Embed Size (px)
DESCRIPTION
Seminar about the Wellness Program for Anxiety & depression. It covers a wide area of implementation...!!
Citation preview

PHINOJ K ABRAHAMI I N D M O T S T U D E N T
A L L I N D I A I N S T I T U T E O F P H Y S I C A L M E D I C I N E & R E H A B I L I T A T I O N ,
( A I I P M & R ) M U M B A I
Wellness program for Anxiety & Depression

2OverviewDefinition of Key TermsClinical DepressionClinical AnxietyImpact of Depression & Anxiety on Human
life: OT PerspectiveWellness Program for Depression &
Anxiety

3
Definitions of Key Terms
FearFear – is a response to a known, external,
definite, or non conflictual threat.
AnxietyAnxiety – is a response to threat that is
unknown, internal, vague, or conflictual.The main psychological difference b/w the 2 emotional
response is the suddenness of fear and the insidiousness of anxiety.

4
Key Terms Cont…
Depression Is an emotion charecterized
by “sadness,” crying, withdrawal from others, and feeling of in adequacy.
Intro to Psycho 7th edn, CT Morgan 1993
Resulting from a past experience

5Key Terms Cont…
Present ?
Avoidable ?
Yes No
Yes No
DANGER
Fear (meeting a Snake)
Anxiety(hearing hissing sound of Snake )
Depression(I will not escape from the Snake)

6
Key Terms Cont…
Anxiety
Fear
DepressionPTSD
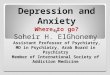
Future
Present
Past
Anxiety
Fear
DepressionPTSD

7Key Terms Cont…
Stress
Stress is a condition or feeling experienced when a person perceives that demands exceed the personal and social resources the individual is able to mobilize.
Richard S Lazarus This depends on how a person perceives, thinks, and
acts on external events or internal drives. Stressors: the situation/events which cause stress.

8
Cont…
Clinical Depression

9
Definition of Depression: DSM-IV-TR
Major depressive episodes: Affective disorders characterized by “sad” feelings & persistent problems in other areas of life.
Intro to Psycho 7th edn, CT Morgan 1993
A major depressive disorder occurs without a history of a manic, mixed, or hypo manic episode.
DSM-IV: one of the following must be present for at least two weeks:
Depressed mood Lack of pleasure (anhedonia)

10
Definitions
Other symptoms:Feelings of overwhelming sadness and/or fearBlunt affectLack of pleasureWeight gain or lossDisturbed sleep patternsPsychomotor agitation nearly every dayFatigue, mental or physical.

11
Cont.. Intense feelings of guilt, nervousness, helplessness,
hopelessness, isolation or anxiety
Cognitive problems: concentrating, keeping focus, poor
memory
Recurrent thoughts of death
Suicide attempt or a specific plan for committing suicide
A total of five symptoms must be present to diagnose a major
depressive disorder

12
Some Facts & Figures About Depression
Nearly 5-10% of persons in a community at a given time are in need of help for depression.
As much as 8-20% of persons carry the risk of developing depression during their lifetime.
The average age of the onset of major depression in between 20 and 40 years.
Women have higher rates of depression than men. Marital status: depression more common in persons
without close IP relationship / among Divorced single person
Race or ethnicity does not influence the prevalence of depression Ref : Conquering Depression: You can get out of the blues WHO

13
Causes 1. Life experiences & Environmental Stress
“Stressful life events more often precede first, rather than subsequent, episodes of mood disorders”
Life event most often associated with development of depression is losing a parent before age 11.
The environmental Stressor most often associated with the episode of depression is the loss of Spouse.

14
Causes Cont…
2. Personality Factors
No single personality trait or type uniquely predispose a person to depression
Person with certain personality disorder like OCD, histrionic & borderline – may be at grater risk.

15
Causes Cont…
•High frequencies of unpleasant un rewarding events
•Less hope & energy in activities / Social Interactions
• This, make them less rewarding to be around
• Thus others tends to avoid depressed people
• This deepens their depression
3. Social Interaction

16Causes Cont…4. Biological factors & Depression
There are four main biological factors that can increase a persons risk for depression Genetic factors Biochemical factors Alterations in hormonal regulation Sleep abnormalities.

