This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
Original Articles
Acute Combined Central and Peripheral
Nervous System Demyelination in ChildrenTanja Adamovic, MD*, Emilie M. Riou, MD†, Genevieve Bernard, MD, MSc†,
Michel Vanasse, MD‡, Jean-Claude Decarie, MD§, Chantal Poulin, MD†,and France Gauvin, MD, MSc*
Reports of acute combined central and peripheral ner-vous system acquired inflammatory demyelination arerare in children. This study aimed to (1) define the clin-ical features and prognoses of patients with this entity;and (2) compare these patients with children presentingisolated acute central or peripheral nervous systemdemyelination. A retrospective chart review of 523children with central or peripheral nervous systemdemyelination hospitalized between 1993-2006 wasundertaken. Among these, 93 fulfilled criteria (clinicalfeatures and positive magnetic resonance imaging orelectromyography/nerve conduction studies) for eitheracute central (n = 37; 39.8%) or peripheral (n = 43;46%) nervous system demyelination, or a combinationof the two (n = 13; 14%). Significant differences betweengroups were evident for age (median, 10 versus 7 versus11 years, respectively; P = 0.047), admission to pediatricintensive care unit (8% versus 30% versus 58%, respec-tively; P = 0.001), length of hospital stay (median, 8 ver-sus 9 versus 29 days, respectively; P < 0.001), treatmentwith steroids (52% versus 7% versus 75%, respec-tively; P < 0.001) and immunoglobulins (11% versus81% versus 75%, respectively; P < 0.001), and poorevolution (3% versus 12% versus 54%, respectively;P = 0.002). This entity in children is not rare, and hasa poorer outcome than isolated central or peripheralnervous system demyelination. Assessment is neededfor a better understanding of risk factors, etiologies,management, and prognosis. � 2008 by Elsevier Inc.All rights reserved.
Adamovic T, Riou EM, Bernard G, Vanasse M, Decarie
J-C, Poulin C, Gauvin F. Acute combined central and pe-
ripheral nervous system demyelination in children. Pediatr
Neurol 2008;39:307-316.
Introduction
Acquired inflammatory demyelinating diseases of the
central nervous system constitute a heterogeneous group
of disorders thought to be of autoimmune origin [1-3], in-
cluding acute disseminated encephalomyelitis, acute hem-
orrhagic leukoencephalitis, Devic’s disease, multiple
sclerosis, transverse myelitis, and clinically isolated syn-
dromes such as optic neuritis.
Acquired inflammatory demyelination of the peripheral
nervous system is also thought to be of autoimmune origin
[3], and can present acutely as the heterogeneous entity
known as Guillain-Barre syndrome or in a more protracted,
sometimes relapsing course, known as chronic inflamma-
tory demyelinating polyradiculoneuropathy.
Combined or sequential inflammatory demyelination of
the central nervous system and peripheral nervous system
in the same patient is thought to result from the same path-
ogenic mechanism [4-6]. Combined acute central nervous
system and peripheral nervous system inflammatory demy-
elination in adults [7-11] and children [7,10-14] was de-
scribed. One study suggests that this association is not
unusual in adults and carries an increased risk of poor neu-
rologic outcome [15]. Aside from case reports, only one ret-
rospective pediatric study discussed this combination,
specifically the combination of myelitis and polyradiculo-
neuritis [11].
The primary objective of our study was to describe the
clinical features and prognoses of a cohort with acute
From the *Paediatric Intensive Care Unit, Department of Paediatrics,Sainte-Justine Hospital, Universite de Montreal, Montreal, Quebec, Can-ada; †Division of Neurology, Department of Pediatrics, Montreal Children’sHospital, McGill University, Montreal, Quebec, Canada; and ‡Division ofNeurology, Department of Pediatrics, and §Department of Radiology,Sainte-Justine Hospital, Universite de Montreal, Montreal, Quebec, Canada.
Communications should be addressed to:Dr. Gauvin; Intensive Care Section (#3406), Sainte-Justine Hospital;3175 Cote Ste.-Catherine; Montreal, Quebec H3T 1C5, Canada.E-mail: [email protected] May 7, 2008; accepted July 30, 2008.
� 2008 by Elsevier Inc. All rights reserved.doi:10.1016/j.pediatrneurol.2008.07.022 � 0887-8994/08/$—see front matter
Adamovic et al: CNS and PNS Demyelination 307
Author's personal copy
combined central nervous system and peripheral nervous
system demyelination in our population of children with
acquired inflammatory demyelinating diseases. Our sec-
ondary objective was to compare these patients with chil-
dren presenting with isolated central nervous system or
peripheral nervous system demyelination.
Methods
This retrospective epidemiologic study was conducted simultaneously
in two pediatric tertiary-care, university-affiliated hospitals (Sainte-Justine
University Hospital and Montreal Children’s Hospital), and covered a 13-
year period.
Recruitment of subjects was based on a systematic search of intrahospi-
tal chart databases for all patients diagnosed with central nervous system or
peripheral nervous system demyelinating syndromes between January
1993 and April 2006. To ensure optimal recruitment, the database was
searched for 18 different diagnostic terms related to demyelinating diseases
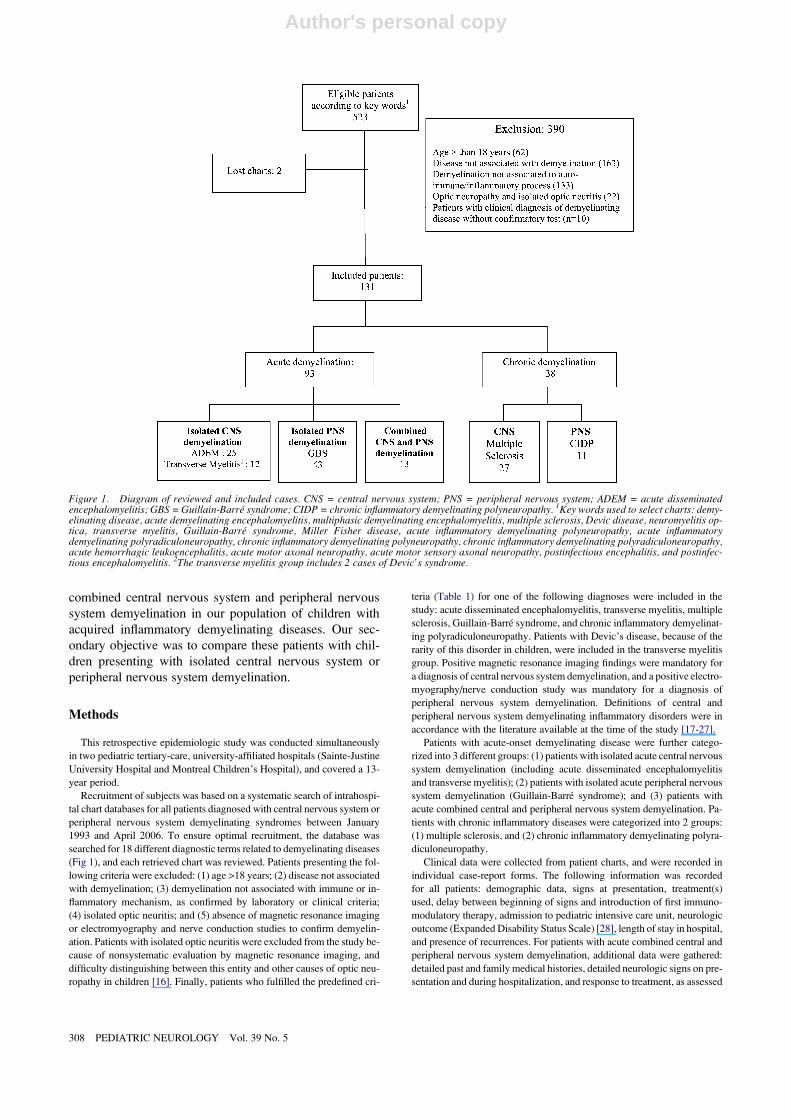
(Fig 1), and each retrieved chart was reviewed. Patients presenting the fol-
lowing criteria were excluded: (1) age >18 years; (2) disease not associated
with demyelination; (3) demyelination not associated with immune or in-
flammatory mechanism, as confirmed by laboratory or clinical criteria;
(4) isolated optic neuritis; and (5) absence of magnetic resonance imaging
or electromyography and nerve conduction studies to confirm demyelin-
ation. Patients with isolated optic neuritis were excluded from the study be-
cause of nonsystematic evaluation by magnetic resonance imaging, and
difficulty distinguishing between this entity and other causes of optic neu-
ropathy in children [16]. Finally, patients who fulfilled the predefined cri-
teria (Table 1) for one of the following diagnoses were included in the
study: acute disseminated encephalomyelitis, transverse myelitis, multiple
sclerosis, Guillain-Barre syndrome, and chronic inflammatory demyelinat-
ing polyradiculoneuropathy. Patients with Devic’s disease, because of the
rarity of this disorder in children, were included in the transverse myelitis
group. Positive magnetic resonance imaging findings were mandatory for
a diagnosis of central nervous system demyelination, and a positive electro-
myography/nerve conduction study was mandatory for a diagnosis of
peripheral nervous system demyelination. Definitions of central and
peripheral nervous system demyelinating inflammatory disorders were in
accordance with the literature available at the time of the study [17-27].
