1……………………………GOOD MEDICAL PRACTICE …...………………………
1
BY Ibrahim Mohammed Farouk Ahmed
M.B.B.Ch. Zagazig University
Under Supervision of
PROF. DR.
Mohammed Adel Foda
Professor of public Health And Community Medicine Faculty of Medicine Zagazig University
Faculty of Medicine
Zagazig University 2010
GOOD MEDICAL PRACTICEGOOD MEDICAL PRACTICEGOOD MEDICAL PRACTICEGOOD MEDICAL PRACTICE
2……………………………GOOD MEDICAL PRACTICE …...………………………
2
رسالة مقدمة منرسالة مقدمة منرسالة مقدمة منرسالة مقدمة من
إبراهيم محمد فاروق أحمد/ الطبيب
بكالوريوس طب وجراحة
جامعة الزقازيق
توطئة للحصول علي درجة الزمالة المصرية في طب األسرةتوطئة للحصول علي درجة الزمالة المصرية في طب األسرةتوطئة للحصول علي درجة الزمالة المصرية في طب األسرةتوطئة للحصول علي درجة الزمالة المصرية في طب األسرة
تحت إشراف
محمد عادل فوده/ األستاذ الدكتور جامعة الزقازيق– كلية الطب –أستاذ الصحة العامة
ازيقازيقازيقازيق جامعة الزق جامعة الزق جامعة الزق جامعة الزق––––كلية الطب كلية الطب كلية الطب كلية الطب
2010
3……………………………GOOD MEDICAL PRACTICE …...………………………
3
CONTENTS NO. SUBJECT
PAGE
1- INTRODUCTION
7
2- DEFINITION OF GOOD MEDICAL PRACTICE
7
3- THE GOOD MEDICAL CARE’s ROLE IN REGULATION
10
4- AIM OF THE WORK
11
5- Good doctors
12
6- Good clinical care must include
12
7- Supporting self care
13
8- Avoid treating those close to you
14
9- Raising concerns about patient safety
14
10- Decisions about access to medical care
14
11- Treatment in emergencies
16
12- Maintaining good medical practice
16
13- Keeping up to date
16
14- Maintaining & improving your performance
16
15- Relationships with patients
17
4……………………………GOOD MEDICAL PRACTICE …...………………………
4
16- Doctor patient partnership
17
17- Good communication
18
18- Maintaining trust in the profession
20
19- Consent
20
20- Confidentiality
21
21- Ending your professional relationship with a patient
21
22- Working with colleagues
22
23- Working in teams
22
24- Conduct and performance of colleagues
23
25- Respect for colleagues
24
26- Arranging cover
24
27- Taking up and ending appointments
24
28- Sharing information with colleagues
25
29- Delegation and referral
25
30- Being honest and trustworthy
26
31- Providing and publishing information about
your services
27
5……………………………GOOD MEDICAL PRACTICE …...………………………
5
32- Writing reports and CVs, giving evidence and signing documents
27
33- Research
28
34- Financial and commercial dealings
28
35- Health maintenance
30
36- The purpose of health maintenance visits
30
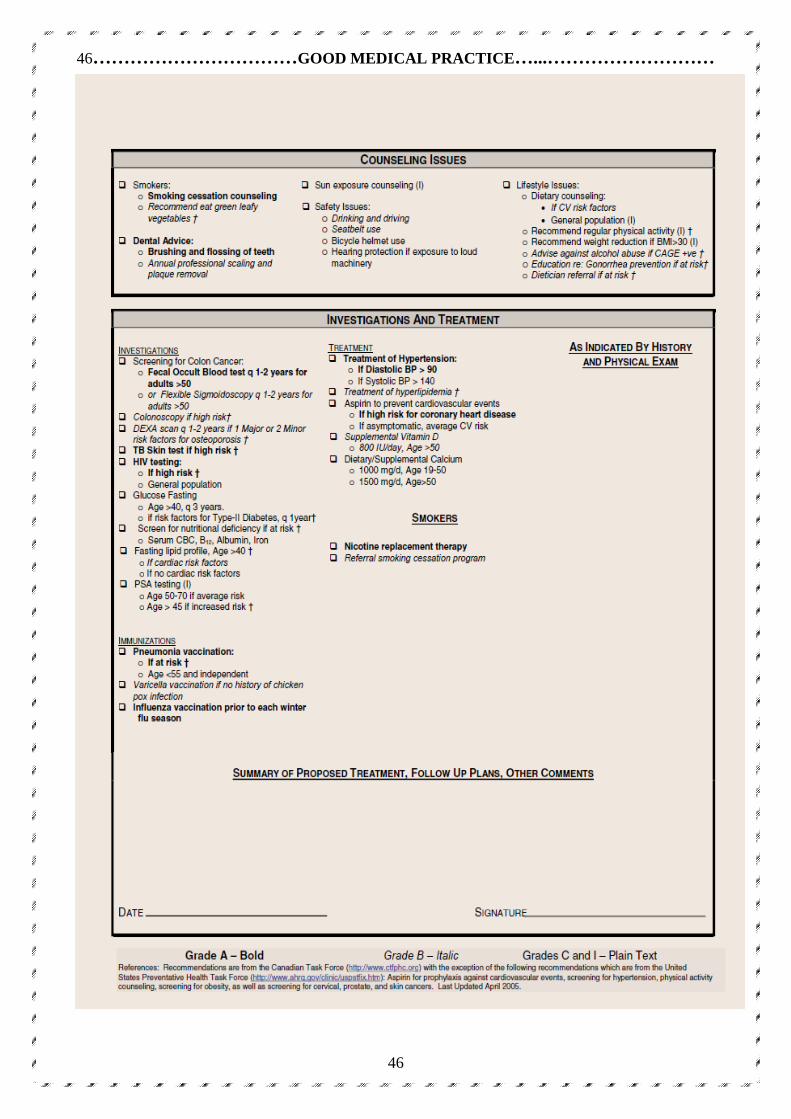
37- IF client is overweight, Impaired fasting glucose
30
38- The screening tests
31
39- Immunization
34
40-
exercise 37
41-
dietary counseling 38
42-
SMOKING CESSATION 39
43-
Counseling 42
44-
Dental health
43
45-
Professionalism and communication issues
47
46-
Expert Recommendations for Prostate Cancer
Screening
50
47-
A structured registration program 57
6……………………………GOOD MEDICAL PRACTICE …...………………………
6
48-
Electronic malfunction 59
49-
Reflection on the reading during the search 60
50- At the level of this search 60
51- At my-self level 60
52- At the level of curriculums 61
53- Points needed to be improved for good
medical practice
61
54- At the level of family practice centers 61
55- At the level of half-day release course 62
56- At the level of Egyptian national guideline 62
57- References 63
7……………………………GOOD MEDICAL PRACTICE …...………………………
7
1- To practise safely, doctors must be competent in what they do. They must establish and maintain effective relationships with patients, respect patients’ autonomy and act responsibly and appropriately if they or a colleague fall ill and their performance suffers. 2. But these attributes, while essential, are not enough. Doctors have a respected position in society and their work gives them privileged access to patients, some of whom may be very vulnerable. A doctor whose conduct has shown that he cannot justify the trust placed in him should not continue in unrestricted practice while that remains the case. 3. In short, the public is entitled to expect that their doctor is fit to practise, and follows the principles of good practice described in Good Medical Practice. It sets out the standards of competence, care and conduct expected of doctors,
under the following main headings:
doctors must provide good standards of clinical care, must practise within the limits of their competence, and must ensure that patients are not put at unnecessary risk.
INTRODUCTIONINTRODUCTIONINTRODUCTIONINTRODUCTION
DEFINITION OF DEFINITION OF DEFINITION OF DEFINITION OF GOOD GOOD GOOD GOOD MEDICAL MEDICAL MEDICAL MEDICAL PRACTICEPRACTICEPRACTICEPRACTICE

8……………………………GOOD MEDICAL PRACTICE …...………………………
8
doctors must keep up to
date with developments in their field, maintain their skills and audit
their performance
doctors must develop and
maintain successful relationships with their patients, by respecting
patients’ autonomy and other rights.
doctors must work effectively with their colleagues.
where doctors have teaching responsibilities they must develop the skills, attitudes and practices of a competent teacher.
doctors must be honest and trustworthy.
doctors must not allow their own health condition to endanger patients.
We aim to be good physicians, providing safe and effective care to our patients.
But is that really the case? Family physicians deliver care through the process of
our practices and the method of our consultations. To understand what sort of
Relationships with patientsRelationships with patientsRelationships with patientsRelationships with patients
Working with colleaguesWorking with colleaguesWorking with colleaguesWorking with colleagues
Teaching and trainingTeaching and trainingTeaching and trainingTeaching and training
Maintaining good medical practiceMaintaining good medical practiceMaintaining good medical practiceMaintaining good medical practice
ProbityProbityProbityProbity
HealthHealthHealthHealth
9……………………………GOOD MEDICAL PRACTICE …...………………………
9
doctors we are, we need to evaluate both aspects of care. Your initial response is
probably skepticism or disbelief. You don’t have the time or the energy, and even
if you did.
so what? We would be concerned if half our patients with hypertension had
systolic blood pressures greater than 160 mm Hg; if our patients with suspected
herpes zoster had no way of seeing us within 3 days; if we ordered a blood test,
urine test, or x-ray scan at every consultation; if we didn’t listen to patients; or if
we finished every consultation by pushing a prescription at the patient. We don’t
believe these things occur, but how can we be certain? The latter issues probably
require video recording of our consultations.
1- For the others, we need to evaluate our clinical practices. Evaluation is a
cyclical process of measuring what we do, making changes if required, then
measuring again
2- To facilitate this we need electronic records
In 1987, one of the authors (M.D.) introduced the first electronic medical record
(EMR) into his UK practice. A “stand alone” personal computer was used for
recording prescriptions and diagnoses of patients with repeat prescriptions. This
came about following a lengthy and costly paper-chart evaluation promoted by the UK equivalent of the College of Family Physicians of Canada, which revealed
both a lack of information and a lack of practice organization for recording
factors related to cardiovascular disease, such as blood pressure Over the next 10
years, a full electronic record was incrementally built up so as not to interfere with
clinical care and consultations. The last evaluation performed followed a talk on
the potential benefits of pneumococcal vaccine after splenectomy. Twelve patients
in M.D.’s practice of 7000 had splenectomy recorded. Six had records of
vaccination; of the remaining had records of vaccination found in their legacy
paper charts, and were invited in to see the nurse to discuss vaccination. The
10……………………………GOOD MEDICAL PRACTICE …...………………………
10
whole process was accomplished in less than 5 minutes. This anecdote reflects the substantial body of evidence for auditing health care
using electronic records.
THE GOOD MEDICAL CARE’s ROLE IN REGULATION
1. All human beings make mistakes from time to time. Doctors are no different.
2. While occasional one-off mistakes need to be thoroughly investigated by those immediately involved where the incident occurred and any harm put right, they are unlikely in themselves to indicate a fitness to practise problem.
A question of fitness to pracA question of fitness to pracA question of fitness to pracA question of fitness to practise is likely to arise if: tise is likely to arise if: tise is likely to arise if: tise is likely to arise if:
1• A doctor’s performance has harmed patients or put patients at risk of harm;
A risk of harm will usually be demonstrated by a series of incidents that cause concern locally. These incidents will indicate persistent technical failings or other repeated departures from good practice which are not being, or cannot be, safely managed locally or local management has been tried and has failed.
2• A doctor has shown a deliberate or reckless disregard of clinical responsibilities towards patients. An isolated lapse from high standards of conduct – such as an atypical rude outburst– would not in itself suggest that the doctor’s fitness to practise was in question. But the sort of misconduct, whether criminal or not, which indicates a lack of integrity on the part of the doctor, an unwillingness to practise ethically or responsibly or a serious lack of insight into obvious problems of poor practice .
3• A doctor has abused a patient’s trust or violated a patient’s autonomy or other fundamental rights.
11……………………………GOOD MEDICAL PRACTICE …...………………………
11
Conduct which shows that a doctor has acted without regard for patients’rights or feelings, or has abused their professional position as a doctor, will usually give rise to questions about a doctor’s fitness to practise. 4• A doctor has behaved dishonestly, fraudulently or in a way designed to mislead or harm others.
Patients must be able to trust doctors with their lives and health. To justify that trust you must show:
1-respect for human life and you must Make the care of your patient your first concern.
2-Protect and promote the health of patients and the public. 3-Provide a good standard of practice and care.
4- Keep your professional knowledge and skills up to date.
5-Recognise and work within the limits of your competence.
6- Work with colleagues in the ways that best serve patients’ interests 7-Treat patients as individuals and respect their dignity .
8-Treat patients politely and considerately.
9-Respect patients’ right to confidentiality. 10-Work in partnership with patients.
11- Listen to patients and respond to their concerns and preferences.
12- Give patients the information they want or need in a way they can Understand.
13- Respect patients’ right to reach decisions with you about their treatment and care.
14- Support patients in caring for themselves to improve and maintain their health. 15-Be honest and open and act with integrity.
AIM OF THE WORKAIM OF THE WORKAIM OF THE WORKAIM OF THE WORK
12……………………………GOOD MEDICAL PRACTICE …...………………………
12
16- Act without delay if you have good reason to believe that you or a colleague may be putting patients at risk.
17-Never discriminate unfairly against patients or colleagues.
18- Never abuse your patients’ trust in you or the public’s trust in the profession.
19-You are personally accountable for your professional practice and must always be prepared to justify your decisions and actions.
