
Cancer Genetics and Cytogenetics 173 (2007) 17e22
A multicenter evaluation of comprehensive analysis of MLLtranslocations and fusion gene partners in acute leukemia
using the MLL FusionChip device
Christine J. Harrisona,*, Mike Griffithsb, Fıona Moormana, Susanne Schnittgerc,Jean-Michel Cayuelad, Sheila Shurtleffe, Enrico Gottardif, Gerlinde Mitterbauerg,
Dolores Colomerh, Eric Delabessei, Vincent Casterasj
aLeukaemia Research Cytogenetics Group, Cancer Sciences Division, University of Southampton, MP 822 Duthie Building,
Southampton General Hospital, Southampton SO16 6YD, UKbWest Midlands Regional Genetics Laboratory, Birmingham Women’s Hospital, Birmingham, UK
cDepartment of Hematology and Oncology, University Hospital Großhadern, Ludwig-Maximilians, University of Munich, Munich, GermanydINSERM U462, Hopital St. Louis, Paris, France
eDepartment of Pathology, St. Jude Children’s Research Hospital, Memphis, TNfDipartimento Scienze Cliniche e Biologiche, Azienda Ospedaliera San Luigi Gonzaga, Turin, Italy
gDepartment of Molecular Diagnostics, General Hospital of Vienna, Vienna, AustriahUnitat d’Hematopatologia Hospital Clinic, Barcelona, Spain
iLaboratoire Central d’Hematologie, Hopital Necker Enfants Malades, Paris, FrancejIpsogen Laboratories, Marseille, France
Received 7 August 2006; accepted 7 September 2006
Abstract Rearrangements of the MLL gene are significant in acute leukemia. Among the most frequenttranslocations are t(4;11)(q21;q23) and t(9;11)(p22;q23), which give rise to the MLL-AFF1 andMLL-MLLT3 fusion genes (alias MLL-AF4 and MLL-AF9) in acute lymphoblastic and acute mye-loid leukemia, respectively. Current evidence suggests that determining the MLL status of acuteleukemia, including precise identification of the partner gene, is important in defining appropriatetreatment. This underscores the need for accurate detection methods. A novel molecular diagnosticdevice, the MLL FusionChip, has been successfully used to identify MLL fusion gene translocationsin acute leukemia, including the precise breakpoint location. This study evaluated the performanceof the MLL FusionChip within a routine clinical environment, comprising nine centers worldwide,in the analysis of 21 control and 136 patient samples. It was shown that the assay allowed accuratedetection of the MLL fusion gene, regardless of the breakpoint location, and confirmed that thismultiplex approach was robust in a global multicenter trial. The MLL FusionChip was shown tobe superior to other detection methods. The type of molecular information provided by MLLFusionChip gave an indication of the appropriate primers to design for disease monitoring ofMLL patients following treatment. � 2007 Elsevier Inc. All rights reserved.
1. Introduction
Genetic rearrangements are recurrent features of the he-matological malignancies. It is well known that certain ofthese abnormalities define distinct clinical subgroups andare related to prognosis [1]. Rearrangements involving theMLL gene, located to chromosomal band 11q23, are one
* Corresponding author. Tel.: þ44-23-8079-8783; fax: þ44-23-8079-
6432.
E-mail address: [email protected] (C.J. Harrison).
0165-4608/07/$ e see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.cancergencyto.2006.09.006
important example [2]. They occur in acute myeloid leuke-mia (AML) and acute lymphoblastic leukemia (ALL), andare present at a significantly high incidence (~70%) ininfants and in the majority of patients with therapy-relatedleukemia induced by inhibitors of topoisomerase II [3e7].
At least 80 chromosomal regions have been identified astranslocation partners of the MLL gene, and more than 50 ofthe partner genes that form fusion transcripts with MLLhave been cloned [8,9]. The most frequently observed11q23 translocation partners are AFF1 (alias AF4) in t(4;11)(q21;q23) and MLLT3 (alias AF9) in t(9;11)(p22;q23),

18 C.J. Harrison et al. / Cancer Genetics and Cytogenetics 173 (2007) 17e22
accounting for ~40% and ~27%, respectively [10,11]. Thechromosomal band 19p13 is the breakpoint site of MLLT1(alias ENL), ELL, and SH3GL1 (alias EEN ); these threedistinct MLL partner genes collectively comprise ~12% of11q23 translocations [12].