Patients with acute-onset demyelinating disease were further catego-
rized into 3 different groups: (1) patients with isolated acute central nervous
system demyelination (including acute disseminated encephalomyelitis
and transverse myelitis); (2) patients with isolated acute peripheral nervous
system demyelination (Guillain-Barre syndrome); and (3) patients with
acute combined central and peripheral nervous system demyelination. Pa-
tients with chronic inflammatory diseases were categorized into 2 groups:
(1) multiple sclerosis, and (2) chronic inflammatory demyelinating polyra-
diculoneuropathy.
Clinical data were collected from patient charts, and were recorded in
individual case-report forms. The following information was recorded
for all patients: demographic data, signs at presentation, treatment(s)
used, delay between beginning of signs and introduction of first immuno-
modulatory therapy, admission to pediatric intensive care unit, neurologic
outcome (Expanded Disability Status Scale) [28], length of stay in hospital,
and presence of recurrences. For patients with acute combined central and
peripheral nervous system demyelination, additional data were gathered:
detailed past and family medical histories, detailed neurologic signs on pre-
sentation and during hospitalization, and response to treatment, as assessed
Figure 1. Diagram of reviewed and included cases. CNS = central nervous system; PNS = peripheral nervous system; ADEM = acute disseminatedencephalomyelitis; GBS = Guillain-Barre syndrome; CIDP = chronic inflammatory demyelinating polyneuropathy. 1Key words used to select charts: demy-elinating disease, acute demyelinating encephalomyelitis, multiphasic demyelinating encephalomyelitis, multiple sclerosis, Devic disease, neuromyelitis op-tica, transverse myelitis, Guillain-Barre syndrome, Miller Fisher disease, acute inflammatory demyelinating polyneuropathy, acute inflammatorydemyelinating polyradiculoneuropathy, chronic inflammatory demyelinating polyneuropathy, chronic inflammatory demyelinating polyradiculoneuropathy,acute hemorrhagic leukoencephalitis, acute motor axonal neuropathy, acute motor sensory axonal neuropathy, postinfectious encephalitis, and postinfec-tious encephalomyelitis. 2The transverse myelitis group includes 2 cases of Devic’s syndrome.
308 PEDIATRIC NEUROLOGY Vol. 39 No. 5

Author's personal copy
by the neurologist during hospitalization. Neurologic outcome was evalu-
ated at discharge from the hospital and at the last available follow-up neu-
rology visit, using the Expanded Disability Status Scale. A good outcome
was defined as an Expanded Disability Status Scale score from 0-4.5 (no
disability or ambulatory without aid), and poor outcome as an Expanded
Disability Status Scale score from 5-10 (severe disability, restriction to
bed or wheelchair, or death).
Laboratory data were collected, when available, including evidence of
albuminocytologic dissociation (increased protein without an increase in
cell count) or oligoclonal bands in cerebrospinal fluid. For patients with
acute combined central and peripheral nervous system demyelination,
additional laboratory evaluations included acute inflammatory markers,
a hematologic, biochemical, metabolic, and vasculitic workup, and micro-
biology and virologic investigations, when available.
For all patients with a diagnosis of central nervous system demyelin-
ation, the results of brain and spine magnetic resonance imaging were re-
viewed to confirm the presence of acute demyelination. For patients with
acute combined central and peripheral nervous system demyelination,
specific abnormalities on magnetic resonance imaging were detailed by
an experienced pediatric neuroradiologist (J.-C.D.), and recorded on stan-
dardized, individual radiologic case-report forms.
The results of electromyography and nerve conduction studies were ver-
ified by an expert neurologist (M.V.) to confirm the presence of abnormal-
ities in patients with a diagnosis of acute peripheral nervous system
demyelination. For patients with acute combined central and peripheral
nervous system demyelination, detailed abnormalities were recorded.
Nerve conduction velocities were recorded according to standard proce-
dures [27]. Abnormal results were confirmed using established normative
values for the respective age groups [27]. Finally, results of nerve and mus-
cle biopsies were recorded, when available.
Statistical Analysis
Descriptive data were expressed as proportions with percentages for cat-
egorical data, and medians with range for continuous data. Data were com-
pared between patients with acute central nervous system demyelination,
acute peripheral nervous system demyelination, and acute combined cen-
tral and peripheral nervous system demyelination. Comparisons between
groups were performed using the Kruskal-Wallis test for continuous
data, and c2 and Fisher’s exact tests for categorical data. All statistical anal-
yses were performed using SPSS (Statistical Package for the Social Sci-
ences, version 15.0, SPSS, Inc., Chicago, IL). The level of significance
was set at P < 0.05. This research project was approved by the Ethics
Committee of the Sainte-Justine Hospital Research Center and the Chart
Archive Department of Montreal Children’s Hospital.
