
www.elsevier.com/locate/forsciint
Forensic Science International 165 (2007) 129–143
Sudden infant death syndrome (SIDS)—Standardised investigations
and classification: Recommendations
Thomas Bajanowski a,*, Ashild Vege b, Roger W. Byard c, Henry F. Krous d,Marianne Arnestad e, Liliana Bachs f, Jytte Banner g, Peter S. Blair h, Arne Borthne i,
Reinhard Dettmeyer j, Peter Fleming h, Peter Gaustad k, Markil Gregersen g,Jens Grøgaard l, Ellen Holter k, Christina V. Isaksen b, Jens V. Jorgensen m,Charlotte de Lange n, Burkhard Madea j, Isabella Moore o, Jorg Morland f,
Siri H. Opdal e, Petra Rasten-Almqvist p, Martin Schlaud q, Peter Sidebotham r,Kari Skullerud s, Gisela Stoltenburg-Didinger t, Arne Stray-Pedersen e,
Lisbeth Sveum e, Torleiv O. Rognum e
a Institute of Legal Medicine, University Duisburg-Essen, Hufelandstr. 55, 45122 Essen, Germanyb Section of Morphology, Department of Laboratory Medicine, Children’s and Women’s health,
Norwegian University of Science and Technology, Trondheim, Norwayc Department of Pathology, University of Adelaide & Forensic Science SA, Adelaide, Australia
d Department of Pathology, Children’s Hospital San-Diego, University of California,
San Diego School of Medicine, La Jolla, CA, USAe Institute of Forensic Medicine, University of Oslo, Norway
f Norwegian Institute of Public Health, Divison of Forensic Toxicology and Drug Abuse, Oslo, Norwayg Institute of Forensic Medicine, University of Aarhus, Denmarkh Institute of Child, Life and Health, University of Bristol, UK
i Department of Pediatric Radiology, Ulleval University Hospital, Oslo, Norwayj Institute of Legal Medicine, Rheinische Friedrich-Wilhelms-Universitat, Bonn, Germany
k Institute of Medical Microbiology, Rikshospitalet, University Hospital, Oslo, Norwayl Department of Pediatric Intensive Care, Divison of Women and Children, Ulleval University Hospital, Oslo, Norway
m Department of Pediatric Research, Rikshospitalet, University of Oslo, Norwayn Department of Radiology, Rikshospitalet, University of Oslo, Norway
o Department of Cellular Pathology, Southampton General Hospital, UKp National Board of Forensic Medicine, Solna, Sweden
q Robert-Koch-Institute, Department of Epidemiology and Health Reporting, Berlin, Germanyr University of Warick, Coventry, UK
s Department of Pathology, Divison of Neuropathology, Rikshospitalet, University hospital, University of Oslo, Norwayt Institute of Neuropathology, Charite, Berlin, Germany
Received 13 April 2006; received in revised form 20 April 2006; accepted 10 May 2006
Available online 27 June 2006
Abstract
Sudden infant death syndrome (SIDS) still accounts for considerable numbers of unexpected infant deaths in many countries. While numerous
theories have been advanced to explain these events, it is increasingly clear that this group of infant deaths results from the complex interaction of
a variety of heritable and idiosyncratic endogenous factors interacting with exogenous factors. This has been elegantly summarised in the ‘‘three
hit’’ or ‘‘triple risk’’ model. Contradictions and lack of consistencies in the literature have arisen from diverse autopsy approaches, variable
applications of diagnostic criteria and inconsistent use of definitions. An approach to sudden infant death is outlined with discussion of
appropriate tissue sampling, ancillary investigations and the use of controls in research projects. Standardisation of infant death investigations
* Corresponding author. Tel.: +49 201 723 3600; fax: +49 201 723 5940.
E-mail address: [email protected] (T. Bajanowski).
0379-0738/$ – see front matter # 2006 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.forsciint.2006.05.028

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143130
with the application of uniform definitions and protocols will ensure optimal investigation of individual cases and enable international
comparisons of trends.
# 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: Sudden infant death; San Diego definition of SIDS; Standardised investigation; Diagnostic criteria
1. Introduction
Despite considerable decline in incidence, sudden infant
death syndrome (SIDS) is still the leading cause of death among
infants between 8 and 365 days of age [1]. In Germany, the
incidence of SIDS decreased from 602 cases in 1998 to 287 in
2004, which is a relative decline of 0.77–0.39 per 1000 live
births [2]. Similar statistics have been reported by most
industrialized countries [3]. This decline is due to a genuine
decrease, rather than as a result of changes in diagnostic
practices [4,5].
A number of theories on possible causes of SIDS have been
proposed in the past, but only a few have clearly been proven,
mostly in single cases. About 30 years ago, Naeye published his
observations in SIDS cases suggesting that seven different
findings could be suitable as tissue markers indicating hypoxia
[6]. By measuring the biochemical marker of acute hypoxia,
hypoxanthine in vitreous humour, Rognum et al. in 1988
showed [7] that a large proportion of the SIDS victims had had
significant periods of hypoxia prior to death. In the 1970s, the
sleep apnea theory [8] became the theoretical basis for the
monitoring of infants showing ‘‘atypical’’ breathing patterns. In
the late 1980s and the 1990s, SIDS research became more and
more interdisciplinary, and identical risk factors for SIDS were
identified by a number of epidemiological studies in different
countries and regions. In the second half of the 1990s,
molecular–genetic studies were performed to investigate the
genetic basis of functional disturbances. Possible cardiovas-
cular causes of SIDS, for example, include abnormal reflexes
and abnormalities of the cardiac conduction system [9,10]. In
addition, ventricular tachycardia or fibrillation, often found
without evidence of structural heart disease (so-called primary
electrical disorders), may be associated with sudden cardiac
death in neonates [11,12]. One such disorder is the long-QT
syndrome (LQTS), which is characterised by increased
sensitivity of the myocardium, with an increased propensity
to develop ventricular fibrillation. Several studies have
investigated a potential association of prolonged QT interval
and SIDS, but the results were not concordant [13–18].
Already by 1972, Wedgewood [19] had introduced a ‘‘three
hit model’’ for SIDS suggesting that sudden and unexpected
death may occur if three conditions are fulfilled simulta-
neously:
(1) A
n infant is at a vulnerable developmental stage.(2) A
predisposing endogenous factor(s) is present.(3) A
n exogenous trigger initiates the lethal process.This hypothesis was later taken up and modified by Rognum
and Saugstad [20], Filiano and Kinney [21], and Kahn et al.
[22]. In particular, Rognum et al. included ‘‘genetic risk
factors’’ or ‘‘genetic make up’’ as predisposing factors [23] and
investigated the significance of mtDNA changes [24],
complement component C4 polymorphisms [25], and poly-
morphisms of the interleukin 10 gene [26]. Schneider et al. [27]
first demonstrated the link between signs of infection prior to
death in SIDS and partial deletions of the C4 gene which was
confirmed by Opdal et al. [25].
The main advantages of these ‘‘three hit theories’’ (in
contrast to others) are that most of the information from
pathology, neuropathology, microbiology, physiology, epide-
miology and pediatrics can be included in one of the three main
areas, and that these models enable integration of new
knowledge.
Currently, it is very difficult to have an overview of all of the
multiple investigations from different fields of SIDS research;
i.e. a search of PubMed using the term ‘‘SIDS’’ produces nearly
6000 publications—including 1300 from the year 2000 to 2005.
The results reported are sometimes not directly comparable as
some authors have used their own definitions for cases and
controls, and the diagnosis of SIDS has not always been
confirmed by autopsy and additional investigations, and is
therefore not in accordance with standard definitions.
2. Case definition
The investigation of cases of sudden and unexpected deaths
in all age groups is one of the major areas of forensic medicine.