Gene expression profiling studies have shown that acuteleukemia with rearrangements of MLL has a unique expres-sion signature, defining a distinct molecular entity of MLLleukemia [13]. Within this defined group, further subdivi-sions can be made dependent on the partner gene. Forexample, among the common translocations, an associationbetween the partner and subtype of leukemia has beendescribed: AFF1 (AF4) occurs almost exclusively in ALLand MLLT3 (AF9) occurs mainly in AML M5 [10,11].
It has been suggested that prognosis differs among sub-groups of patients with the different translocations.Although 11q23 rearrangements overall have been linked toa poor outcome in ALL [3,14] and an intermediate progno-sis in AML [15], improved survival has been reported forpatients with t(9;11) in childhood and adult AML [16,17].These observations imply biological differences betweenMLL subgroups defined by the partner gene. In associationwith evidence emerging from expression studies, subsets ofgenes that define MLL subgroups could provide importanttargets for molecularly based therapeutic strategies [18].Thus, systematic determination of the MLL status of acuteleukemia, including precise identification of the partnergene, is likely to become increasingly important in definingappropriate treatment, which emphasizes the need for accu-rate detection methods.
Current techniques may preclude detection of a signifi-cant number of patients with MLL rearrangements. South-ern blotting detects the occurrence of rearrangementswithin the MLL breakpoint cluster region. Chromosomalanalysis identifies the established MLL translocation part-ners, but cannot always confirm the involvement of MLLin 11q23 rearrangements (notably cryptic rearrangements,or those with a failed cytogenetic result) [19]. Fluorescencein situ hybridization (FISH) usually is reliable in detectingthe involvement of MLL, although on occasion certain rear-rangements are also cryptic by FISH; however, FISH doesnot identify the fusion partner without prior identificationof the translocation to select the appropriate DNA probes[20]. Reverse transcriptase-polymerase chain reaction(RT-PCR) provides sensitive detection of known partners,but has limited multiplexing capabilities [21].
To overcome some of these difficulties and provide anaccurate detection method for all cloned MLL partners,we have developed a novel molecular diagnostic device,the MLL FusionChip. This biochip has been successfullyused in the accurate detection, including precise breakpointlocation, of MLL fusion gene translocations in acute leuke-mia [22].
Our objectives were to verify the performance of theMLL FusionChip within a routine clinical laboratory envi-ronment, in such a way that the analytical characteristics
of the product matched or exceeded the values achievedin the research and development laboratories in which theproduct was manufactured.
2. Patients and methods
2.1. Patient samples and preparation
Samples of RNA, extracted from bone marrow or pe-ripheral blood, were obtained from patients with acute leu-kemia and chronic myeloid leukemia (CML) at diagnosis.The samples were processed within the coauthors’ labo-ratories, using their standard procedures of extraction,because the original evaluation had demonstrated successirrespective of the extraction method used. RNA concentra-tion and quality was also determined according to the prac-tice of the individual laboratories.
One microgram of total RNA was required for eachassay. The assays were run on stored samples, not takenspecifically for this study. Inclusion criteria were as follows:the MLL status was confirmed by one or more molecularmethods, FISH, or cytogenetics; the percentage of blastsin the sample exceeded 20% (which had been previouslydefined as well within the limit of detection for the MLLFusionChip); consent was given; the anonymity of patientswas respected; and optimal sample quality was confirmedprior to hybridization. The result of the assay was notintended to provide unique information, but rather toconfirm an already known diagnosis.
2.2. MLL FusionChip assay
The MLL FusionChip system provides, in a single step,comprehensive screening of all currently characterizedMLL fusion genes with precise identification of the fusiongene partner. It comprises a biochip manufactured froma microporous microarray membrane spotted with longoligonucleotides (50-mer) specific for the breakpoint re-gions within the MLL gene and its known partners. It ismanufactured as a kit containing five biochips and a setof reagents; a detailed protocol is provided.