Table 1. Predefined criteria for confirming diagnosis of acute demyelinating encephalomyelitis, transverse myelitis, Guillain-Barre syndrome,
multiple sclerosis, and chronic inflammatory demyelinating polyneuropathy
Diagnostic Criteria Clinical Criteria MRI Criteria EMG/NCS Criteria
ADEM Acute or subacute onset;
polysymptomatic presentation
including encephalopathy; no history
of neurologic signs suggestive of earlier
demyelinating episode [17,18]
Multifocal, hyperintense
lesions on T2-weighted/
fluid-attenuated inversion recovery
brain-spinal imaging studies [19]
Acute transverse
myelitis
Acute or subacute onset;
sensory and motor deficits
(sometimes autonomic) under site
of medullar lesion; evidence of
inflammation within spinal cord
(MRI or CSF) [20]
High signal intensity lesion
on T2-weighted sequences [20]
with possible rostral-caudal
extent to several spinal
segments [36]; either monofocal
or multifocal [36,37]
Multiple sclerosis Evidence of dissemination in time
and space of demyelinating lesions
according to criteria of McDonald et al.,
and exclusion of all other etiologies
for clinical features [21]
MRI criteria of McDonald et al. [21]
GBS Acute or subacute onset of motor and/or
sensory signs; decreased or absent
reflexes; and/or lumbar puncture revealing
albuminocytologic dissociation [23]
Slowed nerve conduction velocity,
conduction blocks, and/or prolonged
or absent F-waves [27]
CIDP Motor and/or sensory symptoms and
signs in more than one limb;
development over at least 2
months; progressive or
relapsing-remitting course,
with decreased or absent
reflexes; and/or albumino-cytologic
dissociation [24,25]
Slowed conduction velocities, temporal
dispersion, and conduction blocks
[23,24,26]
Abbreviations:
ADEM = Acute disseminated encephalomyelitis
CIDP = Chronic inflammatory demyelinating polyneuropathy
CSF = Cerebrospinal fluid
EMG/NCS = Electromyogram/nerve conduction studies
GBS = Guillain-Barre syndrome
MRI = Magnetic resonance imaging
Adamovic et al: CNS and PNS Demyelination 309

Author's personal copy
Results
Between January 1993 and April 2006, 523 patients were
identified in hospital chart databases as eligible. All charts
were reviewed, except for 2 that were lost. Among eligible
patients, 390 patients were excluded according to prede-
fined criteria (Fig 1). The remaining 131 met the inclusion
criteria and were retained for analysis. Thirty-eight patients
presented chronic demyelination (27 with multiple sclero-
sis, and 11 with chronic inflammatory demyelinating poly-
radiculoneuropathy), and 93 patients presented acute
demyelination. Among the latter, 37 presented acute central
nervous system demyelination (25 with acute disseminated
encephalomyelitis, and 12 with transverse myelitis), and 43
presented acute peripheral nervous system demyelination
(Guillain-Barre syndrome). Thirteen patients met the crite-
ria for acute combined central and peripheral nervous
system demyelination.
Patients With Acute Demyelination (Central orPeripheral Nervous System)
Patients with acute demyelination had a median age at
presentation of 7.9 years (range, 1-18 years), and were
mostly boys (61%). When comparing patients with acute
central nervous system demyelination, acute peripheral ner-
vous system demyelination, and acute combined central
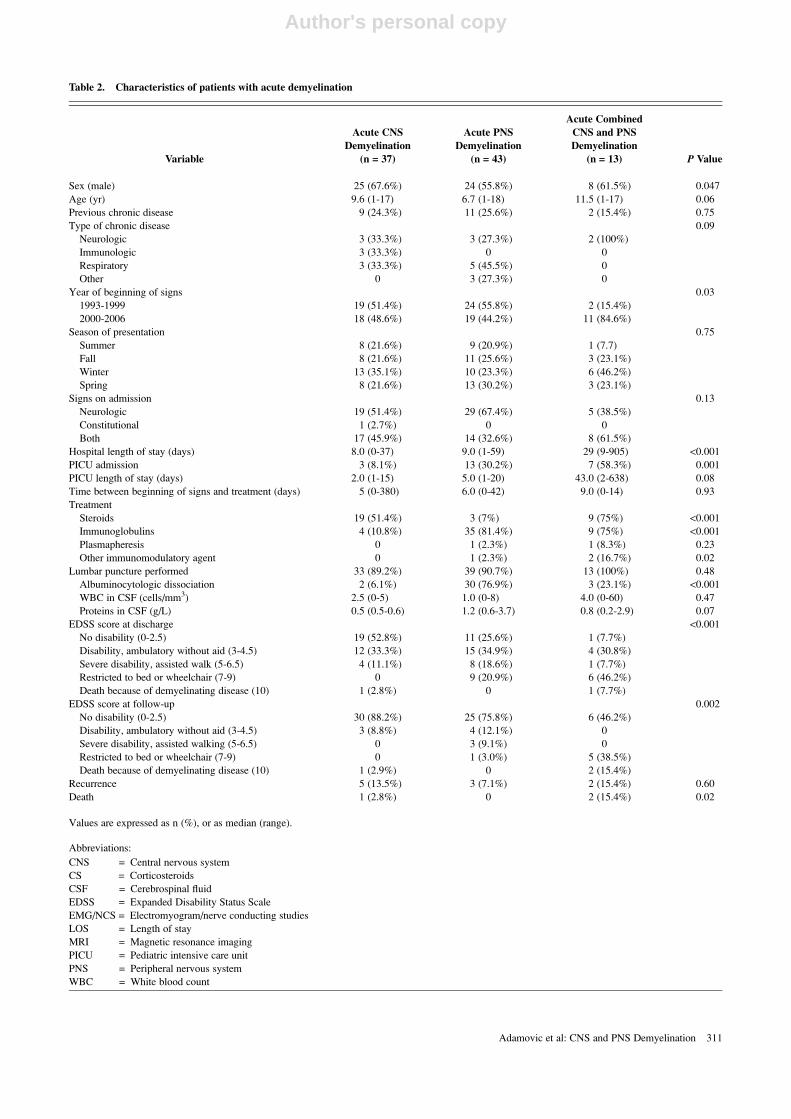
and peripheral nervous system demyelination (Table 2),
there were significant differences between the 3 groups
for age, occurrence of disease between 2000-2006, admis-
sion to pediatric intensive care unit, length of hospital
stay, presence of albuminocytologic dissociation in cere-
brospinal fluid, use of steroids, use of immunoglobulins,
and poor neurologic outcome at discharge and at last fol-
low-up. No significant differences were evident for sex,
presence and type of previous chronic disease, season of oc-
currence, presence of neurologic or constitutional signs on
admission, number of recurrences, and delay between initial
signs and therapy.
Patients With Acute Combined Central and PeripheralNervous System Demyelination
Patients with acute combined central and peripheral ner-
vous system demyelination are detailed in Table 3. Most
presented during the winter (46%), and were diagnosed be-
tween 2000 and 2006 (85%). The disease occurred within 3
weeks of an infectious prodrome in 11 patients (85%). Pro-
dromes consisted of isolated fever (27%), flu-like illness
(27%), malaise/fatigue (18%), gastroenteritis (18%), or up-
per respiratory-tract infection (9%). The family history was
negative for demyelinating diseases in all patients. Most pa-
tients exhibited both neurologic and constitutional signs on
presentation (62%). Median time to maximal neurologic
deficit was of 6.8 days from the onset of neurologic signs.
The most common presenting complaints consisted of
weakness (85%), walking difficulties (85%), sensory distur-
bances (46%), and decreased level of consciousness (23%).
