
Health Policy 71 (2005) 243–253
Facilitators and barriers in the implementation of the meetingcentres model for people with dementia and their carers
Franka J.M. Meiland∗, Rose-Marie Droes, Jacomine de Lange,Myrra J.F.J. Vernooij-Dassen
V U Medical Center, Department of Psychiatry, EMGO Institute, Valeriusplein 9, 1075 BG Amsterdam, The Netherlands
Abstract
The implementation of care innovations that have been proven effective is not matter-of-course. In this study, we tracedfacilitating and impeding factors in the implementation of thirteen meeting centres for people with dementia and their carersin five different regions in The Netherlands. To guide the data collection and analyses, a theoretical model was developedthat distinguishes different phases of implementation, and factors at the level of characteristics of the innovation and otherpreconditions. Qualitative methods were used, including interviews with 23 key figures and other written materials gathered.The interview data were double coded and analyzed, using the computer programme NVivo. Several factors proved to playa facilitating role in all phases of implementation, for example: motivated people, financial resources, continuous and variedPR-activities, and cooperation between organizations. Other important facilitating characteristics of the meeting centres were:the surplus value of the integrated support programme as compared to the local support offer, and the fact that several centres werea mentationg©
K
1
tmts
f
en-a-
es-giesor
reffec-tivegiesthe
0
lready available as an example for new initiators. The findings were used, among other things, to develop an impleuide, to facilitate the implementation of meeting centres.2004 Elsevier Ireland Ltd. All rights reserved.
eywords:Adaptive implementation; Impediments; Facilitators; Dementia; Carers; Support programme
. Introduction
Research showing that an innovation is effective andhe people involved are satisfied with it, does not auto-atically imply its large-scale implementation. That
akes more than writing about positive research re-ults. The innovation will have to be implemented.
∗ Corresponding author. Tel.: +31 20 5736454;ax: +31 20 5736687.
Some innovations benefit from adaptive implemtation [1], which takes into account the local sitution, to which the innovation is tuned and, if necsary, adapted. Which are the most effective stratein the implementation of innovations is not alwaysimmediately clear[2–4]. Various systematic literatureviews show that the strategies that are proven etive in one study are not necessarily proven effecin another. Furthermore, the effectiveness of strateturns out to depend on the type of innovation and
168-8510/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.healthpol.2004.08.011

244 F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253
phase in the implementation process. Multiple (multi-faceted) strategies that take into account facilitators andbarriers in implementation, are expected to be the mosteffective strategies[2,5]. Gaining insight into facilitat-ing and impeding factors in implementation is thereforeconsidered an important step in the process of effectiveimplementation.
In the study that is reported on in this article, wetraced facilitating and impeding factors in the adaptiveimplementation of the meeting centres programme tosupport people with dementia and their carers. Thissupport programme was developed in 1992–1994[6]and it was proven effective in a controlled study in1994–1996[7]. The present study was part of an ex-tensive multi-centre study into the preconditions ofsuccessful implementation of meeting centres in TheNetherlands[8]. To guide the data collection and anal-yses, a theoretical search model was developed[9] onthe basis of a survey of the literature, previous experi-ences with setting up meeting centres and informationfrom experts that were consulted (seeFig. 1). With thismodel, we investigated which characteristics of the in-novation and other preconditions either facilitated orimpeded the implementation of the meeting centres,and which factors at the micro, meso and macro levelsof the successive phases of the implementation processhad facilitated or impeded the implementation. The re-sults will be used to compile an implementation guide
ating a
to facilitate the nationwide implementation of meetingcentres and its evaluation.
2. Research method
2.1. Setting
The study was conducted in the period March 2000to March 2003 in 13 meeting centres, located in fiveregions in The Netherlands. Five meeting centres werealready operational at the start of the study, five centresstarted during the study, and three centres had been dis-continued at the start of the study. The meeting centreswere located mainly in community centres and centresfor the elderly; other meeting centres were located ina church annex, a converted old people’s flat, and in awelfare centre in a home for the elderly.
