Embed Size (px)
DESCRIPTION
Urinary Tract Infections and Vesicoureteral reflux disease
Citation preview

Urinary Tract Infections in Children
BYRAMKUMAR.R

Introduction
• Urinary tract infections (UTI) are a common and important clinical problem in childhood.
• Upper urinary tract infections (ie, acute pyelonephritis) may lead to renal scarring, hypertension, and end-stage renal disease.
• Difficult on clinical grounds to distinguish cystitis from pyelonephritis, particularly in young children (those younger than 2 years)

Introduction
• Most UTIs are caused when bacteria infect the urinary tract, which is made up of the kidneys, ureters, bladder, and urethra.
• Each plays a role in removing liquid waste from the body. The kidneys filter the blood and produce urine; the ureters carry the urine from the kidneys to the bladder; and the bladder stores the urine until it is eliminated from the body through the urethra.
• An infection can occur anywhere along this tract, but the lower part — the urethra and bladder — is most commonly involved. This is called cystitis.
• If the infection travels up the ureters to the kidneys, it's called pyelonephritis and is usually more serious.

Prevalence
• The overall prevalence of UTI is approximately 7 percent in febrile infants.
• White children have a two- to four-fold higher prevalence of UTI than do black children.
• Girls have a two- to four-fold higher prevalence of UTI than do circumcised boys.
• White girls with a temperature of ≥39ºC have a UTI prevalence of 16 percent.

Prevalence
• Older children are more likely to present with urinary symptoms in association with a UTI than younger children.

Microbiology
• Escherichia coli is the most common bacterial cause of UTI (80%)
• Other gram-negative bacterial pathogens include Klebsiella, Proteus, Enterobacter, and Citrobacter.
• Gram-positive bacterial pathogens include Staphylococcus saprophyticus, Enterococcus, and, rarely, Staphylococcus aureus.

Microbiology
• Viruses (eg, adenovirus, enteroviruses) and fungi (eg, Candida spp, Aspergillus spp, Cryptococcus neoformans, endemic mycoses) are less common causes of UTI in children
• Viral UTI are usually limited to the lower urinary tract. • Risk factors for fungal UTI include immunosuppression
and long-term use of broad-spectrum antibiotic therapy, and indwelling urinary catheter

Pathogenesis
• The result of ascending infection. • Colonization of the periurethral area by
uropathogenic enteric pathogens is the first step in the development of a UTI.
• In E. Coli: pili, hair-like appendages on the cell surface aid in attaching to epithelium.
• In the kidney, the bacterial inoculum generates an intense inflammatory response, which may ultimately lead to renal scarring.

Risk Factors
• Boys < 1, Girls < 4 (Short urethra)• Uncircumcised boys• White children x4 > black children• Family history of UTI: Genetic factors• Urinary Obstruction: PUV, UPJ, myelomeningocele,
neurogenic bladder• Vesicoureteral reflux (VUR)• Sexual activity• Bladder catheterization.

VUR
• Vesicoureteral reflux (VUR) is the retrograde passage of urine from the bladder into the upper urinary tract.
• It is the most common urologic anomaly in children, occurring in approximately 1 percent of newborns, and as high as 30 to 45 percent of young children with UTI.

Pathogenesis
• Primary VUR, the most common form of reflux, is due to incompetent or inadequate closure of the ureterovesical junction (UVJ).
• Secondary VUR is a result of abnormally high pressure in the bladder that results in failure of the closure of the UVJ during bladder contraction. Secondary VUR is often associated with anatomic (eg, posterior urethral valves) or functional bladder obstruction

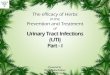
Grading
• Grade I — Reflux only fills the ureter without dilation.• Grade II — Reflux fills the ureter and the collecting system
without dilation.• Grade III — Reflux fills and mildly dilates the ureter and the
collecting system with mild blunting of the calyces.• Grade IV — Reflux fills and grossly dilates the ureter and the
collecting system with blunting of the calyces. Some tortunsity of the ureter is also present.
• Grade V — Massive reflux grossly dilates the collecting system. All the calyces are blunted with a loss of papillary impression and intrarenal reflux may be present. There is significant ureteral dilation and tortuosity.