Most patients (9/13; 69%) first presented signs of central
nervous system demyelination, whereas a few patients (4/
13; 31%) first presented signs of peripheral nervous system
demyelination. The time interval until both central and pe-
ripheral nervous system demyelinations were coexpressed
varied from 1-16 days. Only 3 patients manifested seizures
during hospitalization (Table 3). One patient presented at
admission with generalized tonic-clonic status (patient 2),
another had partial motor seizures in the early phase of
the disease (patient 4), and for a third patient, seizures
were the presenting signs of a first relapse of acute dissem-
inated encephalomyelitis (patient 3).
Results of laboratory examinations were normal, except
for an elevated sedimentation rate in 8 of 10 patients in
whom this test was performed (median, 24 mm/hour; range,
14-62 mm/hour). A cerebrospinal fluid examination was
performed in 89% of patient with central nervous system
demyelination, in 91% of patients with peripheral nervous
system demyelination, and in 100% of patients with com-
bined central and peripheral nervous system demyelination
(Table 2). Cerebrospinal fluid examination indicated a me-
dian cerebrospinal fluid leukocyte concentration of 4 cells/
mm3 (range, 0-60 cells/mm3), with lymphocytic or mono-
cytic predominance (55%) and a median protein level of 0.8
g/L (range, 0.2-2.9 g/L). Albuminocytologic dissociation
was detected in 3 patients (23%). Oligoclonal bands in ce-
rebrospinal fluid were tested in only 4 of 13 patients, and in
all of them were negative. Microbiology revealed serologic
evidence of recent infection in 6 patients (Table 3).
Magnetic resonance imaging indicated isolated brain de-
myelination in 6 (46%) patients, isolated spinal cord demy-
elination in 4 (31%) patients, and combined brain and
spinal-cord demyelination in 3 (23%) patients. Magnetic
resonance imaging of the brain demonstrated an average
of 12 lesions per patient, and was characterized by multifo-
cal areas of high signal intensity mainly in the supratentorial
white matter, along with frequent involvement of the deep
gray matter (Table 4). Most of the lesions were large, asym-
metrical, and confluent, with mild mass effect and occa-
sional contrast enhancement. Similarly, spinal magnetic
resonance imaging revealed large and confluent lesions.
In 2 patients, results of the first magnetic resonance imaging
were normal, and demyelination was evident only on subse-
quent magnetic resonance imaging, performed 16 and 22
days after the initial presentation.
The results of electromyography and nerve conduction
studies are detailed in Table 4. These revealed a predomi-
nantly axonal pattern in 6 patients, and a predominantly de-
myelinating pattern in 5. In the 2 other patients, it was
impossible to conclude whether the involvement was pri-
marily axonal or demyelinating.
Only 1 patient underwent sural-nerve and muscle biop-
sies, which indicated mild axonal neuropathic abnormalities
and myopathic changes. These invasive procedures were
rarely performed, an indication that they are not routinely
used in the diagnosis of demyelinating diseases.
310 PEDIATRIC NEUROLOGY Vol. 39 No. 5
Author's personal copy
Table 2. Characteristics of patients with acute demyelination
Variable
Acute CNS
Demyelination
(n = 37)
Acute PNS
Demyelination
(n = 43)
Acute Combined
CNS and PNS
Demyelination
(n = 13) P Value
Sex (male) 25 (67.6%) 24 (55.8%) 8 (61.5%) 0.047
Age (yr) 9.6 (1-17) 6.7 (1-18) 11.5 (1-17) 0.06
Previous chronic disease 9 (24.3%) 11 (25.6%) 2 (15.4%) 0.75
Type of chronic disease 0.09
Neurologic 3 (33.3%) 3 (27.3%) 2 (100%)
Immunologic 3 (33.3%) 0 0
Respiratory 3 (33.3%) 5 (45.5%) 0
Other 0 3 (27.3%) 0
Year of beginning of signs 0.03
1993-1999 19 (51.4%) 24 (55.8%) 2 (15.4%)
2000-2006 18 (48.6%) 19 (44.2%) 11 (84.6%)
Season of presentation 0.75
Summer 8 (21.6%) 9 (20.9%) 1 (7.7)
Fall 8 (21.6%) 11 (25.6%) 3 (23.1%)
Winter 13 (35.1%) 10 (23.3%) 6 (46.2%)
Spring 8 (21.6%) 13 (30.2%) 3 (23.1%)
Signs on admission 0.13
Neurologic 19 (51.4%) 29 (67.4%) 5 (38.5%)
Constitutional 1 (2.7%) 0 0
Both 17 (45.9%) 14 (32.6%) 8 (61.5%)
Hospital length of stay (days) 8.0 (0-37) 9.0 (1-59) 29 (9-905) <0.001
PICU admission 3 (8.1%) 13 (30.2%) 7 (58.3%) 0.001
PICU length of stay (days) 2.0 (1-15) 5.0 (1-20) 43.0 (2-638) 0.08
Time between beginning of signs and treatment (days) 5 (0-380) 6.0 (0-42) 9.0 (0-14) 0.93
Treatment
Steroids 19 (51.4%) 3 (7%) 9 (75%) <0.001
Immunoglobulins 4 (10.8%) 35 (81.4%) 9 (75%) <0.001
Plasmapheresis 0 1 (2.3%) 1 (8.3%) 0.23
Other immunomodulatory agent 0 1 (2.3%) 2 (16.7%) 0.02
Lumbar puncture performed 33 (89.2%) 39 (90.7%) 13 (100%) 0.48
Albuminocytologic dissociation 2 (6.1%) 30 (76.9%) 3 (23.1%) <0.001
WBC in CSF (cells/mm3) 2.5 (0-5) 1.0 (0-8) 4.0 (0-60) 0.47
Proteins in CSF (g/L) 0.5 (0.5-0.6) 1.2 (0.6-3.7) 0.8 (0.2-2.9) 0.07
EDSS score at discharge <0.001
No disability (0-2.5) 19 (52.8%) 11 (25.6%) 1 (7.7%)
Disability, ambulatory without aid (3-4.5) 12 (33.3%) 15 (34.9%) 4 (30.8%)
Severe disability, assisted walk (5-6.5) 4 (11.1%) 8 (18.6%) 1 (7.7%)
Restricted to bed or wheelchair (7-9) 0 9 (20.9%) 6 (46.2%)
Death because of demyelinating disease (10) 1 (2.8%) 0 1 (7.7%)
EDSS score at follow-up 0.002
No disability (0-2.5) 30 (88.2%) 25 (75.8%) 6 (46.2%)
Disability, ambulatory without aid (3-4.5) 3 (8.8%) 4 (12.1%) 0
Severe disability, assisted walking (5-6.5) 0 3 (9.1%) 0
Restricted to bed or wheelchair (7-9) 0 1 (3.0%) 5 (38.5%)
Death because of demyelinating disease (10) 1 (2.9%) 0 2 (15.4%)
Recurrence 5 (13.5%) 3 (7.1%) 2 (15.4%) 0.60
Death 1 (2.8%) 0 2 (15.4%) 0.02
Values are expressed as n (%), or as median (range).