17
Causes – Psychological Theories
1. Psychodynamic Theory According to this theory “depression is resulting from an
overly demanding super ego – one that sets standard too high for the person to live up to – and from early loss of attachment figures” Un realistic/achievable Goals – Edward Bibring Depressed people have lived for their lives for some one else
(principle, ideal, institution / individual) – Silvano Arieti Parents fails to give the child a positive sense of self esteem &
self cohesion – Heinz Kohut (Self Psychological Theory) Traumatic childhood events – Johm Bowlby Child victimized by a tormenting parent. – Edith Jacobson

18
Causes – Psychological Theories Cont…
2. Cognitive theory According to this theory depression results from
“specific cognitive distortions present in person susceptible to depression”
AARON BECK suggest a cognitive triad of depression that consists of Views about self – a negative self respect About the environment – a tendency to experience
the world as hostile & demanding About the future – the expectation of suffering &
failure.

19
Causes – Psychological Theories Cont…
3. Behavioral Theory Learned Helplessness : this theory connects depressive
phenomena to the experience of uncontrollable life events.
EX: Dog exposed to repetitive electric shocks from which they could not escape Reacted initially Then they reminded passively
According to Behavioral theory “Dog learned that outcomes were independent of response” so they had Cognitive Motivational deficit – not attempted to escape Emotional deficit – decreased reactivity.

20
Causes – Psychological Theories Cont…
Behavioral Theory cont…
In human depression, Uncontrollable stress events produce loss of self
esteem.Behavioral theory stresses that “improvement
of depression is dependent on the patients learning a sense of control & mastery of environment”

21
Types of Depressive Disorders
Major Depressive Disorder
Dysthymic Disorder
Minor Depressive disorder
Recurent Brief Depressive disorders
Full Unipolar Spectrum.

22
Depression; It’s not only a state of mind.
Emotional Symptoms Include: Physical Symptoms Include:
Sadness Vague aches and painsLoss of interest or pleasure HeadacheOverwhelmed Sleep disturbances
Anxiety Fatigue
Diminished ability to think or concentrate, indecisiveness Back pain
Excessive or inappropriate guilt Significant change in appetite resulting in weight loss or gain
Symptoms of Depression
Reference: American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition,Text Revision. 2000:345-356,489.

23
Depression – The Physical Presentation
In primary care, physical symptoms are often the chief complaint in depressed patients
In a New England Journal of Medicine study, 69% of diagnosed depressed patients reported unexplained physical symptoms as their chief compliant1
Reference: Simon GE, et al. N Engl J Med. 1999;341(18):1329-1335.

24
The Importance of Emotional and Physical Symptoms
• 76% of compliant depressed patients with lingering symptoms of depression relapsed within 10 months
94% of depressed patients who experienced lingering symptoms had mild to moderate physical symptoms1
Reference: Paykel ES, et al. Psychol Med. 1995;25:1171-1180.

25
Complications
Alcohol abuse Substance abuse Anxiety Heart disease and other medical conditions Work or school problems Family conflicts Relationship difficulties Social isolation Suicide

26
Clinical Anxiety Disorders

27
Anxiety DisordersA condition characterized by extreme, chronic anxiety
that disturbs mood, thought, behavior and/or physiological activity. www.psychiatric-disorders.com
Anxiety Disorders: DSM-IV-TR Panic Disorder Agoraphobia Social Phobia Specific Phobia Obessive Compulsive Disorder Generalized Anxiety Disorder (GAD) The most commonly diagnosed Separationa Anxiety Disorder

28
Diagnosis
To better differentiate between GAD and other anxiety or depressive disorders, 4 “first rank” and at least 1 “second rank” symptoms are needed
First Inability to relax, restlessness Fatigueability Exaggerated startle response Muscle tension

29
Diagnosis Cont…
First Cont… Sleep disturbances Difficulty in concentrating Irritability
Second Nausea or abdominal complaints Dry mouth Tachycardia Tremor

30
Epidemiology
Incidence & Prevalance National prevalence rates of Anxiety Neurosis
Median 18.5 ; Mode 11-70 Indian Journal of Community Medicine
Vol. 26, No. 4 (2001-10 - 2001-12)
Sex Women : 30.5 % life time prevalence Men : 19.2 % life prevalence
National Co-morbidity Study, USA

31Anxiety FactsMost common mental illness in the U.S. with 19 million
of the adult (ages 18-54) U.S. population affected. Anxiety is highly treatable (up to 90% of cases), but only
one-third of those who suffer from it receive treatmentPeople with an anxiety disorder are three-to-five times
more likely to go to the doctor and six times more likely to be hospitalized for psychiatric disorders than non-sufferers.
Depression often accompanies anxiety disorders Ref: 2003 Anxiety Disorders Association of America

32
Common CausesThere is no one cause for anxiety disorders. Several
factors can play a role Genetics Brain biochemistry Overactive "fight or flight" response
Can be caused by too much stress Life circumstances/experiances Personality
People who have low self-esteem and poor coping skills may be more prone
Certain drugs In very rare cases, a tumor of the adrenal gland
(pheochromocytoma) may be the cause of anxiety.

