Embed Size (px)
Citation preview

Residents Preparedness Level Against Ebola Virus Disease Resurgence
iBabatunde Olowookere 910706002
RESIDENTS PREPAREDNESS LEVEL AGAINST EBOLA VIRUS DISEASE RESURGENNCE: A SURVEY IN THREE LOCAL GOVERNMENT AREAS IN LAGOS STATE
SUBMITTED BY
OLOWOOKERE BABATUNDE ABIODUN
MATRIC NO: 910706002
SUBMITTED TO
THEDEPARTMENT OF COMMUNITY HEALTH AND PRIMARY HEALTH CARE, COLLEGE OF MEDICINE,
UNIVERSITY OF LAGOS
IN PARTIAL FULFILLMENT OF THE REQUIREMENT FOR THE AWARD OF (MSc) DEGREE IN PUBLIC HEALTH
(GENERAL OPTION)
SEPTEMBER 2015

Residents Preparedness Level Against Ebola Virus Disease Resurgence
DECLARATION
I Babatunde Abiodun Olowookere hereby declares that this project titled: Residents
Preparedness Level against Ebola Virus Disease Resurgence: a survey in three local
Government Areas in Lagos State was carried out by me under the supervision of Dr.
Robert A.A. I also declare that it has not been submitted either in part or in full for any other
examination.
NAME SIGNATURE
Babatunde Abiodun Olowookere
I BabatundeAbiodunOlowookerehereby declare that this project titled: A Survey of
Household on Community Mobilization for Ebola Virus Disease in three Local
Government Areas in Lagos State was carried out by me under the supervision of Dr.
Robert A.A. I also declare that it has not been submitted either in part or in full for any other
examination.
NAME
Babatunde Abiodun Olowookere
SIGNATURE
iiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
DATE
iiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
DEDICATION
To Almighty God, for his grace and tremendous love.
To my wife for her love and support.
To our beloved son Jesse. Jese
ivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
CERTIFICATION
CERTIFICATION
I certify that the research project titled Residents Preparedness Level against Ebola Virus
Disease Resurgence: a survey in three local Government Areas in Lagos State was carried out
by Babatunde Abiodun Olowookere under my supervision.
…………………... ………………….……….. ………………………………DR. A. A. ROBERTS DATESupervisor
……………………………………………… ………………………………… BABATUNDE ABIODUN OLOWOOKERE DATEStudent
vBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
……………………………………………… ……………………………… DR. OGUNNOWO DATE
Assessor DATEI certify that the research project Titled Residents Preparedness Level against Ebola Virus Disease Resurgence: A Survey in Three Local Government Areas in Lagos Statewas carried out byBabatundeAbiodunOlowookere under my supervision. The project work is adequate in scope and qualify for partial fulfillment of the requirement for the award of masters of Science Degree in Public Health.
Babatunde Abiodun Olowookere
viBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
ACKNOWLEDGEMENT
I wish to acknowledge the grace of the Almighty God upon my life from the time I was born
till this day; I give all the praise and honour to his holy name.
I wish to thank the past and present postgraduate co-coordinators, Dr Alero Roberts and Dr
Abiola for their assiduous efforts to ensure a smooth running of the MPH session. I am
indebted to my supervisor Dr. A.A Alero for heris calmness, maturity and mentors hip during
the study period despite heris busy schedule.
To my wife, Mrs. Hauwa Olowookere, I wish to say a big thank you for your support and
encouragement throughthroughout the academic year, may the Almighty God continue to
guide and protect you. To my adorable son, Jesse Olowookere, thank you for being sweet and
supportive during this period. To all my friends and colleagues, I thank you all.
I cannot but give thanks to all my colleagues at the National Emergency Management
Agency (NEMA), South West Zonal office particularly the Zonal Coordinator, Dr. Bemdele
Onimode for his support and advice during the course of the program.
Finally, I am extremely grateful to all those who participated in the study for their
willingness, time, commitment and sincere responses. I cannot end my acknowledgment
without appreciating Micheal Agoro an Industrial Attachment student with NEMA Zonal
office and also David Oyedepo an NYSC Corp member serving at the zonal office for their
assistance during the data gathering for the study.
viiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
TABLE OF CONTENTSTITLE PAGE………………………………………………………………………………… ................i
DECLARATION................................................................................................................................... ii
DEDICATION...................................................................................................................................... iii
CERTIFICATION................................................................................................................................ iv
ACKNOWLEDGEMENT.....................................................................................................................v
TABLE OF CONTENTS......................................................................................................................vi
LIST OF TABLES...............................................................................................................................vii
LIST OF FIGURES....................................................................................................................... ixixviii
ABBREVIATIONS.............................................................................................................................. ix
SUMMARY...........................................................................................................................................x
CHAPTER ONE................................................................................................................................211
BACKGROUND TO THE STUDY..................................................................................................211
CHAPTER TWO...............................................................................................................................756
LITERATURE REVIEW..................................................................................................................756
CHAPTER THREE.....................................................................................................................312330
MATERIALS AND METHODOLOGY.........................................................................................3123
CHAPTER FOUR...........................................................................................................................3930
RESULTS........................................................................................................................................3930
DISCUSSION.................................................................................................................................5853
CONCLUSION...............................................................................................................................6155
RECOMMENDATIONS.................................................................................................................6256
REFERENCES................................................................................................................................6357
viiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
LIST OF TABLES
Table 1: Respondents used in the study……………………………………………………… 36
Table 2: Socio-demographic characteristics of respondents…………………………………..
39
Table 3: Socio -economic characteristics of respondents………………………………………. 40
Table 4: Knowledge score of respondents on causes of Ebola disease………………………..…..
41
Table 5: Table 4: Knowledge on the spread of Ebola Viral Disease…………………………………….
….. 42
Table 6:Table 5: Knowledge on when signs of illness of Ebola Viral Disease begins by
respondents (n=390)…………………………………………………………………… 44……
…
Table 7: Level of preparedness against Ebola Viral Disease resurgence………………………. 46
Table 8: Knowledge score of respondents on EVD across all domains………………………….. 48
Table 9: Association between Socio-demographic characteristics of respondents and their
Knowledge of EVD (n=390)…………………………………………………………… 49
Table 10: Association between Socio-economic characteristics of respondents and knowledge
of EVD…………..………………………………………………………………. 50
Table 11: Association between Socio-economic characteristics of respondents and their
Attitude and perception of EVD of EVD…………..………………………… 51
Table 12: Association between Socio-demographic characteristics of respondents and their
Attitude and perception regarding of EVD …………………………………………… 52
Table 13: Association between Socio-demographic characteristics of respondents
and their Level of Preparedness against of EVD resurgence…………………………. 53
Table 14: Association between Socio-economic characteristics of respondents
and their Attitude and perception regarding of EVD………………………….. 54
Table 15: Association between Socio-demographic characteristics of respondents and
practices regarding EVD………………………………………………………….. 55
Table 16: Association between Socio-economic characteristics of respondents and
practices regarding EVD resurgence…………………………………………… 56
ixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 6: Knowledge on drug /remedy to treat Ebola Viral Disease……………………………
Table 7: Knowledge on how to prevent contracting Ebola Viral Disease……………………..
Table 8: Attitude and perception regarding Ebola Viral Disease………………………………
Table 9: Attitude and perception regarding Ebola Viral Disease……………………………..
Table 10: Level of preparedness against Ebola Viral Disease resurgence……………………..
Table 11: Practices regarding Ebola Viral Disease…………………………………………….
Table 12: Knowledge score of respondents on EVD across all
domains………………………
Table 14: Association between Socio-demographic characteristics of
respondents and their Knowledge of EVD (n=416)
……………………………………………………………………
Table 13: Association between Socio-economic characteristics of
respondents
and their Knowledge of EVD (n=390) their Attitude and perception of
EVD (n=416)………..
Table 14: Association between Socio-demographic characteristics of
respondents and their Attitude and perception of EVD (n=390)
……………………………………………………….
Table 15: Association between Socio-economic characteristics of
respondents
and their Attitude and perception regarding of
EVD…………………………………………
xBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 16: Association between Socio-demographic characteristics of
respondents
and their Level of Preparedness against of EVD
resurgence………………………………….
Table 17: Association between Socio-economic characteristics of
respondents
and their level of preparedness EVD
resurgence……………………………………………..
Table 18: Association between Socio-demographic characteristics of
respondents
and practices regarding EVD
…………………………………………………………………
Table 19: Association between Socio-economic characteristics of
respondents
and practices regarding EVD
resurgence……………………………………………………..
xiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
LIST OF FIGURES
Figure 21: Knowledge of Signs and Symptoms of Ebola Viral Disease
mentioned by respondents (n=390)……………………………………………. 3543
Figure 32: Knowledge on sources and channels of information regarding EVD (n=390)... 4539
Figure 31: Overview of Ebola virus pathogenesis………………………………………. 1471
Figure 2: Knowledge of Signs and Symptoms of Ebola Viral Disease
mentioned by respondents (n=390)……………………………………………. 35
Figure 3: Knowledge on sources and channels of information regarding EVD (n=390)... 39
xiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
LIST OF TABLES
Table 1: Socio-demographic characteristics of respondents ..............25
Table 1: Socio-demographic characteristics of respondents
Table 2: Socioeconomic characteristics of respondents
Table 4: Knowledge score of respondents on causes of Ebola
disease
Table 5: Knowledge on the spread of Ebola Viral Disease
Table 6: Knowledge on when signs of illness of Ebola Viral
Disease begins by
Respondents (n=390)
Table 7: Knowledge on drug /remedy to treat Ebola Viral Disease
xiiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
LIST OF FIGURES
xivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
ABBREVIATIONS
CDC Center for Disease Control and Prevention
DRC Democratic Republic of Congo
ECOWAS Economic Community of West Africa State
EEOC Ebola Emergency Operation Center
EID Emerging infectious Disease
ELISA Enzyme-Linked Immunosorbent Assay
EVD Ebola Virus Disease
HF Health Facility
KAP Knowledge, Attitudes, and Practices
LGAs Local Government Areas
GOARN The Global Alert and Response Network
NHP Non-Human Primate
Ig Immuno-globulin
MCP Macrophage Chemotactic protein
NO
PCR
PHCC
Nitric Oxide
Polymerase Chain Reaction
Primary Health Care Centre
PHE
PPE
TF
VHF
UNICEF
Public Health Event
Personal Protective Equipment
Tissue Factor
Viral Hemorrhagic Fever
United Nations Children’s Fund
WHO World Health Organization
xvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
xviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
SUMMARY
Ebola is one of the most virulent human viral diseases with a case fatality ratio between 25%
to 90%. The West African outbreaks in 2014 are the largest and worst in history. The first
ever outbreak of Ebola virus disease (EVD) in Nigeria was declared in July, 2014 but Nigeria
and Liberia were however declared EVD free on 20th October 2014 and 9th May 2015 after no
new cases were reported within the period. A new confirmed case was however reported in
Liberia on Monday 29th June 2015. This latest resurgence of EVD in Liberia is an indication
of how difficult it is for Public Health authorities to eliminate a highly contagious viral
disease and its implications in Nigeria.
The objectives of the study are to determine knowledge, attitude, level of preparedness and
practices of hygiene amongst residents in Ikeja, Agege and Mushin Local Government Areas
of Lagos State.
The survey which assessed the preparedness level against Ebola Virus Disease resurgence in
three (3) Local Government Areas in Lagos State namely Ikeja, Agege and Mushin was
conducted among 416 residents. Selection was focused on Lagos State due to the fact that it
was once hit by an epidemic.
The study was a descriptive, community-based cross-sectional survey and 309 identified
residents were successfully surveyed, with a rate of 93.98%. Among the identified, we had
57.1% men, 48.1% women and majority of the respondents were Christians.
It was noticed that 6.02% have never heard about EDV, 6.2% possessed satisfactory
knowledge in all three domains. Fifteen percent, 24.5%, 2.9% and 13.1% possessed
satisfactory knowledge in signs and symptoms, preventive measures, mode of spread and
level of preparedness. Radio was the most used source of information. Majority (82.3%) of xvii
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
the respondents mentioned regular hand washing with soap and water, while 55.6% said they
regularly used hand sanitizers.
It was discovered from the study that there was high level of preparedness amongst the
studied population against a re-emergence of EVD. Nonetheless, participating in burial rites
of a person that dies of Ebola disease remains a major key knowledge gap. For Nigeria, the
best protective measures are adequate levels of preparedness focused on knowledge, attitude
perception and practices preventing a further spread of the disease.
Ebola is one of the most virulent human viral diseases with a case fatality ratio between 25%
to 90%. The West African outbreaks in 2014 are the largest and worst in history. The first
ever outbreak of Ebola virus disease (EVD) in Nigeria was declared in July, 2014 although
Nigeria and Liberia were declared EVD free on 20th October 2014 and 9th May 2015 after no
new cases were reported within the period.
A new confirmed case was however reported in Liberia on Monday 29 th June 2015. This
latest resurgence of EVD in Liberia is an indication of how difficult it is for Public Health
authorities to eliminate a highly contagious viral disease and its implication in Nigeria.
The survey assessed the preparedness level against Ebola Virus Disease resurgence in three
(3) Local Government Areas in Lagos State was conducted among 416 residents. Selection
was focused on Lagos State due to the fact that it was once hit by an epidemic. From the
identified residents, 309 were successfully surveyed, with a rate of 93.98%. Among the
identified, we had 57.1% men, 48.1% women and majority of the respondents were
Christians.