Abbreviations:
CNS = Central nervous system
CS = Corticosteroids
CSF = Cerebrospinal fluid
EDSS = Expanded Disability Status Scale
EMG/NCS = Electromyogram/nerve conducting studies
LOS = Length of stay
MRI = Magnetic resonance imaging
PICU = Pediatric intensive care unit
PNS = Peripheral nervous system
WBC = White blood count
Adamovic et al: CNS and PNS Demyelination 311
Author's personal copy
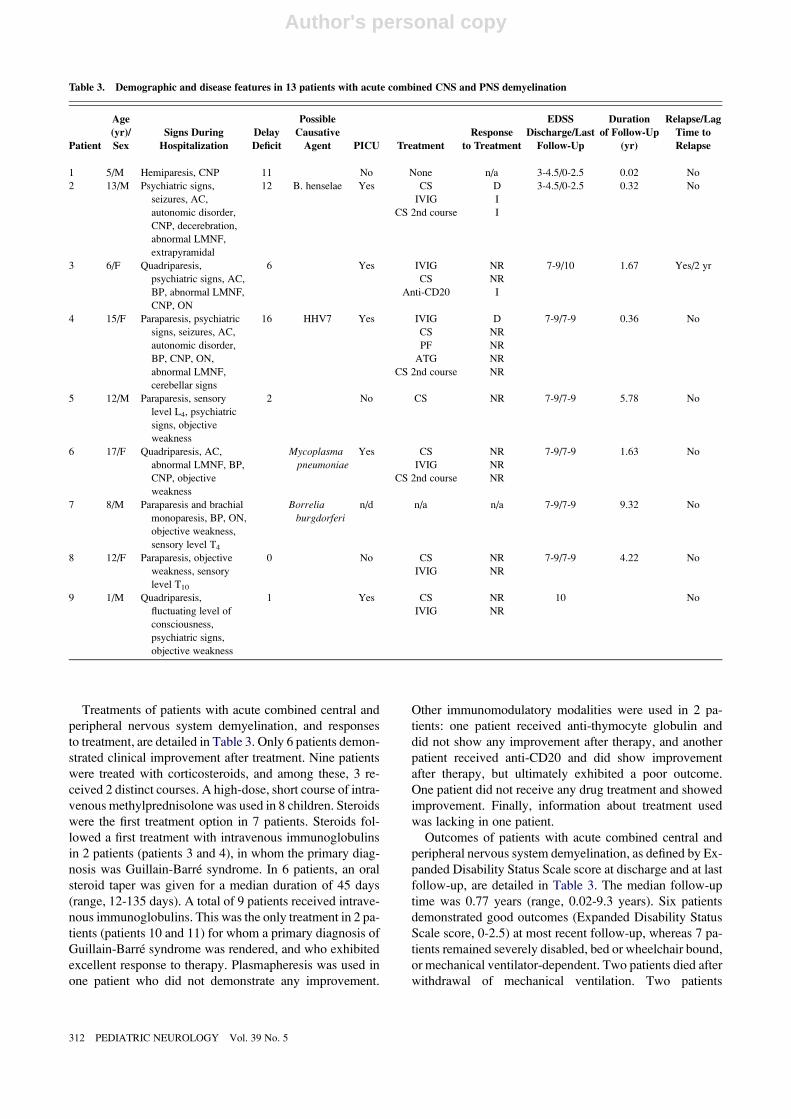
Treatments of patients with acute combined central and
peripheral nervous system demyelination, and responses
to treatment, are detailed in Table 3. Only 6 patients demon-
strated clinical improvement after treatment. Nine patients
were treated with corticosteroids, and among these, 3 re-
ceived 2 distinct courses. A high-dose, short course of intra-
venous methylprednisolone was used in 8 children. Steroids
were the first treatment option in 7 patients. Steroids fol-
lowed a first treatment with intravenous immunoglobulins
in 2 patients (patients 3 and 4), in whom the primary diag-
nosis was Guillain-Barre syndrome. In 6 patients, an oral
steroid taper was given for a median duration of 45 days
(range, 12-135 days). A total of 9 patients received intrave-
nous immunoglobulins. This was the only treatment in 2 pa-
tients (patients 10 and 11) for whom a primary diagnosis of
Guillain-Barre syndrome was rendered, and who exhibited
excellent response to therapy. Plasmapheresis was used in
one patient who did not demonstrate any improvement.
Other immunomodulatory modalities were used in 2 pa-
tients: one patient received anti-thymocyte globulin and
did not show any improvement after therapy, and another
patient received anti-CD20 and did show improvement
after therapy, but ultimately exhibited a poor outcome.
One patient did not receive any drug treatment and showed
improvement. Finally, information about treatment used
was lacking in one patient.
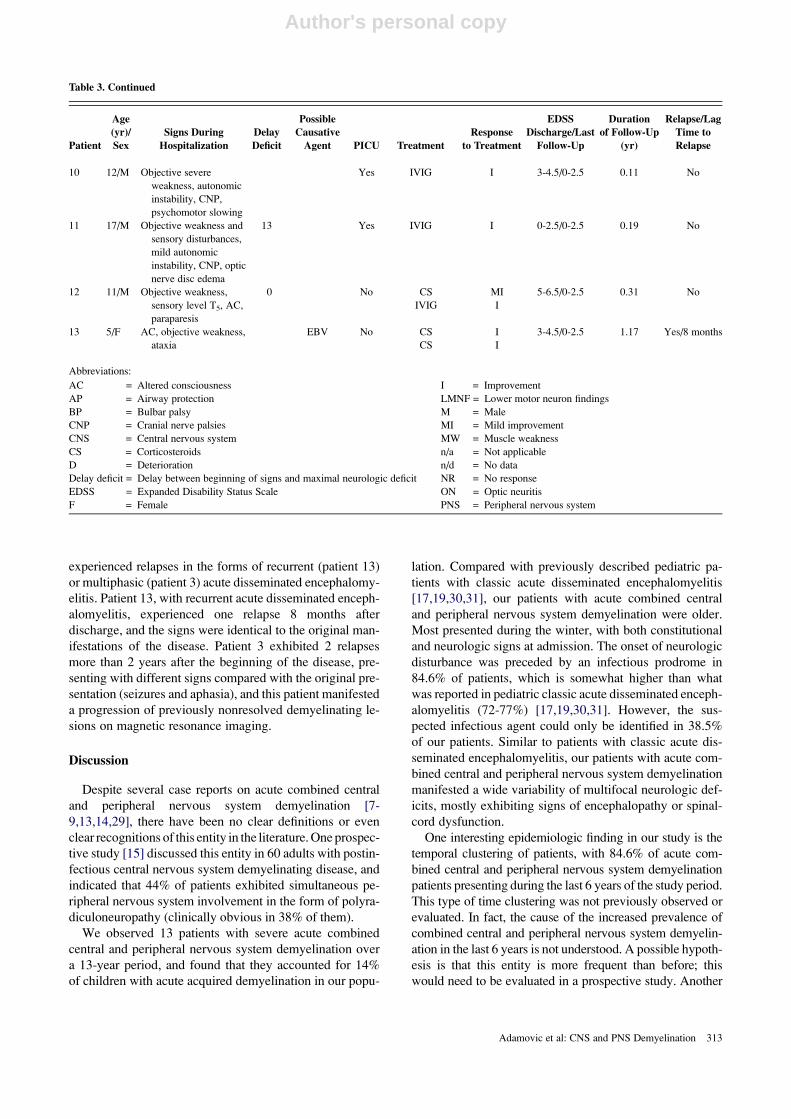
Outcomes of patients with acute combined central and
peripheral nervous system demyelination, as defined by Ex-
panded Disability Status Scale score at discharge and at last
follow-up, are detailed in Table 3. The median follow-up
time was 0.77 years (range, 0.02-9.3 years). Six patients
demonstrated good outcomes (Expanded Disability Status
Scale score, 0-2.5) at most recent follow-up, whereas 7 pa-
tients remained severely disabled, bed or wheelchair bound,
or mechanical ventilator-dependent. Two patients died after
withdrawal of mechanical ventilation. Two patients
Table 3. Demographic and disease features in 13 patients with acute combined CNS and PNS demyelination
Patient
Age
(yr)/
Sex
Signs During
Hospitalization
Delay
Deficit
Possible
Causative
Agent PICU Treatment
Response
to Treatment
EDSS
Discharge/Last
Follow-Up
Duration
of Follow-Up
(yr)
Relapse/Lag
Time to
Relapse
1 5/M Hemiparesis, CNP 11 No None n/a 3-4.5/0-2.5 0.02 No
2 13/M Psychiatric signs,
seizures, AC,
autonomic disorder,
CNP, decerebration,
abnormal LMNF,
extrapyramidal
12 B. henselae Yes CS
IVIG
CS 2nd course
D
I
I
3-4.5/0-2.5 0.32 No
3 6/F Quadriparesis,
psychiatric signs, AC,
BP, abnormal LMNF,
CNP, ON
6 Yes IVIG
CS
Anti-CD20
NR
NR
I
7-9/10 1.67 Yes/2 yr
4 15/F Paraparesis, psychiatric
signs, seizures, AC,
autonomic disorder,
BP, CNP, ON,
abnormal LMNF,
cerebellar signs
16 HHV7 Yes IVIG
CS
PF
ATG
CS 2nd course
D
NR
NR
NR
NR
7-9/7-9 0.36 No
5 12/M Paraparesis, sensory
level L4, psychiatric
signs, objective
weakness
2 No CS NR 7-9/7-9 5.78 No
6 17/F Quadriparesis, AC,
abnormal LMNF, BP,
CNP, objective
weakness
Mycoplasma
pneumoniae
Yes CS
IVIG
CS 2nd course
NR
NR
NR
7-9/7-9 1.63 No
7 8/M Paraparesis and brachial
monoparesis, BP, ON,
objective weakness,
sensory level T4
Borrelia
burgdorferi
n/d n/a n/a 7-9/7-9 9.32 No
8 12/F Paraparesis, objective
weakness, sensory
level T10
0 No CS
IVIG
NR
NR
7-9/7-9 4.22 No
9 1/M Quadriparesis,
fluctuating level of
consciousness,
psychiatric signs,
objective weakness
1 Yes CS
IVIG
NR
NR
10 No
312 PEDIATRIC NEUROLOGY Vol. 39 No. 5
Author's personal copy
experienced relapses in the forms of recurrent (patient 13)
or multiphasic (patient 3) acute disseminated encephalomy-
elitis. Patient 13, with recurrent acute disseminated enceph-
alomyelitis, experienced one relapse 8 months after
discharge, and the signs were identical to the original man-
ifestations of the disease. Patient 3 exhibited 2 relapses
more than 2 years after the beginning of the disease, pre-
senting with different signs compared with the original pre-
sentation (seizures and aphasia), and this patient manifested
a progression of previously nonresolved demyelinating le-