Patients need good doctors. Good doctors make the care of their patients their
first concern: they are competent, keep their knowledge and skills up to date,
establish and maintain good relationships with patients and colleagues, are
honest and trustworthy, and act with integrity
Good clinical care must include
A. adequately assessing the patient’s conditions, taking account of the history (including the symptoms, and psychological and social factors), the patient’s
views, and where necessary examining the patient.
B. providing or arranging advice, investigations or treatment where necessary.
C. referring a patient to another practitioner, when this is in the patient’s best Interests.
GOOD DOCTORSGOOD DOCTORSGOOD DOCTORSGOOD DOCTORS
GOOD CLINICAL CAREGOOD CLINICAL CAREGOOD CLINICAL CAREGOOD CLINICAL CARE
13……………………………GOOD MEDICAL PRACTICE …...………………………
13
In providing care you must
A. recognize and work within the limits of your competence.
B. prescribe drugs or treatment, including repeat prescriptions, only when you have adequate knowledge of the patient’s health, and are satisfied that the
drugs or treatment serve the patient’s needs.
C. provide effective treatments based on the best available evidence.
D. take steps to alleviate pain and distress whether or not a cure may be possible.
E. respect the patient’s right to seek a second opinion.
F. keep clear, accurate and legible records, reporting the relevant clinical findings,
the decisions made, the information given to patients, and any drugs prescribed
or other investigation or treatment.
G. make records at the same time as the events you are recording or as soon as possible afterwards.
H. be readily accessible when you are on duty.
I. consult and take advice from colleagues, where appropriate.
J. make good use of the resources available to you.
Supporting self care
♠ You should encourage patients and the public to take an interest in their health and to take action to improve and maintain it.
♠ This may include advising patients on the effects of their life choices on their health and well-being and the possible outcomes of their treatments.
14……………………………GOOD MEDICAL PRACTICE …...………………………
14
Avoid treating those close to you
♠ Wherever possible, you should avoid providing medical care to anyone with whom you have a close personal relationship.
Raising concerns about patient safety
♠ If you have good reason to think that patient safety is or may be seriously compromised by inadequate premises, equipment, or other resources, policies or
systems, you should put the matter right if that is possible.
♠ In all other cases you should draw the matter to the attention of your employing or contracting body.
♠ If they do not take adequate action, you should take independent advice on how to take the matter further.
♠ You must record your concerns and the steps you have taken to try to resolve them.
Decisions about access to medical care
♠ The investigations or treatment you provide or arrange must be based on the
assessment you and the patient make of their needs and priorities, and on your
clinical judgement about the likely effectiveness of the treatment options.
♠ You mus have contributed to their condition.t not refuse or delay treatment because you believe that a patient’s actions.
♠ You must treat your patients with respect whatever their life choices and beliefs.
♠ You must not unfairly discriminate against them by allowing your personal views to affect adversely your professional relationship with them or the treatment you provide or arrange.
15……………………………GOOD MEDICAL PRACTICE …...………………………
15
♠ You should challenge colleagues if their behaviour does not comply with this guidance If carrying out a particular procedure or giving advice about it
conflicts with your religious or moral beliefs, and this conflict might affect the
treatment or advice you provide, you must explain this to the patient and tell
them they have the right to see another doctor.
♠ You must be satisfied that the patient has sufficient information to enable them to exercise that right. If it is not practical for a patient to arrange to see
another doctor.
♠ you must ensure that arrangements are made for another suitably qualified colleague to take over your role You must give priority to the investigation and
treatment of patients on the basis of clinical need, when such decisions are
within your power.
♠ All patients are entitled to care and treatment to meet their clinical needs.
♠ You must not refuse to treat a patient because their medical condition may put you at risk.
♠ If a patient poses a risk to your health or safety, you should take all available steps to minimise the risk before providing treatment or making suitable
alternative arrangements for treatment.
♠ This includes your views about a patient’s age, colour, culture, disability, ethnic or national origin, gender, lifestyle, marital or parental status, race,
religion or beliefs, sex, sexual orientation, or social or economic status
16……………………………GOOD MEDICAL PRACTICE …...………………………
16
Treatment in emergencies
♠ In an emergency, wherever it arises, you must offer assistance, taking account of your own safety, your competence, and the availability of other
options for care.
Keeping up to date
You must keep your knowledge and skills up to date throughout your working life. You should be familiar with relevant guidelines and developments that
affect your work. You should regularly take part in educational activities that
maintain and further develop your competence and performance
improving your performance& Maintaining
You must work with colleagues and patients to maintain and improve the quality of your work and promote patient safety. In particular, you mustyou mustyou mustyou must A. maintain a folder of information and evidence, drawn from your medical
Practice.
B. reflect regularly on your standards of medical practice in accordance with guidlines on licensing and revalidation.
C. take part in regular and systematic audit.
D. take part in systems of quality assurance and quality improvement.
E. respond constructively to the outcome of audit, appraisals and
Maintaining good medical practiceMaintaining good medical practiceMaintaining good medical practiceMaintaining good medical practice
17……………………………GOOD MEDICAL PRACTICE …...………………………
17
performance reviews, undertaking further training where necessary.
F. help to resolve uncertainties about the effects of treatments.
G. contribute to confidential inquiries and adverse event recognition and reporting, to help reduce risk to patients.
H. report suspected adverse drug reactions in accordance with the relevant reporting scheme.
I. co-operate with legitimate requests for information from organisations monitoring public health when doing so you must follow the guidance in with
Confidentiality: Protecting and providing information.
Doctor patient partnership
Relationships based on openness, trust and good communication will enable you to work in partnership with your patients to address their individual needs To fulfil your role in the doctor-patient partnership you mustyou mustyou mustyou must A. be polite, considerate and honest
B. treat patients with dignity
C. treat each patient as an individual
D. respect patients’ privacy and right to confidentiality
E. support patients in caring for themselves to improve and maintain their health
Relationships with patients
18……………………………GOOD MEDICAL PRACTICE …...………………………
18
F. encourage patients who have knowledge about their condition to use this when they are making decisions about their care
Good communication
To communicate effectively you must
A. listen to patients, ask for and respect their views about their health, and respond to their concerns and preferences
B. share with patients, in a way they can understand, the information they want or need to know about their condition, its likely progression, and the
treatment options available to them, including associated risks and
uncertainties.
C. respond to patients’ questions and keep them informed about the progress of
their care.
D. make sure that patients are informed about how information is shared
within teams and among those who will be providing their care
YOU must make sure, wherever practical, that arrangements
are made to meet patients’ language and communication
needs
CHILDREN AND YOUNCHILDREN AND YOUNCHILDREN AND YOUNCHILDREN AND YOUNG PEOPLEG PEOPLEG PEOPLEG PEOPLE
♠ children and young people as patients. You should be aware of the needs and welfare of children and young people when you see patients who are parents or
carers, as well as any patients who may represent a danger to children or young
people.
19……………………………GOOD MEDICAL PRACTICE …...………………………
19
♠ You must safeguard and protect the health and well-being of children and young People.
♠ You should offer assistance to children and young people if you have reason to think that their rights have been abused or denied.
When communicating with a child or young person you mustyou mustyou mustyou must
A. treat them with respect and listen to their views
B. answer their questions to the best of your ability
C. provide information in a way they can understand
Being open and honest with patients if things go wrongBeing open and honest with patients if things go wrongBeing open and honest with patients if things go wrongBeing open and honest with patients if things go wrong
♠ If a patient under your care has suffered harm or distress, you must act immediately to put matters right, if that is possible.
♠ You should offer an apology and explain fully and promptly to the patient what has happened, and the likely short-term and long-term effects.
♠ Patients who complain about the care or treatment they have received have a right to expect a prompt, open, constructive and honest response including an
explanation and, if appropriate, an apology.
♠ You must not allow a patient’s complaint to affect adversely the care or treatment you provide or arrange.
20……………………………GOOD MEDICAL PRACTICE …...………………………
20
Maintaining trust in the professionMaintaining trust in the professionMaintaining trust in the professionMaintaining trust in the profession
♠ You must not use your professional position to establish or pursue a sexual or improper emotional relationship with a patient or someone close to them.
♠ You must not express to your patients your personal beliefs, including political, religious or moral beliefs, in ways that exploit their vulnerability or
that are likely to cause them distress.
♠ You must take out adequate insurance or professional indemnity cover for any part of your practice not covered by an employer’s indemnity scheme, in
your patients’ interests as well as your own.
♠ You must make sure you are identifiable to your patients and colleagues, for example by using your registered name when signing statutory documents,
including prescriptions.
♠ You must make your registered name and available to anyone who asks for them.
Consent
♠ You must be satisfied that you have consent or other valid authority before you undertake any examination or investigation, provide treatment or involve
patients in teaching or research.
♠ Usually this will involve providing information to patients in a way they can understand, before asking for their consent.
♠ You must follow the guidelines in Seeking patients’ consent: The ethical
21……………………………GOOD MEDICAL PRACTICE …...………………………
21
considerations, which includes advice on children and patients who are not able to give consent.
Confidentiality
♠ Patients have a right to expect that information about them will be held in confidence by their doctors.
♠ You must treat information about patients as confidential, including after a patient has died.
Ending your professional relationEnding your professional relationEnding your professional relationEnding your professional relationship with a patientship with a patientship with a patientship with a patient
♠ In rare circumstances, the trust between you and a patient may break down, and you may find it necessary to end the professional relationship.
♠ For example, this may occur if a patient has been violent to you or a colleague, has stolen from the premises, or has persistently acted
inconsiderately or unreasonably.
♠ You should not end a relationship with a patient solely because of a complaint the patient has made about you or your team, or because of the
resource implications of the patient’s care or treatment.
♠ Before you end a professional relationship with a patient, you must be satisfied that your decision is fair .
♠ You must be prepared to justify your decision. You should inform the patient of your decision and your reasons for ending the professional
relationship.
♠ wherever practical in writing You must take steps to ensure that
22……………………………GOOD MEDICAL PRACTICE …...………………………
22
arrangements are made promptly for the continuing care of the patient, and
you must pass on the patient’s records without delay If you charge fees, you
may refuse further treatment for patients unable or unwilling to pay for
services you have already provided.
WORKING IN TEAMSWORKING IN TEAMSWORKING IN TEAMSWORKING IN TEAMS
♠Most doctors work in teams with colleagues from other professions. Working in teams does not change your personal accountability for your professional
conduct and the care you provide.
♠When working in a team, you should act as a positive role model and try to motivate and inspire your colleagues. You must
A. respect the skills and contributions of your colleagues.
B. communicate effectively with colleagues within and outside the team.
C. make sure that your patients and colleagues understand your role and responsibilities in the team, and who is responsible for each aspect of patient
care.
D. participate in regular reviews and audit of the standards and performance of the team, taking steps to remedy any deficiencies.
E. support colleagues who have problems with performance, conduct or health
Working with colleaguesWorking with colleaguesWorking with colleaguesWorking with colleagues
23……………………………GOOD MEDICAL PRACTICE …...………………………
23
If you are responsible for leading a team, you must follow the guidance in Management for doctors.
Conduct and performance of colleaguesConduct and performance of colleaguesConduct and performance of colleaguesConduct and performance of colleagues
♠ You must protect patients from risk of harm posed by another colleague’s conduct, performance or health.
♠ The safety of patients must come first at all times.
♠ If you have concerns that a colleague may not be fit to practise, you must take appropriate steps without delay, so that the concerns are investigated and
patients protected where necessary.
♠ This means you must give an honest explanation of your concerns to an appropriate person from your employing or contracting body, and follow their
procedures.
♠ If there are no appropriate local systems, or local systems do not resolve the problem, and you are still concerned about the safety of patients, you should
inform the relevant regulatory body.
♠ If you are not sure what to do, discuss your concerns with an impartial colleague or contact your defence body,or a professional organization.
♠ If you have management responsibilities you should make sure that systems are in place through which colleagues can raise concerns about risks to patients,
and you must follow the guidance in Management for doctors.
24……………………………GOOD MEDICAL PRACTICE …...………………………
24
Respect for colleaguesRespect for colleaguesRespect for colleaguesRespect for colleagues
♠You must treat your colleagues fairly and with respect.
♠You must not bully or harass them, or unfairly discriminate against them by allowing your personal views to affect adversely your professional relationship
with them.
♠You must not make malicious and unfounded criticisms of colleagues that may undermine patients’ trust in the care or treatment they receive, or in the
judgement of those treating them.
♠This includes your views about a colleague’s age, colour, culture, disability, ethnic or national origin, gender, lifestyle, marital or parental status, race, religion
or beliefs, sex, sexual orientation, or social or economic status.
Arranging coverArranging coverArranging coverArranging cover
♠ You must be satisfied that, when you are off duty, suitable arrangements have been made for your patients’ medical care.
♠ These arrangements should include effective hand-over procedures, involving
clear communication with healthcare colleagues.
♠ If you are concerned that the arrangements are not suitable, you should take
steps to safeguard patient care.
Taking up and ending appointmentsTaking up and ending appointmentsTaking up and ending appointmentsTaking up and ending appointments
♠ Patient care may be compromised if there is not sufficient medical cover.
♠ Therefore, you must take up any post, including a locum post, you have
25……………………………GOOD MEDICAL PRACTICE …...………………………
25
formally accepted, and you must work your contractual notice period, unless the employer has reasonable time to make other arrangements.
Sharing information with colleaguesSharing information with colleaguesSharing information with colleaguesSharing information with colleagues
♠ Sharing information with other healthcare professionals is important for safe and effective patient care.