It was noticed that 6.02% have never heard about EDV, 6.2% possessed satisfactory
knowledge in all three domains. Fifteen percent, 24.5%, 2.9% and 13.1% possessed
xviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
satisfactory knowledge in signs and symptoms, preventive measures, mode of spread and
level of preparedness. Radio was the most used source of information. Majority (82.3%) of
the respondents mentioned regular hand washing with soap and water, while 55.6% said they
regularly used hand sanitizers.
The study highlights that there was high level of preparedness of the studied population
against re-emergence of EVD. For Nigeria, the best protective measures are adequate levels
of preparedness that focus on knowledge, attitude and perception and practices regarding
EVD to avoid further spread.
xixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
CHAPTER ONEINTRODUCTION
BACKGROUND TO THE STUDY
Ebola Virus Disease (EVD) (Formally known as Ebola haemorrhagic fever) is an active
haemorrhagic illness with a case fatality (death) rate of up to 90%. The disease is caused by
filoviridae family that affects humans and non-human primates (monkey, gorilla and
chimpanzee).1
The World Health Organization (WHO) defines Ebola Virus Disease as a severe often fatal
illness in humans. EVD is transmitted from wild animals and then spread within the human
population through human to human transmission.2
Ebola viral fever, a highly contagious haemorrhagic disease has today become a major public
health concern particularly in developing world.3The first Ebolavirus specie was discovered
in the year 1976 in what has now become the Democratic Republic of Congo near the Ebola
River. The epidemic recorded 318 cases and 280 deaths for a case fatality of 88%.Since then
24 more outbreaks have occurred in multiple African countries.4 The disease in Sudan also
known as Sudan Ebola Virus (SEBOV) has caused six further epidemics in man and while
that of Zaire strain known as (EBOV) has caused 17 further epidemics.5
the World Health Organization (WHO) has reported over 11,306 casualties with an estimated
28,256 people confirmed or suspected of having contracted the disease in nine countries as at
xxBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
September 3rd 2015. A total of 869 confirmed healthcare workers infected with EVD and 507
confirmed dead.6 Majority of these cases occurred in West African Countries of Guinea,
Sierra Leone and Liberia. While Nigeria, Senegal, the USA, Spain, Mail, the United
Kingdom and Italy reported imported cases or import-related local transmission linked to the
epidemic in West Africa.
The recent resurgence of the disease in Liberia which has earlier been certified EVD free
with Nigeria by the World Health Organization is a cause for concern for all.7
NATURE OF THE PROBLEM
The first outbreak of the epidemic in the West African sub region was in 2014 and since then,
curbing the spread of the EVD has been a challenge. The fear that the disease could spread
further is palpable due to the situation in Liberia. The outbreak is also still very active in
Sierra Leone and Guinea.
The greatest mystery regarding the causative organism of EVD is the identity of its natural
reservoir and the mode of transmission from the reservoir to wild animals and man.8 In
addition, EVD present signs and symptoms of that Lassa fever or viral hemorrhagic fever
which is highly prevalent in West Africa; that can also cause delay diagnosis.
THE EXTENT OF THE PROBLEM
The current outbreak in West Africa was first reported in March 2014. It is the largest and
most complex Ebola outbreak since the Ebola virus was discovered in 1976.9 There have
been more cases and deaths in this epidemic than all others combined. It has also spread
between countries starting from Guinea and spreading across land borders to Sierra Leone xxi
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
and Liberia by air (1 traveller) to Nigeria and USA (1 traveller) and by land Senegal (1
traveller) and Mali (2 travellers).10
The West Africa outbreak is so large, so severe and so difficult to contain. The hardest-hit
countries are Guinea, Liberia and Sierra Leone.11 These countries are amongst the poorest in
the world. Both Sierra Leone (1991-2002) and Liberia (1989-2003) have only recently
emerged from protracted conflicts and Civil wars. The Ebola Virus Disease (EVD) epidemic
in West Africa has ravaged the social fabrics of three (3) countries (Guinea, Liberia and
Sierra Leone) with a death toll of over 11 263 people and over 27 642 cases as at July 15,
2015.
In August 2014 WHO declared it a Public Health Emergency of International Concern.
Travel-associated cases have now been documented in five (5) additional countries and
effects are being felt worldwide.12EVD is highly contagious in nature and can be easily
spread if not properly managed; in addition, the fact that the cure for the disease has not been
discovered and no vaccine to inoculate affected victims remains a major concern.
THE SIGNIFICANCE OF THE PROBLEM
The world Health Organization (WHO) declared Nigeria and Liberia Ebola Virus Disease
(EVD) free on 20th October 2014 and 9thMay 2015 after no new cases were
reported.13However, a new confirmed case was reported on Monday 29thJune 2015 in Liberia.
This latest resurgence of EVD in Liberia is an indication of how difficult it is for Public
Health authorities to eliminate a highly contagious viral disease.
xxiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Nigeria is the most occupied country in Africa with an estimated population of about 180
million. It is also the world’s fourth largest oil producer and second largest supplier of natural
gas.14Lagos-State is the commercial nerve center of Nigeria. The State attracts travelers from
all over the world particularly people from other West African countries that are still battling
with the scourge of EVD. This portends danger if proper prevention and control measures are
not sustained to enhance the spread of the disease.
THE JUSTIFICATION AND RATIONALE FOR STUDY
Nigeria containment of Ebola Virus Disease (EVD) has been lauded as nothing short of
remarkable given both the population density in the country and particularly in cities such as
Lagos and Port Harcourt. The outbreak of the disease created public fear, panic and confusion
as is usually seen in outbreaks of previously unknown diseases or epidemics such as malaria,
poliomyelitisetc which are yet to be totally contained in the country. Nonetheless, there is the
need to continuously have a preventive behavior to reduce community transmission to human
by emerging infectious diseases (EIDs).
The trends in globalization including expansion in international travel and trade have also
extended the reach and increased the pace at which infectious diseases spread. Between the
periods of 1996-2009, research shows that 53% of the global EID outbreaks occurred in
Africa.15
As a nation, there is an urgent need to assess our readiness to manage and contain the EVD.
Periodic research through surveys of assessment of the level of preparedness of residents in
three (3) Local Government Areas in Lagos State against EVD Resurgence will further
enhance our response capability and reduce the burden on the health infrastructure caused by
the fatal epidemics.
xxiiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
AIM
The study is to assess the level of preparedness of residents in Ikeja, Agege and Mushin
Local Government Areas of Lagos State against EVD Resurgence.
OBJECTIVES
To achieve this aim the specific objectives are:
1. To determine the level of knowledge of EVD amongst the residents in Ikeja, Agege
and Mushin Local Government Areas of Lagos State.
2. To determine the attitude of residents in Ikeja, Agege and Mushin Local Government
Area of Lagos State on EVD.
[3.] To determine the level of preparedness and practices of hygiene amongstramongst
residents in Ikeja, Agege and Mushin Local Government Areas of Lagos State.
xxivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
xxvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
CHAPTER TWOLITERATURE REVIEW
DEFINITIONS AND BACKGROUND
Ebola Virus Disease (EVD):
EVD can be defined as a severe form of viral haemorrhagic fever or fatal zoonotic infection
caused by a virus of the filoviridae family and designated Ebola Haemorrhagic Fever
(EHF).16
Public Health Event (PHE):
A public health event is defined as any occurrence that may have negative consequences for
human health including those that have not yet caused disease or illness but that have
potential and those that may require a coordinated response.17
Public Health Preparedness:
These are actions taken by Healthcare and Public Health organizations to ascertain effective
response to emergencies that impact health especially events that have timing or scale that
overwhelms normal capacity.18
Individual Preparedness:
Action taken by an individual or family to prevent, protect against and minimize physical and
emotional damage that results from a disaster.18 18Preparedness is a fundamental concept in the
field of Disaster Research and Emergency Management. It is a measure taken prior to the
onset of a disaster to enhance the response capacity.
xxviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
It also implies the ability of social units to accurately assess a hazard, realistically anticipate
likely problems in the event of an actual disaster and appropriately taken precautionary
measures to mitigate impacts and ensure an efficient and effective response.
Knowledge Attitude and Practice:
Knowledge: is defined as “the fact or condition of knowing something with a considerable
degree of familiarity through experience, association or contact’’.19
Three forms of knowledge are identified: explicit, tacit and implicit.
Explicit knowledge is that which is stated in detail and is termed as codified or formal
knowledge.20
Explicit knowledge can be accessed by anyone, for example, books, pictures, or recording
clips.
Tacit knowledge represents knowledge based on the experience of individuals, expressed in
human actions in the form of evaluation, attitudes, points of view, commitments and
motivation. Tacit knowledge is lost with the person who possesses it.21
Implicit knowledge is that which could be expressed, but has not been. In other words
implicit knowledge is that body of knowledge which exists without being stated.19 19
Attitude: Iis a predisposition or tendency to respond positively or negatively towards a
certain idea, object, person or situation. Attitude is un-expressed behavior. It influences an
individual’s choice of action.
Practice: Iis the utilization of rules and knowledge that leads to action. Good practice shares
a corresponding relationship with knowledge and technology.
xxviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
The union of Knowledge, Attitude, and Practice in a common action like the KAP study is an
educational diagnosis of community or subgroup of a community. It evaluates specific
understanding, feelings and actions regarding any matter of interest.
Ebola Resurgence:
Resurgence is bringing again into activity and prominence. Ebola resurgence is therefore the
re-emergence of new cases of Ebola Virus Disease in a place where it has been declared
Ebola-free.
Emergency:
A sudden occurrence that may be due to epidemics, natural, man-induced to technological
catastrophes that demands immediate action.22
Resident:
Someone who lives in a particular place for a prolonged period or who was born there.
EBOLA VIRUS DISEASE - AN OVERVIEW
Ebola Virus Disease (EVD) is caused by Ebola Virus responsible for viral hemorrhagic fever
like Lassa fever (LASV), Yellow fever (YFV), Marburge fever and Dengue fever. Ebola
viruses are the causative agents of a severe form of viral haemorrhagic fever in man,
xxviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
designated Ebola Haemorrhagic Fever (EHF) and are endemic in regions of Central Africa.
They are called hemorrhagic because of the distinct scary bleeding that occurs during the
course of the illness. Nonetheless, the word hemorrhagic is now left out in the case of Ebola
because not all of Ebola patients developed significant hemorrhage symptoms, which usually
occurs only in the terminal phase of fatal illness.23
EVD is one of the most fatal viral diseases worldwide affecting human and non-human
primates. Ebola was first discovered in 1976 near the Ebola River in what is now called the
Democratic Republic of the Congo (DRC).The virus has the potential to spread globally and
is classified as a “category A” pathogen that could be misused as a bioterrorism agent.24
CLASSIFICATION OF EBOLA VIRUS
Ebola virus is a non-segmented, negative-sense highly infectious illness caused by a single-
stranded RNA virus similar to rhabdoviruses and paramyxoviruses in its genome organization
and replication mechanism.
Ebola Virus is amongst the most virulent pathogens that have been shown to cause disease in
humans and nonhuman, and has fast become one of the world’s most feared pathogen. Ebola
Virus alongside causative organisms of Rift valley fever, Crimean Congo hemorrhagic fever,
lassa fever, yellow fever and Dengue hemorrhagic fever are also classified as hemorrhagic
fever virus are all classified as hemorrhagic fever viruses.
xxixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Currently, there are five (5) genetically distinct members of thefiloviridae family (filovirus),
this includes: Zaire Ebolavirus (EBOV), BundibugyoEbolavirus (BDBV), Reston Ebolavirus
(RESTV), Sudan Ebolavirus (SUDV) and Tai Forest Ebolavirus (TAFV) all named after the
country or location where virus was first isolated.
Although, Reston ebolavirus has only caused disease in non-human primates (NHP) and was
found in swine suffering from porcine reproductive and respiratory disease syndrome in the
Philippines and in People’s Republic of Chain.25Zaire, Sudan and Bundibugyo Ebola viruses
are largely responsible for most of the Ebolahaemorrhagic Fever outbreaks in Africa.26The
fifth species, Tai forest ebolavirus was documented in a single human infection caused by
contact with an infected chimpanzee from the Tai forest in Ivory Coast. In sub-saharan Africa
the Zaire ebolavirus constitutes a particularly serious threat to both human and non-human
primates.
The Zaire species which has been identified as the most commonly occurring species in
previous outbreaks is the cause of the number of cases and deaths between 1976 and 2012.
The fatality percentage represents the percentage of people who die after contracting the virus
and Zaire has the highest at 69%, followed by the second most virulent species Sudan at
53%.27The Ebola outbreak (Zaire species) of 2014 has become larger than all previous Ebola
outbreaks combined since its discovery in 1976. Epidemic has occurred in the Sudan,
Democratic Republic of Congo, Gabon, Uganda and Congo.28
EPIDEMIOLOGY OF EBOLA VIRUS DISEASE
xxxBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Two main modes of transmission into human populations have been suggested: either direct
contact to a reservoir or contact to other wildlife that also contracts EBOV from the
reservoir.29
The filoviruses Marburg and Ebola cause fulminant hemorrhagic fever were first recognized
in 1967 when the inadvertent importation of infected monkeys from Uganda resulted in
explosive outbreaks of severe illness among vaccine plant workers in Marburg, Germany and
Belgrade, Yugoslavia.30 Ever since, except in few instances of accidental laboratory
infections reported, all large outbreaks of filoviral disease have been confined to Sub-
Saharan Africa.31
The first recognized outbreaks in Africa occurred in Zaire and Sudan in 1976.Each outbreak
had over 300 people affected but did not spread greatly because of the location of the place.