sions on magnetic resonance imaging.
Discussion
Despite several case reports on acute combined central
and peripheral nervous system demyelination [7-
9,13,14,29], there have been no clear definitions or even
clear recognitions of this entity in the literature. One prospec-
tive study [15] discussed this entity in 60 adults with postin-
fectious central nervous system demyelinating disease, and
indicated that 44% of patients exhibited simultaneous pe-
ripheral nervous system involvement in the form of polyra-
diculoneuropathy (clinically obvious in 38% of them).
We observed 13 patients with severe acute combined
central and peripheral nervous system demyelination over
a 13-year period, and found that they accounted for 14%
of children with acute acquired demyelination in our popu-
lation. Compared with previously described pediatric pa-
tients with classic acute disseminated encephalomyelitis
[17,19,30,31], our patients with acute combined central
and peripheral nervous system demyelination were older.
Most presented during the winter, with both constitutional
and neurologic signs at admission. The onset of neurologic
disturbance was preceded by an infectious prodrome in
84.6% of patients, which is somewhat higher than what
was reported in pediatric classic acute disseminated enceph-
alomyelitis (72-77%) [17,19,30,31]. However, the sus-
pected infectious agent could only be identified in 38.5%
of our patients. Similar to patients with classic acute dis-
seminated encephalomyelitis, our patients with acute com-
bined central and peripheral nervous system demyelination
manifested a wide variability of multifocal neurologic def-
icits, mostly exhibiting signs of encephalopathy or spinal-
cord dysfunction.
One interesting epidemiologic finding in our study is the
temporal clustering of patients, with 84.6% of acute com-
bined central and peripheral nervous system demyelination
patients presenting during the last 6 years of the study period.
This type of time clustering was not previously observed or
evaluated. In fact, the cause of the increased prevalence of
combined central and peripheral nervous system demyelin-
ation in the last 6 years is not understood. A possible hypoth-
esis is that this entity is more frequent than before; this
would need to be evaluated in a prospective study. Another
Table 3. Continued
Patient
Age
(yr)/
Sex
Signs During
Hospitalization
Delay
Deficit
Possible
Causative
Agent PICU Treatment
Response
to Treatment
EDSS
Discharge/Last
Follow-Up
Duration
of Follow-Up
(yr)
Relapse/Lag
Time to
Relapse
10 12/M Objective severe
weakness, autonomic
instability, CNP,
psychomotor slowing
Yes IVIG I 3-4.5/0-2.5 0.11 No
11 17/M Objective weakness and
sensory disturbances,
mild autonomic
instability, CNP, optic
nerve disc edema
13 Yes IVIG I 0-2.5/0-2.5 0.19 No
12 11/M Objective weakness,
sensory level T5, AC,
paraparesis
0 No CS
IVIG
MI
I
5-6.5/0-2.5 0.31 No
13 5/F AC, objective weakness,
ataxia
EBV No CS
CS
I
I
3-4.5/0-2.5 1.17 Yes/8 months
Abbreviations:
AC = Altered consciousness
AP = Airway protection
BP = Bulbar palsy
CNP = Cranial nerve palsies
CNS = Central nervous system
CS = Corticosteroids
D = Deterioration
Delay deficit = Delay between beginning of signs and maximal neurologic deficit
EDSS = Expanded Disability Status Scale
F = Female
I = Improvement
LMNF = Lower motor neuron findings
M = Male
MI = Mild improvement
MW = Muscle weakness
n/a = Not applicable
n/d = No data
NR = No response
ON = Optic neuritis
PNS = Peripheral nervous system
Adamovic et al: CNS and PNS Demyelination 313

Author's personal copy
plausible hypothesis involves increased detection of the en-
tity because of enhanced awareness and increased systematic
neuroimaging and electromyography/nerve conduction stud-
ies in patients with demyelinating diseases. In our study,
although magnetic resonance imaging was performed in all
patients with acute central nervous system demyelination
and with acute combined central and peripheral nervous sys-
tem demyelination, this test was performed in only 9 patients
(20.9%) with isolated peripheral nervous system demyelin-
ation. Similarly, electromyography/nerve conduction studies
were performed in all patients with acute peripheral nervous
system demyelination and with acute combined central and
peripheral nervous system demyelination, but in only 2 pa-
tients with isolated acute central nervous system demyelin-
ation (5%). Further studies using systematic magnetic
resonance imaging and electromyography/nerve conduction
studies in all patients with demyelinating diseases will be
necessary to verify this hypothesis.
