EVALUATION OF CERVICAL SPINE INJURY
SRI SIDDHARTHA MEDICAL COLLEGE,TUMKURDEPARTMENT OF
ORTHOPAEDICSTOPIC:The effect of intact fibula on functional outcome
of reamed intramedullary interlocking nail in open and closed
isolated tibial shaft fractures: A prospective study
Chairperson & Moderator :prof. & HOD Dr.Mahesh K.UDept.
of OrthopaedicsPresenter:Dr. Jaipalsinh MahidaDept. of
Orthopaedics
INTRODUCTIONTibia is main weight-bearing bone in the leg,
carrying greater than 80% of load. Tibia and fibula Fractures
relatively common and have been recognized as serious and
debilitating injuries for centuries.The management is influenced
greatly by the associated soft tissue injury.Severe open fractures
of the tibia are associated with high complication rates and poor
long term outcomes. Tibial fractures have relatively high rates of
nonunion and malunion Compared to fractures elsewhere in the
body
Isolated tibial shaft fractures with intact fibula are a fairly
common injury. have been associated with nonunion rates ranging
from 1% to 17%. Primary fibulectomy has been recommended in order
to overcome the adverse effect of an intact fibula accepting the
additional morbidity associated with this procedure. The intact
fibula is often blamed for problems related to union in these
fractures. The primary aim of the study whether these fractures can
unite without a primary fibulectomy.
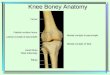
ANATOMYLower leg contains 2 bones1. TibiaTriangular in
shapeThick cortex & strongDistal articular surface is
externally rotated approx. 200 compared to proximal articular
surface. (tibial torsion).Distal articular surface is perpendicular
to the mechanical axis of the tibia, whereas the proximal articular
surface is tilted slightly medial.2. Fibulalies posterior and
lateral to the tibia Both bones are connected by a thick
interosseus membrane
Tibia has medullary and a periosteal blood supply. Outer 25% to
30% of cortex derives its oxygenation primarily from the periosteal
system, Rest of the bone is predominantly supplied by the medullary
system.Main nutrient artery to the tibia is branch of the posterior
tibial artery and enters the bone in its proximal one-third.
Reaming has been shown to temporarily decrease medullary blood
supply in animal studies.However, animal studies have also shown
that loss of the medullary arterial system results in stimulation
of the periosteal system and reversal of the normal direction of
blood flow through the anastomoses between the two vascular
systems.
Compartments and Musculature:The musculature of the leg is
divided into four compartments.
The Four Compartments of the Leg with the Muscles, Arteries, and
Nerves Contained Within ThemCompartmentMusclesArteries &
nervesAnteriorTibialis anterior
Extensor hallucis longus
Extensor digitorum longus
Peroneus tertius Anterior tibial arteryDeep peroneal
nerveLateralPeroneus longus
Peroneus brevisSuperficial peroneal nerve Superficial
posteriorGastrocnemius
Soleus
Plantaris
Deep posteriorTibialis posterior
Flexor hallueis longus
Flexor digitorum longus
PopliteusPosterior tibial artery
Peroneal artery Tibial nerve
The anterior compartment musculature originates predominantly
from the anterolateral aspect of the proximal tibia and includes
the main dorsiflexors of the ankle and toes.
The lateral compartment muscles evert the foot and take origin
from the lateral and posterior aspects of the fibula diaphysis. The
lateral compartment also contains the superficial peroneal nerve
which exits the fascia approximately 10 to 12cm proximal to the tip
of the distal fibula. The superficial Peroneal nerve is at risk
during lateral fasciotomy, distal fibular fixation, and placement
of distal screws during percutaneous plating of the tibia.
The superficial posterior compartment are Primary ankle
plantarflexor, and the plantaris muscle.
The posterior deep compartment is bordered anteriorly by the
posterior surface of the tibia and the interosseus membrane. It
contains tibialis posterior which inverts the foot, flexor hallucis
longus and flexor digitorum longus, which plantarflex the toes, in
addition to popliteus, and the peroneal artery, posterior tibial
artery, and tibial nerve.
The posterior deep compartment can be difficult to assess for
compartment syndrome by clinical examination and it is the
compartment most often incompletely released during fasciotomy.
6
The anterior compartment musculature originates predominantly
from the anterolateral aspect of the proximal tibia and includes
the main dorsiflexors of the ankle and toes.
The lateral compartment muscles evert the foot and take origin
from the lateral and posterior aspects of the fibula diaphysis. The
lateral compartment also contains the superficial peroneal nerve
which exits the fascia approximately 10 to 12cm proximal to the tip
of the distal fibula. The superficial Peroneal nerve is at risk
during lateral fasciotomy, distal fibular fixation, and placement
of distal screws during percutaneous plating of the tibia.