2.2. The intervention
Meeting centres offer an integrated support pro-gramme for people with mild to moderately severedementia who live at home and their carers that isbased on the adaptation coping model[10]. The sup-port programme for the people with dementia consistsof a social club (three days a week); informative meet-ings and ongoing discussion groups for the carers;
Fig. 1. Theoretical model for tracing facilit
nd impeding factors in adaptive implementation.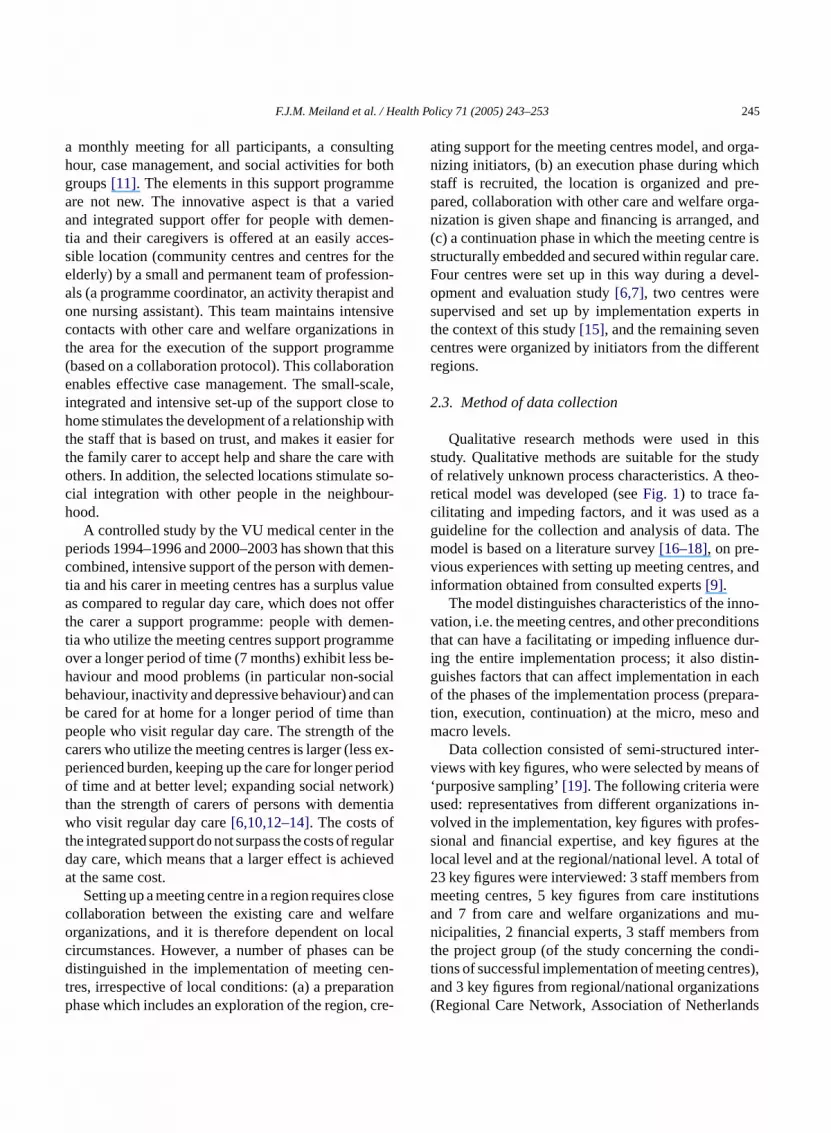
F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253 245
a monthly meeting for all participants, a consultinghour, case management, and social activities for bothgroups[11]. The elements in this support programmeare not new. The innovative aspect is that a variedand integrated support offer for people with demen-tia and their caregivers is offered at an easily acces-sible location (community centres and centres for theelderly) by a small and permanent team of profession-als (a programme coordinator, an activity therapist andone nursing assistant). This team maintains intensivecontacts with other care and welfare organizations inthe area for the execution of the support programme(based on a collaboration protocol). This collaborationenables effective case management. The small-scale,integrated and intensive set-up of the support close tohome stimulates the development of a relationship withthe staff that is based on trust, and makes it easier forthe family carer to accept help and share the care withothers. In addition, the selected locations stimulate so-cial integration with other people in the neighbour-hood.
A controlled study by the VU medical center in theperiods 1994–1996 and 2000–2003 has shown that thiscombined, intensive support of the person with demen-tia and his carer in meeting centres has a surplus valueas compared to regular day care, which does not offerthe carer a support programme: people with demen-tia who utilize the meeting centres support programmeover a longer period of time (7 months) exhibit less be-haviour and mood problems (in particular non-socialb canb hanp thec s ex-p riodo rk)t ntiaw ft gulard eveda
losec lfareo ocalc n bed en-t tionp cre-
ating support for the meeting centres model, and orga-nizing initiators, (b) an execution phase during whichstaff is recruited, the location is organized and pre-pared, collaboration with other care and welfare orga-nization is given shape and financing is arranged, and(c) a continuation phase in which the meeting centre isstructurally embedded and secured within regular care.Four centres were set up in this way during a devel-opment and evaluation study[6,7], two centres weresupervised and set up by implementation experts inthe context of this study[15], and the remaining sevencentres were organized by initiators from the differentregions.
2.3. Method of data collection
Qualitative research methods were used in thisstudy. Qualitative methods are suitable for the studyof relatively unknown process characteristics. A theo-retical model was developed (seeFig. 1) to trace fa-cilitating and impeding factors, and it was used as aguideline for the collection and analysis of data. Themodel is based on a literature survey[16–18], on pre-vious experiences with setting up meeting centres, andinformation obtained from consulted experts[9].
The model distinguishes characteristics of the inno-vation, i.e. the meeting centres, and other preconditionsthat can have a facilitating or impeding influence dur-ing the entire implementation process; it also distin-guishes factors that can affect implementation in eacho para-t andm
ter-v s of‘ eu s in-v es-s t thel l of2 romm ionsa mu-n omt ndi-t res),a ions( nds
ehaviour, inactivity and depressive behaviour) ande cared for at home for a longer period of time teople who visit regular day care. The strength ofarers who utilize the meeting centres is larger (leserienced burden, keeping up the care for longer pef time and at better level; expanding social netwo
han the strength of carers of persons with demeho visit regular day care[6,10,12–14]. The costs o
he integrated support do not surpass the costs of reay care, which means that a larger effect is achit the same cost.