MLL FusionChip methodology is based on the amplifica-tion and detection of fusion transcripts involving the MLLgene by reverse transcription (RT) of patient total RNA,followed by an anchored PCR (30 RACE [30 rapid amplifi-cation of cDNA ends] PCR) step and multiplexed detectionon the biochip. The biochip is designed to provide simpledirect visual reading of test results. A colorimetric reactionexposes the presence of an MLL translocation and the spe-cific partner gene involved in the formation of the fusiontranscript. The sample processing step ensures that all theMLL rearrangements included can be consistently detectedindependent of transcript length and position of the break-point involved in the fusion transcript. The exons adjacentto the breakpoints are also identified.

19C.J. Harrison et al. / Cancer Genetics and Cytogenetics 173 (2007) 17e22
Full details of the development of the system, the meth-odology, a list of the 32 MLL partner genes included on thebiochip, and method of interpretation of test results aregiven in Maroc et al. [22].
2.3. Study design
The present study was organized as a consortium, in-volving the cooperation of nine participating laboratoriesfrom Europe and the United States (as indicated in theauthor list), with each laboratory providing appropriatesamples in equal numbers from two patient cohorts:MLL-negative acute leukemia (eight samples) and thosewith MLL rearrangements (eight samples). The MLL-positive samples were to include equal numbers with MLL-AFF1 (four samples) and other MLL rearrangements (foursamples). MLL-AFF1 was chosen because of its relativelyhigh frequency among MLL translocations, to provide anaccurate assessment of the performance of the test forone specific translocation. Including other MLL transloca-tions ensured a relatively large number of sites, andprovided an indication of the specificity of the test.
The manipulators were required to be blind to the orig-inal diagnostic result. Ipsogen Laboratories (Marseille,France) provided each laboratory with the necessary MLLFusionChip kits and RNA from a control sample positivefor one rare translocation. Optimally, the study was to beconducted in four separate runs of five assays, includingsamples from one control, two MLL negative, one MLL-AFF1 positive, and one other MLL translocation. Twoobservers were required to independently read and reportthe results. The MLL FusionChip gives a qualitative result,so this was intended to assess the subjectivity of interpreta-tion of signal patterns and measure observer-to-observerreproducibility.
In those cases with a discrepancy between the originaldiagnostic result and the result from the MLL FusionChip,a specific RT-PCR test for the transcript detected by theMLL FusionChip was to be run using the product fromthe RT-PCR step.
3. Results
The study ran from June 2003 to February 2004, withfour late results received in January 2005. Table 1 showsthe distribution of samples among centers. Six of the ninecenters ran 21 control samples. In total, 136 patient sampleswere hybridized onto the MLL FusionChip; 49 gave nega-tive results, 23 were MLL-AFF1 positive, 45 showed otherrearrangements of MLL, and in 19 the results were non-interpretable.
Centers 2 and 3 shared the same samples, apart fromfour additional samples run by center 2. Two discrepancieswere observed between centers 2 and 3. A positive MLL-MLLT3 result found in one sample at center 2, concordantwith a cytogenetic result of t(9;11), gave a negative result at
center 3; on review, however, the MLL controls were weakand not quite complete, so this result from center 3 shouldbe reconsidered as uninterpretable. One MLL-MLLT10(alias MLL-AF10) sample found at center 3, concordantwith an insertion of chromosome 11 into chromosome 10,ins(10;11)(p?;q23), yielded a noninterpretable result incenter 2.
Noninterpretable results were seen in 19 samples fromfour centers, of which 11 came from a single center. Seven-teen of the noninterpretable samples were MLL negative byother diagnostic tests, one was MLLT10 positive (at onecenter, as noted in the preceding paragraph), and one wasAFF1 positive. The quality of the RNA had not been testedin all these samples with noninterpretable results prior tohybridization. One noninterpretable result from center 2was described by center 3 to have RNA of inadequate qual-ity for hybridization after the PCRII reaction (i.e., PCRomitting MgCl2 from the buffer). These observations em-phasize the importance of testing the RNA quality priorto hybridization. By contrast, two samples with positive re-sults from center 2 were not hybridized in center 3, becausethe samples were regarded in this laboratory as of inade-quate quality when assessed after the PCRII reaction.