Grading
Mild Moderate Severe

Risk Factors for Renal Scarring
• Recurrent febrile UTI • Delay in treatment of acute
infection• Dysfunctional elimination• Obstructive malformations• VUR

Clinical Presentation
• In young children (<2 yrs): Fever, vomiting, poor feeding, abdominal tenderness, irritability.
• Older Children: fever, urinary symptoms (dysuria, urgency, frequency, incontinence, macroscopic haematuria), and abdominal pain
• The constellation of fever, chills, and flank pain is suggestive of pyelonephritis in older children

History
• Chronic urinary symptoms — Incontinence, lack of proper stream, frequency, urgency, withholding maneuvers
• Chronic constipation • Previous UTI • Vesicoureteral reflux (VUR) • Previous undiagnosed febrile illnesses • Family history of frequent UTI, VUR, and other genitourinary
abnormalities • Antenatally diagnosed renal abnormality • Elevated blood pressure • Poor growth

Clinical Examination
• Documentation of blood pressure and temperature.• Growth parameters• Abdominal examination for tenderness or mass• Assessment of suprapubic and costovertebral
tenderness.• Examination of the external genitalia for anatomic
abnormalities (eg, phimosis or labial adhesions) and signs of vulvovaginitis, vaginal foreign body, sexually transmitted diseases (STDs)

• Evaluation of the lower back for signs of occult myelodysplasia (eg, midline pigmentation, lipoma, vascular lesion, sinus, tuft of hair), which may be associated with a neurogenic bladder.
• Evaluation for other sources of fever.• Urinalysis

Laboratory Investigations
• Urinalysis: Clean catch or suprapubic aspirate– WCC, RCC, Nitrites (E Coli): Sensitivity of 80%. – Urine Microscopy
• Urine Culture• FBC, U/E, CRP• Blood Culture• Lumbar Puncture in a febrile child < 3 months

Management
• Elimination of infection and prevention of urosepsis
• Prevention of recurrence and long-term complications including hypertension, renal scarring, and impaired renal growth and function
• Relief of acute symptoms (eg, fever, dysuria, frequency)

Hospitalization
• Age <3 months • Clinical urosepsis or potential bacteremia • Immunocompromised patient • Vomiting or inability to tolerate oral medication • Lack of adequate outpatient follow-up (eg, no
telephone, live far from hospital, etc.) • Failure to respond to outpatient therapy

Antibiotics
• Amoxicillin ( or Co-amoxiclav)• Gentamycin• Cefotaxime
• Children younger than 2 years and children with febrile or recurrent UTI are usually treated for 10 days

Duration of Therapy
• Children younger than 2 years and children with febrile or recurrent UTI are usually treated for 10 days
• TMP-SMX or nitrofurantoin may be initiated after completion of treatment and continued until the results of the imaging tests are available
• Children older than 2 years who are afebrile, and without abnormalities of the urinary tract or previous episodes of UTI are usually treated for 5 to 7 days; such children have a low risk of recurrence or complications

Imaging Studies
Routine imaging (RUS and MCUG) for:• Girls younger than 3 years of age with a first UTI
(children older than 3 years are more reliably able to verbalize urinary symptoms)
• Boys of any age with a first UTI• Children of any age with a febrile UTI• Children with recurrent UTI (if they have not been
imaged previously)• First UTI in a child of any age with a family history of
renal disease, abnormal voiding pattern, poor growth, hypertension

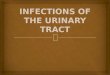
DMSA scan
• Renal scintigraphy using dimercaptosuccinic acid (DMSA) can be used to detect acute pyelonephritis and renal scarring in the acute and chronic settings, respectively
• DMSA is injected intravenously, and uptake by the kidney is measured two to four hours later. Areas of decreased uptake represent pyelonephritis or scarring.
• Scintigraphy at the time of an acute UTI provides information about the extent of renal parenchymal involvement.
• Most (>80 percent) children with moderate to severe VUR (grade III or higher) will have a positive DMSA scan.
• Some have advocated DMSA be used instead of a MCUG to identify children at higher risk for renal scarring.

MCUG

DMSA

Prognosis
• Recurrent UTI — Approximately 14 percent of children younger than 6 years with UTI have a subsequent UTI.
• Long-term sequelae :• Approximately 40 percent have VUR: 96 percent had VUR of grade I, II, or
III, which typically resolves spontaneously over time. • Renal scars (identified by DMSA scan) develop in approximately 8 percent
of patients overall, 15 percent of those who had abnormal DMSA scan at the time of diagnosis, and none of the children who had normal renal scans at the time of diagnosis.
• The long-term significance of scarring, as identified by DMSA, remains to be determined.
• Predicting which children with UTI will develop long-term sequelae remains difficult. The large majority of children with UTI have no long-term sequelae.