Setting up a meeting centre in a region requires collaboration between the existing care and werganizations, and it is therefore dependent on lircumstances. However, a number of phases caistinguished in the implementation of meeting c
res, irrespective of local conditions: (a) a preparahase which includes an exploration of the region,
f the phases of the implementation process (preion, execution, continuation) at the micro, mesoacro levels.Data collection consisted of semi-structured in
iews with key figures, who were selected by meanpurposive sampling’[19]. The following criteria wersed: representatives from different organizationolved in the implementation, key figures with profional and financial expertise, and key figures aocal level and at the regional/national level. A tota3 key figures were interviewed: 3 staff members feeting centres, 5 key figures from care institutnd 7 from care and welfare organizations andicipalities, 2 financial experts, 3 staff members fr
he project group (of the study concerning the coions of successful implementation of meeting centnd 3 key figures from regional/national organizatRegional Care Network, Association of Netherla

246 F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253
Municipalities, Alzheimer Netherlands Foundation).The questions in the interview were derived fromthe theoretical model mentioned above, and modifiedfor the various key figures, depending on their areaof expertise and involvement in the implementationprocess.
The two implementation experts from the studygroup kept a structured log in which the implementa-tion process was recorded in detail. Furthermore, writ-ten material was obtained from the various meetingcentres, such as minutes, annual reports and projectreports.
2.4. Analysis
On average, the interviews lasted 80 min and theywere typed out verbatim and entered into the qualitativecomputer programme NUD*ISTVivo[20]. The inter-views were coded by two assessors (FM and RD, JdL orMV). They assigned key words to extracts from the textwith the aid of the theoretical model described above,which had been used to compile a detailed checklistof subjects that might contain facilitating or impedingfactors. For each of the extracts, the assessors indi-cated whether they observed any facilitating or imped-ing factors. In case of doubt, this was also mentioned.The coding of the first interviews was discussed in greatdetail, which resulted in a sharpening of the key words.Subsequently, all codes assigned by the assessors wereincorporated in the computer programme. Only whena re thec inter-v es tob
ex-t ractsbr d fa-c thei fa-c thei sultsw em-b them ma-t thew jectr
3. Results
3.1. Influencing factors and preconditions
3.1.1. Characteristics of the innovationAn obvious surplus valueas compared to the local
support offer clearly facilitated the implementation ofmeeting centres. For example, the meeting centre is anaddition to the care provision because it focuses on peo-ple with mild to moderately severe dementia who liveat home as well as their carers. Some type of supportwas frequently present in a region, but the combinationof the fragmented support offer for this target groupwas considered an improvement by key figures fromhome care, nursing homes and welfare organizations.The absence of any gaps in the existing offer would im-pede the implementation of a meeting centre. Some ofthe interviewed key figures (from a municipality, a careorganisation and a health insurance company) felt thatthe increasing number of initiatives concerning sup-port for people with dementia and their carers left littleroom for a meeting centre in their region. Another im-peding factor was the failure to recognize the surplusvalue of a meeting centre, despite existing gaps in theoffer.
In the meeting centre model collaboration with otherorganizations is a key issue, as is asound tuning tothe local support offer. This was also a facilitatingfactor. A lack of (good) cooperation with local orga-nizations could generate resistance in those organiza-t ssi-b ’sh an-ai off icesf arei tingc thers resa ouldf en-e re-d In thew eo( aidi trew
ssessors disagreed or codes were unclear, weodes discussed again for the assessment of newiews until consensus was reached about the code entered.
The next step in the analysis was to inventoryracts for each key word, and analyze these exty using the continuous comparison method[21]. Theesults were summarized in matrices that reflecteilitating and impeding factors of characteristics ofnnovation and other preconditions, as well as theilitating and impeding factors for each phase ofmplementation process. These analyses and reere discussed in the project group by four mers (JdL, MV, RD and FM). The relevance ofaterial was checked by consulting several infor
ion sources and comparing interview data withritten materials such as minutes, logs and pro
eports[22].
ions. Another facilitating characteristic was acceility. Meeting centresare more in line with peopleabitsthan institutionalized care, according to a mger from a care organization. Furthermore,they aren line with the present attention for the supportamily carers and the increasing demand for servor the growing numbers of elderly people (whon need of assistance/care). The arrival of a meeentre can help overcome waiting periods for oervices. Finally, havingexamples of meeting centvailableproved an advantage, because people c
orm a clear image of the model and they could bfit from available materials and expertise, whichuced the time needed to set up a meeting centre.ords of one initiator: “the initiators found the vid
on the meeting centres) very illuminating and st had improved their idea of what a meeting cenas”.

F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253 247
3.1.2. Time and other operational preconditionsInitially, it takes a lot of time to explore a region,
get acquainted with the care and welfare organizationsand networks, and to create support.Not taking enoughtime to do this had an impeding effect. However, join-ing an existing facility such as a day care project thatwas transformed into a meeting centre, could save a lotof time. Another facilitator was atransparent projectplan. Linking scientific researchto the implementa-tion process also facilitated implementation because itinspired confidence in the participants that potentialbottlenecks would be demonstrated and improved.
3.1.3. Human and financial resourcesAccording to most of the intervieweesenthusiasm
on the part of the various parties involved (key figures,organizations, initiators, staff) proved to be an impor-tant facilitating factor in implementation. They man-aged to put the implementation of meeting centres onthe agenda time and again, and give shape to the supportprogramme. This effect was enhanced if a staff mem-ber (or implementation expert) who could start prepara-tions, was hired at an early stage. All of the intervieweesconsideredfinancial resourcesimportant. Funds madeavailable by organizations to the initiative facilitatedimplementation. The advantage of transforming an ex-isting facility into a meeting centre was the presence ofsome structural funding. If parties involved expectedfinancing problems, the idea of setting up a meetingcentre would get a noncommittal reaction.