Among those patients with available information ondisease type, the samples (with both positive and negativeresults) originated from acute leukemia across all agegroups. The distribution is shown in Table 2. The majorityof non-MLL rearranged samples originated from adults withAML. One center used a number of BCR-ABL positiveCML cases as negative controls, and another substitutedt(4;11) positive cell lines for MLL-AFF1 positive samples.There was no bias in distribution associated with these sam-ples with noninterpretable results; therefore, disease typewas not associated with the success of the hybridization.
Table 3 gives the distribution of interpretable resultsaccording to whether MLL was negative or positive. Theexpected MLL-MLLT7 (alias MLL-AFX1) positive result
Table 1
Distribution of samples in a multicenter evaluation of MLL translocations
and fusion gene partners in acute leukemia using the MLL FusionChip
device (Ipsogen, Marseille, France)
Center
no.a Controls
Total
patient
samples,
no. Negative
MLL-
AFF1
Other
MLL
Non-
interpretable
results
1 0 9 1 0 8 0
2 0 15 6 2 5 2
3 3 11 6 2 3 0
4 3 14 6 1 2 5
5 3 10 5 3 2 0
6 4 16 8 4 4 0
7 3 14 0 2 1 11
8 5 20 12 4 4 0
9 0 27 5 5 16 1
Total 21 136 49 23 45 19
a The nine centers were located in Austria (1), France (2), Germany
(1), Italy (1), Spain (1), the United Kingdom (2), and the United States (1).
20 C.J. Harrison et al. / Cancer Genetics and Cytogenetics 173 (2007) 17e22
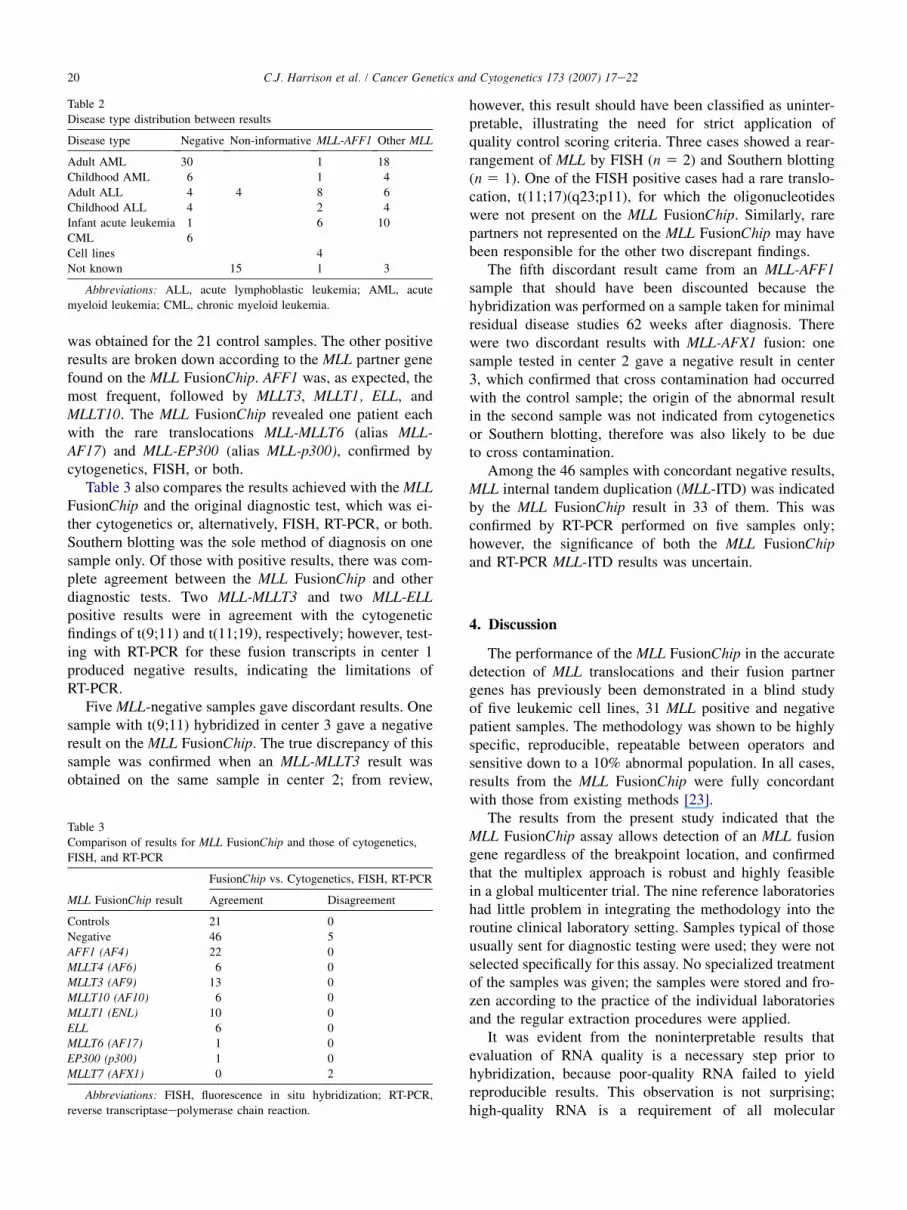
was obtained for the 21 control samples. The other positiveresults are broken down according to the MLL partner genefound on the MLL FusionChip. AFF1 was, as expected, themost frequent, followed by MLLT3, MLLT1, ELL, andMLLT10. The MLL FusionChip revealed one patient eachwith the rare translocations MLL-MLLT6 (alias MLL-AF17) and MLL-EP300 (alias MLL-p300), confirmed bycytogenetics, FISH, or both.