Another notable finding of our study is the poor neuro-
logic evolution and final outcome of 7 (54%) patients
with acute combined central and peripheral nervous system
demyelination. Classic acute disseminated encephalomyeli-
tis is typically a disease characterized by a good evolution
and excellent neurologic outcome [17,19,30,31], although
cases with residual neurologic and cognitive deficit [32]
and even death [33,34] are rarely observed. The same ap-
plies to Guillain-Barre syndrome in the pediatric population
[35]. A pediatric study on transverse myelitis demonstrated
an overall poor outcome, with 40% of children permanently
wheelchair-dependent as a result of the disease [36]. On the
contrary, in our study, we observed excellent functional
outcomes in patients with isolated transverse myelitis,
whereas 7 of 13 patients with acute combined central and
peripheral nervous system demyelination displayed signif-
icantly poorer outcomes. Functional impairment at clinical
onset was not correlated with response to therapy and final
outcome in our cohort. The reason for the worse neurologic
outcome is unclear. Further prospective studies are neces-
sary to identify causes and risk factors of poor neurologic
outcomes in these patients.
The primary therapy in our cohort of patients was chosen
according to the first-appearing or more severe symptom-
atology. Corticosteroids were used for central nervous sys-
tem demyelination, and intravenous immunoglobulins were
used for peripheral nervous system demyelination. In case
of treatment failure or progression of the disease, the alter-
nate therapy was tried. Both therapies failed to produce sig-
nificant benefits in 39% of patients. Two patients were
additionally treated with other immunomodulatory treat-
ments, including plasmapheresis, anti-CD20, and anti-thy-
mocyte globulin, with no significant effect on outcome.
This result suggests that optimal therapeutic options for
acute combined central and peripheral nervous system de-
myelination are still uncertain, and the question of which
treatment to use first remains unanswered. A study of this
entity in adults [15] suggests that intravenous immunoglob-
ulins should be the first-line therapy in patients with both
central and peripheral nervous system involvement, be-
cause it produced better results than steroids.
This study systematically describes epidemiologic and
clinical characteristics of children with severe acute com-
bined central and peripheral nervous system inflammatory
demyelination in 2 pediatric tertiary-care hospitals. We
used broad criteria for eligibility, to include as many poten-
tial subjects as possible. Although consensus definitions for
pediatric multiple sclerosis and related disorders, as re-
cently proposed by the International Pediatric Multiple
Sclerosis Study Group [37], were not available at the time
of the study, the criteria used here were concordant with
Table 4. Detailed abnormal results of confirmatory tests in 13
patients with acute combined CNS and PNS demyelination, with
demyelination according to brain and spinal magnetic resonance
imaging, as well as anomalies evident on nerve conduction studies
and electromyography
Results of MRI* Patients, n (%)
Cerebral demyelination 9 (69%)
Supratentorial lesions 9 (69%)
Subcortical white matter 8 (62%)
Paraventricular white matter 4 (31%)
Supratentorial cortex 3 (23%)
Basal ganglia 3 (23%)
Thalami 2 (15%)
Infratentorial demyelinating lesions 5 (39%)
Brainstem 4 (31%)
Cerebellum 2 (15%)
Spinal cord demyelination 7 (54%)
Cervical spine 1 (14%)
Cervico-thoracic 4 (57%)
Thoraco-lumbar 2 (29%)
Enhancement of ventral and dorsal roots,
and/or cauda equina
3 (23%)
Results of NCS/EMG†
Abnormal motor NCS 13 (100%)
Prolonged distal latencies 4 (31%)
Decreased conduction velocities 2 (15%)
Conduction blocks 1 (8%)
Decreased amplitudes (or absence of response) 8 (62%)
Absence or prolonged F-waves 3 (23%)
Abnormal sensory NCS 6 (60%)
Decreased conduction velocities 3 (30%)
Absence of response 3 (30%)
Abnormal EMG 9 (90%)
Active denervation 8 (80%)
Chronic denervation 4 (40%)
*Cerebral MRI was performed in 12 patients; spinal MRI was
performed in 13 patients.
†Motor nerve conduction was performed in 13 patients, sensory nerve
conduction was performed in 10 patients, and electromyography was
performed in 10 patients.
Abbreviations:
CNS = Central nervous system
EMG = Electromyography
MRI = Magnetic resonance imaging
NCS = Nerve conduction studies
PNS = Peripheral nervous system
314 PEDIATRIC NEUROLOGY Vol. 39 No. 5

Author's personal copy
those recent definitions. Classification of patients was per-
formed in a rigorous manner. All diagnoses were supported
by at least one objective examination, in the form of mag-
netic resonance imaging and/or electromyography/nerve
conduction studies. Finally, this study covered a 13-year
period, which allowed the findings to be representative
and accounted for possible seasonal and annual variations.
However, this study has the limitations inherent in any
retrospective study. Specific risk factors for acute combined
central and peripheral nervous system demyelination could
not be established, because of the small sample size of pa-
tients with this rare entity. A larger prospective study, in-
volving several pediatric centers, is needed to identify
those risk factors. The prevalence of acute combined central
and peripheral nervous system demyelination was probably
underestimated, because most of the patients with acute iso-
lated central nervous system and acute isolated peripheral
nervous system demyelination were not systematically
evaluated for possible associated involvement (magnetic
resonance imaging and/or electromyography/nerve conduc-
tion studies). Some patients with mild involvement were
possibly overlooked because these investigations were not
undertaken. Hence, a potential to bias the apparent out-
comes of patients with acute combined central and periph-
eral nervous system demyelination is possible. In other
words, a selection bias based on the necessity for confirma-
tory tests (magnetic resonance imaging and electromyogra-
phy/nerve conduction studies) in this cohort of patients
could explain the severity of disease seen in this cohort
and the associated poor neurologic outcomes. This could
partly explain the worse prognosis of this subgroup, and
the relatively small number of patients found, compared
with previously reported adult series [15].
Furthermore, it is possible that in some patients, investi-
gations were obtained too early in the evolution of the dis-
ease, and thus failed to demonstrate demyelination. A lag of
a few weeks between the beginning of neurologic signs and
magnetic resonance imaging confirmation of demyelination
was reported previously in acute disseminated encephalo-
myelitis [38].
In conclusion, acute combined central and peripheral ner-
vous system demyelination is not as rare as previously
thought in the pediatric population. Although isolated cen-
tral nervous system or peripheral nervous system demyelin-
ation usually portends a good prognosis, the combination of
these two diseases may have, in some patients, a poorer
prognosis. Systematic assessment of this entity, using mag-
netic resonance imaging and electromyography/nerve con-
duction studies, is important. Further studies are necessary
to clarify its incidence, risk factors, potential etiologies,
optimal management, and prognosis.
References
[1] Gold R. Animal models for autoimmune demyelinating disorders
of the nervous system. Mol Med Today 2000;62:88-91.
[2] Hartung HP, Grossman RI. ADEM: Distinct disease or part of the
MS spectrum? Neurology 2001;56:1257-60.
[3] Menkes J. Autoimmune and postinfectious disease. In: Pine JW,
editor. Textbook of child neurology. Baltimore: Williams & Wilkins,
1995:510-56.