3ere
c n-t up-p nceoag ouldh heywt dd ec -t pts.I licyor ob-
lem is that everybody then starts reinventing the wheel,and that is not nearly as successful as implementing aproven concept”.
3.2. Facilitating and impeding factors in thedifferent phases of the implementation process
3.2.1. Preparation phase3.2.1.1. Micro level. Enthusiastic andactive initiatorswho were willing to take on the responsibility of run-ning a meeting centre had a facilitating effect. One ini-tiator in a welfare organization knew of the meetingcentres and had spent a day there: “we were totally en-thusiastic (. . .) we talked a lot (. . .) read reports andstudied the research results, which were very positive.So then we thought we should do the same thing here.And we started to adapt the model to our situation”.The interviews also showed thatassessing the need fora meeting centre in the regionat an early stage, forexample by means of a survey among potential par-ticipants, had a facilitating effect. Although a surveydid not guarantee the final number of participants, itprovided a better indication than estimates by care andwelfare workers. In two of the regions, attendance wasvery low, despite the fact that care and welfare workershad assessed this need to be high. Perhaps the taboo onthe subject of dementia caused this.
In the preparation phase quickly finding anaccessi-ble location, with sufficient facilities and room to housea meeting centre, also proved to facilitate implementa-t ionh cen-t e ona clubi t thate ntresf m-p ionq nots hereo up,o withd wasa e toa ga-n asi -p to
.1.4. Organizational conditionsOrganizations that facilitated implementation w
haracterized by:a vision in line with the meeting ceres model(for example regarding the method of sorting the target group, and regarding the importaf collaboration between various organizations),beingctive in care networksandtaking initiativeswith re-ard to care innovations. However, organizations cave an impeding influence on implementation if tere afraid the meeting centre would meancompeti-ion for their own facility or its financing, or if they haifferent visions and financing structures. Resistancould also occur if the region was generallyconservaive, or people preferred to develop their own concen the words of one care manager: “Managers, pofficials, they like to do their own doctoring, (. . .) thatesults in much more intrinsic motivation. The pr
ion. It was an advantage if the initiating organizatad a building that could be used as a meeting
re. The large demands the meeting centres makvailable space (for example because the social
s generally open three days a week), and the facxisting locations (such as community centres, ceor the elderly) usually have a full programme, colicated finding a suitable location. Finding a locatuickly was not an easy task. Many locations wereuitable for a variety of reasons: high costs, atmospf the building was not appropriate for the target gror other users would not accept a group of peopleementia. Of course, not finding a suitable locationproblem. In one region the initiators had to movmore distant location. An initiator from a care orization: “It was well appointed, beautiful, but it w
n neighbourhood X (. . .). You would be taking peole out of their own neighbourhood to bring them

248 F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253
neighbourhood X. And it was on the grounds of a homefor the elderly. And I think that is just too much of ahurdle for many people. Not easily accessible. Not likehere (a meeting centre in the middle of a neighbour-hood where many elderly people live), people just popin here”.
3.2.1.2. Meso level. Constructive collaboration be-tween care and welfare organizationsat the local levelhad a facilitating effect. Sometimes this collabora-tion had to be developed, in other regions an activenetwork was already in place. In some cases, coopera-tion within the group of initiators who made the prepa-rations for the meeting centre was also difficult, forexample because responsibilities had not been clearlydefined which resulted in people waiting to see whatwould happen. In some cases, the cultures of the careorganizations and the welfare organizations were sodifferent that collaboration remained difficult and theprocess was very time-consuming. In the words of oneof the interviewed initiators from a care organization:“we also had much to learn from each other (. . .) thatin the care sector you start from diagnosis or indica-tion whereas welfare said (. . .) people just walk in,and obviously they don’t come here without a reason.”The group of initiators did not always consist of manycollaborating organizations. Sometimes a small groupwas successful, provided its members were enthusias-tic, tenacious, decisive and energetic. In that situation,the decision was sometimes made to inform other orga-n voidf them toryr or-g tions.
i am , anda ple,w min-i cts.I o bet thep el-f e thes wel-f oret ike
the meeting centres to be financed in the interim. Thepossibility to negotiate about part of the financing, forexample municipal authorities would take care of ac-commodation costs by providing a space, had a facili-tating effect. Other facilitating strategies for obtainingfinancing were: start announcing the plan at an earlystage, demonstrating the meeting centre is widely sup-ported, and clarifying its surplus value.
3.2.1.3. Macro level.Preparations were facilitated ifthe organizations involvedwere abreast of the lawsand regulationsconcerning financing from the careand welfare sectors. For example, the government hadset up various incentive schemes, such as ‘waiting listsubsidy scheme’, ‘tailor-made care funds’, and the ‘in-formal care subsidy scheme’. In addition the meetingcentres can appeal to structural funds, such as those forday care. In The Netherlands this is done through theAWBZ (the Exceptional Medical Expenses Act).
3.2.2. Execution phase3.2.2.1. Micro level.The following factors proved im-portant during the execution phase: recruiting suitablestaff, finding an appropriate location and recruiting suf-ficient participants.