Table 3 also compares the results achieved with the MLLFusionChip and the original diagnostic test, which was ei-ther cytogenetics or, alternatively, FISH, RT-PCR, or both.Southern blotting was the sole method of diagnosis on onesample only. Of those with positive results, there was com-plete agreement between the MLL FusionChip and otherdiagnostic tests. Two MLL-MLLT3 and two MLL-ELLpositive results were in agreement with the cytogeneticfindings of t(9;11) and t(11;19), respectively; however, test-ing with RT-PCR for these fusion transcripts in center 1produced negative results, indicating the limitations ofRT-PCR.
Five MLL-negative samples gave discordant results. Onesample with t(9;11) hybridized in center 3 gave a negativeresult on the MLL FusionChip. The true discrepancy of thissample was confirmed when an MLL-MLLT3 result wasobtained on the same sample in center 2; from review,
Table 2
Disease type distribution between results
Disease type Negative Non-informative MLL-AFF1 Other MLL
Adult AML 30 1 18
Childhood AML 6 1 4
Adult ALL 4 4 8 6
Childhood ALL 4 2 4
Infant acute leukemia 1 6 10
CML 6
Cell lines 4
Not known 15 1 3
Abbreviations: ALL, acute lymphoblastic leukemia; AML, acute
myeloid leukemia; CML, chronic myeloid leukemia.
Table 3
Comparison of results for MLL FusionChip and those of cytogenetics,
FISH, and RT-PCR
FusionChip vs. Cytogenetics, FISH, RT-PCR
MLL FusionChip result Agreement Disagreement
Controls 21 0
Negative 46 5
AFF1 (AF4) 22 0
MLLT4 (AF6) 6 0
MLLT3 (AF9) 13 0
MLLT10 (AF10) 6 0
MLLT1 (ENL) 10 0
ELL 6 0
MLLT6 (AF17) 1 0
EP300 (p300) 1 0
MLLT7 (AFX1) 0 2
Abbreviations: FISH, fluorescence in situ hybridization; RT-PCR,
reverse transcriptaseepolymerase chain reaction.
however, this result should have been classified as uninter-pretable, illustrating the need for strict application ofquality control scoring criteria. Three cases showed a rear-rangement of MLL by FISH (n 5 2) and Southern blotting(n 5 1). One of the FISH positive cases had a rare translo-cation, t(11;17)(q23;p11), for which the oligonucleotideswere not present on the MLL FusionChip. Similarly, rarepartners not represented on the MLL FusionChip may havebeen responsible for the other two discrepant findings.