33
Causes – Psychological Theories
1. Psychoanalytic Theories Sigmund Freud distinguished two types of anxiety:
I. Traumatic – arising from the person being overwhelmed by stressors
II. Neurotic – anticipation of negative consequences that activates defensive processes
2. Behavioural Theory Postulate that anxiety, is a conditioned response to
a specific stimulus.

34
Causes – Psychological Theories Cont…
3. Existential Theories “…. Person experience feeling of living in a purposeless
universe“
4. Charles D. Spielberger’s State–Trait Anxiety Inventory (STAI) State Anxiety : Anxious personality Trait Anxiety : momentary anxiety to a stimulus

35
SymptomsAnxiety is an emotion often accompanied by
various physical symptoms, including: Twitching or trembling Muscle tension Headaches Sweating Dry mouth Difficulty swallowing Abdominal pain (may be the only symptom of stress
especially in a child)

36
Additional Symptoms
Dizziness Rapid or irregular heart rate Rapid breathing Diarrhea or frequent need to urinate Fatigue Irritability, including loss of your temper Sleeping difficulties and nightmares Decreased concentration Sexual problems

37
Recent Studies‘Freedom From Fear’ conducted a survey among 410 attendees during National Anxiety Disorders Screening Day on May 7, 2003. The results :
An increase in physical aches and pains is directly attributed to anxiety disorders and depression
60% of the respondents with undiagnosed medical conditions said that on days when they feel anxious or depressed, there is a moderate (41%) to severe (19%) change in their physical symptoms or aches and pains.

38
Recent Studies Cont…
These physical symptoms or aches and pains include Backaches (13%) Vague aches and pains (14%) Headaches (14%), Digestive pain (11%) Dizziness (8%).
50% of respondents with diagnosed medical conditions, such as arthritis, migraines, diabetes, heart and respiratory diseases, reported that on days when they feel anxious or depressed, there is a moderate (38%) to severe (12%) change in their physical symptoms or aches and pains.

39
Complication
Emotional Complication risk for depression Substance Abuse
Physical Complications Heart disease, and high blood pressure Sudden death from a heart attack or cardiac event. Gastrointestinal disorders Migraine and tension headaches Obesity as well as anorexia.

40
Vulnerable PeopleStudents
Symptoms of anxiety and symptoms of depression were prevalent in medical students (43% and 14%, respectively) and in humanities students (52% and 12%, respectively).
International Journal of Social Psychiatry, Vol. 54, No. 6, 494-501 (2008)
Main Causes: Improper Time management, Stress, Personal Demands, body image perception & acceptance, un healthy Competition etc..
Job losers & Job seekers A 2002 study at the University of Michigan found “that secondary
stressors of job loss such as financial strain and loss of personal control are the true culprits that lead to depression. The study also found that elevated levels of depression ‘may reduce the likelihood of reemployment.’”

41
Cont…Among workers
In Unorganized sectors out of 457 million workers in India, 395 million (93%) are employed in
the unorganized sectors like construction, agriculture, weaving and fishing and contribute to about 60% of national income.
About 7 % of the total work force is employed in the formal or organized sector
Suicides epidemic is high in this sector. In Organized Sector
Anxiety & Depression is because of Excessive Job demand Problems related to payment Un safe Job environment Job Dissatisfaction / Loosing Interest

42
Cont…Among Elderly
Prevalence of depression 19.8%. The elderly living in a nuclear family system were 4.3
times more likely to suffer from depression than those living in a joint family system
BMC Psychiatry 2007, 7:57doi:10.1186/1471-244X-7-57
Common causes: Changes within the family Chronic pain and illness Difficulty getting around Frustration with memory loss Loss of a spouse or close friend