The investigation of infant deaths requires the application of
special diagnostic methods and includes forensic pathology as
well as other fields of forensic medicine and medicine in
general, e.g. radiology, toxicology, microbiology, virology,
neuropathology, pediatric pathology, pediatrics, clinical chem-
istry, physiology, epidemiology and genetics. In accordance
with the internationally discussed and widely accepted new
SIDS definition (San Diego definition of SIDS [28]) the
diagnosis SIDS can be made only if an infant under 1 year of
age has died suddenly and unexpectedly, the onset of the fatal
episode was apparently associated with sleep, and a thorough
investigation of the case, including performance of a complete
autopsy and review of the circumstances of death and the
clinical history, does not provide an explanation for the death. If
these criteria are not fulfilled the cases can be termed
unclassified infant death (USID) or as sudden unexpected
death in infancy (SUDI).
USID was defined as a part of the San Diego definition of
SIDS and includes all deaths that do not meet the criteria for
SIDS but for which alternative diagnoses of natural and
unnatural conditions are equivocal, including cases for which
autopsies were not performed.

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143 131
In contrast, SUDI has been defined by Huber [29] as the part
of infant mortality where death occurs more or less suddenly
and unexpectedly. The post mortem examination, which ideally
should include a history of the gestation, delivery and postnatal
development, a death scene investigation, a family psycho-
social history, a complete autopsy, and a confidential case
conference:
- m
T
S
S
S
C
S
ay reveal changes that alone – or in combination – constitute
a sufficient cause of death (non-SIDS);
- o
r may reveal changes that even when clearly present are notsufficient to explain the death (‘borderline’ SIDS);
- o
r may fail to demonstrate any abnormalities (SIDS).This means that SUDI is the most heterogeneous group that
includes all categories of sudden and unexpected infant death.
For scientific investigations, the stratified part of the San
Diego definition should be applied. There are three subtypes of
SIDS that rely on many different pieces of information from
specific investigations such as the autopsy findings (including
additional investigations), death scene investigation, and
clinical history (Table 1). This part of the definition was
introduced to:
� ‘‘
a
a
I
t
r
c
provide recommended guidelines for general case assess-
ment, classification and diagnosis;
ble 1
n Diego definition of SIDS
Clinical history (CH) Circums
DS general definition Sudden and unexpected death Unexpla
circumsUnder 1 year of age
Lethal episode associated with sleep
Death unexplained by CH
ratified definition
Category IA SIDS (1) Older than 21 days, under 9 months Scene in
and gav
(2) Normal CH Safe sle
(3) Full term pregnancy (�37 weeks) No evid
(4) Normal growth and development
(5) No similar deaths in siblings/relatives
Category IB SIDS (1–5) Criteria for category IA SIDS Scene in
undertak
Category II SIDS Differences to category I criteria: (6) age
range (0–21 days, 270–365 days)
Mechan
by over
certainty
(7) Neonatal/perinatal conditions that have
resolved by the time of death
(8) Similar deaths in siblings, near relatives
USID Criteria for category I or II SIDS are not
fulfilled
Alternat
unnatur
iteria used in the general and stratified part. USID: Unclassified sudden infant d
ience and Business Media).
� a
ta
in
tan
ve
e n
ep
en
ve
en
ica
lay
iv
al
ea
ssist pathologists by detailing steps for infant death
investigation and diagnostic categorization;
� id
entify and include cases that have been recently incorrectlyexcluded from SIDS groups due to findings of bed sharing
and prone sleeping position;
� f
ormalize current practices among pathologists of separatingcases based on degrees of certainty and the comfort with
which a conclusion of SIDS could be made;
� r
educe diagnostic confusion by introducing uniform terms;� p
rovide a framework for researchers and identify the mosttypical cases for study;
� a
ssist in the evaluation of published data;� p
rovide a readily accessible breakdown of SIDS cases basedon age groups and investigative information’’ [28].
3. Study design
Study designs depend on the hypothesis that is being tested.
In general, SIDS studies can be designated as descriptive
studies (DS), as case-control studies (CCS) or as self-controlled
case series (SCCS).
DS are suitable for comparing SIDS with control cases
for differences in, for example, morphology, immunology,
and genetics. Because cases and controls are not matched, it
has to be shown that the groups do not differ significantly
for important parameters such as age, gender, and region.
nces of death Autopsy
ed after review of the
ces
Unexplained after complete autopsy
stigation performed
o explanation
(1) No lethal pathological findings
environment (2) No unexplained trauma, abuse, neglect
or unintentional injury
ce for an accident (3) No substantial thymic stress
(4) Toxicology, microbiology, radiology,
vitreous chemistry and metabolic screening
negative
stigation was not (1–4); (5) One or more of the following
analyses were not performed: toxicology,
microbiology, radiology, vitreous chemistry
and metabolic; screening
l asphyxia or suffocation
ing not determined with
(1–5); (6) Abnormal growth and development
not thought to have contributed to death
(7) More marked inflammatory changes or
abnormalities not sufficient to cause the death
e diagnoses of natural or
death are equivocal
Autopsy has not been performed
th. Modified from Bajanowski et al. [77] (with kind permission of Springer

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143132
The number of cases in the groups should be similar. A minimal
number of five cases should be achieved as a prerequisite for
statistical tests [30].
The most suitable form of SIDS studies is at present the CCS.
This type of study can be used to evaluate, for example,
morphological variables, chemical parameters, immunological
findings, as well as epidemiological data. The ratio of cases and
controls can differ. For morphological investigations a ratio of
1:1 should be sufficient (because of the availability of suitable
controls). For epidemiological studies the findings in SIDS are
usually compared to findings in living infants who are matched
for age, gender, region, and if necessary for other variables (e.g.
time of death). A higher number of controls (cases:controls = 1:2
or 1:3) can improve the power of the investigation that makes it
possible to identify risk factors with lower relative risk.
SCCS are particularly suitable for investigating very rare
and non-recurring events [31], and were specifically developed
for vaccine safety evaluation.
An ideal study design should have the following character-
istics:
- n
one-selective, prospective case ascertainment (all cases ofsudden and unexpected infant death should be initially
included as often it is not known if the death is explained until
after the investigation),
- s
tandardised analyses of the circumstances of death by anexperienced specialist in forensic medicine and/or a police
officer,
- s
tandardised autopsies in all cases,- f
ull information on clinical history,- f
ull information on outcome, exposure and confounders,- a
dequate selection of controls, and- u
niform diagnostic criteria,- a
ny findings should be systematically entered into the studydatabase for scrutiny alongside the epidemiological findings.
Prior to the beginning of any study the study region, the
study population, inclusion and exclusion criteria for cases and
controls, and the recruitment of cases and controls have to be
defined by the investigators.
4. Controls
Suitable controls for morphological, morphometric, and
chemical studies have been the subject of controversy in the
past. This is not surprising, as controls are needed for a
phenomenon with an unclear pathophysiology. Nevertheless,
there are general requirements that should be fulfilled by the
controls:
Age: Control cases should be of a similar age to SIDS cases.
This means that controls should be matched for age, or if this
is not possible, aged under 6 months.
Gender: The typical ratio of males to females should be
matched by the controls.
Region. Because of different SIDS incidences from region to
region or country to country and other possible differences
(e.g. different infant care practices), controls should have
lived in the same region as the index cases.
Ethnicity. Significant differences in the incidence of SIDS
among populations and different ethnic groups requires
matching by controls.
Cause of death. Most investigators agree that cases of
unnatural death with short clinical courses are suitable for
use as controls. Because ‘‘suffocation’’ may be a possible
factor leading to death in SIDS, other cases of unnatural
death would be better controls. If such cases are only rarely
available, natural deaths with clearly defined causes of
death, and short histories of disease could be used as controls
(e.g. fulminant pneumonia, meningitis, intussusception). It
is important that such cases are investigated separately, and
that the results are clearly separated for statistical analyses.
In addition to these controls, for genetic investigations, material
from the general population could be used.