The fifth discordant result came from an MLL-AFF1sample that should have been discounted because thehybridization was performed on a sample taken for minimalresidual disease studies 62 weeks after diagnosis. Therewere two discordant results with MLL-AFX1 fusion: onesample tested in center 2 gave a negative result in center3, which confirmed that cross contamination had occurredwith the control sample; the origin of the abnormal resultin the second sample was not indicated from cytogeneticsor Southern blotting, therefore was also likely to be dueto cross contamination.
Among the 46 samples with concordant negative results,MLL internal tandem duplication (MLL-ITD) was indicatedby the MLL FusionChip result in 33 of them. This wasconfirmed by RT-PCR performed on five samples only;however, the significance of both the MLL FusionChipand RT-PCR MLL-ITD results was uncertain.
4. Discussion
The performance of the MLL FusionChip in the accuratedetection of MLL translocations and their fusion partnergenes has previously been demonstrated in a blind studyof five leukemic cell lines, 31 MLL positive and negativepatient samples. The methodology was shown to be highlyspecific, reproducible, repeatable between operators andsensitive down to a 10% abnormal population. In all cases,results from the MLL FusionChip were fully concordantwith those from existing methods [23].
The results from the present study indicated that theMLL FusionChip assay allows detection of an MLL fusiongene regardless of the breakpoint location, and confirmedthat the multiplex approach is robust and highly feasiblein a global multicenter trial. The nine reference laboratorieshad little problem in integrating the methodology into theroutine clinical laboratory setting. Samples typical of thoseusually sent for diagnostic testing were used; they were notselected specifically for this assay. No specialized treatmentof the samples was given; the samples were stored and fro-zen according to the practice of the individual laboratoriesand the regular extraction procedures were applied.
It was evident from the noninterpretable results thatevaluation of RNA quality is a necessary step prior tohybridization, because poor-quality RNA failed to yieldreproducible results. This observation is not surprising;high-quality RNA is a requirement of all molecular

21C.J. Harrison et al. / Cancer Genetics and Cytogenetics 173 (2007) 17e22
procedures. The results also confirm that the methodologyis superior to FISH and Southern blotting, which requiremultiple steps in the identification of the partner gene,and more reliable than RT-PCR in the detection of caseswith rare variant transcripts. At the same time, this typeof molecular information provides an indication of theappropriate primers to design for disease monitoring ofpatients following treatment [23].
One limitation, which had also been found in the originalevaluation, was that a positive result on the MLL FusionChipindicating MLL-ITD was not always correlated with a geno-mic internal duplication detected by RT-PCR. Previous stud-ies have shown that splicing of MLL is extremely complex,and several abnormally spliced MLL transcripts have beendescribed in both malignant and normal tissue [24,25]. Inthese misspliced products, MLL exons are joined in aberrantgenomic orientation (exon scrambling) and are not the resultof exon duplication. Standard RT-PCR may also be unreli-able for the detection of MLL-ITD, because it is unlikely tobe sensitive enough to detect transcriptome only missplicingevents. MLL FusionChip results indicating MLL-ITD willtherefore require quantitative RT-PCR or long range genomicPCR for confirmation before they can be regarded as genuine.The ability of the MLL FusionChip to detect backgroundMLL-ITD missplicing events in the transcriptome, whichare not present in the genome, demonstrates the relativelyhigh sensitivity of the MLL FusionChip.