43
Cont…Among People with Chronic Disabilities
The rate for depression occurring with other medical illnesses is quite high: Heart attack: 40%-65% Coronary artery disease (without heart attack): 18%-20% Parkinson’s disease: 40% Multiple sclerosis: 40% Stroke: 10%-27% Cancer: 25% Diabetes: 25% www.cchs.net/health/health-info/docs/2200/2282.asp?index=9288
Spinal Cord Injury: 22% - major depressive <2 months post injury (Krause, Bombardier and Carter, 2008), 11.4% after 1 yr. Krause et al. (2000)

44
Impact of Depression & Anxiety on Human life:
OT Perspective

45
Impact of Depression & Anxiety on Human life: OT Perspective“From an occupational therapy perspective, people
with depression (or anxiety) typically do not have the energy or drive to participate in the things that are important to them,”
Lisa Mahaffey, MS, OTR/L,
OT Evaluation
Model Of Human Occupation (MOHO) Gray Kielhofner
Uniform Terminology for Occupational Therapy 3ird edn
by the American Occupational Therapy Association (AOTA) 1994

46
Model Of Human Occupation (MOHO)
The Model of Human occupation seeks to explain the occupational functioning of person.
It focuses on how person choose, order, and perform in everyday occupational behavior.
This model also stresses the Motivation for mastery, control, personal effectiveness & the need of persons to maintain a positive self – image.

47
MOHO Conceptualize the Human being as an Open System

48
MOHO : Concepts
Knowledge of Self Experience
Decision Making
Physical SocialEnvironment

49
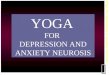
Volition
Habituation
Performance Capacity
Participation
Performance
Skill
Occupational Identity
Occupational Adaptation
Occupational Competence
Model of Human Occupation – (based on diagram by Gary Kielhofner)
MOHO : Person & Environment
Throughput Output Feedback s

50
Evaluation & Intervention Process using MOHO
Evaluation Process “…. Collect and use data to help clients understand
how their personal perceptions and subjective views lead to occupational performance actions and patterns. Gary Kielhofner
Therapeutic Intervention The process of self-maintenance and change is
supported by allowing the person to participate in freely chosen occupations in therapy
Gary Kielhofner

51
Case Study
The application of MOHO in the treatment of a patient with depression in Taiwan: A case study Methods:
Multiple Chinese version MOHO assessments were applied to her at initial stage. The therapeutic relationship with the patient was developed through the discussion of the results of the assessment and treatment planning.
Results:The patient obtained high scores on all symptom checklists and lower satisfaction of her lifestyle and performance initially. A set of meaningful occupations were constructed with her and the steps to apply to her life were negotiated. Before her discharge in a month, her daily living function, role performance, occupational identification and competence improved from previous state.
The MOHO is a useful theoretical base in the clinical assessment and treatment of patients with minor mental disorder.
Yun-Ling Chen et., al MOHO Center Taiwan, Nov 29, 2008

52
Uniform Terminology for Occupational Therapy
According to AOTA, uniform terminology for OT is “…. indented to provide a generic outline of the domains of concerns of Occupational Therapy and is designed to created common terminology for the profession & to capture the essence of OT for succinctly others”
Domains of Concerns are, Performance Areas Performance Components Performance Contexts

53
Uniform Terminology Cont…
Performance Areas Activities of Daily Living Work & productive activities Play & Leisure activities
Performance Components Sensory-motor components Cognitive Integration & Components Psychosocial Skills & Components
Performance Contexts Temporal Aspects Environmental Aspects

54
Wellness Program for Depression & Anxiety

55
“Every tomorrow has two handles.
We can take hold of it with the handle
of anxiety or the handle of faith.”
Henry Ward Beecher

56
Wellness
Wellness is a state of optimal well-being that is oriented toward maximizing an individual’s potential.
This is a life-long processDimensions: physical,
intellectual, emotional, social, spiritual, and environmental well-being.
How? - by adapting patterns of behavior

57
Wellness Program for Depression & Anxiety
Levels Intra – personal
Creative Self Coping Self Essential Self Physical Self General Feeling of Well-Being
Inter-personal Social Self

58
Creative Self
Thinking. Being mentally active and open-minded. The ability to be creative and experimental. Having a sense of curiosity. The ability to apply problem-solving strategies to social conflicts.
Emotions. Being aware of or in touch with your feelings. The ability to express appropriately positive and negative feelings.
Control. Beliefs about your competence, confidence, and personal mastery. Beliefs that you can usually achieve the goals you set out for yourself.
Work. Satisfaction with your work. Feeling that your skills are used appropriately. Feeling you can manage one’s workload. Feeling a sense of job security. Feeling appreciated in the work you do.
Positive Humor. Being able to laugh at your own mistakes. The ability to use humor to accomplish even serious tasks.