For epidemiological CCSs, the minimal matching criteria
are age, gender and region. For each study, it has to be shown
that the groups were similar/comparable for significant
parameters, and that there was no significant re-call bias.
Proportions of response, contact and co-operation can be
calculated according to the definitions of Slattery et al. [32].
5. Circumstances of death
Investigation of the circumstances of death is important to
help to differentiate between natural and unnatural causes of
death. Furthermore, in cases of SIDS deaths the results from
death scene investigations may be suitable for generating new
hypotheses concerning risk factors. Therefore, these investiga-
tions have been included in SIDS definitions from the early
nineties as being mandatory [33]. In some studies, scoring
systems were developed and applied to standardise these
investigations and to compare the results with regard to the
cause of death [34,35]. In a pilot study, the Norwegian group
used the body position when found, the firmness of the mattress,
layers of clothing, type of duvet, room temperature and co-
sleeping as criteria [34]. A more detailed investigation has been
performed as a part of the German SIDS study, the
methodology of which has been described by Schlaud et al.
[36]. Furthermore, some investigators recommend the use of a
video recorder to document the death scene. This can help with
the case discussion held weeks later.
These investigations are usually performed by police
officers who should have had special training in this field of
investigation [34]. Specialists in forensic medicine can perform
these investigations, together with police officers, but in the
past this has been achieved in only a few scientific studies.
6. Standardised autopsy protocol (SAP)
Internationally there are certain protocols that have been
validated by different studies. These SAPs [37–39] are similar
and accord with European guidelines for medico-legal
autopsies [40] and closely reflect the International Standardised
Autopsy Protocol (ISAP, Table 2) [41] of the Global Strategy

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143 133
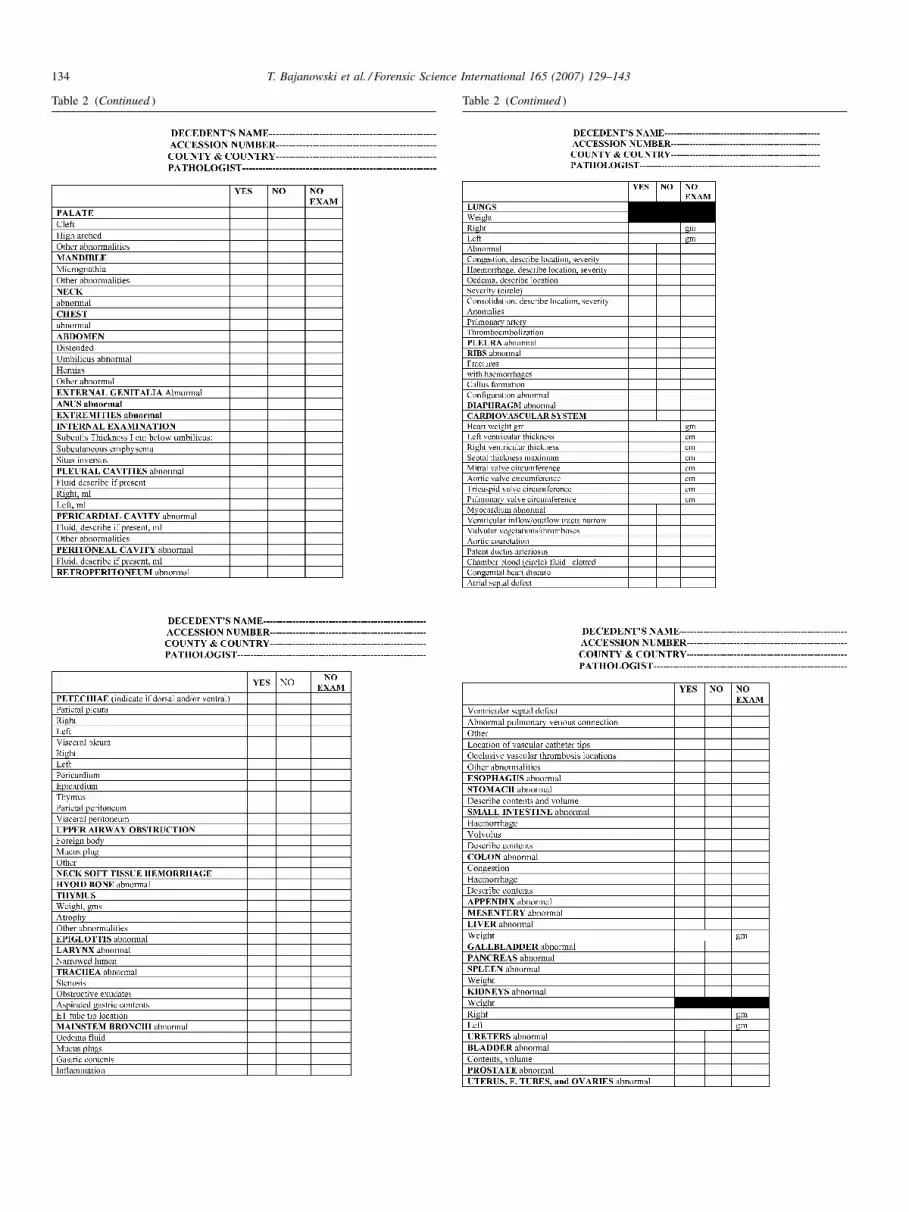
Table 2
International Standardised Autopsy Protocol
Table 2 (Continued )
T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143134
Table 2 (Continued ) Table 2 (Continued )

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143 135
Table 2 (Continued ) Table 2 (Continued )
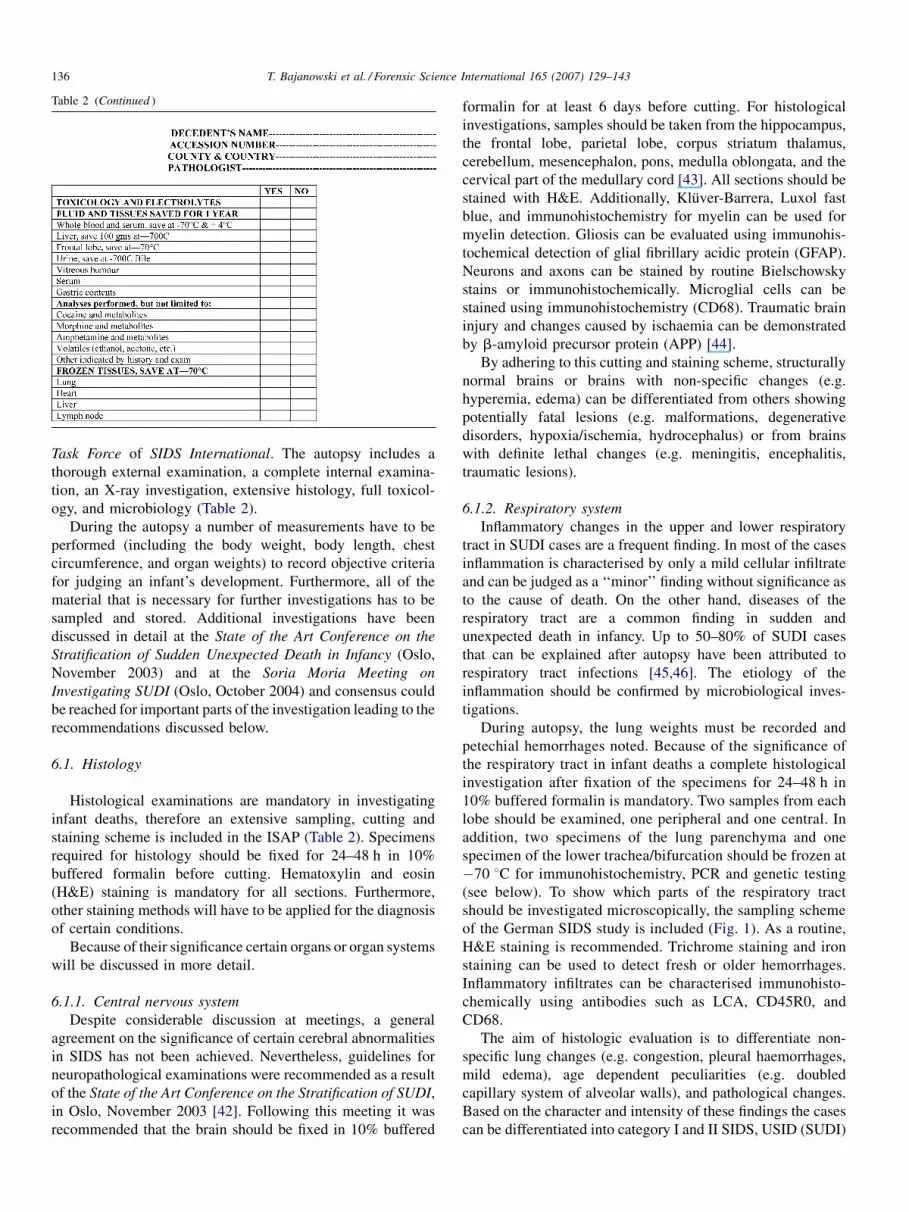
T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143136
Table 2 (Continued )
Task Force of SIDS International. The autopsy includes a
thorough external examination, a complete internal examina-
tion, an X-ray investigation, extensive histology, full toxicol-
ogy, and microbiology (Table 2).
