Embed Size (px)
Citation preview

The 1000-day window of opportunity: Optimal infant and young child feeding (IYCF) practicesBY: DR NWANDO ONUIGBO -CHAT TA
FOR: PRESTON HEALTHCARE CONSULTING LTD.
DATE: 22 ND SEPTEMBER 2017

Outline•Introduction
•Malnutrition
•IYCF
•Breast feeding
•Complementary feeding
•Interventions
•Discuss
•References
Introduction
•Nutrition of pregnant/lactating woman critical to development of child.
•Targeting the 1000 day period is one of the best investments to improve health, nutrition and economic outcomes.
•Nutrition specific interventions will be most impactful when focusing on this window of opportunity.
•A child’s, in fact nation’s future is determined by the quality of nutrition in first 1,000 days.
•Optimal nutrition is critical for cognitive and physical development at this stage.

Introduction cont’d
Why 1000 days?
•1000 days from pregnancy to 2nd birthday = 270+365+365 = 1000.
•Critical window when child’s brain and body are developing rapidly.
•Mothers and babies need good nutrition to lay the right foundation for the child's future cognitive, motor and social skills.
•Good nutrition during pregnancy and infancy has profound impact on a child’s ability to grow and learn.
•Poor nutrition during this window can lead to newborn and child morbidity, mortality, poor fetal growth and stunting.

Introduction cont’dWhy 1000 days?
•Children with restricted development during this window are at risk of neurological problems and poor school achievement.
•Consequently early school drop out, low-skilled employment and poor care of their own children, thus intergenerational transmission of poverty and malnutrition.
•Damage from poor nutrition during this period is often irreversible.
•Preventive efforts should focus on the 1,000 days; therapeutic efforts target severe wasting.

Introduction cont’dKey Facts
•Every infant and child has the right to good nutrition ("Convention on the Rights of the Child“).
•Malnutrition is associated with 45% of children’s deaths.
•171 million (27%) of children stunted; 60 million children (10 %) wasted.
•Underweight and deficiencies linked with 19% and 10% of children’s deaths.
•About 40% of infants 0–6 months old are exclusively breastfed.
•In many countries less than 25% of infants 6–23 months meet criteria of safety, diversity and frequency of diet appropriate for their age.

Malnutrition - Four types1. Stunting:
•Child too short for age.
•Caused by chronic malnutrition
•Generally occurs before age 2.
•Largely irreversible.
•Delayed motor development, impaired cognitive function.

Malnutrition - Four types cont’d2. Wasting:
•A child’s is too thin for their height.
•Caused by acute malnutrition.
3. Underweight:
•Child’s weight is too low for their age.
•Due to stunting, wasting or both.
4. Micronutrient deficiency: •A child lacks essential vitamins or minerals •namely; vitamin A, iron and zinc. •Can be caused by lack of nutrients or worms.

