Embed Size (px)
Citation preview

Chap
ter
71Ross I. Silver, MD, andBeverly G. Coleman, MD
Obstetric UltrasOUnd:secOnd-trimester imaging
1. What are the components of the basic (level 1) second-trimester ultrasound (US) examination?The components of a basic second-trimester US examination include:
• Documentation of the fetal heart rate• Number and lie of fetuses• Estimation of the amniotic fluid volume• Location and appearance of the placenta and its relationship to the internal os• Gestational age• Evaluation of the uterus and adnexa• Assessment of fetal anatomic characteristics, including cerebral ventricles, four-chamber heart, spine, stomach, urinary
bladder, umbilical cord, and kidneys
2. How is the normal amniotic fluid volume estimated?To calculate the amniotic fluid index (AFI), the anteroposterior diameters of the largest empty fluid pocket (no umbilical cord or fetal parts) in each quadrant are added together. The AFI is normally 7 to 25 cm. In addition, each individual pocket of fluid should be 2 to 8 cm. Fluctuations outside of this range define oligohydramnios (too little amniotic fluid) or polyhydramnios (too much amniotic fluid).
Key Points: Components of a Basic Second-Trimester Ultrasound Examination
1. Documentation of fetal heart rate and number and lie of fetuses2. Estimation of amniotic fluid volume3. Location and appearance of the placenta and its relationship to the internal os4. Gestational age5. Evaluation of the uterus and adnexa6. Fetal anatomic characteristics
3. What are the major causes of polyhydramnios?One third of cases of polyhydramnios are idiopathic and not associated with other anomalies. Two thirds of cases are associated with maternal problems, fetal problems, or both. These include gestational diabetes, multiple gestations, structural abnormalities of the fetus that impair swallowing of amniotic fluid (obstruction of the upper gastrointestinal tract, chest narrowing or masses, and severe central nervous system abnormalities), and fetal hydrops.
4. What is the dreaded complication of oligohydramnios?The lungs need an adequate supply of amniotic fluid for proper development. Oligohydramnios leads to pulmonary hypoplasia, which, depending on the severity, can be a major cause of fetal morbidity and mortality.
5. If the placenta appears to be covering the internal os, what entity may be present?This is called placenta previa, which occurs in 1 in 200 to 400 deliveries, more commonly after a previous cesarean section. If the placenta extends to the edge of the internal os, a marginal previa is present. If the placenta partially covers the os, this is called a partial previa, and if it completely covers the internal os, a complete previa is present. A fourth type, a central previa, occurs when a complete previa is centrally located over the internal os. Placenta previa can lead to maternal hemorrhage secondary to premature detachment of the placenta. It can also be a cause of premature delivery and perinatal mortality (Fig. 71-1).
6. A pregnant woman presents with vaginal bleeding, pelvic pain, and tenderness over the uterus. What entity must be considered?This is a common presentation of placental abruption, a serious condition that can cause morbidity in the fetus and, less commonly, in the mother. Risk factors include maternal hypertension, collagen vascular disease, and abdominal trauma.
503

504 Obstetric ultrasOund: secOnd-trimester imaging
Figure 71-2. Sagittal transvaginal US image shows the “hourglass” deformity of an incompetent cervix (arrow).
Figure 71-3. Transabdominal US image shows a normal three-vessel cord with single umbilical vein (arrow) and two umbilical arteries (arrowheads).
Figure 71-1. Sagittal transvaginal US image shows complete placenta previa. The placenta completely covers the internal os (arrow).
US can detect placental abruption by showing blood behind a placenta that has separated from the uterine wall. Blood has a variable US appearance, depending on the age of the bleed, that ranges from hypoechoic or completely anechoic in the acute and chronic phases to hyperechoic and heterogeneous in the subacute phase.
7. What is an “hourglass” deformity of the cervix?An “hourglass” deformity is a severe form of incompetent cervix that occurs when the internal cervical os is open, and the endocervical canal is dilated to the external os. Clinically, the amniotic membranes bulge into the vagina. Spontaneous pregnancy loss usually cannot be avoided (Fig. 71-2).
8. Can the presence of a single umbilical artery be normal?Yes. Normal umbilical cords most commonly have three vessels (two arteries and one vein). A two-vessel cord does not imply fetal abnormality. In single gestations, approximately 50% of two-vessel cords (one artery and one vein) have no associated abnormalities. In multiple gestations, a two-vessel cord is a more common normal variant. Of the abnormalities that may exist with a two-vessel cord, fetal structural abnormalities and growth retardation are the most common. The posterior fossa, face, extremities, and heart should be thoroughly evaluated in pregnancies with a single umbilical artery (Fig. 71-3).