During the autopsy a number of measurements have to be
performed (including the body weight, body length, chest
circumference, and organ weights) to record objective criteria
for judging an infant’s development. Furthermore, all of the
material that is necessary for further investigations has to be
sampled and stored. Additional investigations have been
discussed in detail at the State of the Art Conference on the
Stratification of Sudden Unexpected Death in Infancy (Oslo,
November 2003) and at the Soria Moria Meeting on
Investigating SUDI (Oslo, October 2004) and consensus could
be reached for important parts of the investigation leading to the
recommendations discussed below.
6.1. Histology
Histological examinations are mandatory in investigating
infant deaths, therefore an extensive sampling, cutting and
staining scheme is included in the ISAP (Table 2). Specimens
required for histology should be fixed for 24–48 h in 10%
buffered formalin before cutting. Hematoxylin and eosin
(H&E) staining is mandatory for all sections. Furthermore,
other staining methods will have to be applied for the diagnosis
of certain conditions.
Because of their significance certain organs or organ systems
will be discussed in more detail.
6.1.1. Central nervous system
Despite considerable discussion at meetings, a general
agreement on the significance of certain cerebral abnormalities
in SIDS has not been achieved. Nevertheless, guidelines for
neuropathological examinations were recommended as a result
of the State of the Art Conference on the Stratification of SUDI,
in Oslo, November 2003 [42]. Following this meeting it was
recommended that the brain should be fixed in 10% buffered
formalin for at least 6 days before cutting. For histological
investigations, samples should be taken from the hippocampus,
the frontal lobe, parietal lobe, corpus striatum thalamus,
cerebellum, mesencephalon, pons, medulla oblongata, and the
cervical part of the medullary cord [43]. All sections should be
stained with H&E. Additionally, Kluver-Barrera, Luxol fast
blue, and immunohistochemistry for myelin can be used for
myelin detection. Gliosis can be evaluated using immunohis-
tochemical detection of glial fibrillary acidic protein (GFAP).
Neurons and axons can be stained by routine Bielschowsky
stains or immunohistochemically. Microglial cells can be
stained using immunohistochemistry (CD68). Traumatic brain
injury and changes caused by ischaemia can be demonstrated
by b-amyloid precursor protein (APP) [44].
By adhering to this cutting and staining scheme, structurally
normal brains or brains with non-specific changes (e.g.
hyperemia, edema) can be differentiated from others showing
potentially fatal lesions (e.g. malformations, degenerative
disorders, hypoxia/ischemia, hydrocephalus) or from brains
with definite lethal changes (e.g. meningitis, encephalitis,
traumatic lesions).
6.1.2. Respiratory system
Inflammatory changes in the upper and lower respiratory
tract in SUDI cases are a frequent finding. In most of the cases
inflammation is characterised by only a mild cellular infiltrate
and can be judged as a ‘‘minor’’ finding without significance as
to the cause of death. On the other hand, diseases of the
respiratory tract are a common finding in sudden and
unexpected death in infancy. Up to 50–80% of SUDI cases
that can be explained after autopsy have been attributed to
respiratory tract infections [45,46]. The etiology of the
inflammation should be confirmed by microbiological inves-
tigations.
During autopsy, the lung weights must be recorded and
petechial hemorrhages noted. Because of the significance of
the respiratory tract in infant deaths a complete histological
investigation after fixation of the specimens for 24–48 h in
10% buffered formalin is mandatory. Two samples from each
lobe should be examined, one peripheral and one central. In
addition, two specimens of the lung parenchyma and one
specimen of the lower trachea/bifurcation should be frozen at
�70 8C for immunohistochemistry, PCR and genetic testing
(see below). To show which parts of the respiratory tract
should be investigated microscopically, the sampling scheme
of the German SIDS study is included (Fig. 1). As a routine,
H&E staining is recommended. Trichrome staining and iron
staining can be used to detect fresh or older hemorrhages.
Inflammatory infiltrates can be characterised immunohisto-
chemically using antibodies such as LCA, CD45R0, and
CD68.
The aim of histologic evaluation is to differentiate non-
specific lung changes (e.g. congestion, pleural haemorrhages,
mild edema), age dependent peculiarities (e.g. doubled
capillary system of alveolar walls), and pathological changes.
Based on the character and intensity of these findings the cases
can be differentiated into category I and II SIDS, USID (SUDI)

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143 137
Fig. 1. Recommended sections for non-CNS histology (modified according to Findeisen et al. [39], with kind permission of Springer Science and Business Media).
or explained infant death. The Nordic diagnostic criteria for the
exclusion of SIDS [47] were modified during the State of the
Art Conference on the Stratification of SUDI and the following
recommendations were made [48]:
Category I SIDS: Can be used when neither autopsy nor
clinical information reveals a cause of death. The upper
respiratory tract, bronchi and peribronchial tissue can show
mild to moderate lymphoid infiltrates with insignificant
numbers of neutrophils or no neutrophils within lumina.
Interstitial lung tissue may occasionally contain diffusely
scattered lymphocytes or a few moderate-sized inflamma-
tory foci. Fewer than 10 alveoli may contain a maximum of
10 neutrophils (Fig. 2).

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143138
Fig. 2. Lung histology from an 8-month-old boy in a case of SIDS where the autopsy and histology showed no signs of disease or malformations: (a) congestion and
edema, (b) subpleural intra-alveolar hemorrhage (H&E, magnification: a, �25; b, �100).
Fig. 3. (a) Lung histology in a 3-month-old girl with established bronchop-
neumonia showing intra-alveolar aggregates of polymorphonuclear leukocytes.
H&E, �100. (b) Lung histology in a 4-month-old boy showing interstitial
mononuclear cell infiltrates in a case of interstitial pneumonia. H&E, �40.
Category II SIDS. Congenital disorders or pre-existing
clinical symptoms, and/or post mortem findings that are not
sufficient to explain the cause of death. Mild changes are
present in different parts of the respiratory tract that are
insufficient to explain death. The upper respiratory tract,
bronchi and peribronchial tissue may have a neutrophil
infiltration in mucous membranes but insufficient inflam-
matory infiltrate is present within lumina to obstruct larger
bronchi. Lymphoid cell infiltrates form heavy cuffs around
the bronchi in more than one section. In the interstitium there
are moderate lymphoid infiltrates in several sections. The
alveoli do not show a consolidation, but at least 10 alveoli
contain each 10 or more inflammatory cells.