A suitable staff– i.e. ‘very enthusiastic’, ‘idealistic’and ‘immune to stress’ – was considered very importantfor starting up a meeting centre, according to all ofthe initiators. And another factor that was emphasizedwas that the programme coordinator should not onlyb avem e runb nel.
to outa plew oacht uldb vie-w is ap ithc mes(
c er-r antso e in-f tten
izations in the region at an early stage, in order to aeelings of competition and to increase support foreeting centre. If this did not lead to a satisfac
esult at the early stage, additional talks would beanized later on to take away any doubts and ques
The successfulrecruiting of financiersfacilitatedmplementation. Obtaining financial support for
eeting centre sometimes proved a tricky problemt other times it was surprisingly easy. For examhen a sponsor simply volunteered, or the care ad
stration office made funds available for new projen most regions, two more than one source had tapped, in order to obtain reimbursements for botheople with dementia and the carers. Municipal w
are departments were often approached to financupport for the carers. One disadvantage was thatare organizations often work with budgets for mhan one year, which makes it difficult for projects l
e fully up to date professionally, but should also hanagement experience. The meeting centres ary a small team, and that requires qualified person
With regard tolocation, it proved important thather users of the building were fully informed abnd familiarized with the meeting centre for peoith dementia and their carers, so they could appr
his group with an open mind and opportunities coe created to jointly undertake activities. One interee from a welfare organization: “because therelaygroup here, there is always a lot of interaction whildren. Children have visited the group several ti. . .) they sing songs together and so forth”.Finding a sufficient number of participantswas fa-
ilitated by using multiple strategies: informing refers/referring organizations and potential participf the existence of the meeting centre and getting th
ormation across in various ways (oral as well as wri

F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253 249
information and visual materials). The programme co-ordinators experienced the fact that potential referrerssometimes had little time to be informed, and that in-formation is not adequately distributed among otherworkers within organizations as a barrier. Recruitmentwas also hampered if the potential participants werenot reached, for example because there was no welfareorganization in the region, a lack of PR-activities inthe neighbourhood, or the information was presentedin an inappropriate tone (a childish flyer for instance).The target group of the meeting centres is a difficultgroup to reach in any case: these are people with mildto moderately severe dementia, who have generally notyet had any dealings with the care and welfare services.
3.2.2.2. Meso level.At the meso level,adequate col-laborationof the meeting centres with other care andwelfare workers/organizations, preferably recorded ina collaboration protocol, proved of importance. It fa-cilitated referrals, tuning and placement in institutionalfacilities, as well as the execution of the support pro-gramme in the meeting centre. In some cases, collab-oration was difficult, for example due to pressures ofwork, or organizations having different interests.
Also in the execution phase,financingof the meetingcentres played an important role. Implementation wasobviously facilitated if there were sound agreementswith (different) financiers about bearing the costs ofthe support programme for the people with dementiaas well as the family carers.
3 r-a thatm lE s fort iousf nt.A fromn asiso thatp then dingo ncialp
33 p-p king
according to theadaptation-coping model, offering in-tegrated care(to people with dementia as well as theircarers), andaccessibility. These starting points have allproved to facilitate the continuation of the support pro-gramme. The advantages are that programme coordina-tors gain more insight into behaviour, as well as startingpoints for their supervision/guidance, that a lot of sup-port and safety can be offered because both the personwith dementia and the carer receive support, and thatthe nature of the meeting centre is visibly open becausepeople can walk in without an appointment and theycan try it out a few times first.Integration with otheractivitieswithin the location also proved to contributeto the fact that people like coming to the meeting cen-tre and not feeling like they are in an institution. In thewords of one staff member of a meeting centre whichis located in a centre for the elderly: “One of our par-ticipants is going to take up painting in watercolours,two men have taken a musical course, two ladies par-ticipate in the handicrafts club here (the centre for theelderly). There they also meet people from the immedi-ate neighbourhood”. Family members or friends of theparticipants can also come to the meeting group and,like the people with dementia, utilize other activities orservices in the building (take courses, have their hairdone, visit the restaurant). The participantsappreciatetheprogrammeandtheprogrammecanalsobeadaptedto the participants’ wishes. For example, in one meetingcentre continuation appeared to be hampered becausethe programme was too much for the family carers. Inc oft ousd , be-c f newp e tow thatb par-t portf uledd don
en-t rf ryo anizea
t-i
.2.2.3. Macro level.Interviewees from health insunce, care and welfare organizations indicatedodernization of the AWBZ(the Exceptional Medicaxpenses Act) (as of April 2003), has consequence
he financing of meeting centres. In the new law varunctions (types of support) qualify for reimburseme
disadvantage of these new developments is thatow on the meeting centres will be paid on the bf performed services. This means that the daysarticipants are absent are not reimbursed, whileumber of staff on these days is the same. Depenn the number of absences, this might cause finaroblems for the meeting centre.
.2.3. Continuation phase
.2.3.1. Micro level.The starting points of the suort programmes in the meeting centres are: wor
onsultation with the people involved, the intensityhe support programme was modified. The continuiscussion groups also proved to be an advantageause its continuous nature means that the needs oarticipants can be met quickly. They do not havait until the group is large enough to start. The factoth children and partners of people with dementia
icipated complicated the programming of the supor carers. Many programme elements were scheduring the day, which is positive for partners (whoot work), but a problem for children with jobs.
A barrier to the continuation of the meeting cre support programme waslack of capacity in otheacilities. This makes it increasingly difficult to carut the case management task adequately and orgdditional help quickly.
A facilitator to the continuation of the meeng centres wasstructural financing. Especially key

250 F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253
figures from welfare organizations indicated that thechances of structural financing increased if the projectwas successful and the (scientific) evaluation of thesupport programme was positive. Financial impedi-ments were obviously if the project made a loss orif the initiating organization was itself in financialdifficulty.