The Zaire species caused several hundred cases in 1995 in Kikwit, Democratic Republic of
Congo and the Sudan virus infected more than 400 people in Gulu, Uganda in 2000.32
The 2013-2015 Ebola epidemic is the largest outbreak of Ebola virus ever recorded. It was
caused by the Zaire species of the virus. It is not only the first to occur in West Africa but the
effect far outweighs other previous outbreaks. The West African country of Guinea was
where the first case was first confirmed in December 2013 and it spread to Liberia and Sierra
Leone in 2014.33Subsequently, the cases of EVD outbreaks spread to Nigeria, Senegal and
Mail with isolated case in United Kingdom and another in Sardinia. There were also reported
imported cases in the United States and Spain which led to secondary infections of medical
workers but did not spread further.
Aside of causing human infections, Ebola virus has also spread to wild non-human primates
(NHPs). Fruit bats are considered to be the natural reservoir for Ebola virus in Africa. 34 This
xxxiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
has contributed to a marked reduction in chimpanzee and gorilla populations in Central
Africa and has also triggered some human epidemics due to handling of and/or consumption
of sick or dead animals by local villagers as a source of food.
TRANSMISSION OF EBOLA VIRUS DISEASE
Ebola virus can be transmitted by direct contact with blood, bodily fluid or skin of EVD
patient or individuals who have died of the disease.35As soon as a person becomes infected,
the disease is spread to others through broken skin, mucous membranes, blood or body fluids.
Transmission via inanimate objects contaminated with infected bodily fluid (fomites) is
possible.36The principal mode of transmission in human outbreaks is human-to-human
transmission through direct contact with a symptomatic or dead EVD case or with
contaminated surfaces and materials (e.g. beddings, clothing’s etc.).
Prior to the epidemic in West Africa in 2014, outbreaks of EVD were typically controlled
within a period of weeks to a few months. This is as a result that most outbreaks occurred in
remote regions with low population density, where residents rarely travelled. However, the
epidemic in West Africa has shown that Ebola virus can spread rapidly and widely as a result
of the extensive movement of infected individuals (including undetected travel across
national borders), the spread of the disease to urban areas and the avoidance and/or lack of
adequate Personal Protective Equipment and Medical Isolation Center. Human Ebola
outbreaks usually occur abruptly from a vaguely defined source with subsequent rapid spread
from person to person.
Human-to-human: Human-to-human transmission is through direct or close contact with
infected patients and particularly through contact with blood and body fluids of an infected
patients or bodies of patients who die of the disease. EVD Ebola can also be transmitted in
postmortem care settings by laceration and puncture with contaminated instruments used
xxxiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
during postmortem care, through direct handling of human remains without recommended
PPE and through splashes of blood or other body fluids such as urine, saliva, feces, or vomit
to unprotected mucosa such as eyes, nose or mouth during postmortem care.37
Risk of transmission through bodily Fluids: Ebola virus can also be transmitted through
direct contact with bodily fluids. It remains one of the highest risks of contacting of the virus
between people. Circumstantial evidence from previous outbreaks, epidemiological data and
experiments in non-human primates all demonstrate that contact with ebola virus infected
fluid scan lead to infection. Contact with bodily fluids has also been implicated as the reason
why caregivers often become infected after contact with patients. In a study of the risk factors
associated with contracting Ebola virus during an outbreak in Kikwit, Sudan contact with
bodily fluids strongly predicted risk of infection as did sharing hospital beds.38
Risk of transmission through the airborne/aerosol route: Currently no data exists whether
Ebola virus disease can be spread from human-human by respiratory tract route. However,
epidemiological data have led to the understanding that the disease does not undergo
traditional airborne transmission. Although aerosolized filo viruses are highly infectious for
laboratory animals, in humans, airborne transmission has only been reported among
healthcare workers who were exposed during aerosol generating medical procedures.39
Ebola virus can also be spread through fomites and environmental Stability: A fomite
refers to any surface that a pathogen is able to persist on, and fomite transmission can occur
when an individual comes into contact with that infected surface. Potential routes of Ebola
virus fomite transmission include touching objects such as beddings, clothing and other
personal utensils (plates, cups) that have been in contact with person who is sick of Ebola
virus. Little is known about the stability of Ebola virus on surfaces as limited environmental
testing in outbreak locations has shown little evidence for Ebola virus persistence on surfaces. xxxiii
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
However, one experiment showed that EBOV viral load is reduced by 4 log10 after 5.9 days
when placed on glass and in the dark at 24°C and 40% relative humidity. Another experiment
showed that EBOV could be recovered after 50 days, when dried in culture media on glass at
4 °C.40
Nosocomial transmission: Nosocomial infections are infections that develop as a result of a
stay in hospital or are produced by microorganisms and viruses acquired during
hospitalization. Transmission to healthcare workers due to lack of resources for infection
control and Personal Protective Equipment (PPE) are the main reasons for nosocomial
transmission. Nosocomial transmission has been a major cause of morbidity and mortality in
EVD since the first outbreaks described in Sudan and Zaire (now Democratic Republic of the
Congo, DRC) in 1976. The current outbreak in West Africa had led to documented infection
in 876 health workers with 509 deaths as July 12, 2015.41
Essentially, there is no evidence on mosquitoes or other biting arthropods transmitting filo
viruses. Past epidemic may have been much and more difficult to control if the virus were
transmitted from person to person by these mechanisms.42,43
Due to the high mortality rate of the Ebola virus in human and non-human primate, it is
considered highly dangerous and is a bio-terrorism agent that could jeopardize global health.
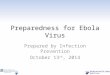
PATHOGENESIS OF EBOLA VIRUS DISEASE
Little is known about the pathogenesis of filovirus infection. Almost all data on the
pathogenesis of Ebola virus disease have been obtained from laboratory experiments
employing mice, guinea pigs and non-human primates. Ebola virus disease can enter the host
body mostly via mucosal surfaces or injuries in the skin.44Also infection through the
xxxivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Iintact skin cannot be excluded, although it is considered unlikely. Aerosol infection
(RESTV) has been demonstrated in non-human primates under experimental conditions in
dispersion chambers.45,46
However, case reports and large-scale observational studies of patients in the 2014-2015
West African outbreaks are providing urgently needed data on the pathogenesis of the disease
in humans.47
Cell entry and tissue damage: — once the virus enters the body through mucous
membranes, it attacks the immune cell of the host namely macrophages and dendritic cells
are probably the first to be infected. The immune cell gets fooled and release large amounts
of cytokines that instead facilitate the entry of the virus into endothelial cells easily.
The virus genetic material (single-stranded RNA) is released into cytoplasm and produces a
new viral proteins/genetic material. The viral genomes migrate to regional lymph nodes
results in further rounds of replication, followed by spread through the bloodstream to
dendritic cells and fixed and mobile macrophages in the liver, spleen, thymus, and other
lymphoid tissues. Necropsies of infected animals have shown that many cell types (except for
lymphocytes and neurons) may be infected, including endothelial cells, fibroblasts,
hepatocytes, adrenal cortical cells and epithelial cells. Fatal infection is characterized by
multifocal necrosis in tissues such as the liver and spleen.
Gastrointestinal dysfunction: — Patients with Ebola virus disease commonly suffer from
vomiting and diarrhoea which can result in acute volume depletion, hypotension and shock.48
It is not clear if such dysfunction in Ebola virus disease is the result of viral infection of the
gastrointestinal tract or if it is induced by circulating cytokines or both.
xxxvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Systemic inflammatory response: — Ebola virus also induces a systemic inflammatory
syndrome by inducing the release of cytokines, chemokines and other pro-inflammatory
mediators from macrophages and other cells.49
Infected macrophages produce tumor necrosis factor (TNF)-alpha, interleukin (IL)-1beta, IL-
6, macrophage chemotactic protein (MCP)-1 and nitric oxide (NO).50 These disruption
products of necrotic cells also stimulate the release of the same mediators. This systemic
inflammatory response is thought to play a role in inducing gastrointestinal dysfunction as
well as diffuse vascular leak and multi-organ failure that is seen later in the disease.
Coagulation defects: — The coagulation defects seen in Ebola virus disease appear to be
induced indirectly through the host inflammatory response. Virus-infected macrophages
synthesize cell-surface tissue factor (TF), triggering the extrinsic coagulation pathway; pro-
inflammatory cytokines also induce macrophages to produce TF.51 The simultaneous
occurrence of these two stimuli helps to explain the rapid development and severity of the
coagulopathy in Ebola virus infection.
Additional factors may also play a role in the coagulation defects that are seen with Ebola
virus disease. As examples, blood samples from Ebola-infected monkeys contain D-dimers
within 24 hours after virus challenge and D-dimers are also present in the plasma of humans
with Ebola virus disease.52In Ebola virus-infected macaques, activated protein C is decreased
on day two but the platelet count does not begin to fall until day three or four after virus
challenge, suggesting that activated platelets are adhering to endothelial cells. As the disease
progresses, hepatic injury may also cause a decline in plasma levels of certain coagulation
factors.
xxxviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Impairment of adaptive immunity: — Failure of adaptive immunity through impaired
dendritic cell function and lymphocyte apoptosis helps to explain how filoviruses are able to
cause a severe, frequently fatal illness.53
Ebola virus acts both directly and indirectly to disable antigen-specific immune responses.
Dendritic cells, which have primary responsibility for the initiation of adaptive immune
responses, are a major site of filoviral replication. In vitro, studies show that infected cells fail
to undergo maturation and are unable to present antigens to naive lymphocytes, potentially
explaining why patients dying from Ebola virus disease may not develop antibodies to the
virus.54,55
Adaptive immunity is also impaired by the loss of lymphocytes that accompanies lethal Ebola
virus infection.56Although these cells appear to remain uninfected they undergo "bystander"
apoptosis, presumably induced by inflammatory mediators and/or the loss of support signals
from dendritic cells. A similar phenomenon is observed in septic shock. However, one study
has shown that at least in Ebola-infected mice, virus-specific lymphocyte proliferation still
occurs despite the surrounding massive apoptosis, but it arrives too late to prevent a fatal
outcome.57 Discovering ways to accelerate and strengthen such responses may prove to be a
fruitful area of research.
xxxviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Figure 1: Overview of Ebola virus pathogenesis
SIGNS AND SYMPTOMS OF EBOLA VIRUS DISEASE
EVD begins to affect infected individuals with a non-specific flu-like symptom. The
incubation period from the time of infection with the virus and onset of signs and symptoms
may appear from about2 to 21 days after exposure (average incubation period is eight (8) to
(ten) 10 days). The signs and symptoms are characterized by sudden onset of fever, headache,
intense weakness, nausea, muscle pain and sore throat.
The symptoms are then followed by vomiting, diarrhea, rash, impaired liver and kidney
function and internal and external bleeding (in some cases). Due to the extensive amount of
bleeding, most patients die of hypovolemic shock and/or systematic organ failure within 2 to
xxxviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
21 days of contracting Ebola virus. Death usually occurs as a result of shock due to body
fluid loss rather than blood loss. However, some patients do defervesce after about 14 days
and are able to survive the virus.58
DIAGNOSIS, TREATMENT AND VACCINE FOR EBOLA VIRUS DISEASE
In considering the diagnosis of Ebola Virus Disease, some of the more common diseases
should not be overlooked (e.g.malaria, cholera, meningitis, hepatitis). A definitive diagnosis
of EVD is confirmed through laboratory testing. No vaccine is available and there is no
specific treatment for EVD. Severely ill patients require intensive supportive care and are
usually dehydrated and at risk for other infectious diseases.
Within a few days after symptoms develop and it has been confirm that it is EVD, test such
as enzyme-linked immunosorbent assay (ELISA), polymerase chain reaction (PCR) and virus
isolation can provide definitive diagnosis. Later in the disease or if the patient recovers, IgM
and IgG antibodies against the infecting Ebola strain can be detected. . Similarly, studies
using immunohistochemistry testing, PCR, and virus isolation in deceased patients are also
done usually for epidemiological purposes.48
There is no yet approved vaccine or medicine (antiviral drug) available for treatment of Ebola
virus disease. According to Centres for Diseases Control and Prevention, standard treatment
for Ebola hemorrhagic fever is still limited to supportive therapy. Supportive therapy is
balancing the patient's body fluid and electrolytes, maintaining their oxygen status and blood
pressure, and treating such patients for any complicating infections.59
xxxixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
INFECTIOUS PREVENTION AND CONTROL MEASURES FOR EBOLA VIRUS
DISEASE
Preventive interventions include the following:-
Avoid handling bush meat (wild animals hunted for sustenance) and contact with bats
(which may be the primary reservoir of Ebola virus). This can reduce the risk of initial
introduction of Ebola virus into humans. Appropriate protective clothing’s, thorough
cooking of animal products before consumption is also very necessary.
Meticulous infection control in health care settings. The greatest risk of transmission is
not from patients with diagnosed infection but from delayed detection and isolation.
Since the early symptoms of EVD — fever, nausea, vomiting, diarrhea and weakness
are nonspecific. Patients may expose family caregivers, health care workers and other
patients before the infection is diagnosed.
Community engagement is vital key to successful control of EVD spread. Educating and
supporting the community to practice save burial of persons who may have died from
EVD.
Reduce direct or close contact with people with Ebola symptoms particularly with
bodily fluids of the infected. Gloves and appropriate Personal Protective Equipment
(PPE) should be worn when taking care of ill patients at home. Regular hand washing is
required after visiting patients in hospitals as well as after taking care of patients at
homes.
GLOBAL TRENDS ON EBOLA VIRUS DISEASE OUTBREAKSxl
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
The 2014 West African Ebola crisis represents the largest global outbreak of a high mortality,
non-vaccine preventable contagious illness in recent history. While the outbreak has been
largely confined to Liberia, Guinea and Sierra Leone, its effects have been felt throughout
Africa and the entire world. Thousands of West Africans have succumbed to Ebola as the
outbreak has extended into densely populated areas and crossed international borders.
