Embed Size (px)
Citation preview

TUBERCULOSIS
PRESENTED BYTHUSHARA . C1ST YEAR M PHARMGRACE COLLEGE OF PHARMACY

INTRODUCTION
Pulmonary Tuberculosis (TB) is an infectious disease that mainly affect the lungs parenchyma.
TB is a contagious bacterial (M. tuberculosis) infection that mainly affects the lungs parenchyma, but may spread to other organs.

The World Health Organization declared TB a world global emergency in 1993; however, economic and political commitment to TB control programs is lacking in many countries, and it is estimated that 95% of new cases of TB occur in countries with limited resources.
This situation facilitates inappropriate or unsustained TB therapy, which in turn has promoted a rise in the rates of multidrug-resistant TB (MDR-TB)
EPIDEMIOLOGY

Over 9 million new cases and 2 million deaths per year worldwide
1/3rd of the world’s population is infected with M. tuberculosis
Tuberculosis remains one of the top three killers
In the U.S.- estimated that 10-15 million people are infected ◦Less than 15,000 cases in US per year◦India is the highest TB burden country in the world and accounts nearly 20% of global burden
◦Every yr approx 0.8 million new smear positive cases


EPIDEMOLOGICAL INDICES
1.Prevalence of infection2.Incidence of infection3.Prevalence of disease or case rate4.Incidence of new cases5.Prevalence of suspected cases6.Case detection rate7.Prevalence of drug-resistant cases8.Mortality rate
ETIOLOGY1.AGENT FACTORS
Mycobacterium tuberculosis◦ Highly aerobic◦ Infects lungs◦ Divides every 15-20 hours ◦ Unable to be digested by microphages◦ Very resistant to many disinfectants, acid, alkali, drying,
etc.Contagious, spread through air by inhalation
of airborne bacteria from infectedEasier to contract with weak immune
system

SOURCE OF INFECTION
Two types1.Human source2. Bovine sources
Communicability
Patients are infective as long as they remain untreated

HOST FACTORS1. Age : Affects all age groups . From an average
of 2% in the 0-14 age group and 20% at age 15-24yrs, and more common in the elderly
2. Sex : More prevalence in males than in females
3. Nutrition: Malnutrition is widely believed to predispose to TB
4. Immunity : man has no inherited immunity against TB . It is acquired as a result
Of natural infection or BCG vaccination

MODE OF TRANSMISSION Airway droplets: the main mode of transmission from person infected with pulmonary TB to others by respiratory droplets.Ingestion: Less frequently transmitted by ingestion of mycobacterium bovis found in unpasteurized milk products Direct inoculation

Pulmonary TB is a disease of respiratory transmission, patients with active disease expel bacilli into the air by:
Coughing
Sneezing
Shouting
Or any other way that will expel bacilli into the air

Millions of tubercle bacilli in lungs ( mainly in cavities)Coughing projects droplets nuclei into the air that contain tubercle bacilliOne cough can release 3,000 droplet nuclei One sneeze can release tens of thousands of droplet nuclei As few as five M. tuberculosis (MTB) bacilli are necessary for human infection

Optimal conditions for transmission include:Overcrowding Poor personal hygienePoor public hygiene

DIAGNOSIS Any cough that persists more than 2 weeks should be evaluated for pulmonary TB in the appropriate clinical context ( poor patient, overcrowded, bad hygiene etc)
A full history and physical examination should be undertaken
A minimum of 2 sputum samples, ( the first on spot and the second in the early morning preferably fasting ) should be examined, the sputum sample should be of a good quality representative of lower respiratory tract.

RADIOLOGYThe following characteristics of chest radiograph favor the diagnosis of tuberculosis
Shadows mainly in the upper zones
Patchy or nodular shadows
The presence of a cavity or cavities
The presence of calcification
Bilateral shadows especially if theses are in the upper zones

SPUTUM EXAMINATION
For patients with suspected pulmonary TB, at least three freshly expectorated first morning sputum samples should be collected from a deep, productive cough in a sterile container with a wide mouth. Ideally, the volume of each sample should be more than 5 mL
Induction of sputum with aerosolized hypertonic saline solution may be required if the patient is having difficulty producing sputum; serial morning gastric lavage and bronchoalveolar lavage are alternative methods of obtaining clinical specimens.

SIGNIFICANT LAB TESTTuberculin skin test (PPD test);
Injecting a small amount of protein from tuberculosis bacteria between the derived layer of the skin (usually forearm).
Sputum examination and Cultures;
Is examined under a microscope to look for tuberculosis bacteria and used to grow the bacteria in a culture.