Another factor that could impede continuation wasthe existence ofwaiting lists for the meeting centres.This would make people tend to neglect publicity,which would in turn result in referrers “starting to for-get about” the meeting centres. An additional problemwas that participants had often deteriorated so they nolonger met the criteria of the target group by the timethere was room for them.
Other factors that hampered obtaining and/or keep-ing the right group of participants were: (a) referrerswere not familiar with the difference between meetingcentres, day care and psychogeriatric day treatment,(b) a lack of suitable alternative facilities for peoplewho werenot part of the target group, (c) stagnationin follow-up day care, and (d) participants who hadtrouble saying goodbye to the meeting centre group.Finally, a few facilitating factors were: a suitable loca-tion and good staff. The qualifications of these factorswere already described in the previous phases, but theywere also considered important during the continuationphase.
3.2.3.2. Meso level.The image other organizationsha theirc or-g te foro xtra-m s oft nda-t andi t foro -s peo hec whent therd ededi ado n-t
Collaborating with other care and welfare institu-tions proved to facilitate continuation, especially thefact that much informal contact is made from the meet-ing centre. Also, solid formal contacts are developed inthe context of executing elements from the programme,such as the discussion groups and the informative meet-ings. Recording collaboration agreements in a protocolhad the advantage that it made frequent negotiation un-necessary. As one initiator (a manager from a welfareorganization) put it: “it calms things down”.
3.2.3.3. Macro level.At the level of legislation, regu-lation and policymaking, the potential problems men-tioned above associated with themodernization ofthe AWBZwere important. However, a type of daytreatment qualification for the meeting centres wouldstimulate adequate financing by the care administra-tion office. During our study, the umbrella organiza-tion of Homes for the Elderly and Nursing Homes,and the Welfare umbrella organization campaignedjointly, to accomplish, among other things, an ade-quate fee for the meeting centres. This can benefit thefurther continuation and implementation of meetingcentres.
4. Conclusion and discussion
In our study of facilitating and impeding factors inthe adaptive implementation of meeting centres, weu rt yses.T en-t riersw vels.I therp ndi tingc
ess-fv -ia -z erall rga-n them sive
ave of the meeting centresand thesignificancetheyssign the meeting centres proved important forontinuation. For example, it was positive if theseanizations felt the meeting centres acted as a gather facilities, and in that way helped shape the euralization of care. Others appreciated the statu
he meeting centres because of the theoretical fouion of the support programme, and their appealingnnovating nature. This status also proved importanbtaining and/or retainingfinancing. However, the posibility of not surviving cutbacks, being the latest tyf care, constituted a risk to further continuation. Thances of this happening were assessed higherhere were few meeting centres in the region. Furissemination of the meeting centres was also imp
f the initiator belonged to a local organization instef an organization with a regional or provincial orie
ation.
sed a theoretical model[9], developed specifically fohis purpose, to guide the data collection and analhe model distinguishes different phases of implem
ation, and for each phase the facilitators and barere investigated on the micro, meso and macro le
n addition, characteristics of the innovation and oreconditions were examined for their facilitating a
mpeding influence on the implementation of meeentres.
Various factors proved to have facilitated succul implementation in all phases. For example,moti-ated organizations and staff members, the availabil
ty of financial resources, continuous and variedPR-ctivities, andsound collaborationwith other organiations. This collaboration proved relevant at sev
evels: both within organizations and between oizations, and both at the executive level and atanagement/board level. In some regions, exten

F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253 251
cooperative relationships were already present, in oth-ers they had to be developed.
Some factors turned out to be facilitators in onephase, but barriers in another, as for example wait-ing lists. The existence of waiting lists for other fa-cilities for the target group (for instance day care) atthe start of the implementation, had a positive influ-ence on the need and support for setting up a meet-ing centre. On the other hand, waiting lists in thecontinuation phase could have an impeding effect be-cause they kept participants from moving on to otherfacilities.
At the macro level, laws and regulations proved im-portant for the financing of the meeting centres. Untilnow, it was not easy arranging the financing of the twoelements of care for people with dementia, and sup-port for the caregivers. The new AWBZ (ExceptionalMedical Expenses Act) makes the financing of bothpossible.
Characteristics of the meeting centres (includingsurplus value as compared to the existing support of-fer, availability of examples) and other preconditions(such as time, finances) proved to be able to facilitateor impede implementation.
Several of the facilitators and barriers we found inour study were also found in other implementationstudies. Examples are: motivation of the people in-volved [23], problems reaching the target group[24],financing problems[25] and organizational character-istics[26].
erep Asoc er-h ivedi resa sys-t rierst edf ingi e int rentl
riesa tet ngf thera
Using models for the implementation of care in-novations is in line with the notion that implementa-tion requires attention because implementation doesnot occur spontaneously[18,27,28]. Both research andpractice show that various strategies can facilitate theimplementation of care innovations, and a combina-tion of strategies is usually more effective than sim-ple strategies[2,4,29]. Adaptation to specific situationsand target groups is always necessary[30]. Because ofthe required cooperation with other organizations, thestrategies one chooses when setting up new meetingcentres will also depend on the local situation. In thistype of innovationadaptiveimplementation is oftenpreferred over programmed implementation[1,18]. Itis advisable to link studies to adaptive implementationprojects, in order to obtain insight into the effectivenessof used strategies and make a contribution to ‘evidence-based’ implementation[3,31].