9. What is the most accurate measurement to assess gestational age in the second trimester?The biparietal diameter (BPD) is accurate from approximately 5 to 7 days up to 24 weeks. It is measured in the transverse plane from the outer edge of the closer temporoparietal bone to the inner edge of the farther temporoparietal bone. The thalamus should be visualized when measuring the BPD. The head circumference is as accurate as the BPD and is measured at the same level. The femur length is as accurate as the BPD after 26 weeks (Fig. 71-4A).
10. How is the abdominal circumference obtained, and why is it used?The abdominal circumference is measured in the transverse plane at the fetal liver, with the umbilical portion of the left portal vein in the center of the abdomen. The abdominal circumference is not as accurate as the BPD and femur length for estimating gestational age. Instead, it is commonly used to determine proportionality with the head. A head-to-abdominal circumference ratio is used for this purpose. Normally, the head is larger than the body in the second and early third trimesters, with a reversal of this ratio at term (Fig. 71-4B).

Obstetric ultrasOund: secOnd-trimester imaging 505ultrasOnOgraphy
A B
Figure 71-4. Measurements of normal gestational age. A, BPD (plus sign) and thalami (arrows). B, Abdominal circumference (plus sign), portal vein (long arrow), stomach (short arrow), and aorta (arrowhead ).
Figure 71-5. Transabdominal US image shows normal four-chamber view of the heart. Apex of the heart (arrow).
11. What is the difference between symmetric and asymmetric intrauterine growth retardation (IUGR)?Asymmetric IUGR constitutes 90% of cases and is due to diminished blood supply and nourishment to the fetus. The abdominal circumference is disproportionately affected compared with the head and femur. It is usually diagnosed in the third trimester. Symmetric IUGR is usually diagnosed in the first or early second trimester and is due to decreased cellular growth, usually secondary to an insult to the mother or fetus early in the pregnancy. The head and body are equally affected in symmetric IUGR.
12. What percentage of cardiac anomalies can be detected by the four-chamber view alone?Approximately 70% of cardiac anomalies can be detected with the four-chamber view, including abnormalities of cardiac position
(situs inversus), septal abnormalities (ventricular septal defect), and masses (rhabdomyomas). The percentage of detected anomalies can be increased to 80% with the addition of a short-axis view of the great vessels at the base of the heart, a view of the right ventricular outflow tract, and a long-axis view of the left ventricular outflow tract (Fig. 71-5).13. Describe the classic US features of fetal hydrops.Whether the cause is immune or nonimmune, the appearance of fetal hydrops is the same: fluid in the serous cavities, including ascites; pleural and pericardial effusions; skin thickening; placental enlargement; and polyhydramnios. Not all of these features may be present in any one case, however. In addition, hepatomegaly may be seen, particularly with immune hydrops.
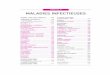
14. What is the most common intrathoracic/extracardiac fetal anomaly?Congenital diaphragmatic hernia (CDH) occurs in 1 of every 2000 to 3000 live births. Of these, 90% are Bochdalek hernias, which are posterolateral in location. The remaining 10% are Morgagni hernias, which occur in an anteromedial location. With a Bochdalek hernia, US shows the normal stomach bubble located in the chest, and the heart is displaced upward and to the right. The presence of peristaltic, fluid-filled bowel loops in the chest is diagnostic. The spleen and left lobe of the liver may also be present in the thorax. Morgagni hernias are more subtle and difficult to diagnose (Fig. 71-6).
506 Obstetric ultrasOund: secOnd-trimester imaging
Figure 71-6. Transabdominal US image shows congenital diaphragmatic hernia. The heart (long arrow), stomach (short arrow), and liver (arrowhead ) are in the thorax.
15. Name the four types of anterior abdominal wall defects. Which are most common?• Omphalocele• Gastroschisis• Pentalogy of Cantrell• Limb–body wall complex
Omphalocele and gastroschisis are the most common, occurring in 1 in 4000 live births (omphalocele) and 1 in 10,000 live births (gastroschisis). The latter two are extremely rare and are associated with a very poor prognosis.