♠ When you refer a patient, you should provide all relevant information about the patient, including their medical history and current condition.
♠ If you provide treatment or advice for a patient, but are not the patient’s general practitioner, you should tell the general practitioner the results of the
investigations, the treatment provided and any other information necessary for
the continuing care of the patient, unless the patient objects.
♠ If a patient has not been referred to you by a general practitioner, you should ask for the patient’s consent to inform their general practitioner before starting
treatment, except in emergencies or when it is impractical to do so.
♠ If you do not inform the patient’s general practitioner, you will be responsible for providing or arranging all necessary after-care
Delegation and referralDelegation and referralDelegation and referralDelegation and referral
♠ Delegation involves asking a colleague to provide treatment or care on your behalf.
♠ Although you will not be accountable for the decisions and actions of those to whom you delegate, you will still be responsible for the overall management of
26……………………………GOOD MEDICAL PRACTICE …...………………………
26
the patient, and accountable for your decision to delegate.
♠ When you delegate care or treatment you must be satisfied that the person to whom you delegate has the qualifications, experience, knowledge and skills to
provide the care or treatment involved.
♠ You must always pass on enough information about the patient and the treatment they need.
♠ Referral involves transferring some or all of the responsibility for the patient’s care, usually temporarily and for a particular purpose, such as
additional investigation, care or treatment that is outside your competence.
♠ You must be satisfied that any healthcare professional to whom you refer a patient is accountable to a statutory regulatory body or employed within a
managed environment.
♠ If they are not, the transfer of care will be regarded as delegation, not referral.
♠ This means you remain responsible for the overall management of the patient, and accountable for your decision to delegate.
Being honest and trustworthyBeing honest and trustworthyBeing honest and trustworthyBeing honest and trustworthy
♠ Probity means being honest and trustworthy, and acting with integrity this is at the heart of medical professionalism.
♠ You must make sure that your conduct at all times justifies your patients’ trust in you and the public’s trust in the profession.
27……………………………GOOD MEDICAL PRACTICE …...………………………
27
A-You must be honest and trustworthy when writing reports, and when completing or signing forms, reports and other documents.
B-You must always be honest about your experience, qualifications and position, particularly when applying for posts.
C-You must do your best to make sure that any documents you write or sign are not false or misleading. This means that you must take reasonable steps to
verify the information in the documents, and that you must not deliberately
leave out relevant information.
D-If you have agreed to prepare a report, complete or sign a document or provide evidence, you must do so without unreasonable delay.
E-If you are asked to give evidence or act as a witness in litigation or formal inquiries, you must be honest in all your spoken and written statements. You
must make clear the limits of your knowledge or competence.
F-You must co-operate fully with any formal inquiry into the treatment of a patient and with any complaints procedure that applies to your work. You
must disclose to anyone entitled to ask for it any information relevant to an
investigation into your own or a colleague’s conduct, performance or health. In
doing so, you must follow the guidance in Confidentiality: Protecting and
providing information.
Writing reports and CVs, giving evidence and signing documents
28……………………………GOOD MEDICAL PRACTICE …...………………………
28
G-You must assist the coroner or procurator fiscal in an inquest or inquiry into a patient’s death by responding to their enquiries and by offering all relevant
information. You are entitled to remain silent only when your evidence may
lead to criminal proceedings being taken against you.
♠ Research involving people directly or indirectly is vital in improving care and reducing uncertainty for patients now and in the future, and improving the
health of the population as a whole.
♠ If you are involved in designing, organising or carrying out research, you must
A. put the protection of the participants’ interests first
B. act with honesty and integrity
C. follow the appropriate national research governance guidelines
YOU MUST BE HONEST AND OPEN IN ANY FINANCIAL YOU MUST BE HONEST AND OPEN IN ANY FINANCIAL YOU MUST BE HONEST AND OPEN IN ANY FINANCIAL YOU MUST BE HONEST AND OPEN IN ANY FINANCIAL
ARRANGEMENTS WITARRANGEMENTS WITARRANGEMENTS WITARRANGEMENTS WITHHHH PATIENTS PATIENTS PATIENTS PATIENTS. . . . IN PARTICULARIN PARTICULARIN PARTICULARIN PARTICULAR....
A. you must inform patients about your fees and charges, wherever possible
before asking for their consent to treatment.
B. you must not exploit patients’ vulnerability or lack of medical knowledge when making charges for treatment or services.
C. you must not encourage patients to give, lend or bequeath money or gifts
Research
Financial and commercial dealings
29……………………………GOOD MEDICAL PRACTICE …...………………………
29
that will directly or indirectly benefit you.
D. you must not put pressure on patients or their families to make donations to other people or organizations.
E. you must not put pressure on patients to accept private treatment.
F. if you charge fees, you must tell patients if any part of the fee goes to another healthcare professional.
YOU MUST BE HONEST IN FINANCIAL AND COMMERCIALYOU MUST BE HONEST IN FINANCIAL AND COMMERCIALYOU MUST BE HONEST IN FINANCIAL AND COMMERCIALYOU MUST BE HONEST IN FINANCIAL AND COMMERCIAL
DEALINGS WITH EMPLOYERS DEALINGS WITH EMPLOYERS DEALINGS WITH EMPLOYERS DEALINGS WITH EMPLOYERS, , , , INSURERS AND OTHERINSURERS AND OTHERINSURERS AND OTHERINSURERS AND OTHER
ORGANIORGANIORGANIORGANIZAZAZAZATIONS OR INDIVIDUALSTIONS OR INDIVIDUALSTIONS OR INDIVIDUALSTIONS OR INDIVIDUALS. . . . IN IN IN IN PARTICULARPARTICULARPARTICULARPARTICULAR
A. before taking part in discussions about buying or selling goods or services, you must declare any relevant financial or commercial interest that you or your
family might have in the transaction.
B. if you manage finances, you must make sure the funds are used for the purpose for which they were intended and are kept in a separate account from
your personal finances.
C.You must act in your patients’ best interests when making referrals and when providing or arranging treatment or care. You must not ask for or accept any
inducement, gift or hospitality which may affect or be seen to affect the way
you prescribe for, treat or refer patients. You must not offer such inducements
to colleagues.
D.If you have financial or commercial interests in organisations providing healthcare or in pharmaceutical or other biomedical companies, these interests
must not affect the way you prescribe for, treat or refer patients.
30……………………………GOOD MEDICAL PRACTICE …...………………………
30
E.If you have a financial or commercial interest in an organisation to which you plan to refer a patient for treatment or investigation, you must tell the patient
about your interest.
We Will Discuss In The Next Pages The Best Example For
Good Medical Practice →→→→ The Health Maintenance
1- The purpose of health maintenance visits are:
The goal of periodic health examinations of asymptomaThe goal of periodic health examinations of asymptomaThe goal of periodic health examinations of asymptomaThe goal of periodic health examinations of asymptomatic adultstic adultstic adultstic adults
Prevent morbidity and mortality by identifying modifiable risk factors and early
signs of treatable disease.
Primary purpose of itPrimary purpose of itPrimary purpose of itPrimary purpose of it assessing overall health and risk factors for disease that
can be prevented by early intervention and it results in the delivery of clinical
preventive services that are tailored to a patient’s age, sex, and clinical risk
factors and laboratory testing. By promoting prevention and enhancing the
patient–provider relationship. Improve patient outcomes and the public’s health.
Reassurance
Patients who seek reassurance from physician visits that include routine screening
procedures often persist in behavior that greatly increases their risk of morbidity.
Education or counseling
Physicians must knowledge their primary role in prevention as that of educators.
Accurate information regarding risk factors is most likely to reinforce health-
enhancing behavior and alter self-destructive behavior. Physicians must
Health maintenanceHealth maintenanceHealth maintenanceHealth maintenance
31……………………………GOOD MEDICAL PRACTICE …...………………………
31
appreciate the potential for behavior modification and familiarize themselves with
local resources that can help patients identify and overcome barriers to healthy
behavior.
Screening
Routine screening for specific diseases, the health maintenance activity most
closely identified with the physician, should be performed selectively. The limits
of screening tests as well as their potential health benefits should be clearly
understood by every primary care physician.
2- IF client is overweight, Impaired fasting glucose (Category of increased risk for
Diabetes), smoker, dyslipidemia (borderline high total cholesterol) and family
history of premature coronary heart disease.
I COULD PREVENT THIS DISEASE TO HAPPEN TO HIM BY:
A- Lowering cholesterol
• The goal in this patient is
o LDL <130 mg per dL (3.35 mmol per L)
• Intervention
o Exercise and diet
B- Smoking cessation
• It reduces the level of risk to that of nonsmokers within about three years of
cessation.
• The goal in this patient is
o Smoking cessation
• Intervention
o Counseling and pharmacological treatment
32……………………………GOOD MEDICAL PRACTICE …...………………………
32
C- Aspirin
• USPSTF grade A recommendation
• 75 mg daily
D- Increase the levels of physical activity.
• Regular aerobic physical exercise e.g. walking at least 30 minutes per day
most days of the week. (JNC7)
• ideally on most days but at least 3 days/week
E- Diet
Adopt DASH eating plan (JNC 7)
• Consume a diet rich in fruits
• Vegetables, and low fat dairy products with a reduced content of saturated
and total fat.
F- Lowering homocysteine levels
• By increased folate intake
• It is a promising but unproven primary prevention strategy.
3- My response to the request of this man to order to him
all investigations to make sure that his health is OK is
• I see you concerned about your health. (Reflection)
• I know you have previous experiences with your father and mother
(Validation)
• It's very good to know that you are OK. (Appreciation and respect)
• Perhaps we can work together to make you feel better. (Partnership)
• We need some investigations which have evidence based benefits.
33……………………………GOOD MEDICAL PRACTICE …...………………………
33
• Some results of investigations are false positive, their presence usually
mandates confirmatory testing that causes additional inconvenience to
physicians and patients. Confirmatory tests may be invasive and put
patients at risk of physical harm.
• Unnecessary tests waste time and money, interfere with providing
worthwhile tests, and may end up doing more harm than good.
• You need just fasting plasma glucose (FPG) again (for DM type 2), lipid
profile (for dyslipidemia) and fecal occult blood (for colorectal cancers).
4- The screening tests I would order for this man
Screening for tScreening for tScreening for tScreening for type 2 DMype 2 DMype 2 DMype 2 DM
• FPG again
• Grade: B The U.S. Preventive Services Task Force(USPSTF)/
Recommendation.
Screening for dyslipidemiaScreening for dyslipidemiaScreening for dyslipidemiaScreening for dyslipidemia
• The U.S. Preventive Services Task Force (USPSTF) strongly recommends
screening men aged 35 and older for lipid disorders.
• Grade: A USPSTF Recommendation.
Screening for colorectal cancerScreening for colorectal cancerScreening for colorectal cancerScreening for colorectal cancer
• The USPSTF recommends screening for colorectal cancer (CRC) using fecal
occult blood testing, sigmoidoscopy, or colonoscopy, in adults, beginning at
age 50 years and continuing until age 75 years. The risks and benefits of
these screening methods vary.
• Grade: A USPSTF Recommendation.
34……………………………GOOD MEDICAL PRACTICE …...………………………
34
5- Immunization
AAAA. . . . Tetanus, diphtheria, and acellular pertussis (Td/Tdap) Tetanus, diphtheria, and acellular pertussis (Td/Tdap) Tetanus, diphtheria, and acellular pertussis (Td/Tdap) Tetanus, diphtheria, and acellular pertussis (Td/Tdap)
vaccinationvaccinationvaccinationvaccination
Tdap should replace a single dose of Td for adults ages 19 through 64 years who
have not received a dose of Tdap previously.
Adults with uncertain or incomplete history of primary vaccination series with
tetanus and diphtheria toxoid-containing vaccines should begin or complete a
primary vaccination series. A primary series for adults is 3 doses of tetanus and
diphtheria toxoid-containing vaccines; administer the first 2 doses at least 4 weeks
apart and the third dose 6–12 months after the second; Tdap can substitute for
any one of the doses of Td in the 3-dose primary series. The booster dose of tetanus
and diphtheria toxoid-containing vaccine should be administered to adults who
have completed a primary series and if the last vaccination was received 10 or
more years previously. Tdap or Td vaccine may be used, as indicated.
BBBB.... Varicella vaccinationVaricella vaccinationVaricella vaccinationVaricella vaccination
All adults without evidence of immunity to varicella should receive 2 doses of
single-antigen varicella vaccine if not previously vaccinated or the second dose if
they have received only one dose, unless they have a medical contraindication.
Special consideration should be giveSpecial consideration should be giveSpecial consideration should be giveSpecial consideration should be given to those whon to those whon to those whon to those who
a) have close contact with persons at high risk for severe disease (e.g., healthcare
personnel and family contacts of persons with immunocompromising conditions)
or
b) are at high risk for exposure or transmission (e.g., teachers; child care
employees; residents and staff members of institutional settings, including
correctional institutions; college students; military personnel; adolescents and
adults living in households with children; nonpregnant women of childbearing
age; and international travelers).
35……………………………GOOD MEDICAL PRACTICE …...………………………
35
Evidence of immunity to varicella in adults includes any of the following:Evidence of immunity to varicella in adults includes any of the following:Evidence of immunity to varicella in adults includes any of the following:Evidence of immunity to varicella in adults includes any of the following:
a) documentation of 2 doses of varicella vaccine at least 4 weeks apart;
b) U.S.-born before 1980 (although for healthcare personnel and pregnant women,
birth before 1980 should not be considered evidence of immunity);
c) history of varicella based on diagnosis or verification of varicella by a
healthcare provider (for a patient reporting a history of or presenting with an
atypical case, a mild case, or both, healthcare providers should seek either an
epidemiologic link with a typical varicella case or to a laboratory-confirmed case
or evidence of laboratory confirmation, if it was performed at the time of acute
disease).
d) history of herpes zoster based on diagnosis or verification of herpes zoster by a
healthcare provider; or
e) laboratory evidence of immunity or laboratory confirmation of disease.