Explained infant death: Bronchi and peribronchial tissue are
infiltrated by a higher number of cells; purulent exudate fills
lobar bronchi or larger branches of bronchial tree; atelectasis
occurs distant to obstruction. The interstitial tissue is
characterised by widespread lymphoid infiltrates in the walls
of alveoli in all sections (interstitial pneumonia). The alveoli
may show marked, obvious pulmonary consolidation.
Furthermore, specific lung diseases (congenital, allergic,
inflammatory) can be sufficient to explain the death, as well
as established bronchiolitis (Fig. 3).
6.1.3. Heart
During autopsy the ventricular thickness and the valve
circumferences should be recorded and compared to age-
dependent reference data. Abnormalities of the heart
configuration as well as of the great vessels should be
described.
One sample of the myocardium from the left ventricle has to
be taken for immunohistochemistry, PCR and genetic testing if
indicated and frozen at �70 8C. The remaining material has to
be fixed in 10% buffered formalin before cutting [49].

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143 139
Fig. 4. Diagramatic representation of sections of the right atrium, including the
SA node, according to the NORD SIDS criteria [49] (with kind permission of
the Scand. J. Forensic Sci.).
For the histological examination, six to eight sections are
recommended (Figs. 4 and 5) [49]. All sections should be
stained with H&E. Other staining methods may be necessary to
show special changes.
The detection of myocarditis may require special methodol-
ogy, as this diagnosis may present difficulties when there are
equivocal histological findings using conventional histological
stains. When applying a comprehensive combination of molecu-
lar and immunohistochemical techniques a higher prevalence of
viral myocarditis can usually be detected. However, the detection
of myocarditis also depends on the extent of sampling.
6.1.3.1. Conventional histology. In 1986, the Dallas criteria
for the histological diagnosis of active myocarditis were
Fig. 5. Recommended sections through the myocardium. (A) Right ventricle,
(B) AV node, (C) posterior papillary muscle, (D) posterior part of the left
ventricle, (E) anterior papillary muscle, (F) anterior part of the left ventricle,
according to the NORD SIDS criteria [49] (with kind permission of the Scand. J.
Forensic Sci.).
introduced [50]. When examining endomyocardial biopsies by
using light microscopy and conventional stains, infiltrating
lymphocytes and myocytolysis were considered markers of an
active (acute) myocarditis. Without myocytolysis, a borderline
or ongoing myocarditis may not be diagnosed despite
lymphocytic infiltration. But the Dallas criteria probably
underestimate the true incidence of myocarditis [51] and the
degree of interobserver variability is large [52]. Myocarditis
can present as a pure focal inflammatory process. Therefore, a
considerable number of myocardial specimens must be
obtained at autopsy to avoid a ‘‘sampling error’’ [53] and
there are cases in which only 1 or 2 of 10 or more myocardial
samples show focal lympho-monocytic infiltrates (Fig. 6).
6.1.3.2. Immunohistochemistry. The use of immunohisto-
chemical methods for the diagnosis of acute myocarditis has
been described in previous studies [54–56]. The immunohis-
tochemistry given below is advised for research purposes: As a
fixative, neutral phosphate-buffered formaldehyde (pH 7.0)
should be used for not longer than 48 h. The de novo expression
of antigens such as the major histocompatibility complex (MHC)
may indicate immune system activation (Fig. 7) as a result of
lympho-monocytic viral myocarditis associated with an
increased number of LCA+-leucocytes, CD45R0+-T-lympho-
cytes and CD68+-macrophages. T-lymphocytes are known to
react with foreign antigens when present on cell surfaces in
conjunction with MHC antigens [57]. Additionally, the expres-
sion of cell adhesion molecules such as E-selectine, vascular cell
adhesion molecule-1, and intercellular adhesion molecule-1, as
well as cytokines (e.g. IL-1, IL-2, tumour necrosis factor—TNF,
perforin), is increased in cases of viral myocarditis [58–61].
In the past, the finding of a mean value of more than 5 T-
lymphocytes per high-power field (HPF), when investigating 20
visual fields at 400-fold magnification, has been regarded as a
sign of active myocarditis in adults [62]. In the younger age
groups, perhaps more rigorous criteria should be applied to
avoid false positive diagnoses of myocarditis [63]. The finding
of more than 15 T-lymphocytes per HPF could be interpreted as
a reliable sign of active myocarditis, in younger age groups.
Fig. 6. Focal lympho-monocytic infiltration in one out of eight myocardial
sections using conventional H&E stains in a 4-month-old boy who had a viremia
due to cytomegalovirus detected by PCR (magnification �400).

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143140
Fig. 7. Marked expression of MHC-class-II-molecules on the endothelium of
small vessels and on interstitial leucocytes (same case as Fig. 6). The case was
suspected as being SIDS according to the death certification and at the time of
autopsy.
Cases with 5–10 T-lymphocytes per HPF can be regarded as
‘‘suspicious’’, as should cases with more than 10 macrophages
per HPF. The significance of cases with an increased number of
macrophages remains unclear at the moment, however, it may
indicate a late inflammatory process. Qualification and
quantification of interstitial leucocytes, T-lymphocytes, and
macrophages may help to identify cases with a high index of
suspicion of myocarditis.
6.1.3.3. Molecular pathological methods. In adults, virus
detection by reverse transcriptase (rt)-PCR and in situ
hybridization has revealed an association between myocarditis
and virus infection, especially enterovirus infection with
coxsackie viruses group B, may occur. These viruses are one
of the most frequently identified infectious agents responsible
for acute myocardial infections and outbreaks have been
described [64]. Several studies have used molecular patholo-
gical methods to detect viral genome in cases of suspected
SIDS [65]. Over the past few years, numerous reports based
mainly on PCR-derived molecular data have shown an
association between other viral infection and myocarditis:
e.g. adenoviruses, Epstein-Barr-virus, cytomegaloviruses,
parvovirus B 19. Modern immunohistochemical techniques
and molecular pathological methods have provided powerful
tools to investigate lethal myocarditis in cases devoid of
traditional histological findings according to the Dallas criteria.
With regard to the time-dependent course of viral myocarditis,
early virus-induced myocardial damage may already have
taken place before histological and immunohistochemical signs
of myocarditis can be observed [66]. Combined investigations
using molecular pathological techniques and immunohisto-
chemical methods may assist in establishing more reliable
diagnoses of myocarditis in certain pediatric fatalities.
6.2. Diagnostic criteria
(1) Category I SIDS: Cases without any significant
pathological changes or with less than 15 lymphocytes in
one section. (2) Category II SIDS: Cases showing changes that
might be associated with functional disturbances, but that
cannot explain death (e.g. focal hemorrhages, patent ductus
arteriosus after the first month of age, minor ventricular septal
defect (VSD) or atrial septal defect (ASD) without significant
influence on cardiac morphology, a family history of sudden
death). (3) Non-SIDS: Changes that are undoubtedly fatal, or
that could be fatal in combination with alterations in other
organs [5].
6.3. Metabolic/genetic investigation
It is recognised that the risk of unexpected infant death is
increased in those families where one infant has died.
Nevertheless, the presence of multiple deaths in one family
should raise concerns. This may reflect the persistence of
underlying recognised risk factors, or may indicate a specific
cause of death including inherited disorders and homicide. In
the past diagnostic tools were limited, but newer methods, such
as tandem mass spectrometry and PCR have opened new
possibilities.
During the State of the Art Conference on the Stratification
of SUDI, Oslo, November 2003 minimal requirements for
metabolic and genetic investigations were discussed [67]. It
was stressed that a detailed family history was necessary in
addition to a full autopsy, including frozen sections of the liver,
the heart and the muscles for fat staining. Metabolic screening
is indicated in all cases. For this reason, material has to be taken
during the autopsy for further testing: blood and spleen for
molecular–genetic investigations, fibroblast cultures for chro-
mosomal analysis, and blood or bile spots for metabolic
screening, as well as urine when possible.