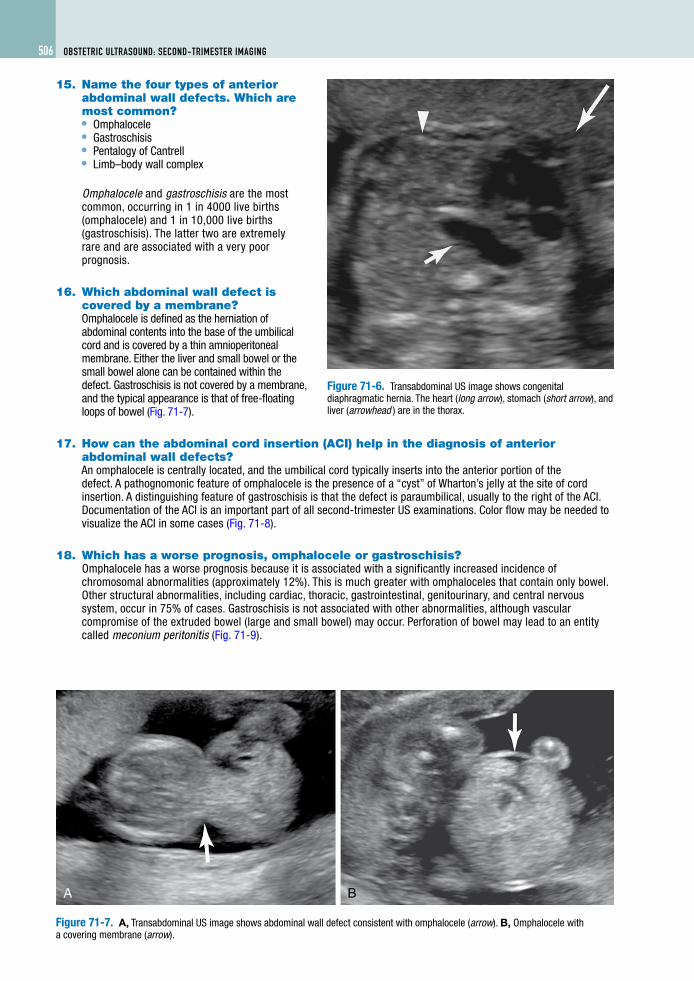
16. Which abdominal wall defect is covered by a membrane?Omphalocele is defined as the herniation of abdominal contents into the base of the umbilical cord and is covered by a thin amnioperitoneal membrane. Either the liver and small bowel or the small bowel alone can be contained within the defect. Gastroschisis is not covered by a membrane, and the typical appearance is that of free-floating loops of bowel (Fig. 71-7).
17. How can the abdominal cord insertion (ACI) help in the diagnosis of anterior abdominal wall defects?An omphalocele is centrally located, and the umbilical cord typically inserts into the anterior portion of the defect. A pathognomonic feature of omphalocele is the presence of a “cyst” of Wharton’s jelly at the site of cord insertion. A distinguishing feature of gastroschisis is that the defect is paraumbilical, usually to the right of the ACI. Documentation of the ACI is an important part of all second-trimester US examinations. Color flow may be needed to visualize the ACI in some cases (Fig. 71-8).
18. Which has a worse prognosis, omphalocele or gastroschisis?Omphalocele has a worse prognosis because it is associated with a significantly increased incidence of chromosomal abnormalities (approximately 12%). This is much greater with omphaloceles that contain only bowel. Other structural abnormalities, including cardiac, thoracic, gastrointestinal, genitourinary, and central nervous system, occur in 75% of cases. Gastroschisis is not associated with other abnormalities, although vascular compromise of the extruded bowel (large and small bowel) may occur. Perforation of bowel may lead to an entity called meconium peritonitis (Fig. 71-9).
A B
Figure 71-7. A, Transabdominal US image shows abdominal wall defect consistent with omphalocele (arrow). B, Omphalocele with a covering membrane (arrow).

Obstetric ultrasOund: secOnd-trimester imaging 507ultrasOnOgraphy
Figure 71-8. Transabdominal US image shows normal ACI (arrow).
Figure 71-9. Transabdominal US image shows gastroschisis. Free floating bowel loops are seen (arrow). Doppler flow shows umbilical cord inserting to the side of the defect (arrowhead ).
19. Why might the urinary bladder not be visualized?The bladder should be identified by 16 weeks. Nonvisualization of the urinary bladder is not abnormal, however. Because of the normal cycling of the bladder, rescanning after initial nonvisualization every 15 to 20 minutes for 1 hour is recommended. If the bladder is still not present, an abnormality likely exists, such as impairment of renal function from an intrinsic renal abnormality or upper urinary tract obstruction. Generalized growth retardation can also lead to functional renal impairment. In bladder exstrophy, typically there is an infraumbilical wall defect with nonvisualization of the urinary bladder.