Malnutrition – Malnutrition crisis•Yearly 7.6 million children die before they reach the age of 5, mostly from preventable or treatable illnesses and almost all in developing countries.
•Malnutrition is an underlying cause of about 35% of these deaths.
•A malnourished child is up to 10 times as likely to die from an easily preventable or treatable disease as a well-nourished child.
Malnutrition - Malnutrition crisis cont’d
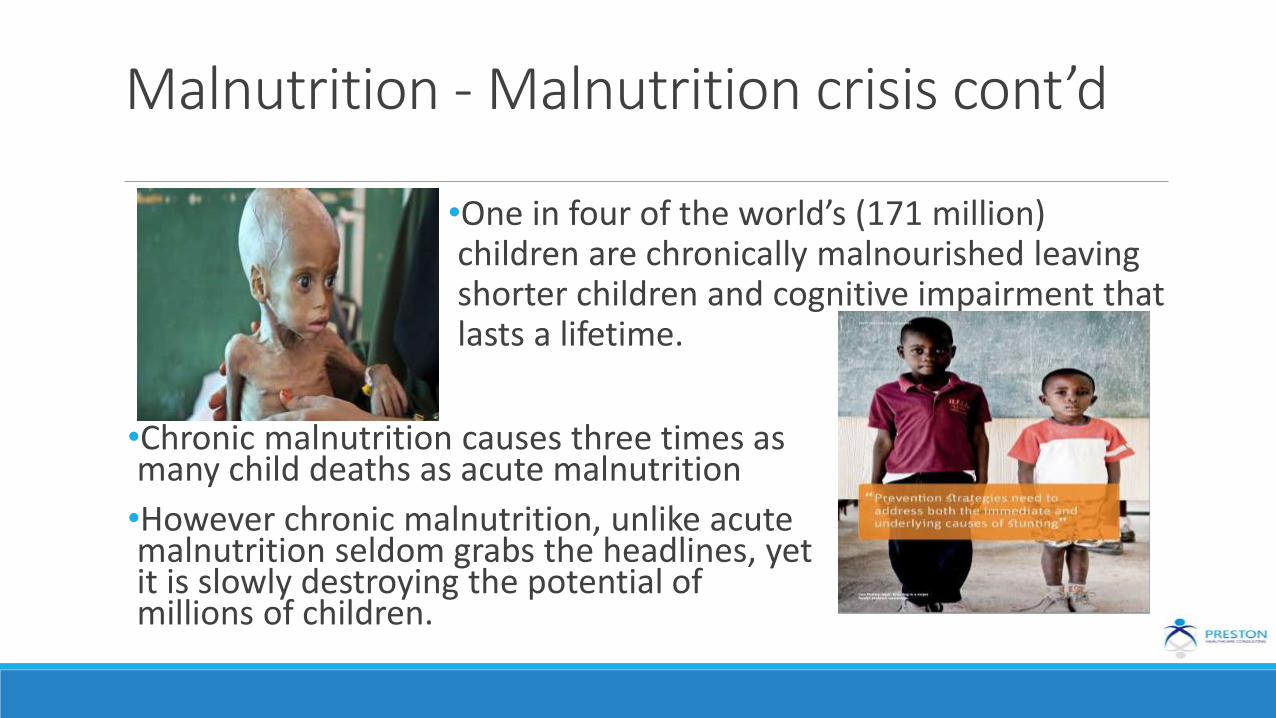
•One in four of the world’s (171 million) children are chronically malnourished leaving shorter children and cognitive impairment that lasts a lifetime.
•Chronic malnutrition causes three times as many child deaths as acute malnutrition
•However chronic malnutrition, unlike acute malnutrition seldom grabs the headlines, yet it is slowly destroying the potential of millions of children.
IYCF - What is IYCF?•Infant and Young Child Feeding (IYCF) is a global strategy for feeding of children.
•Issued by World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) in 2002, to reverse disturbing trends in infant and young child feeding practices.
•Focus world attention on impact feeding practices have on growth, development and health; thus survival of infants and young children.


IYCF - overviewOptimal breastfeeding is so critical that it could save the lives of over 820 000 children under 5 per year.
WHO and UNICEF recommend:
•early initiation of breastfeeding within 1 hour of birth.
•exclusive breastfeeding for the first 6 months of life.
•introduction of nutritional and safe complementary (solid) foods at 6 months plus breastfeeding up to 2 years of age or beyond.

Breastfeeding•Exclusive breastfeeding for 6 months
•Imptnt source of energy; less likely to develop obesity.
•Benefits for the infant: Reduces GI infections/diarrhea and confers immunity.
•Benefits to mother: reduces the risk of ovarian and breast cancer and natural contraception (not fail safe) due to lactation amenorrhoea
Complementary feeding•Breast milk no longer enough, therefore complementary foods added.
•Transition from exclusive breast feeding to family foods is ‘complementary feeding.’
•6 to 24 months and vulnerable period.
•Gradually increase consistency (liquid, puree to mash).•Feed variety of food; at least 3 types daily including animal food (egg, fish, liver, meat).

Complementary Feeding cont’d

Intervention
•About 1/3 of stunting manifested as small for gestational age & preterm babies
•This reflects the importance of targeting women during pregnancy and the pre-pregnancy period.
• An integral part of 1,000 days nutrition programming is to integrate maternal and newborn care as health outcomes for mothers and their newborns/children are inextricably linked

Intervention overviewThe six life saving intervention areas:
•Iron folate during pregnancy
•Breastfeeding
•Complementary feeding
•Vit. A supplementation
•Zinc for treatmnet of diarrhea
•WASH

Intervention

IYCF Strategies1. Breastfeeding Support:
•Adoption of policies like ILO’s "Maternity Protection Convention’’
•Adoption of the "International Code of Marketing of Breast-milk Substitutes" and subsequent relevant World Health Assembly resolutions.
•Implementation of the "Ten Steps to Successful Breastfeeding" specified in the Baby-Friendly Hospital Initiative.
•Provision of supportive health services with IYCF counselling during contacts with caregivers and young children.
•Community support i.e. mother support groups and community-based health promotion and education activities.
IYCF Strategies
•Continue frequent, on-demand breastfeeding until at least 2 years.
•Responsive feeding: Feed infants directly and assist older children. Feed slowly and patiently, encourage but don’t force, talk to child and maintain eye contact.
•Good hygiene and proper food handling.
•Start small amounts of food and increase gradually as child gets older.
2.Complementary feeding: Developmentally ready at 6 months.