There is growing consensus that a method to systemati-cally screen all acute leukemia subtypes is required: toidentify the MLL partners; to determine the true value ofthe partners in risk stratification; and to engender new intra-cellular therapeutic technologies. Fusion proteins anddownstream gene products are potential points of interven-tion in leukemia patient treatment, and some emergingmolecular-based technologies for targeting chromosomaltranslocation products have been proposed [26]. The multi-plex approach of MLL FusionChip has proved its worth andhas confirmed that molecular strategies such as this maycontribute to new insights into diagnosis and follow-up ofpatients with MLL rearrangements.
Acknowledgments
The authors are grateful for the expert technical assis-tance of Lisa James, Susanna Akiki, and Helen Worley.
References
[1] Harrison CJ. The management of patients with leukaemia: the role of
cytogenetics in this molecular era. Br J Haematol 2000;108:19e30.
[2] Secker-Walker LM, European 11q23 Workshop Participants. General
Report on the European Union Concerted Action Workshop on
11q23, London, UK, May 1997. Leukemia 1998;12:776e8.
[3] Pui CH, Gaynon PS, Boyett JM, Chessells JM, Baruchel A,
Kamps W, Silverman LB, Biondi A, Harms DO, Vilmer E,
Schrappe M, Camitta B. Outcome of treatment in childhood acute
lymphoblastic leukaemia with rearrangements of the 11q23 chromo-
somal region. Lancet 2002;359:1909e15.
[4] Hayette S, Tigaud I, Maguer-Satta V, Bartholin L, Thomas X,
Charrin C, Gadoux M, Magaud JP, Rimokh R. Recurrent involvement
of the MLL gene in adult T-lineage acute lymphoblastic leukemia.
Blood 2002;99:4647e9.
[5] Biondi A, Cimino G, Pieters R, Pui CH. Biological and therapeutic
aspects of infant leukemia. Blood 2000;96:24e33.
[6] Bloomfield CD, Archer KJ, Mrozek K, Lillington DM, Kaneko Y,
Head DR, Dal Cin P, Raimondi SC. 11q23 balanced chromosome ab-
errations in treatment-related myelodysplastic syndromes and acute
leukemia: report from an international workshop. Genes Chromo-
somes Cancer 2002;33:362e78.
[7] Dimartino JF, Cleary ML. MLL rearrangements in haematological
malignancies: lessons from clinical and biological studies. Br J
Haematol 1999;106:614e26.
[8] Bernard OA, Berger R. Molecular basis of 11q23 rearrangements in
hematopoietic malignant proliferations. Genes Chromosomes Cancer
1995;13:75e85.
[9] Huret JL, Dessen P, Bernheim A. An atlas of chromosomes in hema-
tological malignancies. Example: 11q23 and MLL partners. Leuke-
mia 2001;15:987e9.
[10] Swansbury GJ, Slater R, Bain BJ, Moorman AV, Secker-Walker LM,
European 11q23 Workshop participants. Hematological malignancies
with t(9;11)(p21-22;q23): a laboratory and clinical study of 125
cases. Leukemia 1998;12:792e800.
[11] Johansson B, Moorman AV, Haas OA, Watmore AE, Cheung KL,
Swanton S, Secker-Walker LM, European 11q23 Workshop partici-
pants. Hematologic malignancies with t(4;11)(q21;q23): a cytoge-
netic, morphologic, immunophenotypic and clinical study of 183
cases. Leukemia 1998;12:779e87.
[12] Moorman AV, Hagemeijer A, Charrin C, Rieder H, Secker-
Walker LM, European 11q23 Workshop participants. The transloca-
tions, t(11;19)(q23;p13.1) and t(11;19)(q23;p13.3): a cytogenetic
and clinical profile of 53 patients. Leukemia 1998;12:805e10.
[13] Armstrong SA, Staunton JE, Silverman LB, Pieters R, den Boer ML,
Minden MD, Sallan SE, Lander ES, Golub TR, Korsmeyer SJ. MLL
translocations specify a distinct gene expression profile that distin-
guishes a unique leukemia. Nat Genet 2002;30:41e7.
[14] Pui CH, Behm FG, Downing JR, Hancock ML, Shurtleff SA,
Ribeiro RC, Head DR, Mahmoud HH, Sandlund JT, Furman WL.