CCCC. Seasonal Influenza vaccination. Seasonal Influenza vaccination. Seasonal Influenza vaccination. Seasonal Influenza vaccination
Vaccinate all persons age 50 years and older as well as any younger persons who
would like to decrease their risk of getting influenza. Vaccinate persons ages 19
through 49 years with any of the following indications.
Medical: Chronic disorders of the cardiovascular or pulmonary systems, including
asthma; chronic metabolic diseases, including diabetes mellitus; renal or hepatic
dysfunction, hemoglobinopathies, or immunocompromising conditions (including
immunocompromising conditions caused by medications or human
immunodeficiency virus [HIV]); cognitive, neurologic or neuromuscular disorders;
and pregnancy during the influenza season. No data exist on the risk for severe or
complicated influenza disease among persons with asplenia; however, influenza is
a risk factor for secondary bacterial infections that can cause severe disease among
persons with asplenia.
36……………………………GOOD MEDICAL PRACTICE …...………………………
36
Occupational: All healthcare personnel, including those employed by long-term
care and assisted-living facilities, and caregivers of children younger than age 5
years.
Others: Residents of nursing homes and other long-term care and assisted-living
facilities; persons likely to transmit influenza to persons at high risk (e.g., in-home
household contacts and caregivers of children younger than age 5 years, persons
50 years and older, and persons of all ages with high-risk condition[s]).
Healthy, nonpregnant adults younger than age 50 years without high-risk medical
conditions who are not contacts of severely immunocompromised persons in
special care units can receive either intranasally administered live, attenuated
influenza vaccine (FluMist®) or inactivated vaccine. Other persons should receive
the inactivated vaccine.
DDDD. Pneumococcal polysaccharide (PPSV) vaccination. Pneumococcal polysaccharide (PPSV) vaccination. Pneumococcal polysaccharide (PPSV) vaccination. Pneumococcal polysaccharide (PPSV) vaccination
Vaccinate all persons with the following indications.
Medical: Chronic lung disease (including asthma); chronic cardiovascular diseases;
diabetes mellitus; chronic liver diseases, cirrhosis; chronic alcoholism; functional
or anatomic asplenia (e.g., sickle cell disease or splenectomy [if elective
spletnectomy is planned, vaccinate at least 2 weeks before surgery]);
immunocompromising conditions (including chronic renal failure or nephrotic
syndrome); and cochlear implants and cerebrospinal fluid leaks. Vaccinate as close
to HIV diagnosis as possible.
Others: Residents of nursing homes or long-term care facilities and persons who
smoke cigarettes.
ACIP Releases 2010 Immunization Schedules.
Available at: http://www.cdc.gov/vaccines/pubs/ACIP-list.htm.
37……………………………GOOD MEDICAL PRACTICE …...………………………
37
6- My exercise prescription for this man
The benefitThe benefitThe benefitThe benefitssss o o o of exercise are:f exercise are:f exercise are:f exercise are:
• Maintain normal BMI.
• Reduce elvation of blood pressure.
• Reduce cholesterols.
• Prevent cancers.
• Physical fitness.
Intervention Intervention Intervention Intervention ::::
• Exercise guidelines should be tailored to patient with his fitness level .
• Regular aerobic physical exercise e.g. brisk walking at least 30 minutes per
day most days of the week. (JNC7).
• ideally on most days of week but at least 3 days/week.
Tips to help start physical activityTips to help start physical activityTips to help start physical activityTips to help start physical activity : : : :
• Identify an activity that will be enjoyed.
• Start slowly, perhaps 5-10 minutes at a time.
• Increase duration and intensity slowly.
• Consider doing exercise in a group or with a partner.
• Prevent boredom by varying the activities.
• Set realistic goals.
• Encourage people to reward themselves when goals are met.
38……………………………GOOD MEDICAL PRACTICE …...………………………
38
7. I would conduct dietary counseling to this man
based on the above findings of clinical examination.
I will ask this patient about the number of meals and snacks eaten in a 24-hour
period, dining-out habits and frequency of consumption of fruits, vegetables,
meats, poultry, fish, dairy products and desserts to know the dietary habits of the
patient.
This patient in the prehypertensionThis patient in the prehypertensionThis patient in the prehypertensionThis patient in the prehypertension stage, who will require lifestyle
modification.
• Lifestyle modifications reduce BP and decrease cardiovascular risk.
• Dietary Approaches to Stop Hypertension (DASH) eating plan
o It is rich in potassium and calcium, dietary sodium reduction,
physical activity.
o Consume a diet rich in fruits.
o Vegetables and low fat dairy products with a reduced content of
saturated and total fat.
This patient is advised to take breaThis patient is advised to take breaThis patient is advised to take breaThis patient is advised to take breakfast as kfast as kfast as kfast as
• It is an important meal because it offers the opportunity to eat low fat,
whole grain foods such as hot or cold cereal, which is also an excellent
source of calcium if it includes skim or low-fat milk.
• Breakfast is intended to break the overnight fast.
• A good breakfast helps prevent hunger and overeating later in the day.
This patient will advised to reduce fat consumption,This patient will advised to reduce fat consumption,This patient will advised to reduce fat consumption,This patient will advised to reduce fat consumption, which iswhich iswhich iswhich is
• An important step in reducing serum cholesterol and triglyceride levels.
• Lowering the risk of cardiovascular disease and some cancers.
• Preventing and treating overweight.
39……………………………GOOD MEDICAL PRACTICE …...………………………
39
This patient should prevent eating outside the home if he does thatThis patient should prevent eating outside the home if he does thatThis patient should prevent eating outside the home if he does thatThis patient should prevent eating outside the home if he does that
becausebecausebecausebecause :
• Meals eaten away from home contain more fat and calories than those
prepared at home.
This patient should be encourage tThis patient should be encourage tThis patient should be encourage tThis patient should be encourage to eat food rich in fiberso eat food rich in fiberso eat food rich in fiberso eat food rich in fibers becausebecausebecausebecause::::
• It decreases cardiovascular disease, as well as cancers of the digestive tract.
• Soluble fiber, which is contained in cereal grains, citrus fruits, apples, beans
and corn, has also been shown to reduce serum cholesterol and low-density
lipoprotein levels.
• Also fresh fruits and vegetables are excellent sources of fiber and
phytochemicals, which may explain their probable protective effect against
certain cancers of the digestive tract
8. I would help this man to quit smoking
• I should encourage this man making a quit attempt to use both counseling
and medication, as the combination of counseling and medication is more
effective than either alone. I think medications to stop smoking are not
available in Egypt
SMOKING CESSATSMOKING CESSATSMOKING CESSATSMOKING CESSATION COUNSELING STRATEGY FOR OFFICE ION COUNSELING STRATEGY FOR OFFICE ION COUNSELING STRATEGY FOR OFFICE ION COUNSELING STRATEGY FOR OFFICE
PRACTICEPRACTICEPRACTICEPRACTICE
I will use the five A’s (Ask, Advise, Assess, Assist, and Arrange) mode when
treating this patients.
1. ASK—about smoking at every visit: “Do you smoke?”
2. ADVISE: I will advice him to stop.
a) CLEAR ADVICECLEAR ADVICECLEAR ADVICECLEAR ADVICE: “I think it is important for you to quit smoking urge
every tobacco user (or using chewing tobacco) now, and I can help you.” to
quit. “Cutting down while you are ill is not enough.” “Occasional or light
smoking is still dangerous.”
40……………………………GOOD MEDICAL PRACTICE …...………………………
40
b) STRONGSTRONGSTRONGSTRONG: “As your clinician, I need you to know that quitting smoking is
the most important thing you can do to protect your health now and in the
future. The clinic staff and I will help you.”
c) PERSONALIZEDPERSONALIZEDPERSONALIZEDPERSONALIZED: Quitting may dramatically improve your health,
reduce your risk for hypertension, DM and coronary heart disease and you
will not suffer like your father Inshaa Allah.
3. ASSESS—readiness to quit: “Are you interested in quitting?”
4. ASSIST—the smoker in stopping smoking.
a. For smokers ready to quit. For smokers ready to quit. For smokers ready to quit. For smokers ready to quit
1. Set a quit date. Ideally, the quit date should be within 2 weeks.
2. Tell family, friends, and coworkers about quitting and request
understanding and support.
3. Anticipate challenges to the upcoming quit attempt, particularly during the
critical first few weeks. These include nicotine withdrawal symptoms.
4. Remove tobacco products from your environment. Prior to quitting, avoid
smoking in places where you spend a lot of time (e.g., work, home, car).
Make your home smoke-free.
b. For smokers not ready to quit
1. Discuss advantages and barriers to cessation, from smoker’s viewpoint.
2. Provide motivational booklet to take home.
3. Advise smoker to avoid exposing family members to passive smoke.
4. Indicate willingness to help when the smoker is ready.
5. Ask again about smoking at the next visit.
5. ARRANGE—follow-up visits.
a. Make follow-up appointment 1 week after quit date.
b. At follow-up, ask about smoking status.
c. For smokers who have quit:
(1) Congratulate!
(2) Ask smoker to identify future high-risk situations.
41……………………………GOOD MEDICAL PRACTICE …...………………………
41
(3) Rehearse coping strategies for future high-risk situations.
d. For smokers who have not quit:
(1) Ask: “What were you doing when you had that first cigarette?”
(2) Ask: “What did you learn from the experience?”
(3) Ask smoker to set a new “quit date.”
PHARMACOTHERAPYPHARMACOTHERAPYPHARMACOTHERAPYPHARMACOTHERAPY
• The pharmacologic agents approved by the U.S. Food and Drug
Administration (FDA) for the treatment of tobacco dependence have
similar long-term success rates.
• These agents include five forms of nicotine replacement therapy (NRT; e.g.,
gum, patch, nasal spray, inhaler, lozenge) and bupropion sustained release .
ALTERNATIVE THERAPIESALTERNATIVE THERAPIESALTERNATIVE THERAPIESALTERNATIVE THERAPIES
• A number of complementary and alternative therapies such as hypnosis and
acupuncture have been considered for smoking cessation.
FOLLOWFOLLOWFOLLOWFOLLOW----UPUPUPUP
• Relapse (in general or, more specifically, smoking on seven consecutive days
or once each week over two consecutive weeks) is common. Physicians can
use a number of brief strategies to help prevent relapse. At a minimum,
patients should be encouraged to identify their smoking cues and triggers
and decide on alternative coping strategies before they attempt to quit
smoking. During follow-up visits, physicians should assess patients’
progress, congratulate success, and encourage continued cessation. Patients
also should be encouraged to discuss the benefits of cessation including
health benefits; the successes they have had (e.g., duration of abstinence,
effective coping strategies); and problems or barriers to cessation (e.g.,
negative mood, irritability, alcohol, other smokers).
• For patients who have experienced a relapse, it is recommended that the
physician review with the patient the circumstances surrounding the relapse
42……………………………GOOD MEDICAL PRACTICE …...………………………
42
and elicit a new commitment to quit. It also is important to counsel these
patients on the proper use of pharmacotherapy and to arrange a timely
follow-up visit (i.e., about one week after the new quit date). Behavior
modification for smoking cessation also should be considered. Finally,
patients should be reminded that a relapse is an opportunity for them to
learn what tempted them to smoke and how to cope better with similar
situations in the future.
Counseling for AllCounseling for AllCounseling for AllCounseling for All----AgesAgesAgesAges
Injury prevention :
1. Seats.
2. Helmets-bicycles, motorcycles.
3. Smoke detector.
4. Firearm- safe storage or removal.
5. Interpersonal violence- physical, emotional, sexual.
Substance use :
1. Avoid tobacco use.
2. Avoid underage drinking and illicit drug use.
3. Avoid EtOH use while driving, swimming, boating.
Sexual behavior :
1. Sexual disease prevention – abstinence, avoid high-risk behavior.
2. Unintended pregnancy – contraception.
Diet and exercise :
1. Limit fat and cholesterol; maintain caloric balance, emphasize grains,
fruits, vegetables.
43……………………………GOOD MEDICAL PRACTICE …...………………………
43
2. Women – adequate calcium intake (prevent osteoporosis).
3. Regular exercise.
Sun exposure – avoid excess mind-day, use protective clothing; avoid
sunburn.
Dental health :
1. Regular visits to dental care provider.
2. Daily – brush with fluoride toothpaste.
Ages Ages Ages Ages uuuup to 24 yearsp to 24 yearsp to 24 yearsp to 24 years : : : :
Screen the following :
1. Height and weight
2. Blood pressure – periodic blood pressure for age older than 21
3. Pap smear every 1 to 3 years – if sexually active at present or in past
4. Chlamydia screening annually - if sexually active at present or in past
5. Rubella serology or vaccinaction history
6. Assess for alcohol drinking
AGE SPECIFIC COUNSELINGAGE SPECIFIC COUNSELINGAGE SPECIFIC COUNSELINGAGE SPECIFIC COUNSELING
Immunization :
1. Confirm primary immunization.
2. Confirm previous infection with chicken pox if no primary infection,
consider vermicelli vaccine.