The ability of EVD to spread rapidly across several West African states within the short time
of the onset of the disease is a cause of concern. The virus now threatens to undermine the
security and economic prospects of the entire region. Till date, the World Health
Organization (WHO) has reported over 11,306 casualties with an estimated 28,256 people
confirmed or suspected of having contracted the disease in nine countries as at September 3rd
2015. A total of 869 confirmed healthcare workers infected with EVD and 507 confirmed
dead.60
Previous outbreaks of Ebola Virus Disease (EVD) have predominantly occurred in Central
African rainforest. Until the outbreaks of 2014 in West Africa, all known previous outbreaks
originated in Democratic Republic of Congo (than Zaire) or country sharing its border. Since
1976, 26 outbreaks of Ebola virus cases have occurred in ten(10) countries of Africa,
including Democratic Republic of Congo (DRC), Sudan, Gabon, Cote d’Ivoire, South Africa,
Uganda, Congo, Guinea, Sierra Leone and Liberia; one imported case in Nigeria, Senegal
Spain and United States of America.3
Till date DRC is the country with the highest number of outbreaks with (7) outbreaks
followed by Uganda (5), Sudan (3) and (3) in Gabon. The unprecedented magnitude and
geographic extent of the Ebola virus Disease has overwhelmed the local response capacity,
posing as extreme challenge for the whole world.29
xliBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
An outbreak outside Africa was the Reston subtype of Ebola virus; first identified in 1989 in
the United States of America, through monkeys housed in a quarantine facility in Reston,
Virginia. At least four humans became infected but none became ill. Additional outbreaks of
the Reston subtype occurred between 1989 and 1996 in Texas, Pennsylvania and Italy. No
humans suffered illness in any of these cases. The source of all the Reston subtype outbreaks
was late traced to a single facility in the Philippines that exported the monkeys.61
On 13th March 2014, the Guinean Ministry of Health issued an alert concerning an
unidentified disease. World Health Organization (WHO) announced its involvement that
same day thinking that the outbreak was Lassa fever or viral hemorrhagic fever which is
highly prevalent in West Africa. After laboratory tests, it was confirmed that the hemorrhagic
fever outbreak was caused by the Ebola virus.62
The first victim of this outbreak was an 18-month-old boy from an area close to where
Guinea shares a border with northern Liberia. The child died on 28 thDecember,
2013.Guineashares borders with Liberia and Sierra Leone, other factor is the socio cultural
ties amongst these countries make it easy for the virus to spread quickly. Within days of the
WHO announcement of the EVD outbreak in Guinea, both Liberia and Sierra Leone had
announced EVD cases outbreaks.63
On April 1, 2014, Guinea reported 24 confirmed cases of EVD. Liberia had 2 confirmed
cases to report and Sierra Leone was monitoring 2 probable cases of EVD infection. By late
April 2014, Guinea had reported 208 “clinical cases” of EVD and 136 deaths. Efforts to
identify those who had come into contact with individuals suffering from the illness led
medical authorities to place 217 others in Guinea under medical observation.64
xliiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
According to World Health Organization, Liberia had 34 probable cases of EVD with 6
confirmed cases and 6 deaths at the time. Liberia had 162 total contacts to trace, 59 of whom
had completed the 21-day follow-up period and were no longer under medical observation.
Sierra Leone reported its first EVD case on 25thMay 2014.By the end of May 2014, WHO
reported that Sierra Leone had 50 clinical cases of EVD and 6 deaths spread across 5 distinct
geographical regions. Guinea had 291 clinical cases of EVD with 193 deaths spread across
seven regions.65
On 17thJune 2014, the Liberian government announced that Ebola was present in its capital,
Monrovia. Later that month, health authorities reported a total of 618 EVD cases and 357
EVD deaths. Infection and fatality statistics as at 30thJuly 2014 indicated that the total number
of cases of EVD had reached 1,440 with 826 deaths. By the end of month, the Government of
Liberia had quarantined communities most at risk and put troops in place to enforce the
quarantine.66
On 2ndAugust2014, an American doctor who had been working as a missionary physician in
Liberia was flown to Atlanta, Georgia, for treatment after contracting EVD. A second
American, a missionary nurse with EVD was flown to Atlanta from Liberia for treatment 3
days later. On 8thAugust 2014, the World Health Organization (WHO) declared that EVD
represent a “Public Health Emergency of International Concern” (PHEIC) and urged the
international community to take action to stop the spread.67
A Spanish priest who had been working in Monrovia, Liberia, contracted EVD and was
flown to Spain for treatment where he died on 12thAugust 2014. On August 2014, a British
healthcare provider was also flown back to the United Kingdom after reportedly contracting
EVD in Sierra Leone.
xliiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Mali reported its first confirmed Ebola case on October 23, 2014 when a two-year-old girl
admitted to a hospital in Mali on 22nd October 2014 died on 24th October 2014. No secondary
infections linked to this case. There was also a case of an Imam from Guinea that was
admitted to hospital for renal failure in a hospital in Mali that subsequently died. Diagnosis
not made until after one of his caregivers became ill and after thousands attended his funeral
7 additional cases and 5 deaths were linked to this case.
Following a heightened sense of panic, tightened restrictions on travel and trade have begun
to take a toll on the economies of the countries affected. Tourism and export revenues have
been hit hard while multinational companies have threatened to halt their operations in the
region. There is no doubt that the epidemic is becoming a global pandemic with potential to
continue to spread beyond the West African stronghold further.
The wider risks and implications of the epidemic are becoming more evident in endemic
region as entire communities are placed in quarantine and frontiers closed. Riots have erupted
in certain areas where the infected – and those with whom they have had contact – have
simply been confined without proper medical attention or even food and water. Furthermore,
border closures and travel bans are largely ineffective (or even counterproductive) given the
region’s porous land frontiers.
Global responses and the current collective mood is one of crisis management, efforts to
improve local healthcare capacities in Liberia, Sierra Leone and Guinea. The Centers for
Disease Control and Prevention (CDC), its leading public institution for infectious diseases
(with over 15,000 employees and a yearly budget of $11.3 billion), has sent a rotating team of
70 experts to assist West Africa and gather any information which could assist in the
effective diagnosis and further understanding. The experimental treatment ZMapp (already
used for Ebola patients with a varying degree of success) is made by the American firm Mapp
xlivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Biopharmaceutical, a company with which the US Department of Health has signed a $25
million contract.
The international community’s response to Ebola particularly African institutions such as the
Economic Community of West African States (ECOWAS) and the African Union (AU) have
expressed their support for the fight against Ebola, their resources are scarce and local leaders
seek primarily to protect their own countries.
The success of containment is therefore in large part contingent on the ability of international
actors to act fast – and in concert – so as to ensure that the spread of Ebola is effectively
halted and that the disease is ultimately vanquished.
THE OUTBREAK OF EBOLA VIRUS DISEASE IN 2014 IN NIGERIA
An acutely ill traveller from Liberia arrived Lagos by air on 20 th July 2014 via Lome, Togo,
and Accra, Ghana. He was hospitalized immediately at the First Consultant Hospital,
Obalende; blood specimen examined at Lagos University Teaching Hospital (LUTH)
indicated the presence of acute Ebola virus infection. On arrival at the airport the index case
had contacts with 15 airport staff and 44 persons at the hospital. The index case died 5 days
later.68
Prior to the current outbreak, Nigeria has not had an occurrence of the disease hence the
scenario created public fear, panic and confusion, as is usually seen in outbreaks of
previously unknowndunknown diseases.69 Consequent upon the above, the Federal Ministry
of Health and the Nigerian Centers for Disease control (FMOH/NCDC) in collaboration with
the Lagos State Ministry of Health and partner Agencies established an Ebola Emergency
Operations Centre (EEOC), the use of an Incident Management System (IMS) and all public
health assets available to the Federal and Lagos State government were used to contained the
spread of the disease.
xlvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
On the 20th of October 2014, the WHO declared Nigeria free of EVD. This was after 42 days
with no new case of EVD and now considered free of Ebola transmission. Modern-day
mobility is a widely recognized conduit for the rapid spread of highly contagious diseases as
demonstrated by one particular case in Senegal which involved several actors from the same
family spread across the region. In Nigeria, a cluster of Ebola cases were sparked by a
traveller from Liberia.
The fundamental controls for all infectious outbreaks are based on enhanced hand-hygiene,
cough and sneezing etiquette, social distancing, sick-contact isolation and environmental
cleaning. Appropriate messaging, supplies and signage are often the best preventative
strategies to mitigate infectious diseases.
We all live in a global community; strategic plans assert a human outbreak anywhere means
risk everywhere. With the recent EVD resurgence in Liberia and Sierra Leone, Nigeria must
note relent in strengthening her preparedness and readiness against the reemergence of EVD.
PUBLIC HEALTH EMERGENCY PREPAREDNESS AGAINST EBOLA VIRUS
DISEASE
The World Health Organization (WHO) declared on August 8 th, 2014 that EVD “Public
Health Emergency of International Concern” and urges the international community to take
action to stop the spread.62EVD is an active haemorrhagic illness with 90% case fatality rate, is
currently an epidemic in some countries in West Africa; although the WHO had declared
Nigeria and Liberia free of Ebola its reemergence in Liberia on May 9 th, 2015 make it a
public health concerns.
xlviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Based on the anticipated risks for the resurgence of Ebola to Nigeria, the WHO organization
recommends that all high risk and medium risk countries strengthen their respective country
preparedness and readiness to EVD.70
Public health emergency preparedness and response efforts seek to prevent epidemics and the
spread of disease, protect against environmental hazards, prevent injuries, promote healthy
behaviors, and assure the quality and accessibility of health services. Each of these is
expected by the public and each is evident in effective preparedness and response related to
public health emergencies. Together they make preparedness and response a special and
particularly critical component of modern public health practice.
Public health emergencies, preparedness and response are inextricably linked.71 Preparedness
is based on lessons learned from both actual and simulated response situations. Effective
response and containment of a potential outbreak of EVD in any country can only be
achieved through anticipation, preparedness and readiness for response in the event of an
outbreak.
With proper preparedness and readiness at country level, Ebola can easily be contained, and
the consequential possible impact on health care systems and the society at large can be
minimized. Against this background, the WHO overarching objectives for the Ebola response
roadmap includes strengthening preparedness of all countries to rapidly detect and respond to
the potential introduction of Ebola in States currently not affected by the outbreak and in
response to the on-going outbreak in West Africa.72
This study tends to assess the level of preparedness of residents in Agege, Ikeja and Mushin
Local Government Areas of Lagos State against EVD Resurgence. Ebola outbreak is a health
related event or disaster, that could come in various forms and may seem to be increasing in
xlviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
frequency, scale and complexity. As a result, households, organizations, and residents must
continue to devise effective means for protecting themselves against those threats.
In discussing and thinking about preparedness, several important points should be kept in
mind. First, preparedness can be viewed and measured at different levels of analysis. At one
extreme, for instance, individuals and households can take protective measures such as
engaging in good hygienic behavior like watching hands with soap and water, using hand
sanitizer and avoiding contact with a person who is sick of Ebola disease etc.
At another extreme, as part of support to Member States, and within the context accounting to
the context of the International Health Regulations (IHR 2005).73 Countries can provide
capacity-building for public health events.
Preparedness is a matter of degree, ranging from low to high and very over time and across
locations with some households engaging in few or no preparedness activities and others
undertaking as many precautionary measures as possible.
At the household and organization levels of analysis, researchers typically use checklists to
measure disaster preparedness, asking respondents to indicate which activities they have
undertaken.74
KNOWLEDGE, ATTITUDE AND PRACTICES (KAP) ON EBOLA
VIRUS DISEASE STUDIES IN AFRICA AND BEYOND Literature review was conducted based on the study’s specific objectives. The information
gathered was used to have a broader view on the public knowledge, attitude and practices on
Ebola Viral Infection. However, there was paucity of information on EVD preparedness level
before the recent outbreak in Liberia.
xlviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Within the continent, EVD outbreaks have been confined to Central and East Africa until the
2014 outbreak in West Africa (WA). Since EVD was discovered in Africa in 1979, about
twenty six (26) outbreaks have occurred.75
Studies on Knowledge of Ebola Viral Disease
In September 2014, Saheed Gidado Abisola, M. Oladimeji,Alero Ann Roberts et al carrired
out a study on Public Knowledge, Perception and source of information on Ebola virus
Disease in Nigeria. The objectives were to assess the public preparedness level to adopt
disease preventive behavior which is premised on appropriate knowledge, perception and
adequate information.84 An interview administered questionnaire on 5,322 respondents in the
twenty LGAs of Lagos State. Thirty three percent of respondents do not know the cause of
EVD, Forty one percent of the respondents possessed satisfactory general knowledge; 44%
and 43.1% possessed satisfactory knowledge on mode of spread and preventive measures,
respectively. Sixty-six percent and 49% of respondents mentioned regular hand washing
with soap and water, and avoiding contact with EVD case or suspect, respectively as a
preventive measure to prevent EVD. Sixteen percent mentioned avoiding eating bush meat
while 5% mentioned not participating in the burial rite of a person who died of EVD.
The findings indicate a gap in EVD related Knowledge and perception. There is a need for
targeted public health messages to raise knowledge level, correct misconception and
discourage stigmatization should be widely disseminated, with television and radio as media
of choice.