59
Coping Self
Leisure. Satisfaction with your time spent in leisure. Feeling that your skills are used appropriately.
Stress Management. On-going self-assessment of your coping resources. The ability to organize and manage resources such as time, energy, and setting limits.
Self-Worth. Accepting who and what you are, positive qualities along with imperfections. A sense of being genuine within yourself and with others.
Realistic Beliefs. Ability to process information and perceive reality accurately. The absence of persistent irrational beliefs and thoughts and need for perfection.

60
Essential Self
Spirituality. Personal beliefs and behaviors practiced as part of the recognition that we are more than the material aspects of mind and body. Belief in a higher power. Hope and optimism. Practice of worship, prayer, and/or meditation; purpose in life. Compassion for others. Moral values. Transcendence (a sense of oneness with the universe).
Gender Identity. Satisfaction with and feeling supported in one’s gender. Ability to be androgynous.
Cultural Identity. Satisfaction with and feeling supported in one’s cultural identity. Cultural assimilation.
Self-Care. Taking responsibility for one’s wellness through self-care and safety habits that are preventive in nature.

61
Physical Self
Nutrition. Eating a nutritionally balanced diet. Maintaining a normal weight (within 15% of the ideal).
Exercise. Engaging in sufficient physical activity through exercise or in your work to keep in good physical condition.

62
General Feeling of Well-Being
Perceived Wellness. The extent to which you believe you have achieved wellness in all areas, or total wellness. Your estimate of your total wellness.
Perceived Safety. The extent to which you believe you are safe in your home, neighborhood, and community, and the extent to which you feel safe from harm by terrorists.
Context. The extent to which your wellness is influenced, in a conscious manner, by individual, institutional, and global contexts, and the extent to which you are aware of and intentional in responding positively to changes in wellness over time.

63
Social Self
Friendship. Social relationships that involve a connection with others individually or in community. Having a capacity to trust others. Having empathy for others. Feeling understood by others.
Love. The ability to be intimate, trusting, self-disclosing with another. The ability to give as well as express affection with significant others and to accept others without conditions.

64
Implementation of Mental Wellness Program
Among, Students Job losers & Job Seekers Employers/workers
In Organized Sectors In Un organized sectors
Elderly People People with Disabilities

65
Students
Methods Creating a nurturing learning environment Identifying and assisting struggling students Counseling Promoting self-awareness Teaching skills for stress management Helping students promote personal health Activity Scheduling &Time management
Mayo Clin Proc December 2005;80(12):1613-1622

66
Job Losers
OT’s can teach/advice/ impliment the following things Stick to a schedule after losing job Spend time each day looking for work. Get plenty of exercise Enjoy with family during this time of uncertainty
Take your kids to the park or go on a walk. Volunteer at your kid's school.
Seek professional help.

67
Job seekersBy incorporating MOHO concepts, OT’s can do Prevocational
, Work capacity evaluation and can suggest suitable vocation for the person based on his personal factors
Aim: “Right Job for Right Person”Variables Include;
• VolitionPersonal CausationValuesInterests
• HabituationRolesHabits
• PerformanceSkills

68
Employers / workers
In Organized SectorsDiscuses & find out possible solution for the
problems of employers with the employee.Suggest a Nurturing working environment
Activity Scheduling & Time managementArranging Recreational Activities like trips, sports
or cultural activitiesEncourage Meditation, Yoga, Relaxation techniques
activitiesMusic Therapy

69
Employers / workers
In Un-organized Sectors
Social security
Social Support groups
Arranging Community Recreational Activities
Counseling Cells

70
Elderly People
Early Screening
Social supports
Family Support
Engaging In Fruitful/Productive activities
Spend More time for Recreational activities
Relaxation techniques, Yoga, Meditation, Music Therapy

71
People with Disabilities
CounselingBehavioral Technique : ModelingCBT : Biblio-therapy by reading; & Counseling, engaged in
meaningful activities Self help groups
EX: MSSI. AAAArranging Recreational Activities, Seminars, Gatherings etcPhysical Exercises programsGood NutritionSelf Management skillsRelaxation techniques, Yoga, Meditation, Music Therapy

72Thank You..