The scientific relevance of this study is that it yieldsnew information on facilitators and barriers in adaptiveimplementation of a new support programme for per-sons with dementia and their carers. This programmeoperates on the borderline between care and welfare,and focuses on more effective cooperation between al-ready existing care and welfare organizations. Becausethis implementation area is rather new, the results ofthe study could also be very useful for other researchinto the adaptive implementation of innovations on theborderline between care and welfare.
The social relevance of this study lies in the fact thatac-n of
en-sin-d (1)(2),bar-pedbasis, anptive
retepyplesaseed to
The results on facilitating and impeding factors wrimarily obtained from interviews with key figures.nly two key figures had been involved in theunsuc-essfulimplementation of (three) meeting centres, paps the information on impeding factors has rece
nsufficient attention. However, all of the key figulso supplied examples of impeding factors. The
ematic method used to trace facilitators and baro implementation proved extremely useful. It allowor structured interviews with key figures, while taknto account their specific expertise and experienche different implementation phases and at the diffeevels (micro, meso and macro).
Our theoretical model combines existing theond classifications[16–18]. We therefore anticipa
hat this model for tracing facilitating and impediactors in implementation can also be used in odaptive implementation projects.
the obtained insight into facilitating and impeding ftors may contribute to an effective implementatiointegrated support programmes for people with demtia who live at home and their carers. Grol[2] suggesta cyclical five-step plan for the implementation ofnovations. After a proposal to change is developeand facilitating and impeding factors are identifiedstrategies must be tuned to these facilitators andriers (3), an implementation plan must be develo(4) and executed and evaluated (5). Partly on theof the facilitators and barriers found in our studyimplementation guide was developed for the adaimplementation of meeting centres[32]. In addition toinformation and advice, this guide also offers concaids to facilitate implementation (for example flopdisks containing forms and questionnaires, examof applications for funding, etc.). Such aids increthe chances of successful implementation compar

252 F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253
merely providing information[23]. Furthermore, planswere prepared for the continued nationwide implemen-tation and evaluation of meeting centres in which pre-dictors of facilitating or impeding implementation willbe studied on a nationwide scale. In addition to the im-plementation guide, local initiators can use the knowl-edge that is available in the national working groupmeeting centres, a help desk, and a training course de-veloped for the staff of new meeting centres.
Acknowledgments
The study received financial support from ZonMw(Dutch Health Research and Development Council),the Valerius Foundation, Association for Support ofChristian Care of people with Mental and Nervous Dis-eases, Novartis, National Fund Elderly Support, Foun-dation Sluyterman Van Loo, VSB-fund, the Provincesof Groningen, Utrecht and Gelderland. The authorswish to thank all the personnel and participants of themeeting centres programme and the responsible orga-nizations for their cooperation.
References
[1] Boekholdt M, Pepels R. Implementatie: het invoeren vanvernieuwingen in de ouderenzorg. In: Nies H, Kollaard S, edi-tors. De praktijk van vernieuwingswerk in de ouderenzorg. [Im-
thein94.
ce.
evi-ual-
nce
n-g-de-
; eenereneet-de-y].
eenen en
hun verzorgers. Eindrappport effectstudie [Amsterdam meetingcentres; a new type of support for elderly people with dementiaand their caregivers – final report outcome study]. Amsterdam:Thesis Publishers; 1996.
[8] Droes RM, Meiland FJM, Schmitz MJ, Vernooij-Dassen MJFJ,de Lange J, Derksen E, Boerema I, Grol RPTM, van TilburgW. Implementatie Model Ontmoetingscentra. Een onderzoeknaar de voorwaarden voor succesvolle landelijke implementatievan ontmoetingscentra voor mensen met dementie en hun ver-zorgers. Eindrapport. [Implementation meeting centres model;a study into the conditions for successful nationwide implemen-tation of meeting centres for people with dementia and their car-ers. Final report]. Amsterdam: VU Medisch Centrum, AfdelingPsychiatrie; 2003.
[9] Meiland FJM, Droes RM, de Lange J, Vernooij-Dassen MJFJ.Development of a theoretical model for tracing facilitatorsand barriers in adaptive implementation of innovative prac-tices in dementia care. Archives of Gerontology and Geriatrics2004;38(Suppl 9):279–90.
[10] Droes RM, Breebaart E, Tilburg Wvan, Mellenbergh GJ. Theeffect of integrated family support versus day care only on be-havior and mood of patients with dementia. International Psy-chogeriatrics 2000;12(1):99–116.
[11] Droes RM, Meiland FJM, de Lange J, Vernooij-Dassen MJFJ,van Tilburg W. The Meeting Centres Support Programme: aneffective way of supporting people with dementia who live athome and their carers. Dementia International Journal of SocialResearch and Practice 2003;2(3):426–33.
[12] Droes RM, Breebaart E, Meiland FJM, van Tilburg W, Mel-lenbergh GJ. Effect of Meeting Centres Support Programme onfeeling of competence of family caregivers and delay of insti-tutionalization of people with dementia. Aging Mental Health2004;8(3):201–11.
[13] Droes RM, Meiland FJM, Schmitz MJ, van Tilburg W. Effectof Meeting Centres Support Programme on psychological and
nsti-lti-
[ ctver-with
. In-4.
[ J,nt-anceperi-
[ he
[ lei-arens].
[ vanorg.
eory
psychosomatic symptoms of family carers and delay of itutionalization of people with dementia; results from a mucentre implementation study, submitted for publication.