TUBERCULIN TESTING 0.1 ml of 5 tuberculin units ( TU) PPD
Injected intra dermally over the volar aspect of the arm
Should be read in 48-72 hours
Measure induration not erythema
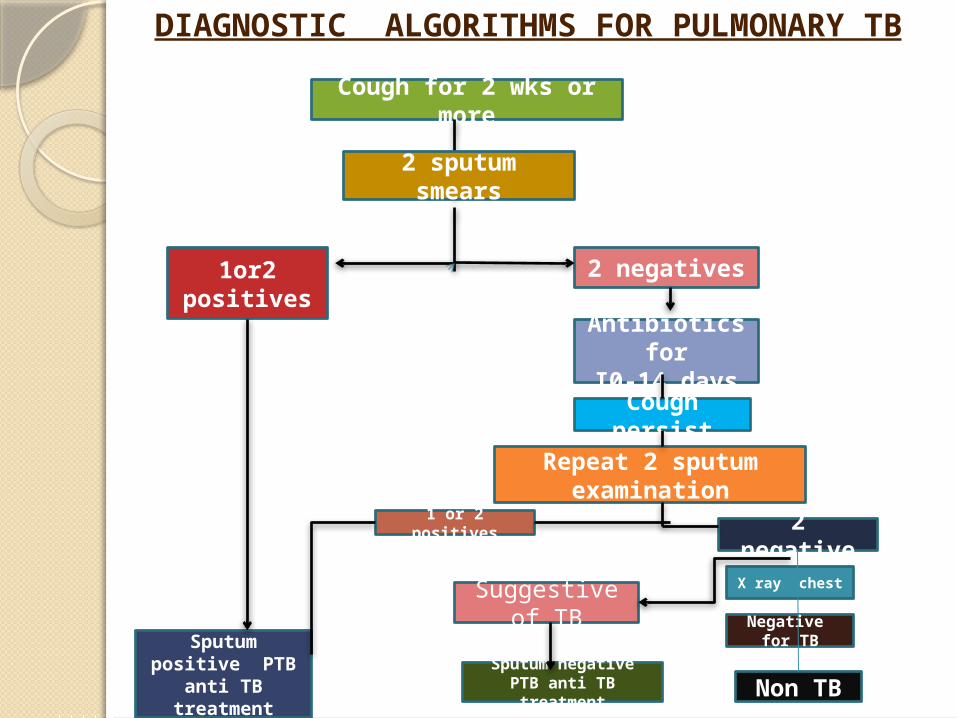
Cough for 2 wks or more
2 sputum smears
1or2 positives
2 negatives
Antibiotics for
I0-14 daysCough persist
Repeat 2 sputum examination
1 or 2 positives 2 negativeX ray chest
Negative for TB
Non TB
Suggestive of TB
Sputum negative PTB anti TB treatment
Sputum positive PTB
anti TB treatment
DIAGNOSTIC ALGORITHMS FOR PULMONARY TB

Interferon-gamma Blood test;A simple blood is mixed with synthetic
proteins similar to those produced by the tuberculosis bacteria.
If people are infected with tuberculosis bacteria, their white blood cells produce certain substances (interferons) in response to the synthetic proteins.
CHEMOTHERAPY
FIRST LINE DRUGS1. RIFAMPICIN2. INH3. STREPTOMYCIN4. PYRAZINAMIDE5. ETHAMBUTOL6. THIOACETAZONE
SECONDLINE DRUG
Fluoroquinolones, ethionamade, capreomycin, kanamycin and amikacin

Chemotherapy
Initial phase Continuation phase
Reduce bacterial population rapidly. Destroy any
remaining bacteria.
• Standard treatment involves 6 months treatment with isoniazid, rifampicin, pyrazinamide and ethambutol.
• Fixed-dose tablets combining two or three drugs are preferred.
• Treatment should be started immediately in any patient who is smear-positive or smear-negative but with typical chest x-ray changes and no response to standard antibiotics.