[4] Abramsky O, Teitelbaum D, Webb C, Arnon R. Neuritogenic and
encephalitogenic properties of the peripheral nerve basic proteins. J Neuro-
pathol Exp Neurol 1975;34:36-45.
[5] Poser CM. The peripheral nervous system in multiple sclerosis. A
review and pathogenetic hypothesis. J Neurol Sci 1987;79:83-90.
[6] Hamaguchi K. Guillain-Barre syndrome and acute disseminated
encephalomyelitis (ADEM) [in Japanese]. Rinsho Shinkeigaku 1996;36:
1301-7.
[7] Aimoto Y, Moriwaka F, Matsumoto A, Tashiro K, Abe K. A case of
acute disseminated encephalomyelitis (ADEM) associated with demyelin-
ating peripheral neuropathy [in Japanese]. No To Shinkei 1996;48:857-60.
[8] Katchanov J, Lunemann JD, Masuhr F, et al. Acute combined
central and peripheral inflammatory demyelination. J Neurol Neurosurg
Psychiatry 2004;75:1784-6.
[9] Nadkarni N, Lisak RP. Guillain-Barre syndrome (GBS) with bi-
lateral optic neuritis and central white matter disease. Neurology 1993;
43:842-3.
[10] Lee WT, Wang PJ, Liu HM, et al. Acute disseminated enceph-
alomyelitis in children: Clinical, neuroimaging and neurophysiologic
studies. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi 1996;37:
197-203.
[11] Martens-Le Bouar H, Korinthenberg R. Polyradiculoneuritis
with myelitis: A rare differential diagnosis of Guillain-Barre syndrome.
Neuropediatrics 2002;33:93-6.
[12] Amit R, Shapira Y, Blank A, Aker M. Acute, severe, central and
peripheral nervous system combined demyelination. Pediatr Neurol 1986;
2:47-50.
[13] Blennow G, Gamstrop I, Rosenberg R. Encephalo-myelo-radi-
culo-neuropathy. Dev Med Child Neurol 1968;10:485-90.
[14] Mariotti P, Batocchi AP, Colosimo C, et al. Multiphasic demy-
elinating disease involving central and peripheral nervous system in a child.
Neurology 2003;60:348-9.
[15] Marchioni E, Ravaglia S, Piccolo G, et al. Postinfectious inflam-
matory disorders: Subgroups based on prospective follow-up. Neurology
2005;65:1057-65.
[16] Boomer JA, Siatkowski RM. Optic neuritis in adults and chil-
dren. Semin Ophthalmol 2003;18:174-80.
[17] Tenembaum S, Chamoles N, Fejerman N. Acute disseminated
encephalomyelitis: A long-term follow-up study of 84 pediatric patients.
Neurology 2002;59:1224-31.
[18] Schwarz S, Mohr A, Knauth M, Wildemann B, Storch-
Hagenlocher B. Acute disseminated encephalomyelitis: A follow-up study
of 40 adult patients. Neurology 2001;56:1313-8.
[19] Murthy SN, Faden HS, Cohen ME, Bakshi R. Acute dissemi-
nated encephalomyelitis in children. Pediatrics 2002;110:e21.
[20] Transverse Myelitis Consortium Working Group. Proposed
diagnostic criteria and nosology of acute transverse myelitis. Neurology
2002;59:499-505.
[21] McDonald WI, Compston A, Edan G, et al. Recommended diag-
nostic criteria for multiple sclerosis: Guidelines from the International
Panel on the Diagnosis of Multiple Sclerosis. Ann Neurol 2001;50:121-7.
[22] Barkhof F, Filippi M, Miller DH, et al. Comparison of MRI cri-
teria at first presentation to predict conversion to clinically definite multiple
sclerosis. Brain 1997;120:2059-69.
[23] van der Meche FG, Vermeulen M, Busch HF. Chronic inflam-
matory demyelinating polyneuropathy. Conduction failure before and dur-
ing immunoglobulin or plasma therapy. Brain 1989;112:1563-71.
[24] Barohn RJ, Kissel JT, Warmolts JR, Mendell JR. Chronic in-
flammatory demyelinating polyradiculoneuropathy. Clinical characteris-
tics, course, and recommendations for diagnostic criteria. Arch Neurol
1989;46:878-84.
[25] Feasby TE. Inflammatory-demyelinating polyneuropathies.
Neurol Clin 1992;10:651-70.
[26] van Doorn PA, Vermeulen M, Brand A, Mulder PG, Busch HF.
Intravenous immunoglobulin treatment in patients with chronic
Adamovic et al: CNS and PNS Demyelination 315

Author's personal copy
inflammatory demyelinating polyneuropathy. Clinical and laboratory
characteristics associated with improvement. Arch Neurol 1991;48:
217-20.
[27] Jones RHJ, Harmon RH, Harper CM, Bolton CF. An approach to
pediatric electromyography. In: Royden H, Jones CFB, Harper CM, edi-
tors. Pediatric clinical electromyography. Philadelphia: Lippincott-Raven
Publishers, 1996:1-36.
[28] Kurtzke JF. Rating neurologic impairment in multiple sclero-
sis: An expanded disability status scale (EDSS). Neurology 1983;33:
1444-52.
[29] Amit R, Glick B, Itzchak Y, Dgani Y, Meyeir S. Acute severe
combined demyelination. Childs Nerv Syst 1992;8:354-6.
[30] Dale RC, de Sousa C, Chong WK, Cox TC, Harding B,
Neville BG. Acute disseminated encephalomyelitis, multiphasic dissemi-
nated encephalomyelitis and multiple sclerosis in children. Brain 2000;
123:2407-22.
[31] Hynson JL, Kornberg AJ, Coleman LT, Shield L, Harvey AS,
Kean MJ. Clinical and neuroradiologic features of acute disseminated
encephalomyelitis in children. Neurology 2001;56:1308-12.
[32] Hahn CD, Miles BS, MacGregor DL, Blaser SI, Banwell BL,
Hetherington CR. Neurocognitive outcome after acute disseminated
encephalomyelitis. Pediatr Neurol 2003;29:117-23.
[33] Epperson LW, Whitaker JN, Kapila A. Cranial MRI in acute dis-
seminated encephalomyelitis. Neurology 1988;38:332-3.
[34] Johnson RT, Griffin DE, Hirsch RL, et al. Measles encephalomy-
elitis—Clinical and immunologic studies. N Engl J Med 1984;310:137-41.
[35] Ryan MM. Guillain-Barre syndrome in childhood. J Paediatr
Child Health 2005;41:237-41.
[36] Pidcock FS, Krishnan C, Crawford TO, Salorio CF, Trovato M,
Kerr DA. Acute transverse myelitis in childhood: Center-based analysis of
47 cases. Neurology 2007;68:1474-80.
[37] Krupp LB, Banwell B, Tenembaum S. Consensus definitions
proposed for pediatric multiple sclerosis and related disorders. Neurology
2007;68(Suppl.):S7-12.
[38] Khurana DS, Melvin JJ, Kothare SV, et al. Acute dissemi-
nated encephalomyelitis in children: Discordant neurologic and neuroi-
maging abnormalities and response to plasmapheresis. Pediatrics 2005;
116:431-6.
316 PEDIATRIC NEUROLOGY Vol. 39 No. 5
Recommended

