14] Droes RM, Meiland FJM, Schmitz MJ, van Tilburg W. Effeof combined support for people with dementia and carerssus regular day care on behaviour and mood of personsdementia: results from a multi-centre implementation studyternational Journal of Geriatric Psychiatry 2004;19:673–8
15] Boerema I, Derksen E, Droes RM, Meiland FJM, de LangeVernooij-Dassen M. Begeleiding bij implementatie helpt omoetingscentra verder. Ervaringen met elkaar delen. [Guidduring implementation helps meeting centres. Sharing exences]. Ouderenzorg 2002;11:23–7.
16] Rogers EM. Diffusion of innovations. 3rd ed. New York: TFree Press; 1983.
17] Nies H. Innovatie in de ouderenzorg. Een methodischedraad tot zorgvernieuwing. [Innovation in the field of cfor the elderly. A systematic guideline to care innovatioHouten/Zaventem: Bohn, Stafleu Van Lochum; 1994.
18] van der Linden BA, Schrijvers AJP. Het implementerentransmurale zorg: theorie en praktijk. In: Handboek ThuiszG1.1.1–G1.32. [Implementation of transmural care: th
plementation: introducing innovations in the field of care forelderly. In: Innovation work in the field of care for the elderlypractice]. Houten/Zaventem: Bohn, Stafleu Van Lochum; 19
[2] Grol R. Beliefs and evidence in changing clinical practiBritish Medical Journal 1997;315:418–21.
[3] Grol R, Grimshaw J. Evidence-based implementation ofdence based medicine. The Joint Commission Journal on Qity Improvement 1999;25(10):503–13.
[4] NHS Centre for Reviews and Dissemination. Getting evideinto practice. Effective Health Care 1999;5(1):1–16.
[5] Wensing M, Laurant M, Hulscher M, Grol R. Methods for idetifying barriers and facilitators for implementation. In: Chaning professional practice. Theory and practice of clinical guilines implementation. Copenhagen: DSI; 1999.
[6] Droes RM, Breebaart E. Amsterdamse Ontmoetingscentranieuwe vorm van ondersteuning voor dementerende ouden hun verzorgers Eindrapport voorstudie. [Amsterdam ming centres; a new type of support for elderly people withmentia and their caregivers – final report preliminary studAmsterdam: Thesis Publishers; 1994.
[7] Droes (red.) RM. Amsterdamse Ontmoetingscentra –nieuwe vorm van ondersteuning voor dementerende mens

F.J.M. Meiland et al. / Health Policy 71 (2005) 243–253 253
and practice. In: Guide Home Care]. Utrecht: De Tijdstroom;1998.
[19] Barbour RS. The case for combining qualitative and quantita-tive approaches in Health Services Research. Journal of HealthServices Research Policy 1999;4:39–43.
[20] Qualitative Solutions and Research. Melbourne, Australia:NUD*IST Vivo (Nvivo) Pty. Ltd., 1999.
[21] Strauss A, Corbin J. Basics of qualitative research; Groundedtheory procedures and techniques. London: Sage; 1990.
[22] Wester F, Maso I. Het analyse proces in kwalitatief onderzoek.In: Wester F, Maso I, editors. Moeilijkheden en mogelijkheden.Het omgaan met problemen in de praktijk van de kwalitatieveanalyse. [The process of analysis in qualitative research. In: Dif-ficulties and possibilies. Dealing with problems in het practiceof qualitative research] SISWO Publ. 354. Amsterdam: SISWO;1991.
[23] Wilkinson EK, Bosanquet A, Salisbury C, Hasler J, BosanquetN. Barriers and facilitators to the implementation of evidence-based medicine in general practice: a qualitative study. Euro-pean Journal of General Practice 1999;5:66–70.
[24] Poppelaars FA, van der Wal G, Braspenning JC, Cornel MC,Henneman L, Langendam MW, ten Kate LP. Possibilities andbarriers in the implementation of a preconceptional screeningprogramme for cystic fibrosis carriers: a focus group study. Pub-lic Health 2003;117(6):396–403.
[25] Mur-Veeman I, van Raak A, Maarse H. Dutch home care: to-wards a new organization. Health Policy 1994;27:151–6.
[26] Berlowitz DR, Young GJ, Hickey EC, Saliba D, Mittman BS,Czarnowski E, et al. Quality improvement implementationin the nursing home. Health Services Research 2003;38:65–83.
[27] Hulscher M, Wensing M, Grol R. Effectieve implementatie: the-orieen en strategieen. [Effective implementation: theories andstrategies]. Den Haag: ZON; 2000.
[28] Grol R, Wensing M. Implementatie: effectieve verander-ing in de patientenzorg. [Implementation: Effective changein patient care]. Maarssen, Gezondheidszorg: Elsevier;2001.
[29] Bero LA, Grilli R, Grimshaw JM, Harvey E, Oxman AD, Thom-son MA. Closing the gap between research and practice: anoverview of systematic reviews of interventions to promote theimplementation of research findings. British Medical Journal1998;317:65–8.
[30] Grol R, Grimshaw J. From best evidence to best practice: ef-fective implementation of change in patients’ care. The Lancet2003;362:1225–30.
[31] Wensing M, van der Weijden T, Grol R. Implementingguidelines and innovations in general practice: which inter-ventions are effective. British Journal of General Practice1998;48:991–7.
[32] Droes RM, van Ganzewinkel J. Draaiboek Ontmoetingscentravoor mensen met dementie en hun verzorgers. [ImplementationGuide Meeting Centres for persons with dementia and theircarers]. Amsterdam, 2003.
Recommended

