IYCF Strategies2. Complementary feeding:
•Gradually increase consistency and variety.
•Increase feeding frequency: 2–3 meals to 3–4 meals per day with 1–2 additional snacks.
•Use fortified complementary foods or vitamin-mineral supplements as needed.
•During illness, increase fluid intake including more breastfeeding, and offer soft, favouritefoods.

IYCF Strategies3. Feeding in exceptionally difficult circumstances: Breastfeeding recommended wherever possible.
•low-birth-weight or premature infants
•mothers living with HIV
•adolescent mothers
• Settings where diarrhoea, pneumonia and malnutrition are prevalent.•infants and young children who are malnourished•families suffering the consequences of complex emergencies.
IYCF Strategies4. HIV and infant feeding
•Breastfeeding (especially early and exclusive) is one of the most significant ways to improve infant survival rates.
•While HIV can pass from a mother to her child through breast-milk, evidence shows antiretroviral treatment (ART) reduces the risk of transmission through breastfeeding.

Recommendations1. Invest in proven, low-cost solutions to save children’s lives and prevent stunting:
•Iron supplements prevents anaemia
•vit A prevents blindness and lowers risk of death from common dzs,
•zinc plus good hygiene can save a child from diarrhea,
•6 months of exclusive breastfeeding.
Although not expensive it’s a tragedy that millions of mothers and children don’t have access.

Recommendations2. Invest in health workers:
•to reach the most vulnerable mothers and children.
•CHWs are critical to save lives and prevent stunting
3. Help more girls go to school and stay in school:
•one of the most effective
•educated women tend to have fewer, healthier and better nourished children.

Recommendations cont’d•education gives girls knowledge, self confidence, skills and hope for bright future.
•It can also delay marriage, child bearing and improve spacing.
4. Increase private sector partnerships to improve nutrition for mothers and children.
5. Improve laws, policies and actions that support families and encourage breastfeeding.
Recommendations cont’d6. Increase government support for proven solutions:
•to meet SDG, lifesaving services must be increased for women and children who need them most.
•Nigeria should commit to and fund national nutrition plans that are integrated with plans for maternal and child health.
•Donors should support these goals by keeping their funding commitments to achieving the SDGs.
•Countries should endorse and support the Scaling Up Nutrition (SUN) movement.
Best Practices1. Promote and support good maternal nutrition during pregnancy and lactation
•Micronutrients iron, folic acid, calcium, iodine and vit. A via supplementation, fortification and food consumption.
•Standards of nutritional care for pre natal and post natal care developed and followed. e.g. optimum weight gain in pregnancy, diagnosis and treatment of anemia, support dietary diversity, etc.
Best Practices cont’d1. Promote and support good maternal nutrition during pregnancy and lactation cont’d
•Education on optimum nutrition for exclusive breast feeding.
•Health provider/community worker continuing education on nutrition.
•Education of fathers/family in providing of good nutrition for pregnant/lactating women.

Best Practices cont’d2. Promote and support optimal IYCF and care practices.
•Immediate initiation of breastfeeding (1 hour) and exclusive breastfeeding for the 6 months.
•Engagement of fathers, family and community influencers on supporting pregnant and lactating mothers.
•Starting at 6 months appropriate complementary feeding (e.g., dietary diversity) plus breastfeeding to 2 years or beyond.
•Adequate feeding of sick children to prevent wasting or stunting.
Best Practices cont’d2. Promote and support optimal IYCF and care practices:
•Integration of IYCF with WASH (safe drinking water, hand-washing with soap, safe disposal of excreta, and food hygiene).
•National programs: supplementation, fortification (ensure adequate intake of essential micronutrients).