3. Hepatitis B – if not previously immunized.
4. Rubella – girls older than 12 years old.
5. Consider PPD – immigrants, TB contacts.
44……………………………GOOD MEDICAL PRACTICE …...………………………
44
Ages 25 to 64Ages 25 to 64Ages 25 to 64Ages 25 to 64 YE YE YE YEAAAARSRSRSRS : : : :
Screening
1. Blood pressure .
2. Height and weight.
3. Total blood cholesterol – women age 45 to 64, men ages 35 to 64.
4. Pap smear every 1 to 3 years – if sexually active at present or in past
5. Fecal occult blood test:annually and sigmoidoscopy every 3 to 5 years
(older than 50 years).
6. Mammography every year (with or without clinical breast examination
(CBE) – women age 50 to 69 years).
7. Assess for alcohol drinking.
8. Rubella (women of childbearing age -) – serology or vaccination history.
AGE SPECIFIC COUNSELINGAGE SPECIFIC COUNSELINGAGE SPECIFIC COUNSELINGAGE SPECIFIC COUNSELING
Sexual behavior – erectile dysfunction or dyspareunia.
ImmunizationsImmunizationsImmunizationsImmunizations
1. Tetanus-diphtheria (Td) every 10 years.
2. Rubella – women of childbearing age.
ChemoprophylaxisChemoprophylaxisChemoprophylaxisChemoprophylaxis
1. Multi-vitamin with folic acid – women planning pregnancy.
2. Discus hormone prophylaxis – peri- or post-menopaual women.
45……………………………GOOD MEDICAL PRACTICE …...………………………
45
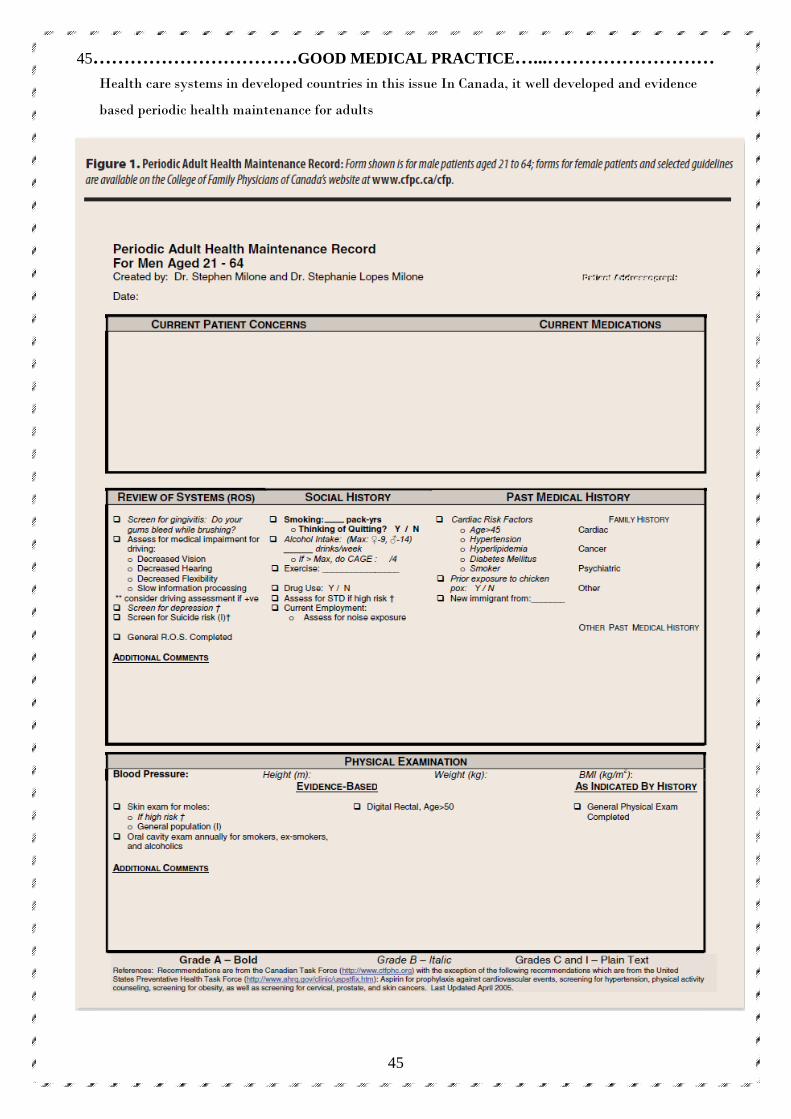
Health care systems in developed countries in this issue In Canada, it well developed and evidence
based periodic health maintenance for adults
46……………………………GOOD MEDICAL PRACTICE …...………………………
46
47……………………………GOOD MEDICAL PRACTICE …...………………………
47
Summary of Recommendations and Evidence regarding Prostatic
Specific Antigen test (PSA) as a tool for screening of prostate cancer
1. The U.S. Preventive Services Task Force (USPSTF) concludes that the
current evidence is insufficient to assess the balance of benefits and harms of
prostate cancer screening in men younger than 75 years. I statement.
2. The USPSTF recommends against screening for prostate cancer in men 75
years and older. D recommendation.
Detection. The USPSTF found convincing evidence that prostate-specific
antigen (PSA) screening can detect some cases of prostate cancer.
Benefits of detection and early treatment. In men younger
than 75 years, the USPSTF found inadequate evidence to determine whether
treatment for prostate cancer detected by screening improves health outcomes,
compared with treatment after clinical detection.
In men 75 years and older, the USPSTF found adequate evidence that the
incremental benefits from treatment for prostate cancer detected by screening are
small to none.
Harms of detection and early treatment. The USPSTF
found convincing evidence that treatment for prostate cancer detected by
screening causes moderate-to-substantial harms, such as erectile dysfunction,
urinary incontinence, bowel dysfunction, and death. These harms are especially
important because some men with prostate cancer who are treated would not have
developed symptoms related to cancer during their lifetime. There is also adequate
Professionalism and Professionalism and Professionalism and Professionalism and
communication issuescommunication issuescommunication issuescommunication issues
48……………………………GOOD MEDICAL PRACTICE …...………………………
48
evidence that the screening process produces at least small harms, including pain
and discomfort associated with prostate biopsy and psychological effects of false-
positive test results.
USPSTF assessment. The USPSTF concludes that in men younger
than 75 years, the benefits of screening for prostate cancer are uncertain, and the
balance of benefits and harms cannot be determined.
In men 75 years and older, there is moderate certainty that the harms of screening
for prostate cancer outweigh the benefits.
Clinical ConsiderationsClinical ConsiderationsClinical ConsiderationsClinical Considerations
• Patient population. This recommendation applies to men in the
general U.S. population.
• Risk assessment. Older men, black men, and men with a family
history of prostate cancer are at increased risk of diagnosis and death from
prostate cancer. The previously described gaps in the evidence regarding
potential benefits of screening also apply to these men.
• Screening tests. The PSA test is more sensitive than the digital
rectal examination for detecting prostate cancer. The conventional PSA
screening cutpoint of 4.0 ng per mL (4.0 mcg per L) detects many prostate
cancer cases; however, some early cases of prostate cancer will be missed by
this cutpoint. Using a lower cutpoint to define an abnormal PSA level
detects more cases of cancer.
The proportion of cancer cases detected by lower cutpoints that would become
clinically apparent is unknown; lower cutpoints would label many more men as
potentially having cancer. For example, lowering the PSA cutpoint to 2.5 ng per
mL (2.5 mcg per L) would more than double the number of U.S. men between 40
and 69 years of age with abnormal results.
49……………………………GOOD MEDICAL PRACTICE …...………………………
49
Variations of PSA screening, including the use of age-adjusted PSA cutpoints, free
PSA, PSA density, PSA velocity, PSA slope, and PSA doubling time, have been
proposed to improve detection of “clinically important” prostate cancer cases.
However, no evidence suggests that any of these testing strategies improves
health outcomes.
• Suggestions for practice. Given the uncertainties and
controversy surrounding prostate cancer screening in men younger than 75
years, physicians should not order PSA testing without first discussing with
the patient the potential but uncertain benefits and the known harms of
prostate cancer screening and treatment. Men should be informed of the
gaps in the evidence and should be assisted in considering their personal
preferences before deciding whether to be tested.
• Treatment. Because of the uncertainty about the benefits of treating
prostate cancer detected by screening in men younger than 75 years, there is
no consensus regarding optimal treatment. Current management strategies
for localized prostate cancer include watchful waiting (observation with
palliative treatment for symptoms only), active surveillance (periodic
biochemical monitoring with conversion to curative treatment for signs of
disease progression), radical prostatectomy, external-beam radiation
therapy, and brachytherapy (or radioactive seed implantation therapy).
If treatment for prostate cancer detected by screening improves health outcomes,
the population most likely to benefit from screening will be men 50 to 74 years of
age. Even if prostate cancer screening is determined to be effective, the length of
time required to experience a mortality benefit is greater than 10 years. Because a
75-year-old man has an average life expectancy of about 10 years, few men 75
years and older would experience a mortality benefit. Similarly, men younger
than 75 years who have chronic medical problems and a life expectancy of less
than 10 years are also unlikely to benefit from screening and treatment.
50……………………………GOOD MEDICAL PRACTICE …...………………………
50
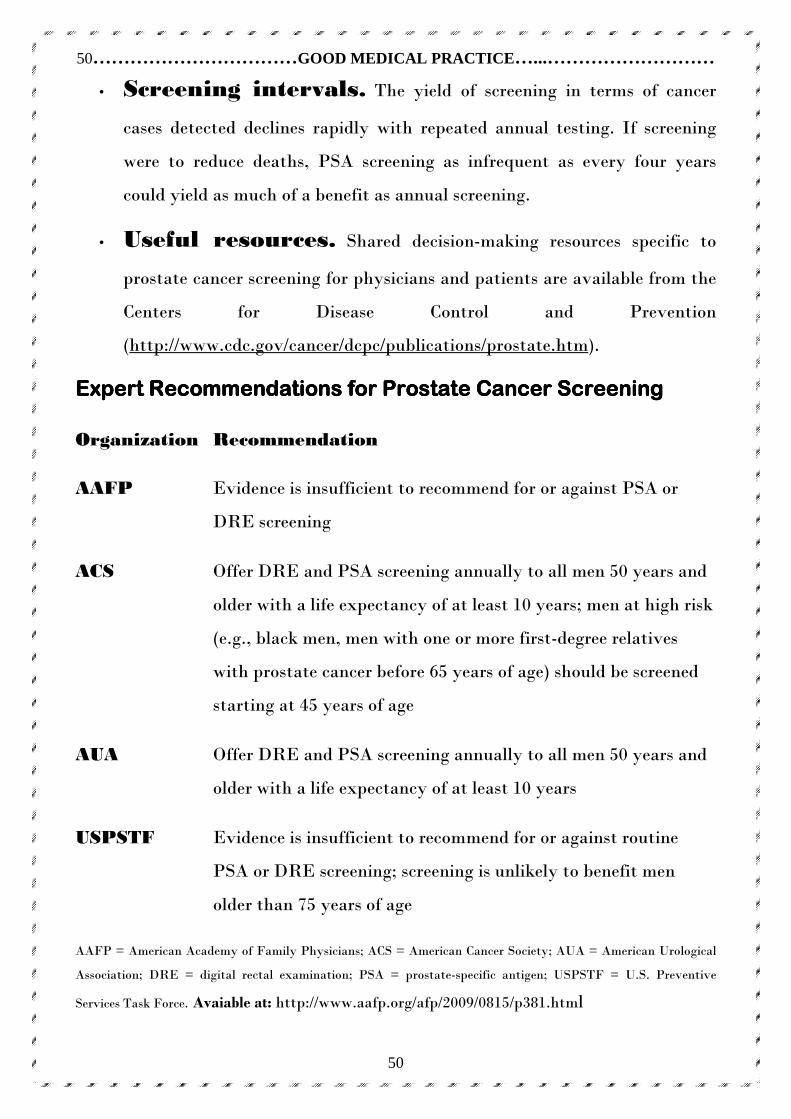
• Screening intervals. The yield of screening in terms of cancer
cases detected declines rapidly with repeated annual testing. If screening
were to reduce deaths, PSA screening as infrequent as every four years
could yield as much of a benefit as annual screening.
• Useful resources. Shared decision-making resources specific to
prostate cancer screening for physicians and patients are available from the
Centers for Disease Control and Prevention
(http://www.cdc.gov/cancer/dcpc/publications/prostate.htm).