The increasing knowledge of genetically determined
disorders associated with sudden death in infancy and
childhood makes it difficult to recommend a defined set of
analyses or investigations. If there is any indication of the
presence of a genetically determined disturbance, for example
disorders of cardiac function or metabolism, specific testing
must be pursued.
6.4. Bacteriology and virology
Bacteriological and virological investigations are manda-
tory in cases of sudden death in infancy and childhood. In
cases of histologically diagnosed infection these investi-
gations may prove the etiology. A discussion of all of
the findings may be necessary to enable correct interpreta-
tion of the findings. Important questions to be answered are
[68]:
- C
ould the bacteria/virus be a cause of death or a contributor todeath or not have any significance as to the death?
- D
o other findings support the diagnosis of infection (e.g.previous history, histology)?
- D
o the potentially pathogenic bacteria detected belong to thenormal post mortem flora? Are the viruses detected a
reflection of asymptomatic carriage?

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143 141
7. Radiology
Radiological investigation is mandatory as part of the post
mortem investigation of infant death. In particular, older
traumatic lesions, minor changes, and skeletal abnormalities
and diseases may be overlooked if these investigations are not
performed. Radiology should be performed prior to the autopsy
to define which parts of the skeleton have to be removed for
subsequent investigations, e.g. histology. From the literature, it is
known, that radiology contributes to the diagnosis in about 3–4%
of infant deaths [69] and in about 25% of unnatural deaths [70].
As a first approach the use of high quality radiographs is
recommended [71]. The standard projections are: antero-
posterior, as well as lateral views of the appendicular and axial
skeleton and thorax/abdomen, and two oblique views of the ribs
[72]. These standard views can be completed by additional
projections if necessary. New techniques (multislice computed
tomography, magnetic resonance imaging) can be used for the
detection of specific lesions [73,74], but are not routinely used
in the post mortem investigation of SUDI at present [71].
8. Toxicology
The frequency of poisoning as a cause of death in infancy
has varied between 2 and 4% of all sudden und unexpected
infant deaths [75] and reached about 10–12% in unnatural
deaths [70]. Therefore, toxicological analyses are mandatory in
investigating SUDI.
Although blood from the femoral vein is the most suitable
material to perform toxicological analyses on, blood from the
cardiac ventricles has to be used in most cases because it is
often impossible to obtain sufficient amounts of femoral vein
blood from infants at autopsy. Bachs et al. [76] suggest that the
primary screening could be done using cardiac blood, and that
positive results should be confirmed by investigating femoral
vein blood. Furthermore, cerebrospinal fluid, vitreous humour,
urine, stomach contents, and liver tissue should also be taken
and retained for possible future analyses.
Toxicological screening should include alcohols, narcotics
and common prescription and illicit drugs [76]. as a minimum.
If positive results are obtained the significance of the findings
has to be established, i.e. is this within the therapeutic range, or
is it toxic or even lethal? To answer these questions detailed
knowledge of the drug history, clinical circumstances
(resuscitation attempts), circumstances of death, drug distribu-
tion in infants, and metabolic capacity in this age group, is
necessary. Therefore, Bachs et al. recommend cooperation
among pediatricians, pathologists/forensic pathologists and
toxicologist in interpreting such results [76]. It is recognised,
however, that the interpretation of toxicologic findings in
infants may be difficult, and that therapeutic, toxic and lethal
levels in adults may not be the same in infants.
9. Final diagnosis
Finally, it is essential that all information available should
be shared at a multiprofessional meeting where the case is
thoroughly discussed, so that the members of the case
conference may contribute to the classification. The task of
solving these cases requires the knowledge of all the
professionals involved, and should not be left to a single
person, whatever the field of expertise.
10. Conclusions
During the previous 2 years discussions on the investigation
of sudden and unexpected deaths in infancy have led to detailed
recommendations for the examination of different organs and
organ systems as well as for additional investigations.
Furthermore, consensus at various meetings has been achieved
for diagnostic criteria for SIDS, and for the exclusion of SIDS
with regards to cardiac pathology, lung pathology, metabolic/
genetic investigations, toxicology, microbiology/virology, and
radiology. Nevertheless, the new San Diego definition of SIDS
can only be successfully used if further progress in the
standardisation of diagnostic criteria can be achieved. The
recommendations above can be used as a guide for such further
standardisation.
References
[1] T. Dwyer, A.L. Ponsonby, SIDS epidemiology and incidence, Pediatr.
Ann. 24 (1995) 354–356.
[2] Statistisches Bundesamt Deutschland, Gestorbene Sauglinge nach Alter
und ausgewahlten Todesursachen. (ICD10: R95) Statistischer Informa-
tionsservice, Gustav-Stresemann-Ring 11, Wiesbaden, 2004.
[3] K. Fitzgerald, The ‘‘reduce the risks’’ campaign, SIDS International, the
Global strategy task force and the European society for the study and
prevention of infant death, in: R.W. Byard, H.F. Krous (Eds.), Sudden
Infant Death Syndrome. Problems, Progress and Possibilities, Oxford
University Press, 2001, pp. 310–318.
[4] R.W. Byard, S.M. Beal, Has changing diagnostic preference been respon-
sible for the recent fall in incidence of sudden infant death syndrome in
South Australia? J. Paediatr. Child. Health 31 (1995) 197–199.
[5] A. Vege, T.O. Rognum, Use of new Nordic criteria for classification of
SIDS to reevaluate diagnoses of sudden unexpected infant deaths in the
Nordic countries, Acta Paediatr. 4 (1997) 391–396.
[6] R.L. Naeye, Sudden infant death, Sci. Am. 242 (1980) 52–58.
[7] T.O. Rognum, O.D. Saugstad, S. Øyasaeter, B. Olaisen, Elevated levels of
hypoxanthine in the vitreous humour indicate prolonged cerebral hypoxia
in victims of sudden infant death syndrome, Pediatrics 81 (1988) 395–398.
[8] C. Guilleminault, T.F. Anders, The pathophysiology of sleep disorders in
pediatrics. Part II. Sleep disorders in children, Adv. Pediatr. 22 (1976)
151–174.
[9] T.N. James, Sudden death in babies: new observations in the heart, Am. J.
Cardiol. 22 (1968) 457–506.
[10] T. Bajanowski, C. Ortmann, K. Teige, H. Wedekind, F. Zack, I. Rose, B.
Brinkmann, Pathological changes of the heart in sudden infant death, Int.
J. Legal Med. 117 (2003) 193–203.
[11] P.J. Schwartz, S.G. Priori, R. Dumaine, C. Napolitano, C. Antzelevitch, M.
Stramba-Badiale, T.A. Richard, M.R. Berti, R. Bloise, A molecular link
between the sudden infant death syndrome and the long-QT syndrome, N.
Engl. J. Med. 343 (2000) 262–267.
[12] P.J. Schwartz, S.G. Priori, R. Bloise, C. Napolitano, E. Ronchetti, A.
Piccinini, C. Goj, G. Breithardt, E. Schulze-Bahr, H. Wedekind, J. Naftoli,
Molecular diagnosis in a child with sudden infant death syndrome, Lancet
358 (2001) 1342–1343.
[13] B.J. Maron, C.E. Clark, R.E. Goldstein, S.E. Epstein, Potential role of Q–T
interval prolongation in sudden infant death syndrome, Circulation 54
(1976) 423–430.

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143142
[14] M.K. Kukolich, A. Telsey, J. Ott, A.G. Motulsky, Sudden infant death
syndrome: normal Q–T interval in ECGs of relatives, Pediatrics 60 (1977)
51–54.
[15] D.P. Southall, W.A. Arrowsmith, V. Stebbens, J.R. Alexander, QT interval
measurements before sudden infant death syndrome, Arch. Dis. Child. 61
(1986) 327–333.
[16] P.J. Schwartz, M. Stramba-Badiale, A. Segantini, P. Austoni, G. Bosi, R.