In a similar study on Public Knowledge, Attitudes, and Practices Relating to Ebola Virus
Disease (EVD) Prevention and Medical Care in Sierra Leone 2014. It was observed that the
comprehensive knowledge on EVD prevention by the public is generally low. Only 39% of
xlixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
the respondents were able to identify three means of prevention and rejected three
misconceptions. Also it was found out that everyone (100%) is aware of EVD and 97% of the
respondent surveyed belief EVD exist in Sierra Leone.76
Comprehensive knowledge of Ebola transmission and prevention is a prerequisite, although
Insufficient in itself, for the adoption of behaviors that reduce the risk of EVD. Correct
knowledge of the false modes of transmission is as important as knowing the correct modes –
and enables one to better understand how to protect oneself.
In August 2014, UNICEF and partners carried out a study on public Knowledge, attitudes
and practices related to EVD prevention and medical care in Sierra Leone. The objectives
were to examine public KAP related to EVD, identify barriers hindering containment of
disease, and use the study to inform evidence based strategies in preventing the transmission
of EVD and caring for those infected and affected by the outbreak.77 Key findings of the
study highlighted good level of awareness and low denial of EVD, low comprehensive
knowledge.
Another study was sponsored by Start Fund in Sierra Leone.78 The aim was to find out if
sensitization was effective in changing behavior to prevent Ebola transmission. One month
after the first case of EVD was reported in the country. Start Fund through its partners
responded by focusing on social mobilization and sensitization for 6 weeks. From 28 June to
12 August, the campaign reached 26% of the country’s approximately 6 million people.
Eighty eight percent of the people reached opined that the campaign against Ebola was a way
for the government and NGO’s to make money. At the end of the 45 day campaign, there was
an increase from 39% to 85% of households that could correctly identify EVD prevention
methods but there was no significant improvement in the time it takes for potential cases to
seek care.77 Importantly though, specific changes like reduced attendance at funerals,
lBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
increased hand washing and using gloves, decreased hand shaking and better precautions
from frontline health workers were observed.
Studies on Attitude of Ebola Viral Disease
A study on Public Knowledge, Attitudes, and Practices Relating to Ebola Virus Disease
(EVD) Prevention and Medical Care in Sierra Leone 2014.
A positive attitude towards preventive measures was also reported. Majority of respondents
reported behavioral change due to the comprehensive knowledge on the causes of EVD.
Radio was the preferred mean of receiving information and 96% of respondents reported
some discriminatory attitude towards suspected victims and survivors of disaster.76
Respondents mentioned that health professionals and government agencies are the most
trusted sources of information.
However, a study in Sierrra Leone conducted by Catholic Relief Service in conjunction with
UNICEF and FOCUS 1000, found out that nearly everyone (95%) is reporting some change
in behavior since learning about Ebola. However, the percentage of people reporting that they
avoid physical contact is alarmingly low (36%).76
Studies on Practices of Ebola Viral Disease
In March 2015, the Knowledge, Attitudes and Practice (KAP) study was conducted between
December 7th and 22nd , 2014, to gauge the success of social mobilization efforts to educate the
general public on key Ebola prevention messages in the country. The study design included
quantitative and qualitative components. A questionnaire survey from a representative sample
of 1,140 households was conducted in 6 purposively selected counties (Montserrado, Grand
Gedeh, Lofa, Nimba, River Cess and Grand Cape Mount). Counties were selected to cover a li
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
range in the timing and impact of the Ebola epidemic in different parts of Liberia. The
findings of the study indicated that the results demonstrate a high degree of community
mobilization against Ebola in all of the sampled counties. Virtually all Liberians had heard
about Ebola, accepted that Ebola was real, could identify the most common symptoms and
name at least 3 ways of avoid becoming infected. Overwhelming agreement with intended
behaviours such as isolation of those with symptoms, early treatment and safe burial show a
newly emerged consensus supporting public health recommendations. Comparable levels of
reported behaviour change in areas such as increased hand washing and reduced physical
contact suggest new behaviour norms were being put into action across sampled communities
by this stage in the Ebola epidemic. Perhaps the most striking finding is the high degree of
community engagement in the response, where people were not only changing their own
behaviour but interacting with family, friends, and neighbours to encourage them to do the
same. Survey results found nearly half of respondents had engaged in some form of
community action since the start of the epidemic.
Overall 93% of respondents reported they first learned about Ebola through the radio. The
next most common sources of information about Ebola were interpersonal communication
with family, friends and neighbors (39%) and house to house visits by health extension
workers (36%). Focus group discussions suggested radio reports, health visits and person-to-
person interaction sometimes worked to mutually reinforce each other.79
A study on the KAP of care professional regarding EVD was carried out in India in
August/September 2014. The study found satisfactory knowledge, attitude and practices
(<50% score) among 73.6%, 83.1% and 69.2% of the participants respectively.80
liiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
liiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
CHAPTER THREEMATERIALS AND METHODOLOGY
DESCRIPTION OF STUDY AREA
Lagos State was created in 1967 out of the former western region by the then regime of the
Military Head of State; General Yakubu Gowon (GCON) with its capital in Ikeja.
Location/Extent
The State is located ion the south- western part of Nigeria on the narrow coastal flood plain
of Bight of Benin. It lies approximately on longitude 20 420 E and 3 220 E East respectively
and between latitude 600 220 N. Lagos State shares boundaries with Ogun State of Nigeria
both in the North and East and is bounded on the west by the Republic of Benin and in the
South by the Atlantic Ocean. It has five administrative divisions of Ikeja, Badagry, Ikorodu,
Lagos Island and Epe.
Lagos State has population of about 17.5 million.81 Administratively, the State has 20 Local
Government Areas (LGAs).82 Lagos is a highly heterogeneous state comprising ethnic
groups from virtually all over the country and home to significant international populations.
There are 379 wards spread across these 20 LGAs with 276 Primary Health Care Centers
(PHCC) which serve as the first points of contact for citizens seeking health care services.
The smallest State in the Federation, it occupies an area of 358,862 hectares or 3,577 square
kilometers, 22% (or 787sq. km) which consists of lagoons and creeks. Lagos State is the
nation's economic nerve center with over 2,000 industries. Sixty five percent of the country's
commercial activities are carried out in the state. In addition, it served as the nation busiest
airport with two terminals international and cargo. Two of the nation's largest seaports -
Apapa and Tin-Can Ports are located in the State. The State is also a tourist center with many
livBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
tourism zones namely: Bar Beach Water; Lekki-Maiyegun resort; Kuramo Water; Epe-
Marina Cultural zone; Badagry Marina Recreation etc. Other prominent tourist attractions in
the State include; City Hall (Headquarters of the Lagos Island Local Government); the
National Arts Theatre, Iganmu; National Museum, Onikan; Holy Cross Cathedral, Lagos, the
seat of Catholic Archdiocese; Relics of Brazilian and other colonial quarters; the site of the
fallen Agia tree, Badagry, where Christianity was first preached in Nigeria in 1842; Oso-
Lekki Breakwaters.
There is also the Eyo festival which is held to mark important events in the state. While the
State is essentially a Yoruba speaking environment, it is nevertheless a socio-cultural melting
pot attracting both Nigerians and foreigners alike.
The population of the three local Government Areas covered by this survey includes; Agege
with an estimated population of 1,033,064, Ikeja 648,720 and Mushin 1,321,517.83 There are
30 Primary Health Care Centers (PHCC) in these three Local Government Areas which serve
as the first points of contact for citizens seeking health care services.
STUDY DESIGN
The study was a descriptive; community-based cross-sectional survey assessing the level of
preparedness amongst residents of Agege, Ikeja and Mushin Local Government Areas of
Lagos State against EVD Resurgence.
STUDY POPULATION
The population was individuals aged 18 years and above who live or trade in the
communities studied. The criteria for any respondent to be eligible for recruitment for the
survey was that (s)he must have lived in the area for not less than three (3) months.
lvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
SAMPLE SIZE DETERMINATION
The minimum sample size was determined using Cochran’s formula.84 The sample size for a
Cross-sectional study design is given as n=Z2pq/d2
p = estimated prevalence rate of knowledge of (58%). Gotten from previous similar
work done on the topic.85
q = 1-p
d = margin of error (0.05)
z = Confidence interval (Z score for 95% CI = 1.96)
n=1.962∗0.58(1−0.58)
0.05²=374.32
Anticipating a response rate of 90% was made by dividing the sample size calculated with a
factor f that is n/f, where f is the estimated response rate. Thus the calculated sample size
=374/0.09. The sample size is 416.
INCLUSION CRITERIA
Individuals of the household must be 18 years and above and live or trade in Agege, Ikeja and
Mushin LGAsthe communities studied for not less than 3 months.
EXCLUSION CRITERIA
Individuals of the household below 18 years who do not live or trade in Agege, Ikeja and
Mushin LGA for less than 3 months.the communities studied.
lviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
SAMPLING METHODOLOGY
A multi-stage sampling was used. Multistage refers to sampling plans where the sampling is
carried out in stages using smaller and smaller units at each stage.
Stage one:
Using simple random sampling (SRS) method, three local government areas (LGAs) were
selected from the sampling frame of twenty (20) LGAs in Lagos State. The selected local
government areas were Agege, Ikeja and Mushin.
Stage two:
The three (3) selected LGAs have 22 political wards from which, 5 wards per LGA were
selected from each LGA using simple random sampling method from the list of wards in each
LGA making a total of 15 wards. To select residents for the study, I divided my sample size
(416) by three (3) which represent the LGAs. This gave 139 study participants per LGA.
Thereafter, I divided the 139 per LGA by five (5) which represent the wards in each LGA
selected, this cumulated to 28 residents per ward in each of the three (3) selected LGAs.
To this end, having gotten the street names per ward from the three (3) LGAs information
officers, each street per ward was listed alphabetically by thein their name. i r names.
Stage three:
Using SRS method, four streets in each ward were selected The list of streets in each ward
alphabetically alphabetically interviewers visited the first street house starting from the first
house on the right side of street. Any respondent who met the inclusion criteria was selected
from each house, in other to meet the 28 residents per ward. arranged. Interviewers visited the lvii
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
first street, house starting from the first house on the right side of street. Any respondent who
met the inclusion criteria was selected from each house using SRS method.
In multi-dwelling houses, one household was selected using SRS method from each house
by balloting. A total of 28 residents interviewed per ward to ensure a sample size of 139 per
LGA. Multiple by 3 to give a total of 416. n=z2pq/d
DATA COLLECTION TOOL AND TECHNIQUE
Data was collected using a structured paper-based interviewer administered questionnaire; it
was both open-ended and close-ended. The questionnaire was written in English Language.
The three (3) interviewers who are Corps members serving with National Emergency
Management Agency (NEMA) were trained to administer the questionnaires and interpret it
to respondents who may not understand English well enough. The collection of data lasted
for two (2) months (July and August 2015).
The survey questionnaire which contains 21 items was adapted and modified from several
studies on knowledge, attitude and perception, level of Preparednessa against EVD
resurgence and practices regarding EVD.19 19 The questionnaire was structured in this format
to elicit response from the respondents.
Section A: Socio-demographic characteristics
The variables are:
Age: in years as at last birthday.
Sex: male and female.
Occupation: categories (professional, intermediate, manual skilled, non-manual skilled,
unskilled)86
lviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Professional: medical doctors, lawyers, architects
Intermediate: civil servant, banker, insurance brokers, stock brokers
Manual skilled: artisans
Non- manual skilled: office clerk, office assistants
Unskilled: traders, unemployed, housewives, students
Religion: Christian, Islam, Traditional and other
Highest level of education: None, Primary, Secondary, Tertiary
How long have you been resident here? Individuals of the household must be 18 years and
above and live or trade in the communities studied for not less than 3 months
Have you ever heard about Ebola Disease? Only residents that have heard of Ebola were
interviewed and submitted for analysis.
Section B: Knowledge of Ebola Viral Disease
The variables are:
What causes Ebola disease? (multiple responses allowed)
How can EbolaEbola can be spread
When the signs of illness are begin after the Ebola virus enters the body
Is there a specific drug/ remedy to treat Ebola disease
Is there a specific vaccine to treat Ebola Disease?
How can you prevent yourself from contracting Ebola Disease?
Section C: Sources and Channel of Information regarding EVD
The variable is: How did you hear about Ebola virus disease (multiple responses allowed)
Section D: Attitude and Perception regarding EVD
lixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
The variables are:
Do you think Ebola virus disease is a problem in Lagos (multiple responses allowed)
Do you think you are in danger of infection with Ebola virus disease?
Do you think government can do more to contain Ebola virus disease?
Section D: Level of Preparedness against EVD resurgence
The variable: What is done to prevent risk of spread of EVD at home or work, using five key
practices, which are regular hand washing with soap and water, regular use of hand sanitizer,
avoidance of bushmeat, not touching people with EVD, non-participation in burial rites and
what is done if a family member, relative/neighbor develop signs of Ebola.
PRE-TESTING
The questionnaires were pre-tested in assigned selected streets in Suru-lere LGA of Lagos
State which is not included in the sample. Feedbacks from the pre-test were used to improve
the questionnaire.
INFORMED CONSENT
Respondent’s informed consent duly obtained after explaining the purpose and procedure of
the Research. This is in line with the “Helsinki Declaration” which emphasis the need for
confidentiality of their responses, assured of voluntary participation and the opportunity for
them to withdraw at any time without prejudice.
ETHICAL CONSIDERATIONSlx
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Ethical approval was gotten from the Human Research and Ethics Committee (HREC) of the
Lagos University Teaching Hospital and Informed consent was sought from each participant
before the commencement of the exercise.