Expert Recommendations for Prostate CaExpert Recommendations for Prostate CaExpert Recommendations for Prostate CaExpert Recommendations for Prostate Cancer Screeningncer Screeningncer Screeningncer Screening
Organization Recommendation
AAFP Evidence is insufficient to recommend for or against PSA or
DRE screening
ACS Offer DRE and PSA screening annually to all men 50 years and
older with a life expectancy of at least 10 years; men at high risk
(e.g., black men, men with one or more first-degree relatives
with prostate cancer before 65 years of age) should be screened
starting at 45 years of age
AUA Offer DRE and PSA screening annually to all men 50 years and
older with a life expectancy of at least 10 years
USPSTF Evidence is insufficient to recommend for or against routine
PSA or DRE screening; screening is unlikely to benefit men
older than 75 years of age
AAFP = American Academy of Family Physicians; ACS = American Cancer Society; AUA = American Urological
Association; DRE = digital rectal examination; PSA = prostate-specific antigen; USPSTF = U.S. Preventive
Services Task Force. Avaiable at: http://www.aafp.org/afp/2009/0815/p381.html
51……………………………GOOD MEDICAL PRACTICE …...………………………
51
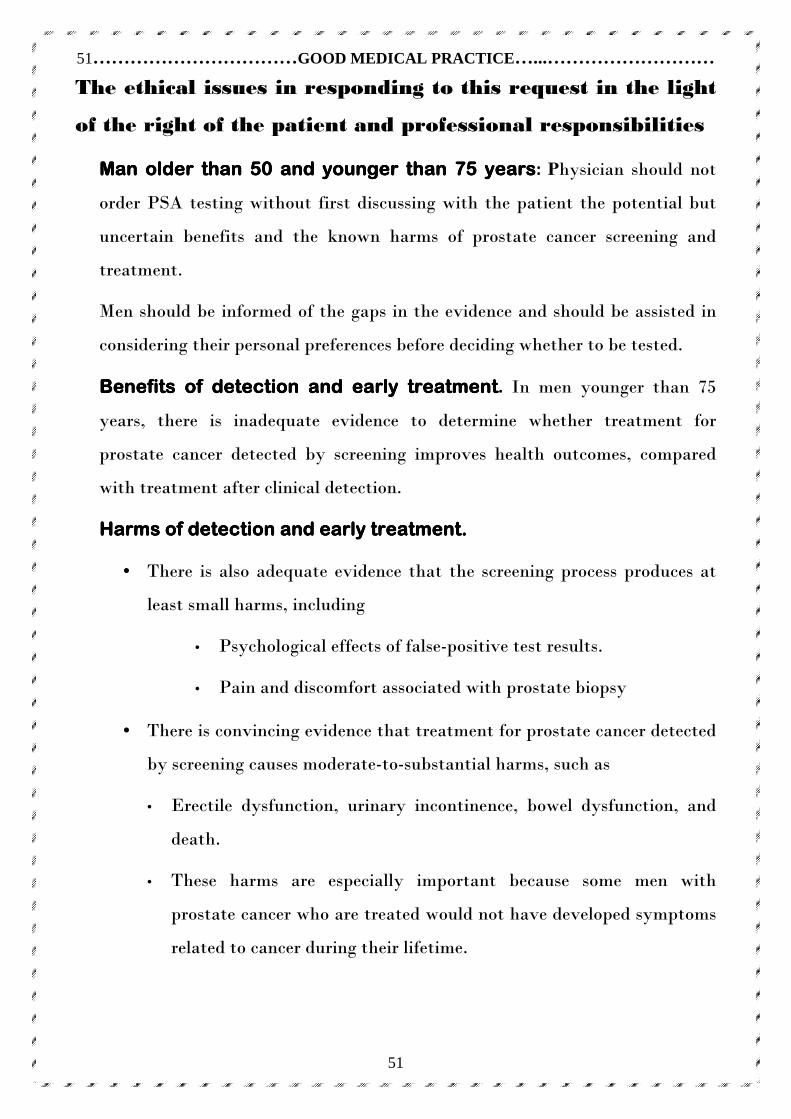
The ethical issues in responding to this request in the light
of the right of the patient and professional responsibilities
Man Man Man Man older than 50 and younger than 75 yearsolder than 50 and younger than 75 yearsolder than 50 and younger than 75 yearsolder than 50 and younger than 75 years: Physician should not
order PSA testing without first discussing with the patient the potential but
uncertain benefits and the known harms of prostate cancer screening and
treatment.
Men should be informed of the gaps in the evidence and should be assisted in
considering their personal preferences before deciding whether to be tested.
Benefits of detection and early treatmentBenefits of detection and early treatmentBenefits of detection and early treatmentBenefits of detection and early treatment. In men younger than 75
years, there is inadequate evidence to determine whether treatment for
prostate cancer detected by screening improves health outcomes, compared
with treatment after clinical detection.
Harms of detection and early treatment. Harms of detection and early treatment. Harms of detection and early treatment. Harms of detection and early treatment.
• There is also adequate evidence that the screening process produces at
least small harms, including
• Psychological effects of false-positive test results.
• Pain and discomfort associated with prostate biopsy
• There is convincing evidence that treatment for prostate cancer detected
by screening causes moderate-to-substantial harms, such as
• Erectile dysfunction, urinary incontinence, bowel dysfunction, and
death.
• These harms are especially important because some men with
prostate cancer who are treated would not have developed symptoms
related to cancer during their lifetime.
52……………………………GOOD MEDICAL PRACTICE …...………………………
52
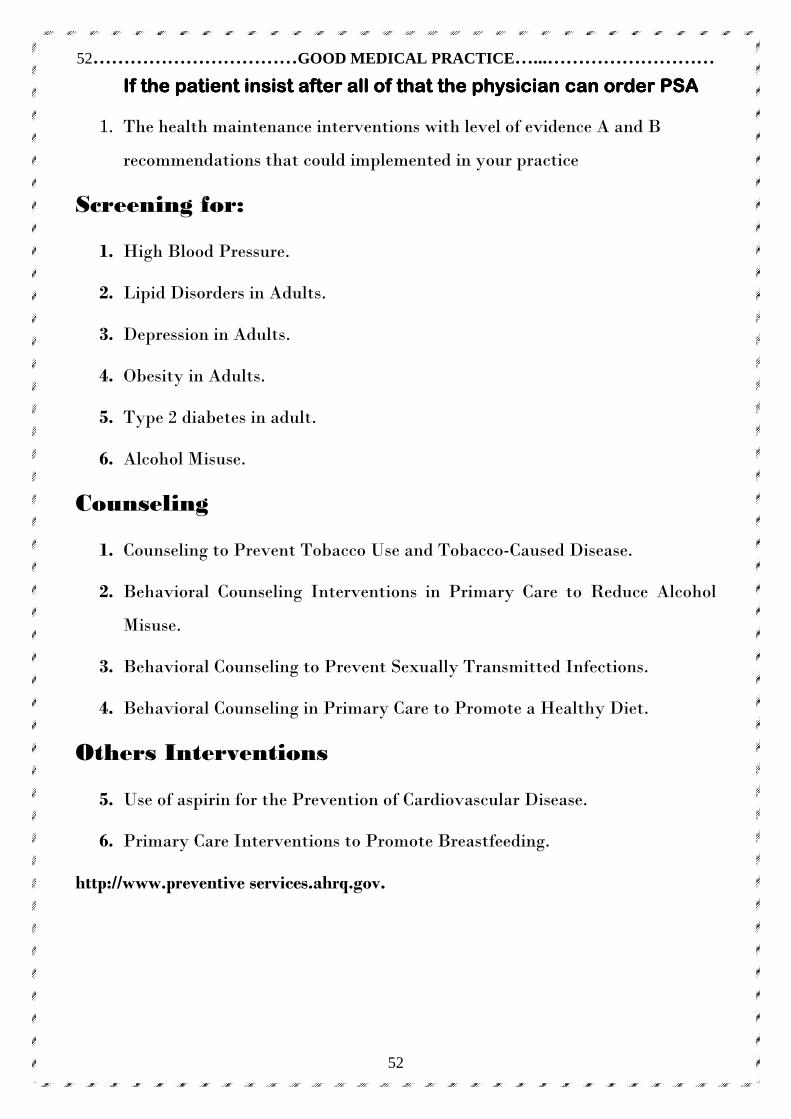
If the patient insist after all of that the physician can order PSAIf the patient insist after all of that the physician can order PSAIf the patient insist after all of that the physician can order PSAIf the patient insist after all of that the physician can order PSA
1. The health maintenance interventions with level of evidence A and B
recommendations that could implemented in your practice
Screening for:
1. High Blood Pressure.
2. Lipid Disorders in Adults.
3. Depression in Adults.
4. Obesity in Adults.
5. Type 2 diabetes in adult.
6. Alcohol Misuse.
Counseling
1. Counseling to Prevent Tobacco Use and Tobacco-Caused Disease.
2. Behavioral Counseling Interventions in Primary Care to Reduce Alcohol
Misuse.
3. Behavioral Counseling to Prevent Sexually Transmitted Infections.
4. Behavioral Counseling in Primary Care to Promote a Healthy Diet.
Others Interventions
5. Use of aspirin for the Prevention of Cardiovascular Disease.
6. Primary Care Interventions to Promote Breastfeeding.
http://www.preventive services.ahrq.gov.
53……………………………GOOD MEDICAL PRACTICE …...………………………
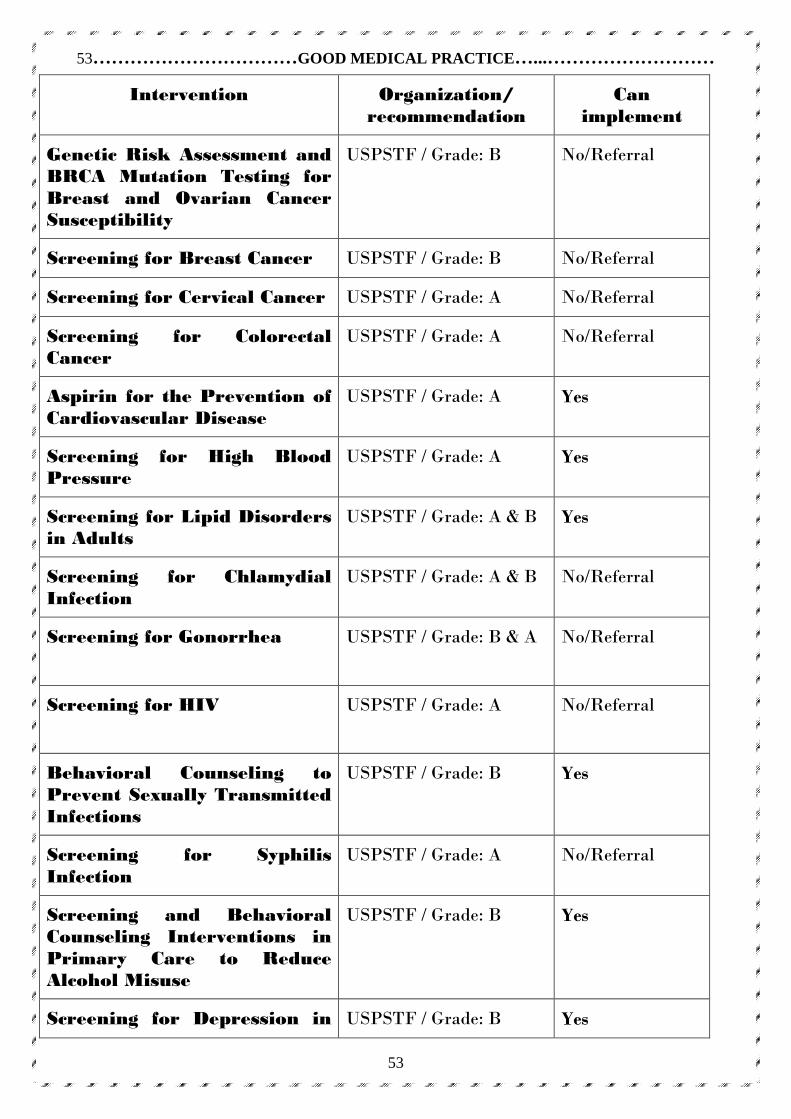
53
Intervention Organization/ recommendation
Can implement
Genetic Risk Assessment and BRCA Mutation Testing for Breast and Ovarian Cancer Susceptibility
USPSTF / Grade: B
No/Referral
Screening for Breast Cancer USPSTF / Grade: B No/Referral
Screening for Cervical Cancer USPSTF / Grade: A No/Referral
Screening for Colorectal Cancer
USPSTF / Grade: A No/Referral
Aspirin for the Prevention of Cardiovascular Disease
USPSTF / Grade: A Yes
Screening for High Blood Pressure
USPSTF / Grade: A Yes
Screening for Lipid Disorders in Adults
USPSTF / Grade: A & B Yes
Screening for Chlamydial Infection
USPSTF / Grade: A & B No/Referral
Screening for Gonorrhea
USPSTF / Grade: B & A No/Referral
Screening for HIV
USPSTF / Grade: A No/Referral
Behavioral Counseling to Prevent Sexually Transmitted Infections
USPSTF / Grade: B Yes
Screening for Syphilis Infection
USPSTF / Grade: A No/Referral
Screening and Behavioral Counseling Interventions in Primary Care to Reduce Alcohol Misuse
USPSTF / Grade: B Yes
Screening for Depression in USPSTF / Grade: B Yes
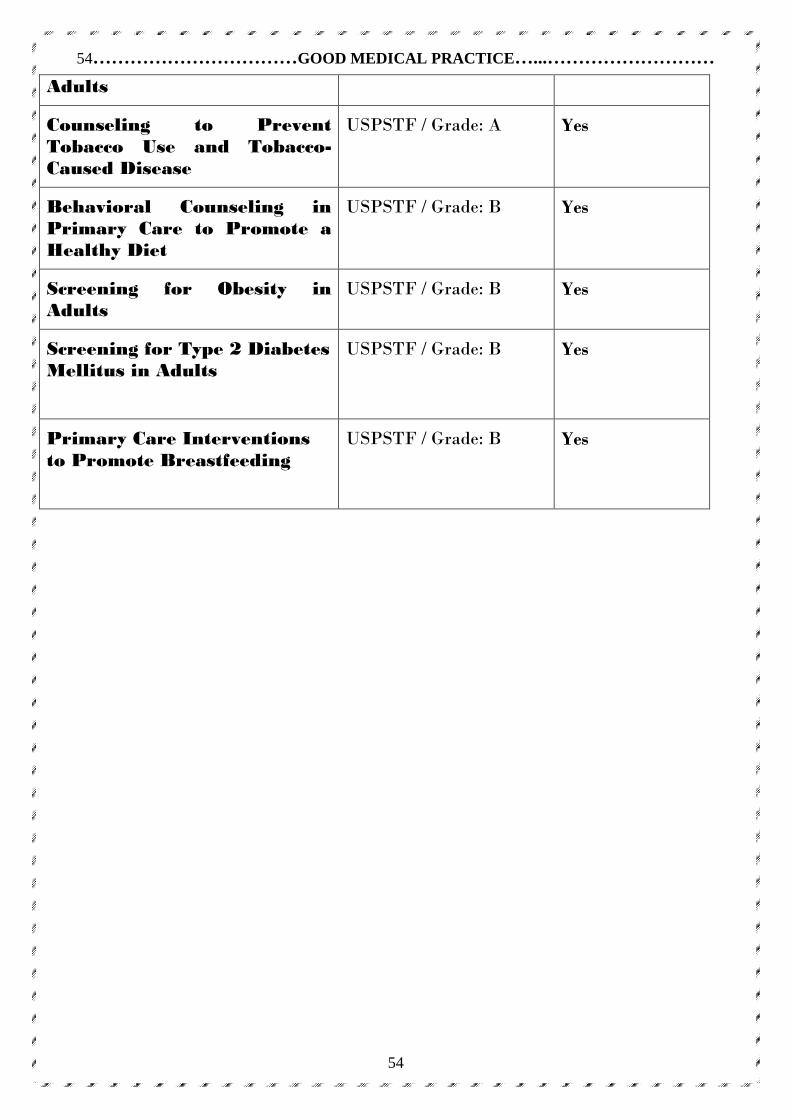
54……………………………GOOD MEDICAL PRACTICE …...………………………
54
Adults
Counseling to Prevent Tobacco Use and Tobacco-Caused Disease
USPSTF / Grade: A Yes
Behavioral Counseling in Primary Care to Promote a Healthy Diet
USPSTF / Grade: B Yes
Screening for Obesity in Adults
USPSTF / Grade: B Yes
Screening for Type 2 Diabetes Mellitus in Adults
USPSTF / Grade: B Yes
Primary Care Interventions to Promote Breastfeeding
USPSTF / Grade: B Yes
55……………………………GOOD MEDICAL PRACTICE …...………………………
55
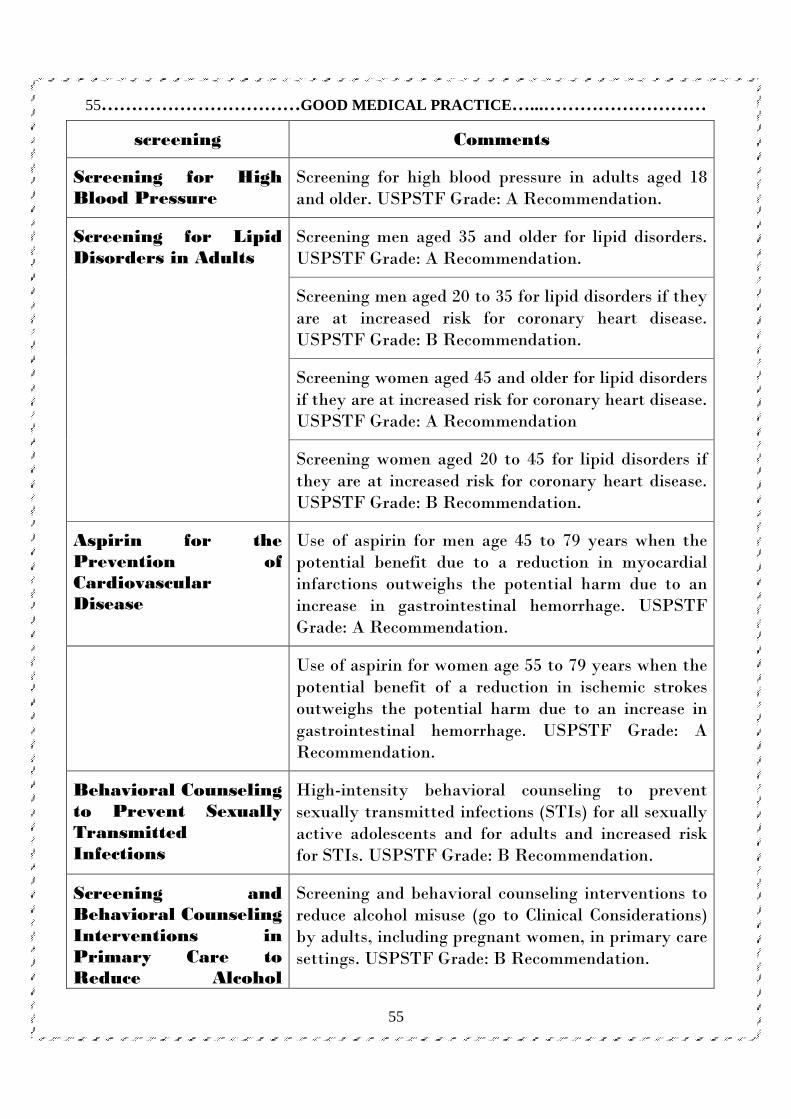
screening Comments
Screening for High Blood Pressure
Screening for high blood pressure in adults aged 18 and older. USPSTF Grade: A Recommendation.
Screening men aged 35 and older for lipid disorders. USPSTF Grade: A Recommendation.