Best Practices cont’d3. Focus on the 1,000-day period through health, nutrition, agriculture, and humanitarian assistance programs
•Scale up community management of acute malnutrition in emergency settings.
•Proper IYCF guidance for HIV-infected mothers and exposed infants
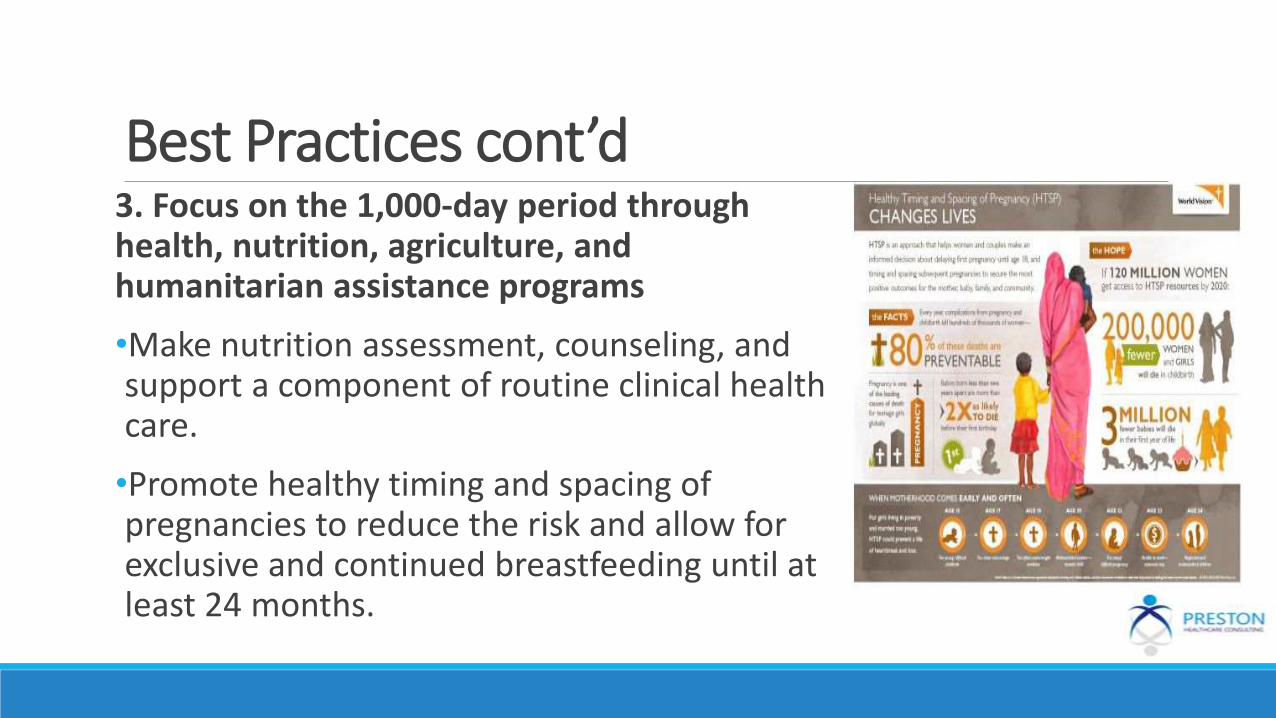
Best Practices cont’d3. Focus on the 1,000-day period through health, nutrition, agriculture, and humanitarian assistance programs
•Make nutrition assessment, counseling, and support a component of routine clinical health care.
•Promote healthy timing and spacing of pregnancies to reduce the risk and allow for exclusive and continued breastfeeding until at least 24 months.

Best Practices cont’d3. Focus on the 1,000-day period through health, nutrition, agriculture, and humanitarian assistance programs cont’d
•Promote dietary diversity for women and children through integrated agriculture and nutrition programming.
•Strengthen evidence base for scale up of proven nutrition-sensitive agriculture interventions.
•Increase professionals and frontline workers, especially women, trained and employed in nutrition to meet country/local needs.

Best Practices cont’d4. Social and behavior change communication: Messaging reinforced by community mobilization and mass media should include:
Interpersonal counseling•Nutrition-specific services for
mothers/caregivers and their families.
•Home visits, peer support, “mothers groups,” and counseling by health workers.
Best Practices cont’d4. Social and behavior change:
Multiple media channels• Informal means (community theater
and songs), videos, posters, and leaflets.
• Targeted mass media (community radio), mass media (television and social media), cell phones, and other technology.
Community mobilization and advocacy

DiscussAdults who were malnourished as children can earn an estimated 20 percent less on average than those who weren’t. (SC, 2012)
•Can malnutrition cause/transmit poverty? Explain.
Referenceshttps://www.usaid.gov/what-we-do/global-health/nutrition/1000-day-window-opportunity
Nutrition in the First 1,000 Days State of the World’s Mothers 2012
http://www.who.int/mediacentre/factsheets/fs342/en/






