20. A markedly distended bladder and ureters with bilateral hydronephrosis are visualized during a routine second-trimester US of a male fetus. What abnormality may be present?This is the classic US appearance of a severe, prolonged lower urinary tract obstruction. In a male fetus, this is most commonly caused by posterior urethral valves. In female fetuses, this is likely a result of urethral atresia. Cases of severe lower urinary tract obstruction are usually fatal because of marked oligohydramnios and the pulmonary hypoplasia that results (Fig. 71-10).
21. Name the four patterns of limb shortening seen with skeletal dysplasias.Skeletal dysplasias can be differentiated by determining which portion of the limb is affected. A micromelic pattern of shortening affects the proximal and the distal limbs. If only the proximal segment is shortened, a rhizomelic type of dysplasia is present. Less common patterns of dysplasia include the mesomelic pattern, in which only the forearm and foreleg are shortened, and
A B
Figure 71-10. A, Transabdominal US image shows normal bladder (arrow). B, Lower urinary tract obstruction with distended bladder (arrow) and ureters (arrowheads).

508 Obstetric ultrasOund: secOnd-trimester imaging
the acromelic pattern, in which only the distal segment is shortened. The most common type of skeletal dysplasia, heterozygous achondroplastic dysplasia, is characterized by a rhizomelic pattern of shortening.
22. What would produce an enlarged cisterna magna on US?A Dandy-Walker malformation causes an enlarged cisterna magna. From the inside of the occiput to the back of the cerebellar vermis, the cisterna magna normally measures 2 to 10 mm. Dandy-Walker malformations are caused by dysgenesis (Dandy-Walker variant) or agenesis of the cerebellar vermis and are associated with midline central nervous system abnormalities, including lateral and third ventricle hydrocephalus, encephalocele, and agenesis of the corpus callosum. Additional abnormalities of the body, including cardiac and renal abnormalities, may be found (Fig. 71-11).
23. What is the significance of the nuchal skin?Directly posterior to the occiput is a thin rim of soft tissue that normally measures 6 mm or less in the second trimester. An increased nuchal skin thickness greater than 6 mm is concerning for Down syndrome. The sensitivity of this finding is 50%, and the false-positive rate is less than 1%.
24. Which open neural tube defect contains elements of spinal cord?A myelomeningocele contains spinal cord elements; myelo is the Latin prefix referring to the spine. The herniation of meninges alone through an open neural tube defect is known simply as a meningocele. On US, these defects usually appear as a cystic structure projecting through splayed posterior elements, most commonly in the lumbosacral region. If the cyst is completely anechoic, a meningocele is likely present. Hyperechoic strands representing neural elements within the cystic projection indicate that the likely diagnosis is myelomeningocele (Fig. 71-12).
A B
Figure 71-11. A, Transabdominal US image shows normal posterior fossa. Cross hairs measure the cerebellum (plus sign) and cisterna magna (x). B, Dandy-Walker malformation with absent vermis (arrow) and enlarged cisterna magna (arrowhead ).
A B
Figure 71-12. A, Transverse transabdominal US view of myelomeningocele. The posterior elements are splayed (arrows ). B, Sagittal view of spine shows a low-lying, tethered spinal cord (arrow) and cystic mass arising from the spine (arrowhead ).

Obstetric ultrasOund: secOnd-trimester imaging 509ultrasOnOgraphy
25. When an open neural tube defect is discovered, what else should be evaluated?The fetal head should be thoroughly evaluated whenever an open neural tube defect is discovered. These defects are almost always associated with Arnold-Chiari type II malformations, in which the cerebellar hemispheres herniate downward through the foramen magnum. Two US signs are associated with this malformation: the “banana” sign and the “lemon” sign. With the “banana” sign, the cerebellum is shaped like a downward-curved C, and with the “lemon” sign, the bilateral frontoparietal bones are flattened. Both signs are sensitive and specific for open neural tube defects; the “banana” sign is seen in more than 90% of cases, and the “lemon” sign is present in approximately 98% of cases.
BiBliography
[1] W.E. Brant, Ultrasound: The Core Curriculum, Lippincott Williams & Wilkins, Philadelphia, 2001.[2] P.W. Callen, Ultrasonography in Obstetrics and Gynecology, third ed., Saunders, Philadelphia, 1994.[3] A.B. Kurtz, W.D. Middleton, Ultrasound: The Requisites, Mosby, St. Louis, 1996.