Screening men aged 20 to 35 for lipid disorders if they are at increased risk for coronary heart disease. USPSTF Grade: B Recommendation.
Screening women aged 45 and older for lipid disorders if they are at increased risk for coronary heart disease. USPSTF Grade: A Recommendation
Screening for Lipid Disorders in Adults
Screening women aged 20 to 45 for lipid disorders if they are at increased risk for coronary heart disease. USPSTF Grade: B Recommendation.
Aspirin for the Prevention of Cardiovascular Disease
Use of aspirin for men age 45 to 79 years when the potential benefit due to a reduction in myocardial infarctions outweighs the potential harm due to an increase in gastrointestinal hemorrhage. USPSTF Grade: A Recommendation.
Use of aspirin for women age 55 to 79 years when the potential benefit of a reduction in ischemic strokes outweighs the potential harm due to an increase in gastrointestinal hemorrhage. USPSTF Grade: A Recommendation.
Behavioral Counseling to Prevent Sexually Transmitted Infections
High-intensity behavioral counseling to prevent sexually transmitted infections (STIs) for all sexually active adolescents and for adults and increased risk for STIs. USPSTF Grade: B Recommendation.
Screening and Behavioral Counseling Interventions in Primary Care to Reduce Alcohol
Screening and behavioral counseling interventions to reduce alcohol misuse (go to Clinical Considerations) by adults, including pregnant women, in primary care settings. USPSTF Grade: B Recommendation.
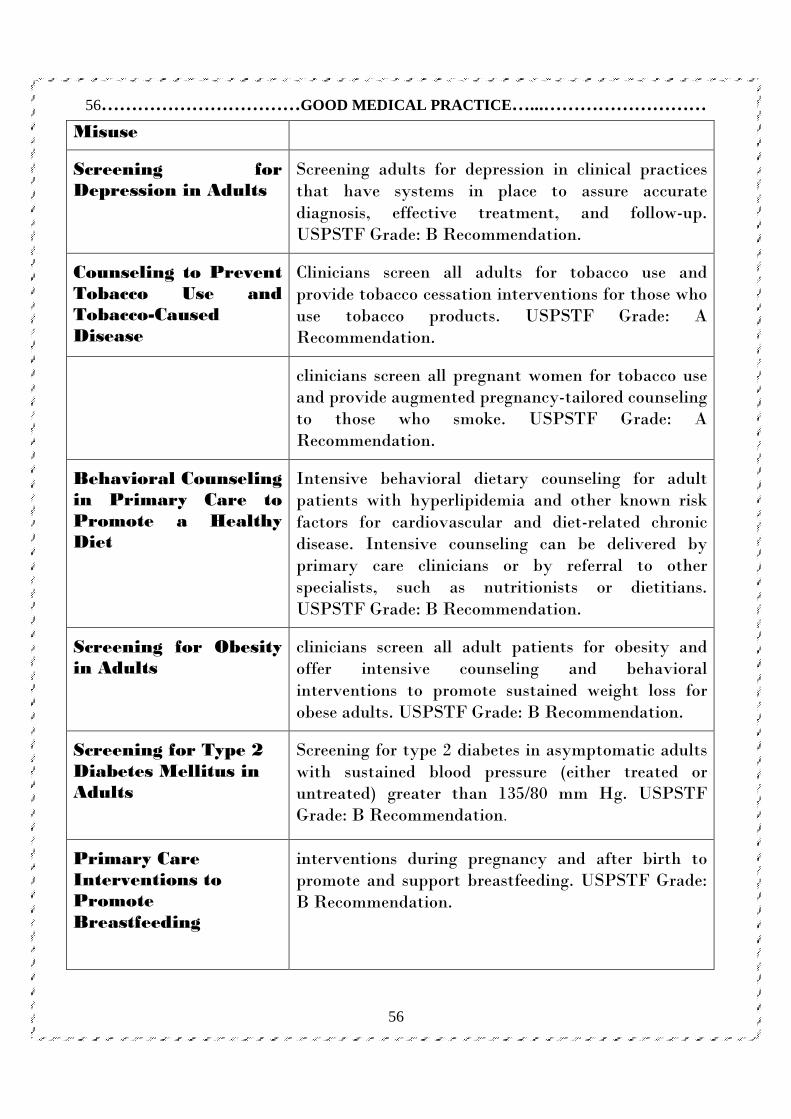
56……………………………GOOD MEDICAL PRACTICE …...………………………
56
Misuse
Screening for Depression in Adults
Screening adults for depression in clinical practices that have systems in place to assure accurate diagnosis, effective treatment, and follow-up. USPSTF Grade: B Recommendation.
Counseling to Prevent Tobacco Use and Tobacco-Caused Disease
Clinicians screen all adults for tobacco use and provide tobacco cessation interventions for those who use tobacco products. USPSTF Grade: A Recommendation.
clinicians screen all pregnant women for tobacco use and provide augmented pregnancy-tailored counseling to those who smoke. USPSTF Grade: A Recommendation.
Behavioral Counseling in Primary Care to Promote a Healthy Diet
Intensive behavioral dietary counseling for adult patients with hyperlipidemia and other known risk factors for cardiovascular and diet-related chronic disease. Intensive counseling can be delivered by primary care clinicians or by referral to other specialists, such as nutritionists or dietitians. USPSTF Grade: B Recommendation.
Screening for Obesity in Adults
clinicians screen all adult patients for obesity and offer intensive counseling and behavioral interventions to promote sustained weight loss for obese adults. USPSTF Grade: B Recommendation.
Screening for Type 2 Diabetes Mellitus in Adults
Screening for type 2 diabetes in asymptomatic adults with sustained blood pressure (either treated or untreated) greater than 135/80 mm Hg. USPSTF Grade: B Recommendation.
Primary Care Interventions to Promote Breastfeeding
interventions during pregnancy and after birth to promote and support breastfeeding. USPSTF Grade: B Recommendation.
57……………………………GOOD MEDICAL PRACTICE …...………………………
57
The debate regarding conducting annual comprehensive medical examinations for
health maintenance versus periodic selective health maintenance examination
reflecting on these Evidence suggests that the PHE improves delivery of some
recommended preventive services and may lessen patient worry. Although additional
research is needed to clarify the long term benefits, harms, and costs of receiving the
PHE, evidence of benefits in this study justifies implementation of the PHE in
clinical practice.
♠ In general practice the use of electronic medical records (EMRs) instead of paper
patient records has become more and more common.
♠ In an EMR data about a patient’s medical history, clinical outcomes and
demographic information is recorded.
♠ It can provide information about guidelines, patient condition, clinical
outcomes and treatment.
♠ These benefits from the EMR could result in more efficient and better patient care
and care management} Use of EMRs can not only improve care management, but
can also be beneficial for research.
♠ Data collection from an EMR is less time-consuming than from a paper patient
record.
♠ However, data retrieval from the EMR is still complex and in some cases
registration of data is inadequate.
♠ Because clinical consultation is a complex interaction between caregiver
and patient, in EMRs the information is often recorded as a mixture of free-text and
coded data Registration, here understood to be all or part of patient information, is
influenced by personal, cultural, technical, health system and financial factors
A structured registration program can be validly used for A structured registration program can be validly used for A structured registration program can be validly used for A structured registration program can be validly used for
quality assessment in general practicequality assessment in general practicequality assessment in general practicequality assessment in general practice....
58……………………………GOOD MEDICAL PRACTICE …...………………………
58
Besides registration differences, the types of electronic databases available is large
and can vary in methodology, size and type of data collected.
♠ Variability in record systems and information registration makes efficient and
valid data retrieval difficult.
♠ A structured registration program (SRP) is designed for use in addition to the
EMR, and has easy data extraction possibilities.
♠ In an SRP data can be entered in a structured way, these systems are often disease
specific.
♠ SRPs use predefined fields for data entry; data (certain selected parameters) can
be entered and extracted in one way only. This results in uniformity of data with
easy extraction benefits.
♠ With such a program, the caregivers have a good overview of patients with a
certain disease over a specific period of time.
♠ Due to the easy extraction possibilities data can be used for research,
benchmarking and care management purposes.