The superficial posterior compartment are Primary ankle
plantarflexor, and the plantaris muscle.
The posterior deep compartment is bordered anteriorly by the
posterior surface of the tibia and the interosseus membrane. It
contains tibialis posterior which inverts the foot, flexor hallucis
longus and flexor digitorum longus, which plantarflex the toes, in
addition to popliteus, and the peroneal artery, posterior tibial
artery, and tibial nerve.
The posterior deep compartment can be difficult to assess for
compartment syndrome by clinical examination and it is the
compartment most often incompletely released during fasciotomy.
7
Mechanisms of Injury:
Tibial fractures have a bimodal distribution with low-energy
spiral patterns more common in patients over 50 years most common
causes falls from a standing height and sporting
injuries.high-energy transverse and comminuted fracturesmore common
in patients under 30 years of age. most commonly associated with
vehicular trauma.
Because of its subcutaneous location open fractures of the tibia
are common with reported rates varying between 12% and 47% Open
fractures are even more common with high-energy mechanisms with
rates as high as 63% being reported following motorcycle crashes.
When open fractures occur in the tibia they are more commonly type
IIIB requiring flap coverage.
CLINICAL EVALUATIONSigns & Symptoms: PainInability to walk
or bear weight on the legDeformity or instability of the legBone
"tenting" the skin or protruding through a break in the skinOn
physical examination focus on:Compromised
SkinWoundsVascularMotorSensory
Evaluation of compartment syndrome: pain out of proportion to
injury severity, pain on passive stretch of the relevant
compartment musculature, paresthesiae, paralysis of the muscles in
the affected compartments, severely swollen or indurated
compartments, and in rare cases, pulselessness.
Imaging & Diagnostic studies: Radiographic evaluation (full
length tibia with knee and ankle joint)Anteroposterior viewLateral
view
Computed tomography ordered to exclude commonly associated
fractures near joints.
The management of tibia diaphyseal fractures is influenced most
significantly by the state of the soft tissues. Therefore, in
clinical practice tibial fracture classification is meaningless
without a classification of the associated soft tissue
injury.Classification:
The Tscherne classification is used to classify closed
fractures.
C0 - simple fracture configuration with little or no soft tissue
injury.C1 Superficial abrasion, mild to moderately severe fracture
configuration.C2 deep contamination with local skin or muscle
contusion, moderately severe fracture configuration. C3 extensive
contusion or crushing of skin or destruction of muscle, severe
fracture.
15
The Gustilo - Anderson classification used to classify open
fractures.
TYPE I - Clean wound of less than 1 cm in lengthTYPE II - Wound
larger than 1 cm in length without extensive soft tissue damageTYPE
III - Wound associated with extensive soft tissue damage; usually
longer than 5cmTYPE IIIA - Adequate periosteal cover TYPE IIIB -
Presence of significant periosteal strippingTYPE IIIC - Vascular
repair required to revascularize leg
16
The most commonly used classification system for fractures of
the tibia and fibula is the AO/OTA classification which separates
fractures into Type A - simple fractures,Type B - wedge fractures,
and Type C - complex fractures
Treatment Options:
Nonoperative Treatment:Multiple studies have demonstrated that
nonoperative management is associated with poorer results when
compared to IM nails with reference to nonunion, malunion, return
to work, outcome scores, or time to union. Despite this there is
still a role for nonoperative management in treating adults with
tibial diaphyseal fractures. Displaced tibial fractures without a
fibular fracture are prone to fall into varus with nonoperative
treatment, Require particular caution and close monitoring when
treated closed.
The Indications and Relative Contraindications for Nonoperative
ManagementIndicationsRelative ContraindicationAdequate alignment,
length, and rotation in a splint or castSignificant anesthetic
riskPatient refuses operative treatmentInadequate alignment,
length, and rotation after application of splint or castOpen
fractureArterial injuryDisplaced proximal or distal
fractureCompartment syndrome or high risk of compartment
syndromeSoft tissues will not tolerate a splint, cast, or
bracePatient unable to comply with nonoperative protocolIpsilateral
femoral diaphyseal fractureHigh-energy mechanism or soft tissue
injury
Acceptable Malalignment in Tibial Diaphyseal FracturesAlignment
ParameterAcceptable MalalignmentVarus
Valgus
Apex anterior/ posterior
Rotation
Shortening
![Meta-analysis of plate fixation versus intramedullary fixation ......intramedullary fixation (IF), the common devices in clinics are Knowles pinning [14,15], elastic stable intramedullary](https://img.pdfslide.net/doc/110x75/60ec8dbb516bc21c1e0f6489/meta-analysis-of-plate-fixation-versus-intramedullary-fixation-intramedullary.jpg)