METHODS OF DATA ANALYSIS
The data gathered were analysed by Epi-info 3.5.4 and reported as frequencies and
percentages. Also associations between variables were tested statistically using Chi-square
and reported at a significance level of p < 0.05. The knowledge will be based on three EVD
domains; mode of spread, symptoms and signs and preventive and control measures. scores
were assigned to correct responses mentioned by respondents. Furthermore stratified analysis
was done on satisfactory knowledge to access knowledge across each domain.83 78 77
Scoring of response
Knowledge of Ebola Viral Disease-each correct response of the knowledge question was
scored 1 mark and a wrong answer or non-response was scored 0. Total score achievable was
27 marks: 16 marks and above was categorized as satisfactory, below 16 marks was
categorized as poor.
Attitude and perception regarding Ebola Viral Disease- a set of 9 questions were used to
evaluate overall level of attitude and perception of respondents to EVD. The maximum
achievable score for attitude and perception was 9 marks.
Rrespondentsrespondentsespondents who scored 6 marks and above were categorized as
positive attitude and perception while respondents that scored below 5 marks had a negative
attitude and perception.
lxiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Practices regarding Ebola viral Disease- Overall level of preparedness by Respondents
against EVD resurgence. The maximum achievable for level of preparedness was 6 marks.
Respondents who scored 4 marks and above were categorized as high level of preparedness
while respondents that scored below 4 marks had low level of preparedness.
LIMITATION OF THE STUDY
`Self-Reported behaviours may not always be arrayed with respondent’s actual practices.
Current desirable responses may be claimed due to high awareness, sensitization of EVD
being undertaken. Moreover, the study is a new research area; literature reviews documents
particularly preparedness level against EVD resurgence was difficult to get.
lxiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
CHAPTER FOUR RESULTS
A total of 416 questionnaires were administered to the respondents. Three hundred and ninety
said yes they have heard about Ebola Disease (93.98%) and were interviewed and submitted
for analysis. While 26 respondents said they have not heard about Ebola Disease (6.02%) and
no further analysis was done.
Table 31: Respondents used in the study
Heard about Ebola Disease (n=416) Number of respondents (%)
Yes 390 ( 93.98)
No 26 (6.02)
lxiiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 42: Socio-demographic characteristics of respondents
lxivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Socio-demographic characteristics (n= 390) Number of
respondents (Frequency (%)
Age distribution (in years)
<20 19 (4.6%)
21-30 130 (31.3%)
31-40 153 (36.8%)
41-50 70 (16.8%)
51-60 23 (5.5%)
> 60 21 (5.0%)
Sex
Male 215 (51.7)
Female 200 (48.1)
Religion
Christianity 249 (59.9)
Islam 158 (38.0)
Traditional 8(1.9)
Others 1 (0.2)
A total of 390 respondents were interviewed. Fifty one point seven percent were male; the
mean age was 41 years (+35.7 years). Majority of the respondents were Christians (59.9%)
(Table 2).
lxvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 53: Socioeconomic characteristics of respondents
Highest level of formal education Frequency (%)
None 5 (1.2)
Primary 24 (5.8)
Secondary 140 (33.7)
Tertiary 247 (59.4)
Occupation
Professional 25 (6.0)
Intermediate 38 (9.1)
Manual Skilled 50 (12.0)
Non- Manual Skilled 27 (6.5)
Unskilled 209 (50.2)
Duration of Residency
< 1Year 93 (22.3)
> 1Year 323 (77.6)
lxviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Highest level of formal education Frequency (%)
None 5 (1.2)
Primary 24 (5.8)
Secondary 140 (33.7)
Tertiary 247 (59.4)
Occupation
Professional 25 (6.0)
Intermediate 38 (9.1)
Manual Skilled 50 (12.0)
Non- Manual Skilled 27 (6.5)
Unskilled 209 (50.2)
Duration of Residency
< 1Year 93 (22.3)
> 1Year 323 (77.6)
The respondents were largely with tertiary education (59.4%) and (77.6%) of the respondents
have lived in the survey area for more than one year and were mainly traders, unemployed,
students or housewives (50.2%) (Table 3).
lxviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 4: Knowledge score of respondents on causes of Ebola disease
What causes Ebola disease Correct (%) Incorrect (%)
From infected animals 301 (77.0) 89(23)
Contact with a person who is sick of Ebola disease
241 (57.9) 149 (42.1)
Touching blood, urine, stool or saliva from a person who is sick with Ebola disease
190 (48.6) 200 (51.4)
Sharing sharp objects such as razors, needles, etc. with a person who has Ebola disease
148 (37.9) 242 (62.1)
Contact with beddings, clothing and
other personal utensils (plates, cups)
119 (30.4) 271 (69.6)
Participating in burial rites of a person
who has died from Ebola Disease
98 (25.1) 292 (74.1)
98 (25.1)
lxviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
28 (7.2)
35 (9.0)
Seven-seven percent of the respondents believed that EVD is caused by infected animals to man,
57.9% of the respondents mentioned that it is caused by contact with a person who is sick of EVD
EVDwhile 9.0% of the respondents do not know the cause of EVD (Table 4).. However, 74.1%
incorrectly said that participating in burial rites of a person who has died from Ebola disease
cannot cause EVD. This is a major key knowledge (Table 4).
Table 5: Knowledge on the spread of Ebola Viral disease (n=390)
What causes Ebola disease Correct (%) Incorrect (%)
From infected animals to man 271 (69.3) 119 (30.7)
Touching blood, urine, stool or saliva from a person who is sick with Ebola disease
221 (56.5) 169 (43.5)
Contact with a person who is sick of Ebola disease
201 (51.4) 189 (48.6)
Sharing sharp objects such as razors, needles, etc. with a person who has Ebola disease
139 (35.5) 251 (64.5)
lxixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Contact with beddings, clothing and other personal utensils (plates, cups) of a person who is sick of Ebola disease
130 (33.2) 260 (66.8)
Participating in burial rites of a person
who has died from Ebola Disease
110 ( 28.1) 280 (71,9)
Sixty nine point three percent of the respondents correctly mentioned believed that EVD is
spread through infectious animals to man. While 56.5% of the said that is through touching
blood, urine, stool, or saliva from a person who is sick of EVD and 71.9%28.1 % incorrectly
mentioned bythat by not participating in burial rites of a person who has died from Ebola
disease cannot spread the disease (Table 5).
Table 5: Knowledge on the spread of Ebola Viral Disease
How can Ebola be spread Frequency (%)
From infected animals to man 271 (69.3)
lxxBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Touching blood, urine, stool, or saliva from a person
who is sick with Ebola disease 221 (56.5)
Contact with a person who is sick of Ebola disease 201 (51.4)
Sharing sharp objects such as razors, needles etc
with a person who has Ebola disease 139 (35.5)
Contact with beddings, clothing and other personal utensils (plates, cups)
of a person who is sick of Ebola disease 130 (33.2)
Participating in burial rites of a person who has
died from Ebola disease 110 (28.1)
Through spiritual attack 50 (12.8)
Through insect bites 44(11.3)
Through the air 37 (9.5)
I don’t know 14 (3.6)
Sixty nine point three percent of the respondents believed that EVD is spread through
infectious animals to man. While 56.5% of the said that is through touching blood, urine,
stool, or saliva from a person who is sick of EVD and 28.1 % mentioned by not participating
in burial rites of a person who has died from Ebola disease (Table 5).
lxxiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Figure 12: Knowledge of Signs and Symptoms of Ebola Viral Disease mentioned by
respondents (n=390)
The top three signs and symptoms of EVD mentioned by respondents were diarrhea (94.0%),
fever (52.6%) and weakness (45.9) (Figure 12).
lxxiiBabatunde Olowookere 910706002
Rash on the body
Sore throat
Body pains
Abnormal bleeding from any part of the body
General feeling of unwell
Headache
Weakness
Vomiting
Fever
Diarrhoea
0.0 20.0 40.0 60.0 80.0 100.0
21.9
24.0
26.4
32.2
36.1
43.8
45.9
47.1
52.6
94.0
Percentage (%)

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 6: Knowledge on when signs of illness of Ebola Viral Disease begins by
Respondents (n=390)
When do signs of illness begin after
the EVD enters the body
Correct (%) Incorrect (%)
Between 2 and 21 days 208 (60.5) 182 (39.5)
Only (60.5% 0.0%) of the respondents knew the correct duration before signs of illness of
Ebola Viral Disease begins. Indicated that the signs of illness of EVD begin between 2 and
21 days which is good knowledge (Table 6).
Majority (50.0%) of the respondents indicated that the signs of illness of EVD begin between
2 and 21 days which is good knowledge. While (11.5%) indicated that the signs of illness of
EVD begin less than 2 days (Table 6).
Knowledge of causes of EVD Correct Incorrectlxxiii
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
When do signs of illness begin after the EVD enters
the body
208 () 182 ()
Is there a specific drug/remedy to treat Ebola disease 153 () 237 ()
Knowledge of spread of EVD Correct Incorrect
When do signs of illness begin after the EVD enters
the body
208 () 182 ()
Is there a specific drug/remedy to treat Ebola disease 153 () 237 ()
Knowledge of signs of EVD Correct Incorrect
When do signs of illness begin after the EVD enters
the body
208 () 182 ()
153 () 237 ()
lxxivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Knowledge of treatment and prevention of EVD Correct Incorrect
Is there a specific drug/remedy to treat Ebola disease
lxxvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 7: Knowledge on drug /remedy to treat Ebola Viral Disease
Is there a specific drug/remedy to treat
Ebola disease Frequency (%)
Yes 150 (36.1)
No 153 (36.8)
I don’t know 87 (27.1)
Is there a specific vaccine to treat Ebola disease?(Multiple responses allowed)
Yes 94 (22.6)
No 135 (32.5)
I don’t know 161 (44.9)
Thirty-six point eight percent of respondents indicated that there is either no specific drug or
specific remedy to treat EVD while 32.5% affirmed that there is no specific vaccine to
prevent the disease (Table 7).lxxvi
Babatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 8: Knowledge on how to prevent contracting Ebola Viral Disease
How can you prevent yourself from
Contracting Ebola disease Frequency(%)
Regular hand washing with soap and water307 (78.5)
By not touching a person with suspected Ebola infection 232 (59.5)
Regular use of hand sanitizer 215 (55.0)
Avoid eating bush meat 132 (33.9)
Regular hand washing with water only 45 (11.5)
By not participating in burial rites of a person that dies of Ebola disease 104 (26.7)
Eating bitter kola 57 (14.6)
lxxviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Drinking salt water 34 (8.7)
By staying at home 36 (9.3)
Going for special prayers 35 (9.0)
Bathing with salt water 32 (8.2)
Regular hand washing with ash 31 (7.9)
I don’t know 15 (3.8)
Of the various EVD preventive measures 78.5% of respondents mentioned regular hand washing with soap and water, 59.5% affirmed to not touching a person with suspected Ebola infection. Fifty-five percent mentioned regular use of hand sanitizer while 33.9% mentioned avoid eating bush meat and 26.7% said not participating in burial rites of a person that dies of Ebola disease. This show that there is knowledge gap concerning respondent’s knowledge in not participating in burial rites of a person that dies of EVD (Table 8).
Figure 23: Knowledge on sources and channels of information regarding EVD (n=390)
lxxviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Figure 2
shows the
sources of
information on EVD. Majority respondents 84.1% heard about EVD from radio, 83.8% got
the information through television. While 7.7%, 14.3%, 6.1%, 7.2%, 17.4%, 12.6%, 10.3%,
11.5%, 10.6%, 25.6%, 15.4%, 25.6%, 24.8%, 23.5% heard about EVD from journal,
newspapers, town announcer, mosque, church, family member, peers, health facility, flyer,
internet site, social media, GSM/SMS, market, neighbourhoods respectively (Figure 23).
lxxixBabatunde Olowookere 910706002
Radio
Televi
sion
Journal
Newspap
er
Town an
nouncer
Mosque
Church
Family
mem
ber
Peers
Health fa
cility
Flyer
Internet
sites
Socia
l med
ia N
GSM/SM
S
Market
Neighbourh
ood
0
10
20
30
40
50
60
70
80
90

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 79: Attitude and perception regarding Ebola Viral DiseaseLevel of preparedness
against Ebola Viral Disease resurgence
What do you do at Home/work to
Reduce the risk of exposure?
Correct (%) Incorrect (%)
Regular hand wash with soap and water 321 (82.3) 69 (17.7)
Regular use of hand sanitizer 217 (55.6) 173 (44.4)
Avoid eating bush meal 112 (28.7) 278 (71.3)
By not touching a person with suspected Ebola
infection
92 (23.6) 298 (76.4)
By not participating in burial rites of a person
that dies of Ebola disease
57 (14.7) 333 (85.3)
Do you think Ebola Virus Disease
is a problem in Lagos? Frequency (%)
Yes 195 (46.9)
No 161 (38.7 )
I don’t know 34 (14.4)
If yes, specify(multiple responses allowed)
It is a deadly disease 153 (76.1)
It creates a lot of panic 90 (44.8)
It is highly infectious 85 (42.3)
It has no cure 82 (40.8)
It is an attack by the Western world 45 (22.4)
If no, specify(multiple responses allowed)
There are only few cases 87 (53.0)
lxxxBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
It is just being exaggerated 74 (45.1)
I do not believe that there are cases of EVD 66 (40.2)
People just want to make money with Ebola drug 35 (21.3)
Majority (82.3%) 46.9 % of respondents correctly identified regular hand wash with soap and
water, 55.6% the respondents said they use hand sanitizer. while 28.7% respondents avoid
eating bush meat and 85.3% incorrectly said they will participate in burial rites of a person
that died of Ebola disease (Table 7).
perceived EVD as a problem in Lagos State. Seventy-six percent believed that EVD is a
deadly diseaseasdiseases the reasons for this perception while 53% believed that there are
only few cases (Table 9).
lxxxiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 10: Attitude and perception regarding Ebola Viral Disease
Do you think you are in danger of infection
with Ebola Virus Disease? Frequency (%)
Yes 185 (44.5)
No 158 (38.0)
I don’t know 47 (17.5)
Do you think government can do more to contain Ebola Virus Disease outbreak?