• 6-months therapy is appropriate for new onset pulmonary TB.
• However, a 12-months therapy is recommended for meningeal TB, including involvement of the spinal cord.
• Treatment may be given daily throughout the course or intermittently (either thrice or twice weekly)
• Patients with cavitary pulmonary TB and delayed sputum-culture conversion should have continuation phase extended by 3 months.
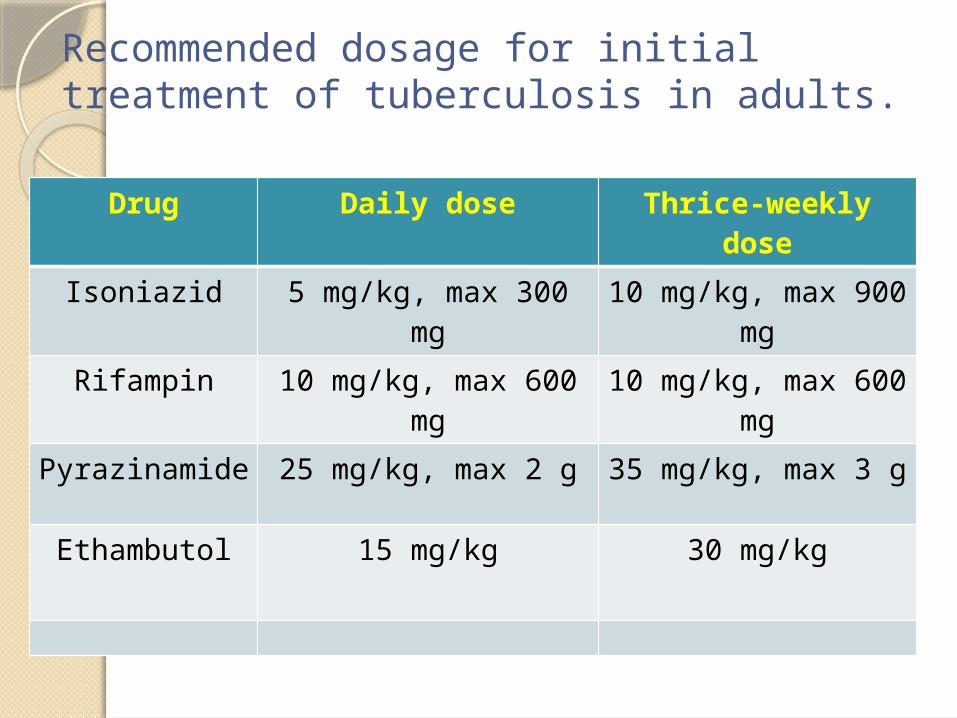
Recommended dosage for initial treatment of tuberculosis in adults.
Drug Daily dose Thrice-weekly dose
Isoniazid 5 mg/kg, max 300 mg
10 mg/kg, max 900 mg
Rifampin 10 mg/kg, max 600 mg
10 mg/kg, max 600 mg
Pyrazinamide 25 mg/kg, max 2 g 35 mg/kg, max 3 g
Ethambutol 15 mg/kg 30 mg/kg

Initial phase Continuation phaseDuration, months
Drugs Duration, months
Drugs
New smear or culture positive cases
2 HRZE 4 HR
New culture negative cases
2 HRZE 4 HR
Pregnancy 2 HRE 7 HR
Relapses and default (pending susceptibility testing)
3 HRZES 5 HRE
Resistance to H 6 RZE
Resistance to R 12-18 HZEQ
Resistance to all first-line drugs.
Atleast 20
months
1 injectable agent + 3 of these 4: E,
cycloserine, Q, PAS.

Regimens for the treatment of latent TB infection in adults.Regimen Schedule Duration
Isoniazid 300 mg daily (5 mg/kg)
9 months
Rifampin 600 mg daily (10 mg/kg)
4 months
Isoniazid plus rifapentine
900 mg weekly + 900 mg weekly (15 mg/kg)
4 months

• BCG is live attenuated strain derived from M. bovis → stimulates development of hypersensitivity to M. tuberculosis • Within 2-4wks swelling at injection site, progresses to papule about 10mm diam & heals in 6-12 wks • Aim of BCG vaccination is to reduce a benign, artificial primary infection which will stimulate an acquired resistant to possible subsequent infection with virulent tubercule bacilli, and thus reduce morbidity and mortality
BCG vaccine

TYPES OF BCG VACCINE 1. Liquid vaccine 2. Freeze dried vaccine
• BCG vaccine stored in a cool place preferably refrigerated at a temperature below 10˚c• Normal saline is recommended for diluent for reconstituting the vaccine. Reconstitute vaccine May be used up with in 3 hrs.• Dosage : Usual strength is 0.1mg in 0.1 ml volume. The dose to newborn aged below 4 weeks is .05ml•Administration :Injected vaccine intradermally using tuberculin syringe , site of injection should be just above the deltoid muscle

CONTRAINDICATIONS• BCG should not be given to patients suffering from generalised eczema, infective dermatosis, to those patient with a history of deficient immunity, Patient under immunosupressive treatment, and in pregnancy

DOTS (directly observed treatment, shortcourse), is the name given to the World Health Organization-recommended tuberculosis control strategy that combines five components: • Government commitment (including both political will at all levels, and establishing a centralized and prioritized system of TB monitoring, recording and training) •
DOTS

• Case detection by sputum smear microscopy Standardized treatment regimen directly observed by a healthcare worker or community health worker for at least the first two months • A regular drug supply • A standardized recording and reporting system that allows assessment of treatment result
DOTS helps in ……

The advantages of DOTS are
• Accuracy of TB diagnosis is more than doubled• Treatment success rate is up to 95 percent• Prevents the spread of the tuberculosis infection , thus reducing the incidence and prevalence of TB • Improves quality of health care and removes stigma associated with TB• Prevents failure of treatment and the emergence of MDR-TB by ensuring patient adherence and uninterrupted drug supply.

THANK YOU….