♠ For clinical practice, such a structured registration program means the physician
has to use an extra program. Also, the structured set-up may conflict with clinical
practice.
♠ Because of that, user compliance may be lower despite the advantages. However,
as long as other solutions for valid and easy data retrieval are not generally available
or applicable, SRP can be used.
♠ To be able to confidently use SRP data, data have to agree between the EMR and
SRP programs. But evidence on this concordance is incomplete.
♠ Thiru et al reviewed the validity of data in EMRs, using data from questionnaires,
consultations, survey data or paper-based information as golden standard, but most
of these studies only concerned patient diagnoses as outcomes.
♠ The available studies of data extraction or data structuring describe solutions,
rather than assessing validity of recorded data.
♠ One study found a high concordance assessing validity between data manually
59……………………………GOOD MEDICAL PRACTICE …...………………………
59
extracted from an EMR and data that were extracted from the EMR using a
computerized method.
♠ However, these computerized methods for extraction data from the EMR are not
commonly available or applicable yet.
♠ In actual practice an additional program, SRP, is still used.
♠ There are several reasons why data in the SRP can differ from those in the
EMR: the person entering the data can differ and only specific data gathered at a
certain point in time from a particular group of patients are to be used. Differences
between the recorded data in the two programs are not unlikely.
♠ As evidence on agreement between data from EMRs and SRP programs is lacking,
this study was designed to assess such an agreement.
♠ Aim of the study is to examine the agreement between data from an SRP and
from routine EMRs, to determine whether the use of SRP data.
♠ Physicians often worry that their EMR systems might crash, leaving them without any records.
♠ The rate of system crashes without backup has not been documented.
♠ However, experience in many countries indicates that most systems work despite
lack of supervision and adherence to recommendations for installation and servicing.
♠ A literature search could find no reported incidences of catastrophic data loss; for
most users, developing a clinical EMR in an office-based system is a safe way to
proceed.
Interference with the doctor-patient relationship
Undoubtedly, having a computer on the desk does introduce a new dynamic to
the patient-doctor relationship, as does having a medical student, being
interrupted by telephone calls, or other every day occurrences. However, patients
generally find the EMR experience to be positive. In a study published in this
Electronic malfunctionElectronic malfunctionElectronic malfunctionElectronic malfunction
60……………………………GOOD MEDICAL PRACTICE …...………………………
60
issue on computer use in Canadian practices (www.cpf.ca), Lelievre and Schultz
found that computers had a positive effect on overall satisfaction with the
patient-physician encounter.
♣♣♣♣ AT THE LEVEL OF THIS SEARCH.AT THE LEVEL OF THIS SEARCH.AT THE LEVEL OF THIS SEARCH.AT THE LEVEL OF THIS SEARCH.
It is very good search which based on learning competencies.
1. I learn learning competencies in depth through this search.
2. This search has specific, measurable, relevant and applicable objectives.
3. This search included many methods & resources of teaching & learning.
♣♣♣♣ AT MYAT MYAT MYAT MY----SELF LEVELSELF LEVELSELF LEVELSELF LEVEL
1. In fact, Good medical practice was out of my scope before this search. through
next months, after this search I include it in my learning plan.
2. After this search, I will able to teach and learn Good medical practice for
undergraduate and postgraduate.
3. After this search, I know the components of health maintenance visit better
than before.
4. I learned cardiovascular risk assessment in depth.
5. After this search, I can able to conduct smoking cessation counseling in my
practice and I know the medical management of smoking cessation but it is not
available in my area, as I know.
Reflection on reading the searchReflection on reading the searchReflection on reading the searchReflection on reading the search
61……………………………GOOD MEDICAL PRACTICE …...………………………
61
6. After this search, I can mention immunization program for American adult.
7. After this search, I know the USPSTF recommendation 2009 better than
before.
8. After this search, I can able to give appropriate exercise prescription.
9. After this search, I am some confident in planning diet in adults.
10. After this search, I able to improve practice experience in implementing
health maintenance program.
11. After this search, I can able to deal with ethical issues related to implement
health maintenance program in family practice settings.
♣♣♣♣ AT THE LEVEL OF CURRICULUMSAT THE LEVEL OF CURRICULUMSAT THE LEVEL OF CURRICULUMSAT THE LEVEL OF CURRICULUMS
I think, it is better to include GOOD MEDICAL PRACTICE in undergraduate
curriculums.
♣♣♣♣ AT THE LEVEL OF FAMILY PRACTICE CENTERSAT THE LEVEL OF FAMILY PRACTICE CENTERSAT THE LEVEL OF FAMILY PRACTICE CENTERSAT THE LEVEL OF FAMILY PRACTICE CENTERS
I hope to conduct tangible health maintenance program suitable for all centers we
can organize workshop for that.
PoinPoinPoinPoints needed to be improved for good ts needed to be improved for good ts needed to be improved for good ts needed to be improved for good
medical practicemedical practicemedical practicemedical practice
62……………………………GOOD MEDICAL PRACTICE …...………………………
62
♣♣♣♣ AT THE LEVEL OF HALFAT THE LEVEL OF HALFAT THE LEVEL OF HALFAT THE LEVEL OF HALF----DAY RELEASE COURSEDAY RELEASE COURSEDAY RELEASE COURSEDAY RELEASE COURSE
I need including smoking cessation counseling in the half-day release course. I
assume that role-play is a good method of teaching and learning, playing multiple
roles regarding stage of change will be better in learning.
♣♣♣♣ AT THE LEVEL OF EGYPTIAN NATIONAL GUIDELINEAT THE LEVEL OF EGYPTIAN NATIONAL GUIDELINEAT THE LEVEL OF EGYPTIAN NATIONAL GUIDELINEAT THE LEVEL OF EGYPTIAN NATIONAL GUIDELINE
I didn't found Egyptian GOOD MEDICAL PRACTICE program in the Egyptian
national guidelines, so our professors can give advice to the responsible authority
to include it in the national guidelines.
63……………………………GOOD MEDICAL PRACTICE …...………………………
63
1- Milone SD, Milone SL. Evidence-based periodic health examination of adults
Memory aid for primary care physicians. Can Fam Physician 2006;52:40-47.
Available at: http://www.cfpc.ca/cfp/2006/Jan/vol52-jan-cme-1.asp
2- Boulware LE et al. Systematic Review: The Value of the Periodic Health
Evaluation. Ann Intern Med. 2007;146:289-300. Available at;
http://www.annals.org/content/146/4/289.full
3- Goroll, Allan H.; Mulley, Albert G. Health Maintenance and the Role, of
Screening.
Primary Care Medicine Office Evaluation and Management of the Adult Patient, 5th
Edition, Lippincott Williams & Wilkins, Chapter 3 ,2007.
4-BRITISH HYPERTENSION SOCIETY GUIDELINES. Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society2005—BHS IV. 5 - Al-Gelban KS, Al-Khaldi YM. and Diab MM. Periodic health maintenance. F.M.2007.
6 - Milone SD, Milone SL. Evidence-based periodic health examination of adults
Memory aid for primary care physicians. Can Fam Physician 2006;52:40-47.
Available at: http://www.cfpc.ca/cfp/2006/Jan/vol52-jan-cme-1.asp.
7 - Boulware LE et al. Systematic Review: The Value of the Periodic Health
Evaluation. Ann Intern Med. 2007;146:289-300. Available at;
http://www.annals.org/content/146/4/289.full
8 - Berner ES, Detmer DE, Simborg D. Will the wave finally break? A brief view
ReferencesReferencesReferencesReferences
64……………………………GOOD MEDICAL PRACTICE …...………………………
64
of the adoption of electronic medical records in the United States. J Am Med
Inform Assoc. 2005;12(1):3–7. doi: 10.1197/jamia.M1664. [PMC free article]
[PubMed] [Cross Ref de Lusignan S, Teasdale S, Little D, Zapp J, Zuckerman A,
Bates DW.
9 - Knottnerus JA. Role of the electronic patient record in the development of general practice in The Netherlands. Methods of information in medicine.
1999;38(4-5):350–4. [PubMed
10 - Dorr D, Bonner LM, Cohen AN, Shoai RS, Perrin R, Chaney E. Informatics systems to promote improved care for chronic illness: a literature review. J Am
Med Inform Assoc. 2007;14(2):156–63. doi: 10.1197/jamia.M2255. [PMC free
article] [PubMed] [Cross Ref 11 - Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, Roth E. Systematic review: impact of health information technology on quality, efficiency, and costs
of medical care. Ann Intern Med. 2006;144(10):742–52. [PubMed
12 - de Lusignan S, van Weel C. The use of routinely collected computer data for research in primary care: opportunities and challenges. Fam Pract.
2006;23(2):253–63. doi: 10.1093/fampra/cmi106. [PubMed] [Cross Ref}
13 - Roukema J, Los RK, Bleeker SE, van Ginneken AM, van der LJ, Moll HA. Paper versus computer: feasibility of an electronic medical record in general
pediatrics. Pediatrics. 2006;117(1):15–21. doi: 10.1542/peds.2004-2741. [PubMed]
65……………………………GOOD MEDICAL PRACTICE …...………………………
65
[Cross Ref} 14 - Voorham J, Denig P. Computerized extraction of information on the quality
of diabetes care from free text in electronic patient records of general practitioners.
J Am Med Inform Assoc. 2007;14(3):349–54. doi: 10.1197/jamia.M2128. [PMC free
article] [PubMed] [Cross Ref}
15 - Klein Woolthuis EP, de Grauw WJ, van Gerwen WH, Hoogen HJ van den, Lisdonk EH van de, Metsemakers JF. Identifying people at risk for undiagnosed
type 2 diabetes using the GP’s electronic medical record. Fam Pract.
2007;24(3):230–6. doi: 10.1093/fampra/cmm018. [PubMed] [Cross Ref}
16 - de Lusignan S, Hague N, van Vlymen J, Kumarapeli P. Routinely-collected
general practice data are complex, but with systematic processing can be used for
quality improvement and research. Inform Prim Care. 2006;14(1):59–66. [PubMed}
17 - Cruz-Correia RJ, Vieira-Marques PM, Ferreira AM, Almeida FC, Wyatt JC, Costa- Pereira AM. Reviewing the integration of patient data: how systems are
evolving in practice to meet patient needs. BMC Med Inform Decis Mak.
2007;7:14. doi: 10.1186/1472-6947-7-14. [PMC free article] [PubMed] [Cross Ref
18 - Liu H, Friedman C. CliniViewer: a tool for viewing electronic medical records based on natural language processing and XML. Medinfo. 2004;11(Pt 1):639–43
Los RK, van Ginneken AM, Roukema J, Moll HA, Lei J van der. Why are
66……………………………GOOD MEDICAL PRACTICE …...………………………
66
structured data different? Relating differences in data representation to the rationale of OpenSDE. Med Inform Internet Med. 2005;30(4):267–76. doi:
10.1080/14639230500367563. [PubMed] [Cross Ref
19 - Hobma S, Ram P, Muijtjens A, van der Vleuten C, Grol R. Effective improvement of doctor-patient communication: a randomised controlled trial. Br J
Gen Pract. 2006;56(529):580–6. [PMC free article] [PubMed
20 - Ammenwerth E, Schnell-Inderst P, Machan C, Siebert U. The effect of electronic prescribing on medication errors and adverse drug events: a systematic review J Am
Med Inform Assoc 2008. 155585–600. Epub 2008 Jun 25. [PMC free article]
[PubMed}
21 - Vandenberghe HE, Van Casteren V, Jonckheer P, Bastiaens H, Van der Heyden
J, Lafontaine MF, et al. Collecting information on the quality of prescribing in
primary care using semi-automatic data extraction from GPs’ electronic medical
records. Int J Med Inform. 2005;74(5):367–76. [PubMed}
22 - Persell SD, Dunne AP, Lloyd-Jones DM, Baker DW. Electronic health record-
based cardiac risk assessment and identification of unmet preventive needs. Med
Care. 2009;47(4):418–24. [PubMed}
23.personal.umich.edu/~danhorn/reprints/horn_1999_speech_recognition_patterns_c
hi_99.pdf Accessed 2009 Nov 20
24 - Rodríguez-Vera FJ, Marín Y, Sánchez A, Borrachero C, Pujol E. Illegible
67……………………………GOOD MEDICAL PRACTICE …...………………………
67
handwriting in medical records. J R Soc Med. 2002;95(11):545–6. [PMC free article]
[PubMed} Wheeler DA. Why open source software/free software (OSS/FS, FLOSS,
or FOSS)? Look at the numbers!Washington, DC:
2007;com.dwheeler.www: Available from html .why_fs_oss/com.dwheeler.www
27Nov 2009 Accessed
25 - Pearce C, Trumble S, Arnold M, Dwan K, Phillips C. Computers in the new consultation: within the first minute Fam Pract 2008. 253202–8.Epub 2008 May 25.
[PubMed}
26 - Kaner E, Heaven B, Rapley T, Murtagh M, Graham R, Thomson R, et al.
Medical communication and technology: a video-based process study of the use of
decision aids in primary care consultations. BMC Med Inform Decis Mak. 2007;7:2.
[PMC free article] [PubMed
27 - Ventres W, Kooienga S, Vuckovic N, Marlin R, Nygren P, Stewart V.
Physicians, patients, and the electronic health record: an ethnographic analysis. Ann
Fam Med. 2006;4(2):124–31. [PMC free article] [PubMed
28 - Lelievre S, Schultz K. Does computer use in patient-physician encounters influence patient satisfaction? Can Fam Physician. 2010;56:e6–12
Recommended

