Yes 218 (52.4)
No 90 (21.6)
I don’t know 82 (26)
About 44.5% of respondents thought that they are in danger of infection with Ebola virus
disease while 38.0 % thought otherwise. 52.4% of respondents also thought that government
is doing enough to contain Ebola virus disease outbreak. (Table 10).
lxxxiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 11: Level of preparedness against Ebola Viral Disease resurgence
What do you do at Home/work to
reduce the risk of exposure?Frequency (%)
Regular hand wash with soap and water 321 (82.3)
Regular use of hand sanitizer 217 (55.6)
Avoid eating bush meat 112 (28.7)
By not touching a person with suspected Ebola infection 92 (23.6)
Regular hand wash with water only 66 (16.9)
By not participating in burial rites of a person that dies of Ebola disease 57 (14.7)
Regular hand wash with ash 56 (14.4)
Going for special prayers 39 (10.0)
Drinking salt water 21 (5.4)
Eating bitter kola 27 (6.9)
Bathing with salt water 27 (6.9)
By staying at home 24 (6.2)
lxxxiiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
I don’t know 21 (5.4)
Majority (82.3%) of the respondents mentioned regular hand wash with soap and water,
55.6% the respondents said they use hand sanitizer. While 28.7% respondents avoid eating
bush meat and14.7% not participating in burial rites of a person that died of Ebola disease
as precautionary measures to reduce risk of exposure to EVD (Table 11).
Table 12: Practices regarding Ebola Viral Disease
What do you do if you develop signs of Ebola(multiple responses allowed) Frequency (%)
Go to the hospital 339 (86.9)
Call the Ebola help number 197 (50.5)
Pray 125 (32.1)
Go to religious centre 31 (7.9)
Go to a traditional healer 28 (7.2)
lxxxivBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Treat myself 16 (4.1)
Hide 9 (2.3)
Stay at home 8 (2.1)
Do nothing 6 (1.5)
If a family member, relative/neighborneighbour develop signs of Ebola(multiple responses allowed)
Go to the hospital 337 (86.4)
Call the Ebola help number 195 (50.0)
Pray 125 (32.1)
Go to religious centre 28 (7.2)
Go to a traditional healer 27 (6.9)
Treat myself 14 (3.6)
Hide 10 (2.6)
Stay at home 9 (2.3)
Do nothing 7 (1.8 )F
Eighty-six point four percent of respondents mentioned that they will go or advise someone
to go to hospital if they develop EVD-like signs and symptoms; 50.0% would call or tell
someone to call the Ebola Alert number. Thirty-two point one said they will pray or ask
someone to pray if they develop signs and symptoms of EVD (Table. 12).
lxxxvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Figure 3:Table 7: Overall level of knowledge of respondents on EVD
135; 32%
281; 68%
PoorSatisfactory
The overall level of knowledge shows thatof the the 309 respondents, 281.68% possessed
ssatisfactory knowledge on the Ebola while 135.32% possessed poor knowledge.( (Figure 3).
lxxxviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table Table 813: Knowledge score of respondents on EVD across all domains
Respondents with good knowledge across all domains
LGA Mode of
spread
Symptoms
& Signs
Preventive
measure
Level of
Preparednes
s
Knowledge in all
domains
Ikeja (139) 21(15.1%) 41(29.5%) 4(2.9%) 3 (2.2%) 10 (7.2%)
Agege (136) 21 (15.4%) 32 (23.5%) 2 (1.5%) 2 (1.5%) 3 (2.2%)
Mushin
(141)
20 (14.2%) 29 (20.6%) 6(4.3%) 8 (5.7%) 13 (9.2%)
All
respondents
62 (15.0%) 102 (24.5) 12(2.9%) 13 (3.1%) 26 (6.2)
lxxxviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Knowledge across all domains shows that of the 390 respondents, 6.2% possessed
satisfactory knowledge in all three domains. 15%, 24.5%, 2.9% and 13.1% possessed
satisfactory knowledge in signs and symptoms, preventive measures and mode of spread and
level of preparedness (Table 138).
Table 914: Association between Socio-demographic characteristics of respondents and
their Knowledge of EVD (n=416)
lxxxviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Variable Knowledge of EVD (%)X2 df p-value
Poor Satisfactory
Age
< 20 8 (42.1%) 11 (57.9%) 19 8.476 6 0.205
21-30 42 (32.3%) 88 (67.7%) 130
31-40 43 (28.1%) 110 (71.9) 153
41-50 23 (32.9) 47 (67.1%) 70
51-60 9 (39.1%) 14(60.1%) 23
> 60 10 (43.5%) 11 (56.5%) 21
Sex
Female 59 (29.5%) 141 (70.5%) 200 1.531 1 0.216
Male 76 (35.2%) 140 (64.8%) 216
Religion
Christian 70 (28.1%) 179 (71.9%) 249 6.034 3 0.110
Islam 62 (39.2) 96 (60.8) 158
Traditional 3 (37.5%) 5 (62.5%) 8
Others 0 (0%) 1 (100.0%) 1
There was no statistically significant relationship between age and knowledge (p=0.205), sex
and knowledge (p=0.216) and religion and knowledge (p=0.110). This means age, sex and
religious does not determine the level of knowledge of respondents towards the prevention
and spread of EVD (Table 149).
lxxxixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 15: Association between Socio-economic characteristics of respondents and their
Knowledge of EVD (n=390)
Variable Knowledge of EVD (%) X2 df p-value
Poor Satisfactory Total
Highest level Education
None 5 (100.0%) 0 (0%) 5 23.968 3 0.000
Primary 14 (58.3%) 10 (41.7%) 24
Secondary 52 (37.1%) 88 (62.9%) 140
Tertiary 64 (25.9%) 183 (74.1%) 247
Occupation
Professional 1 (4.0%) 24 (96.0%) 38 21.124 5 0.001
Intermediate 4 (10.5%) 34 (89.5%) 36
Manual
skilled17 (34.0%) 33 (66.0%) 50
Non-manual
skilled9 (33.3%) 18 (66.7%) 27
Partly skilled 26 (38.8%) 41 (61.2%) 67
Unskilled 78 (37.3%) 131 (62.7%) 209
Variable Knowledge of EVD (%) X2 df p-value
Poor Satisfactory Total
Highest level Education
None5 (100.0%) 0 (0%) 5 23.968 3 0.000
xcBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Primary 14 (58.3%) 10 (41.7%) 24
Secondary 52 (37.1%) 88 (62.9%) 140
Tertiary 64 (25.9%) 183 (74.1%) 247
Occupation
Professional 1 (4.0%) 24 (96.0%) 38 21.124 5 0.001
Intermediate 4 (10.5%) 34 (89.5%) 36
Manual
skilled17 (34.0%) 33 (66.0%) 50
Non-manual
skilled9 (33.3%) 18 (66.7%) 27
Partly skilled 26 (38.8%) 41 (61.2%) 67
Unskilled 78 (37.3%) 131 (62.7%) 209
Table 10: Association between Socio-economic characteristics of respondents and their Knowledge of EVD (n=390)
There was a statistically significant association between educational status and knowledge
(p=0.000) and occupation and knowledge (p=0.001). This buttresses the fact that the higher
the educational level and professionalism, the higher the knowledge of respondents on EVD
prevention (Table 150).
Table 11: Association between Socio-demographic characteristics of respondents and their
Attitude and perception of EVD (n=390).
Variable Attitude and perception (%)
xciBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 16: Association between Socio-demographic characteristics of respondents and their
Attitude and perception of EVD (n=416390) X2 df
p-value
Negative Positive Total
Age
< 20 15 (78.9%) 4 (21.1%) 19 8.802 6 0.185
21-30 66 (50.8%) 64 (49.2%) 130
31-40 83 (54.2%) 70 (45.8%) 153
41-50 43 (61.4%) 27(38.6%) 70
51-60 14 (60.9%) 9 (39.1%) 23
> 60 15 (77.3%) 6 (22.7%) 21
Sex
Female 111 (55.5%) 89 (44.5%) 200 0.238 1 0.626
Male 125 (57.9%) 91(42.1%) 216
Religion
Christian 138 (55.4%) 111 (44.6%) 249 6.034 3 0.110
Islam 92 (58.2%) 66 (41.8%) 158
Traditional 5 (62.5%) 3 (37.5%) 8
Others 1 (0%) 0 (100.0%) 1
There was no statistically significant relationship between age and attitude and perception
(p=0.185), sex and attitude and perception (p=0.626) and religion and attitude and
xciiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
perception (p=0.110) this indicates that age, attitude and perception, sex and religion does not
determine a person’s level of knowledge towards the prevention of EVD (Table 161).
Variable Attitude and perception (%) Total X2 X2X2 df p-value
Negative Positive
Highest level Education
None 4 (80.0%) 1 (20.0%) 5 3.916 3 0.271
Primary 17 (70.8%) 7(29.2%) 24
Secondary 74 (52.9%) 66 (47.1%) 140
Tertiary 141 (57.1%) 106 (42.9%) 247
Occupation
Professional 18 (72.0%) 7 (28.0%) 38 21.124 5 0.001
Intermediate 23 (60.5%) 15 (39.5%) 36
Manual
skilled
26 (52.0%) 24 (48.0%) 50
Non-manual
skilled
19 (70.4%) 8 (29.6%) 27
xciiiBabatunde Olowookere 910706002
Table 17: Association between Socio-economic characteristics of respondents and their
Attitude and perception regarding of EVD

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Partly skilled 37 (55.2%) 30 (44.8%) 67
Unskilled 113 (54.1%) 96 (45.9%) 209
Table 12: Association between Socio-economic characteristics of respondents and their
Attitude and perception regarding of EVD.
Highest level Education
None 4 (80.0%) 1 (20.0%) 5 3.916 3 0.271
Primary 17 (70.8%) 7(29.2%) 24
Secondary 74 (52.9%) 66 (47.1%) 140
Tertiary 141 (57.1%) 106 (42.9%) 247
Occupation
Professional 18 (72.0%) 7 (28.0%) 38 21.124 5 0.001
Intermediate 23 (60.5%) 15 (39.5%) 36
Manual
skilled
26 (52.0%) 24 (48.0%) 50
Non-manual
skilled
19 (70.4%) 8 (29.6%) 27
Partly skilled 37 (55.2%) 30 (44.8%) 67
Unskilled 113 (54.1%) 96 (45.9%) 209
Table 17: Association between Socio-economic characteristics of respondents and their Attitude and perception regarding of EVD
There was no statistically significant relationship between highest level of education and attitude and perception (p=0.271). However, there was statistically significant relationship between occupation and attitude and perception (p=0.001). This supports the fact that
xcivBabatunde Olowookere 910706002
Variable Attitude and perception (%) Total X2 df p-value

Residents Preparedness Level Against Ebola Virus Disease Resurgence
professionalism can determine attitudinal change and perception towards EVD prevention (Table 17).
There was no statistically significant relationship between highest level of education and
attitude and perception (p=0.271). However, there was statistically significant relationship
between occupation and attitude and perception (p=0.001). This supports the fact that
professionalism can determine attitudinal change and perception towards EVD prevention
(Table 12).
Table 183: Association between Socio-demographic characteristics of respondents and
their Level of Preparedness against of EVD resurgence
Variable
Level of preparedness (%) X2 Df p-value
Low High Total
Age
< 20 16 (84.2%) 3 (15.8%) 19 8.9333 6 0.177
21-30 88 (67.7%) 42 (32.3%) 130
31-40 95 (62.1%) 58 (37.9%) 153
41-50 48 (68.6%) 22(31.4%) 70
51-60 18 (78.3%) 5 (21.7%) 23
> 60 18 (86.7%) 4 (13.3%) 21
Sex
Female 141 (70.5%) 59 (29.5%) 200 1.081 1 0.298
Male 142 (65.7%) 74 (34.3%) 216
xcvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Religion
Christian 156 (66.3%) 84 (33.7%) 249 1.532 3 0.675
Islam 112 (70.9%) 46 (29.1%) 158
Traditional 5 (62.5%) 3 (37.5%) 3
Others 1 (100.0%) 0 (0.0%) 1
There was no statistically significant relationship between age and level of preparedness
(p=0.177), sex and level of preparedness (p=0.298) and religion and level of preparedness
(0.675). Preparedness against EVD re-emergence do not determine by age, sex and religion
(Table 138).
xcviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 149: Association between Socio-economic characteristics of respondents and their
level of preparedness EVD resurgence
Variable Level of preparedness (%) X2 Df p-value
Low High Total
Highest level Education
None 5 (100.0%) 0 (0.0%) 5 4.916 3 0.185
Primary 18 (75.0%) 6 (25.0%) 24
Secondary 100 (71.4%) 40 (28.6%) 140
Tertiary 160 (64.8%) 87 (35.2%) 247
Occupation
Professional 14 (56.0%) 11 (44.0%) 25 3.235 1 0.072
Intermediate 20 (52.6%) 18 (47.4) 38
Manual
skilled30 (60.0%) 20 (40.0%) 50
Non-Manual
skilled20 (74.1%) 7 (25.9%) 27
Partly
skilled50 (74.6%) 17 (25.4%) 67
Unskilled 149 (71.3%) 60 (28.7%) 209
There was no statistical significance between the highest level of education and level of
preparedness (0.185). However there was a statistical significant association between
occupation and level of preparedness (p=0.072). This affirmed to the fact that preparedness is
a function of availability of resources and social class (Table 149).
xcviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Table 2150: Association between Socio-demographic characteristics of respondents and
practices regarding EVD
Variable Practices regarding (%) X2 df p-value
Negative Positive Total
Age
< 20 2 (10.5%) 17 (89.5%) 19 3.852 6 0.697
21-30 22 (16.9%) 108 (83.1%) 130
31-40 18 (11.8%) 135 (88.2%) 153
41-50 7 (10.0%) 63 (90.0%) 70
51-60 4 (17.4%) 19 (82.6%) 23
> 60 2 (13.3%) 19 (86.7%) 21
Sex
Female 23 (11.5%) 177 (88.5%) 200 0.995 1 0.319
Male 32 (14.8%) 184 (85.2%) 216
Religion
Christian 146 (58.6%) 103 (41.4%) 249 4.119 3 0.249
Islam 106 (67.1%) 52 (32.9%) 158
Traditional 6 (75.0%) 2 (25.0%) 8
Other 1 (100%) 0 (0%) 1
xcviiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
There was no statistically significant relationship between age and practices (p=0.697), sex
and knowledge (p=0.319) and sex and practices (p=0.249). This shows that the age and sex
do not determine practices towards EVD prevention (Table 1520).