Giorgetti, F. Grancini, E.D. Marni, F. Perticone, D. Rosti, P. Salice,
Prolongation of the QT interval and the sudden infant death syndrome,
N. Engl. J. Med. 338 (1998) 1709–1714.
[17] M.J. Ackerman, B.L. Siu, W.Q. Sturner, D.J. Tester, C.R. Valdivia, J.C.
Makielski, J.A. Towbin, Postmortem molecular analysis of SCN5A
defects in sudden infant death syndrome, JAMA 286 (2001) 2264–
2269.
[18] H. Wedekind, T. Bajanowski, P. Friederich, G. Breithardt, T. Wulfing, C.
Siebrans, B. Engeland, G. Monning, W. Haverkamp, B. Brinkmann, E.
Schulze-Bahr, Sudden infant death syndrome and long QT syndrome: an
epidemiological and genetic study, Int. J. Legal. Med. 13 (2005) 1–9.
[19] R.J. Wedgewood, Review of USA experience, in: F.E. Camps, R.G.
Carpenter (Eds.), Sudden and Unexpected Death in Infancy (cot death),
Wright, Bristol, 1975, p. 28.
[20] T.O. Rognum, O.D. Saugstad, Biochemical and immunological studies in
SIDS victims. Clues to the understanding of the death mechanism, Acta
Paediatr. 389 (Suppl.) (1993) 82–85.
[21] J.J. Filiano, H.C. Kinney, A perspective on neuropathologic findings in
victims of the sudden infant death syndrome: the triple-risk model, Biol.
Neonate 65 (1994) 194–197.
[22] A. Kahn, J. Groswasser, I. Kelmanson, Risk factors for SID: risk factors
for ALTE? From epidemiology to physiology, in: T.O. Rognum (Ed.),
Sudden Infant Death Syndrome. New Trends in the Nineties, Scandina-
vian University Press, Oslo, 1995, pp. 132–137.
[23] S.H. Opdal, T.O. Rognum, The sudden infant death syndrome gene: does it
exist? Pediatrics 114 (2004) e506–e512.
[24] S.H. Opdal, A. Vege, T. Egeland, M.A. Musse, T.O. Rognum, Possible role
of mtDNA mutations in sudden infant death, Pediatr. Neurol. 27 (2002)
23–29.
[25] S.H. Opdal, A. Vege, A.K. Stave, T.O. Rognum, The complement
component C4 in sudden infant death, Eur. J. Pediatr. 158 (1999) 210–212.
[26] S.H. Opdal, A. Opstad, A. Vege, T.O. Rognum, IL-10 gene polymorph-
isms are associated with infectious cause of sudden infant death, Hum.
Immunol. 64 (2003) 1183–1189.
[27] P.M. Schneider, C. Wendler, T. Riepert, L. Braun, U. Schacker, M. Horn,
H. Althoff, R. Mattern, C. Rittner, Possible association of sudden infant
death with partial complement C4 deficiency revealed by post-mortem
DNA typing of HLA class II and III genes, Eur. J. Pediatr. 149 (1989) 170–
174.
[28] H.F. Krous, J.B. Beckwith, R.W. Byard, T.O. Rognum, T. Bajanowski, T.
Corey, E. Cutz, R. Hanzlick, T.G. Keens, E.A. Mitchell, Sudden infant
death syndrome (SIDS) and unclassified sudden infant deaths (USID): a
definitional and diagnostic approach, Pediatrics 114 (2004) 234–238.
[29] J. Huber, Talk given in a panel discussion on the definition of SIDS, Third
SIDS International Conference, Stavanger 1994. Quoted in: T.O. Rognum,
M. Willinger, The story of the ‘‘Stavanger, definition’’, In: T.O. Rognum
(Ed.), Sudden Infant Death, Syndrome, New Trends in the Nineties,
Scandinavian University Press, Oslo, 1995, pp. 17–20.
[30] H. Shahai, A. Khurshid, Statistics in Epidemiology: Methods, Techniques,
and Application, CRC press, Hardea, 1996, p. 216.
[31] C. Farrington, Relative incidence estimation from case-series for vaccine
safety evaluation, Biometrics 51 (1995) 228–235.
[32] M.L. Slattery, S.L. Edwards, B.J. Caan, R.A. Kerber, J.D. Potter, Response
rates among control subjects in case-control studies, Ann. Epidemiol. 5
(1995) 245–249.
[33] T.O. Rognum, M. Willinger, The story of the ‘‘Stavanger-definition’’, in:
T.O. Rognum (Ed.), Sudden Infant Death Syndrome. New Trends in the
Nineties, Scandinavian University Press, Oslo, 1995, pp. 17–20.
[34] L. Sveum, P.D. Sidebotham, M. Schlaud, P.S. Blair, T.O. Rognum,
Significance of death scene investigation, Nordisk Rettsmedisin 9
(2003) 64–65.
[35] P.J. Fleming, P.S. Blair, P.D. Sidebotham, T. Hayler, Investigating sudden
unexpected deaths in infancy and childhood and caring for bereaved
families: an integrated multiagency approach, BMJ 328 (2004) 331–334.
[36] M. Schlaud, A. Fieguth, D. Geissler, B. Giebe, S. Heide, K.P. Larsch, C.F.
Poets, U. Schmidt, J. Sperhake, C. Weihs, W.J. Kleemann, Details from the
German case-control death-scene investigation study on SIDS, J. Perinat.
Med. 29 (Suppl. 2) (2001) 49 (Abstract).
[37] E.A. Mitchell, R. Scragg, A.W. Stewart, D.M. Becroft, B.J. Taylor, R.P.
Ford, I.B. Hassall, D.M. Barry, E.M. Allen, A.P. Roberts, Results from
the first year of the New Zealand cot death study, N. Z. Med. J. 104 (1991)
71–76.
[38] M.P. l’Hoir, A.C. Engelberts, G.Th.J. van Well, T. Bajanowski, K.
Helweg-Larsen, J. Huber, Sudden unexpected death in infancy; epide-
miology determined risk factors related to a pathology classification, Acta
Paediatr. 87 (1998) 1279–1287.
[39] M. Findeisen, M. Vennemann, B. Brinkmann, C. Ortmann, I. Rose, W.
Kopcke, G. Jorch, T. Bajanowski, German study on sudden infant death
(GeSID): design, epidemiological and pathological profile, Int. J. Legal.
Med. 118 (2003) 163–169.
[40] B. Brinkmann, Harmonisation of medico-legal autopsy rules, Int. J. Legal.
Med. 113 (1999) 1–14.
[41] H.F. Krous, Instruction and reference manual for the International Stan-
dardise Autopsy Protocol for sudden unexpected infant death, J. SIDS
Infant Mortal. 1 (1996) 203–246.
[42] G. Stoltenburg-Didinger, K. Skullerud, H.F. Krous III, Cerebral changes,
Nordisk Rettsmedisin 9 (2003) 66–67.
[43] D.L. Sparks, J.C. Hunsacker, Neuropathology of sudden infant death
(syndrome): literature review and evidence of a probable apoptotic
degenerative cause, Childs Nerv. Syst. 18 (2002) 568–592.
[44] R.R. Reichard, C. Smith, D.I. Graham, The significance of beta-APP
immunoreactivity in forensic practice, Neuropathol. Appl. Neurobiol. 31
(2005) 304–313.
[45] T. Bajanowski, B. Rolf, G. Jorch, B. Brinkmann, Detection of RNAviruses
and pulmonary viral infection in sudden infant death (SID), Int. J. Legal.
Med. 117 (2003) 237–240.
[46] T. Bajanowski, B. Brinkmann, Pulmonary viral infection in SIDS, in: T.O.
Rognum (Ed.), Sudden Infant Death Syndrome. New Trends in the
Nineties, Scandinavian University Press, Stockholm, 1995, pp. 199–202.
[47] M. Gregersen, E. Gidlund, J. Hirvonen, E.M. Loberg, Classification of
lung changes, in: T.O. Rognum (Ed.), Sudden Infant Death Syndrome.
