as culture and living conditions.
Skodova Z, van Dijk JP, Nagyova I, Rosenberger J, Ondusova D, Studencan M, et al. Psychosocial factors of coronary heart disease and quality of life among Roma coronary patients: a study matched by socioeconomic position. Int J Public Health. 2010 Oct;55(5):373–380.

J Epidemiol Community Health. 2009 Jun;63(6):455-60. doi: 10.1136/jech.2008.079715. Does socioeconomic status fully mediate the effect of ethnicity on the health of Roma people in Hungary? Vokó Z, Csépe P, Németh R, Kósa K, Kósa Z, Széles G, Adány R.

RESULTS:The health status of people living
in Roma settlements was poorer than that of the general population (odds ratio of severe functional limitation after adjustment for age and gender 1.8 (95% confidence interval 1.4 to 2.3)). The difference in self-reported health and in functionality was fully explained by the socioeconomic status.

RESULTS:. The less healthy behaviours of people living
in Roma settlements was also related very strongly to their socioeconomic status, but remained significantly different from the general population when differences in the socioeconomic status were taken into account, (eg odds ratio of daily smoking 1.6 (95% confidence interval 1.3 to 2.0) after adjustment for age, gender, education, income and employment).

CONCLUSION:Socioeconomic status is a strong determinant of
health of people living in Roma settlements in Hungary. It fully explains their worse health status but only partially determines their less healthy behaviours.

CONCLUSION:
Efforts to improve the health of Roma people should include a focus on socioeconomic status, but it is important to note that cultural differences must be taken into account in developing public health interventions.

Int J Public Health. 2009;54(4):274-82. doi: 10.1007/s00038-009-7108-7.
Socioeconomic indicators and ethnicity as determinants of regional mortality rates in Slovakia.
Rosicova K, Geckova AM, van Dijk JP, Rosic M, Zezula I, Groothoff JW.

OBJECTIVES:Regional differences in mortality might reflect socioeconomic and
ethnic differences between regions. The present study examines the relationship between education, unemployment, income, Roma population and regional mortality in the Slovak Republic.
METHODS:Separately for males and females, data on standardised mortality in
the Slovak population aged 20-64 years in the year 2002 were calculated for each of the 79 districts. Similarly the proportions of respondents with tertiary education, unemployed status, Roma ethnicity and income data were calculated per district. A linear regression model was used to analyse the data.

RESULTS:Socioeconomic differences in regional mortality were found among
males, but not among females. While education and unemployment rate significantly contributed to mortality differences between regions, income and the proportion of Roma population did not. The model explained 32.9% of the variance in standardised mortality rate among districts for males and 7.6% for females.
CONCLUSION:Low education and high unemployment rate seems to be an indicator
of regions with high mortality of male and therefore should be targeted by policy measures aimed at decreasing mortality in productive age.

Potential health related cultural characteristics
• past oriented people• guided by belief• time of relative value – punctuality is not valued (not necessarily meant as
an offense)– belief in predestination is common (why bother,
why plan, whatever will be will be)

Potential health related cultural characteristics
• tabu subjects (usualy sexual matters)• group oriented people:– loyality to family is paramount, – respect to elders,– sometimes ostility towards the outsiders – gadje
are unclean as they do not follow the rules of separating the halves of the body.

Potential health related cultural characteristics
• schooling may be precarious – cultural background places little value on gadje culture – age of ten may be a threshold in following school – ability to follow complex therapeutic regimens is reduced.
• ierarchic society – age may matter in health decisions, elder oriented society

Potential health related cultural characteristics
• health and disease beliefs
– healthy as long as autonomy is maintained – late to seek medical advice, improbable to complete long treatments
– natural/traditional/herbal treatments may be prefered/taken without medical advice (older people)

Potential health related cultural characteristics
• health and disease beliefs
– spiritual dimension may play a role
• lower half of the body is considered impure,• curses/evil eye may work, • asking forgiveness from the dying

Potential health related cultural characteristics
• health and disease beliefs– hygiene is considered important but may have
different conotations • may avoid medical institutions as they are impure;• upper body secretions are pure lower body secretions
are unclean;• baths are less acceptable than showers; • prepubescent and older women are purer as there is no
menstruation.

Potential health related cultural characteristics
• health and disease beliefs
– older physicians are better– famous physicians are sought– medication sharing is common – general anesthesia may not be acceptable

Ethnification of poverty means..

…postmodern racism!Flecha R. Harvard Educ Review 2004

It is important for public health across Europe that the health needs of the Rroma are prioritised by governments concerned.
Parekh N, Rose T. Cent Eur J Public Health 2011