11q23/MLL rearrangement confers a poor prognosis in infants with
acute lymphoblastic leukemia. J Clin Oncol 1994;12:909e15.
[15] Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C,
Harrison G, Rees J, Hann I, Stevens R, Burnett A, Goldstone A, Med-
ical Research Council Adult and Children’s Leukaemia Working
Parties. The importance of diagnostic cytogenetics on outcome in
AML: analysis of 1,612 patients entered into the MRC AML10 trial.
Blood 1998;92:2322e33.
[16] Rubnitz JE, Raimondi SC, Tong X, Srivastava DK, Razzouk BI,
Shurtleff SA, Downing JR, Pui CH, Ribeiro RC, Behm FG. Favorable
impact of the t(9;11) in childhood acute myeloid leukemia. J Clin
Oncol 2002;20:2302e9.
[17] Martinez-Climent JA, Espinosa R 3rd, Thirman MJ, le Beau M,
Rowley JD. Abnormalities of chromosome band 11q23 and the
MLL gene in pediatric myelomonocytic and monoblastic leukemias:
identification of the t(9;11) as an indicator of long survival. J Pediatr
Hematol Oncol 1995;17:277e83.
[18] Ayton PM, Cleary ML. Molecular mechanisms of leukemogenesis
mediated by MLL fusion proteins. Oncogene 2001;20. 5695e07.
[19] Harrison CJ, Moorman AV, Barber KE, Broadfield ZJ, Cheung KL,
Harris RL, Jalali GR, Robinson HM, Strefford JC, Stewart A,
Wright S, Griffiths M, Ross FM, Harewood L, Martineau M. Inter-
phase molecular cytogenetic screening for chromosomal abnormali-
ties of prognostic significance in childhood acute lymphoblastic
leukaemia: a UK Cancer Cytogenetics Group Study. Br J Haematol
2005;129:520e30.

22 C.J. Harrison et al. / Cancer Genetics and Cytogenetics 173 (2007) 17e22
[20] Cuthbert G, Thompson K, Breese G, McCullough S, Bown N. Sensi-
tivity of FISH in detection of MLL gene rearrangements. Genes Chro-
mosomes Cancer 2000;29:180e5.
[21] Pallisgaard N, Hokland P, Riishoj DC, Pedersen B, Jorgensen P. Mul-
tiplex reverse transcription-polymerase chain reaction for simulta-
neous screening of 29 translocations and chromosomal aberrations
in acute leukemia. Blood 1998;92:574e88.
[22] Maroc N, Morel A, Beillard E, De La Chapelle AL, Fund X,
Mozziconacci MJ, Dupont M, Cayuela JM, Gabert J, Koki A, Fert V,
Hermitte F. A diagnostic biochip for the comprehensive analysis of
MLL translocations in acute leukemia. Leukemia 2004;18:1522e30.
[23] Gabert J, Beillard E, van der Velden VH, Bi W, Grimwade D,
Pallisgaard N, Barbany G, Cazzaniga G, Cayuela JM, Cave H,
Pane F, Aerts JL, De Micheli D, Thirion X, Pradel V, Gonzalez M,
Viehmann S, Malec M, Saglio G, van Dongen JJ. Standardization
and quality control studies of ‘real-time’ quantitative reverse
transcriptase polymerase chain reaction of fusion gene transcripts
for residual disease detection in leukemia: a Europe Against Cancer
program. Leukemia 2003;17:2318e57.
[24] Caldas C, So CW, MacGregor A, Ford AM, McDonald B, Chan LC,
Wiedemann LM. Exon scrambling of MLL transcripts occur com-
monly and mimic partial genomic duplication of the gene. Gene
1998;208:167e76.
[25] Nam DK, Honoki K, Yu M, Yunis JJ. Alternative RNA splicing of the
MLL gene in normal and malignant cells. Gene 1996;178:169e75.
[26] Rabbitts TH, Stocks MR. Chromosomal translocation products
engender new intracellular therapeutic technologies. [Commentary].
Nat Med 2003;9:383e6.
Recommended

