New Trends in the Nineties, Scandinavian University Press, Stockholm,
1995, pp. 51–53.
[48] C.V. Isaksen, M. Gregersen, T. Bajanowski IV, Lesions in the respiratory
system, Nordisk Rettsmedisin 9 (2003) 67–68.
[49] A. Vege, P. Rasten-Almqvist, H.F. Krous V, Heart lesions, Nordisk
Rettsmedisin 9 (2003) 69–70.
[50] H.T. Aretz, M.E. Billingham, W. Edward, S.M. Factor, J.T. Fallon, J.J.
Fenoglio Jr., E.G. Olsen, F.J. Schoen, Myocarditis: a histopathologic
definition and classification, Am. J. Cardiovasc. Pathol. 1 (1987) 5–14.
[51] A.M. Feldmann, D. McNamara, Myocarditis, N. Engl. J. Med. 343 (2000)
1388–1398.
[52] J.G. Shanes, J. Ghali, M.E. Billingham, V.J. Ferrans, J.J. Fenoglio, W.D.
Edwards, C.C. Tsai, J.E. Sffitz, J. Isner, S. Furner, Interobserver variability
in the pathologic interpretation of endomyocardial biopsy results, Circu-
lation 75 (1987) 401–405.
[53] B. Strauer, R. Kandolf, R.G. Mall, B. Maisch, T. Mertens, H.R. Figulla, S.
Schwartzkopff, M. Brehm, H.P. Schultheiss, Myokarditis—Kardiomyo-
pathie, Med. Klin. 96 (2001) 608–625, Update 2001.
[54] R. Dettmeyer, M. Schlamann, B. Madea, Immunohistochemical techni-
ques improve the diagnosis of myocarditis in cases of suspected sudden
infant death syndrome (SIDS), Forensic Sci. Int. 105 (1999) 83–94.
[55] A. Heusch, U. Kuhl, S. Rammos, O.N. Krogmann, H.P. Schultheiss, M.
Bourgeois, Complete AV-block in two children with immunohistological
proven myocarditis, Eur. J. Pediatr. 155 (1996) 633–636.
[56] R. Wojnicz, E. Nowalany-Kozielska, J. Wodniecki, Immunhistological
diagnosis of myocarditis, Eur. Heart J. 19 (1998) 1564–1572.
[57] T. Ino, M. Kishiro, M. Okubo, K. Akimoto, K. Yabuta, R. Okada, Late,
persistent expressions of ICAM-1 and VCAM-1 on myocardial tissue in

T. Bajanowski et al. / Forensic Science International 165 (2007) 129–143 143
children with lymphocytic myocarditis, Cardiovasc. Res. 34 (1997) 323–
328.
[58] A. Henke, M. Nain, A. Stelzner, D. Gemsa, Induction of cytokine release
from human monocytes by coxsackievirus infection, Eur. Heart J. 12
(Suppl. D) (1991) 134–136.
[59] M. Noutsias, B. Seeberg, H.P. Schultheiss, U. Kuhl, Expression of cell
adhesion molecules in dilated cardiomyopathy. Evidence for endothelial
activation in inflammatory cardiomyopathy, Circulation 99 (1999) 2124–
2131.
[60] E. Thorsby, Structure and function of HLA molecules, Transplant. Proc.
19 (1987) 29–35.
[61] Y. Seko, N. Takahashi, S. Ishiyama, T. Nishikawa, T. Kasajima, M. Hiroe,
S. Suzuki, S. Ishiwata, S. Kawai, M. Azuma, H. Yagita, K. Okumura, Y.
Yazaki, Expression of costimulatory molecules B7-1, B7-2 and CD40 in
the heart of patients with acute myocarditis and dilated cardiomyopathy,
Circulation 97 (1998) 637–639.
[62] W.D. Edwards, D.R. Holmes, G.S. Reeder, Diagnosis of active lympho-
cytic myocarditis by endomyocardial biopsy. Quantitative criteria for light
microscopy, Mayo Clin. Proc. 57 (1982) 419–425.
[63] R. Dettmeyer, A. Baasner, M. Schlamann, S.A. Padosch, C. Haag, R.
Kandolf, B. Madea, Role of virus-induced myocardial affections in sudden
infant death syndrome: a prospective postmortem study, Pediatr. Res. 55
(2004) 947–952.
[64] E. Druyts-Voets, L. van Renterghem, S. Gerniers, Coxsackie B virus
epidemiology and neonatal infection in Belgium, J. Infect. 27 (1993) 311–
316.
[65] H. Shimizu, C. Rambaud, G. Cheron, C. Rouzioux, R. Anuradha, G.
Stanway, H.F. Krous, Burns, Molecular identification of viruses in sudden
infant death associated with myocarditis and pericarditis, Ped. Infect. Dis.
J. 14 (1995) 584–588.
[66] R. Kandolf, K. Klingel, R. Zell, A. Canu, U. Fortmuller, C. Hohenadl, M.
Albrecht, B.Y. Reimann, W.M. Franz, A. Hein, Molecular mechanism in
the pathogenesis of enteroviral heart disease: acute and persistent infec-
tions, Clin. Immuno. Immunopathol. 68 (1993) 153–158.
[67] M. Arnestad, S.H. Opdal, R.W. Byard, A. Vege, J.V. Jørgensen, J. Banner,
T. Bajanowski VI, Metabolic and genetic investigation, Nordisk Rettsme-
disin 9 (2003) 70–71.
[68] P. Gaustad, E. Holter, A. Vege, Bacterial and virological examinations in
cases of sudden unexpected deaths in infancy and early childhood,
Nordisk Rettsmedisin 9 (2003) 72.
[69] M. Arnestad, A. Vege, T.O. Rognum, Evaluation of diagnostic tools
applied in the examination of sudden unexpected deaths in infancy and
early childhood, Forensic Sci. Int. 125 (2002) 262–268.
[70] T. Bajanowski, M. Vennemann, E.A. Mitchell, B. Brinkmann, The GeSID
Group, Unnatural causes of sudden unexpected deaths thought initially to
be SIDS, Int. J. Legal Med. 119 (2005) 213–216.
[71] C. de Lange, A. Stray-Pedersen, A. Borthne, T.O. Rognum, Radiological
investigation of SUDI, Scand. J. Forensic Sci. 10 (2004) 74.
[72] Guidelines for paediatric radiology; skeletal survey for suspected child
abuse. http://www.radiologiforeningen.no/prosedyrer/prosedyrer1-barn/
2004.
[73] M. Bauer, S. Polzin, D. Patzelt, The use of clinical CCT images in the
forensic examination of closed head injuries, J. Clin. Forensic Med. 11
(2004) 65–70.
[74] M.J. Thali, K. Yen, W. Schweitzer, P. Vock, C. Boesch, C. Ozdoba, G.
Schroth, M. Ith, M. Sonnenschein, T. Doernhoefer, E. Scheurer, T.
Plattner, R. Dirnhofer, Virtopsy, a new imaging horizon in forensic
pathology: virtual autopsy by post-mortem multislice computed tomo-
graphy (MSCT) and magnetic resonance imaging (MRI)—a feasibility
study, J. Forensic Sci. 48 (2003) 386–403.
[75] N.I. Langlois, P.S. Ellis, D. Little, B. Hulewicz, Toxicological analysis in
cases of possible sudden infant death syndrome, Am. J. Forensic Med.
Pathol. 23 (2002) 162–166.
[76] L. Bachs, T. Bajanowski, T.O. Rognum, M. Arnestad, Toxicological
investigation of SUDI, Scand. J. Forensic Sci. 10 (2004) 73.
[77] T. Bajanowski, B. Brinkmann, M. Vennemann, The San Diego definition
of SIDS—practical application and comparison with the GeSID classi-
fication, Int. J. Legal. Med. (2006), doi:10.1007/s00414-005-0043-0.
Recommended

