Table 216: Association between Socio-economic characteristics of respondents and
practices regarding EVD resurgence
Variable Practices regarding EVD Total X2 df p-value
Negative Positive
Highest level Education
None 3 (60.0%) 2 (40.0%) 5 24.048 3 0.000
Primary 8 (33.3%) 16 (66.7%) 24
Secondary 23 (16.4%) 117 (83.6%) 140
Tertiary 21 (8.5%) 226 (91.5%) 247
Occupation
Professional 0 (0.0%) 25 (100.0%) 25 10.359 5 0.066
xcixBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Intermediate 1 (2.6%) 37 (97.4%) 38
Manual
skilled7 (14.0%) 43 (86.0%) 50
Non-Manual
skilled3 (11.1%) 24 (88.9%) 27
Partly skilled 13(19.4%) 54 (80.6%) 67
Unskilled 31 (14.8%) 178 (85.2%) 209
However there was a statistically significant association between educational status and
practices (p=0.000) and occupation and practices (0.066). This implies that educational level
and professionalism enhanced positive practices in EVD prevention and mode of spread
(Table 216).
CHAPTER FIVE
DISCUSSION
Preparedness is a function of availability of resources, satisfactory knowledge, positive
attitude and standard practices/protocols. It envisages entire health system from physician’s
preparedness; hospital preparedness, laboratory and diagnostic preparedness to the public
health preparedness.
cBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
Ebola Virus Disease Preparedness has been underscored worldwide and in countries away
from the epicenters of the current outbreak.87 Worthy of note is the fact that there was little
interest in EVD preparedness level before the recent occurrence.88
The demographic pattern of participants in this study shows that majority of the respondents
were male (51.7%) and are Christians (59.9%). More than half (58.1%) of the respondents
had tertiary education and 50.2% were mainly traders, unemployed, students or housewives
which had the highest number of respondents.
The study also revealed that majority of the respondents have moderate knowledge of the
signs of EVD (94%), spread of EVD (69.3%), signs of illness (50.0%), likely wise 78.5% of
the respondents affirmed that to prevent contracting EVD by regular hand washing with soap
and water, 59.5% of the respondents stated that not touching persons with suspected EVD
infection, 55.0% mentioned regular use of hand sanitizer while 3.8% of the respondents do
not know how to prevent contacting EVD.
The findings above is not in tandem with the report of International Federation of Red cross
and Red Crescent Societies stating that Liberian citizens have limited knowledge regarding
the mode of transmission of the Ebola virus.89
Preparedness is a function of availability of resources, satisfactory knowledge, positive attitude and standard practices/protocols. It envisages entire health system from physician’s preparedness, hospital preparedness, laboratory and diagnostics preparedness to the public health preparedness.Ebola Virus Disease Preparedness has been underscored worldwide and in countries away from the epicenters of the current outbreak.90 Worthy of note is the fact that there was little interest in EVD preparedness level before the recentoccurrence.91
The demographic pattern of participants in this study shows that majority of the respondents were male (51.7%) and are Christians (59.9%). More than half (58.1%) of the respondents had tertiary education and 50.2% were mainly traders, unemployed, students or housewives which had the highest number of respondents.
ciBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
The study also revealed that majority of the respondents have moderate knowledge of
thesigns of EVD (94%), spread of EVD (69.3%), signs of illness (50.0%), likely wise 78.5%
of the respondents affirmed that to prevent contracting EVD by regular hand washing with
soap and water, 59.5% of the respondentsstated that not touching persons with suspected
EVD infection, 55.0% mentioned regular use of hand sanitizer while 3.8% of the respondents
do not know how to prevent contacting EVD.
The findings above is not in tandem with the report of International Federation of Red cross
andRed Crescent Societies stating that Liberian citizens have limited knowledge regarding
the mode of transmission of the Ebola virus.92
Likewise, the survey established that knowledge across all domains shows that of the 390
respondents, 6.2% possessed satisfactory knowledge in all three domains. 15%, 24.5%, 2.9%
and 13.1% possessed satisfactory knowledge in signs and symptoms, preventive measures
and mode of spread and level of preparedness.
There was a significantassociationsignificant association of residents’knowledgeresidents’
knowledge on educational status andoccupationand occupation (p-value: 0.000 and 0.001).
This study found out that the higher the educational status and occupation the more
satisfactory knowledge of EVD. This favors the argument that income and education are
positively associated with disaster preparedness.93 Education in particular is a key tool to
promote disaster preparedness because highly educated individuals have better economic
resources to undertake preparedness actions and because education may influence cognitive
elements and shape how individuals perceived and received and assess risks, and how they
ciiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
process risk- minimizing information.94Likewise, earlier research has found that highly
educated individuals in Indonesia are reported to cope better with the post-tsunami phase of
the disaster, especially over the long run.95
However, there was statistically significant relationship between occupation and attitude and
perception (p-value: 0.001). This study found out that socio-economic status of residents such
as occupation enhanced positive attitude and perception.
There was also a statistically significant association between occupation and level of
preparedness (p-value: 0.072). This also shows that high level of preparedness of residents is
determined by their occupation. The empirical evidence on the relationship between the
preparedness level and the income has been adequately established.8787 8784
There was a statistically significant association between educational status and practices
(p=0.000) and occupation and practices (0.066). This implies that educational level and
professionalism enhanced positive practices in EVD prevention and mode of spread.
The commendation by World Health Organization and other nations on thecontainmentthe
containment of EVD outbreak in Nigeria was corroborated by respondents (52.4%) who
believed that government is doing enough to contain the EVD outbreak.8479 This also
translated to respondents high level of preparedness level and practices such as regular hand
ciiiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
wash with soap and water and use of hand sanitizers to prevent the spread of highly infectious
diseases.
Preparedness is a function of availability of resources, satisfactory knowledge, positive
attitude and standard practices/protocols. It envisages entire health system from physician’s
preparedness, hospital preparedness, laboratory and diagnostics preparedness to the public
health preparedness.
civBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
CONCLUSION
Findings from this study indicates that majority of the respondents have adequate knowledge
of causes, spread and prevention of EVD in the study areas. There is positive attitude towards
prevention of EVD resurgence in the three LGAs surveyed. The result demonstrates a high
degree of preparedness level against the resurgence of Ebola Virus Disease in the three (3)
LGAs of Lagos State. Majority of the respondents who had heard about Ebola accepted that
Ebola was real and could not identify the most common things.
Given that being affected by Ebola is a truly life changing experience with far reaching
consequences on both survivors and caregivers, appropriate interventions are needed to
improve the preparedness level against the resurgence of the disease.
The results demonstrate a high degree of preparedness levelagainstlevel against the
reemergence of Ebola Virus Disease in the three (3) LGAs of Lagos State. Majority of the
respondents who had heard about Ebola accepted that Ebola was real and could identify the
most common signs
Survey result reveals gaps on respondent’s knowledge in not participating in burial rites of a
person that dies of Ebola disease. Targeted public health messages are is required to raise the
knowledge level of the citizenry. , correct misconception and should be widely disseminated,
with radio and television as media of choice.
Furthermore,large Furthermore, a large numbers of respondents (from the study area) are now
acquainted with relevant steps to take in preventing the outbreak and consequent spread of
cvBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
EVD thus signifying an . This is an indication of improved level of awareness in the fight
against the disease. in tandem with positive practices regarding EVD.
Overwhelming agreement with intended behaviors such as isolation of those with symptoms,
early treatment and safe burial shows a new and emerging consensus akin to public health
recommendations. Perhaps Tthe most striking finding is the high degree of community
involvement in containing the scourge and the widespread effort at reaching out to family,
friends, and neighbors to imbibe the culture.
cviBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
RECOMMENDATIONS
The recommendations that will be cited here are in line with the findings of this study and
should be implemented by policy makers in the health sector. They are as follows:
1. The Government should increase awareness of the disease so as to reduce the
misconception especially amongst the people with low level of education as this also
affects their understanding of the disease.
2. In the practice towards EVD, the public should ensures good practice such as ensuring
high level of personal hygiene, good environmental sanitation, avoids eating bush
meats, practice safe sex, avoids pets especially monkeys, ensure good burial
procedure, wear protective clothing and help disseminate the information on Ebola.
3. Standard protocols should be developed and enforced by the Federal Ministry of
Health and state Ministries y of Health to ensure best practices at Primary Health Care
facilities. uniformity of practice at primary care facilities.
4. Majority of respondents in this study learnt about EVD from mass media sources,
health institutions from community level to federal level should device means of
transmitting reliable health information to staff.
5. Hand sanitizers should be provided freely for the populace.
cviiBabatunde Olowookere 910706002

Residents Preparedness Level Against Ebola Virus Disease Resurgence
REFERENCES
cviiiBabatunde Olowookere 910706002

1 .WHO/Ebola virus disease (EVD). Geneva: World Health Organization, 2014 (http://www
who.int/csr/don/archive/disease/ebola/en). 2014. (accessed Jan.10, 2015)
2 .World Health Organization Ebola Virus Disease fact sheet, September, 2014. Available at
http://www.who.int/mediacentre/factsheets/fs103/en/ 2014. (accessed Feb. 15, 2015)
3 .Centre for Disease Control. Ebola Virus Disease outbreak-Nigeria. Washington, D.C., 2014
Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6339a5.htm. 2014.
(accessed Feb.20, 2015)
4 .Ebola virus disease: fact sheet no.103 updated September 2014. Geneva: World Health
Organization(http://www.who.int/mediacentre/factsheets/fs103/en/). (accessed March
3,2015)
5 . .Borchert M, Mutyaba I, Kerkhove MDV, Lutwama J, Luwaga H, Bisoborwa G, et al.
Ebola Hemorrhagic Fever outbreak in Masindi District, Uganda: Outbreak description and
lessons learned. BMC infectious diseases, 2011, 11: 357 Available at
www.biomedcentral.com/14712334/11/357 (accessed March, 16, 2015).
6 . http://apps.who.int/ebola/en/status-outbreak/situation-reports/ebola-situation-report-
31-September-2015. (assessed September 6th 2015)7 . WHO/Ebola Situation Reports. app.who.int/ebola/ebola-situation-report (accessed April,
20, 2015).
8 . Pourrut X, Kumulungui B, Wittmann T, Moussavou G, Delicat A, Yaba P, et al.
The natural history of Ebola virus in Africa. Microbes infect 2005; 7: 1005. Available at
www.ncbi.nlm.nih .gov/pubmed/16002313 (accessed July 16, 2015).9
. Dixon MG, Schafer IJ, Centers for Disease C, Prevention, Ebola viral disease outbreak-West
Africa, 2014. MMWR Morb Mortal Widy Rep. 2014; 63 (25): 548-51.
10
. http://www.who.int/csr/dis ease/ebola/manual_EVD/en/ (accessed July 25, 2015)
11 .World Health Organization. Mali confirms its first case of Ebola.
http://www.who.int/mediacentre/news/ebola/24-october-2014/en/ (Accessed on July 25,

2015).
12 . WHO, “WHO: Air travel is low-risk for Ebola transmission,” Note for the Media, August
14, 2014 and WHO, “Statement on travel and transport in relation to Ebola virus disease
(EVD) outbreak, August 2, 2014.
13 .WHO Ebola Response Team, 2014.Ebola virus disease in West Africa-the first 9 months of
the epidemic and forward projections. N. Engl. J. Med. 371, 1481–1495,
http://dx.doi.org/10.1056/NEJMoa1411100.
14 . . www.worldometers.info/world-population/nigeria-population
15 . Emily HC, Timothy FB, Lawrence CM, Marjorie PP, Amy LS, Mikaela K, et al. Global
capacity for emerging infectious disease detection. Pnas.org.
2010http://www.pnas.org/content/107/50/21701.long (accessed August 2, 2015).
16 . Nicholas JB. Clinical review- Ebola Virus Disease. BMJ 2014: 349. G7348: doi:
http:dxdoi.org/10.1136/bmj.g7348 (accessed August 3, 2015)
17 17. . The WHO. Public Health Events of Initially Unknown Etiology: A framework for
Preparedness and Response in the Africa Region; WHO Regional Office for Africa: Geneva,
Switzerland, 2014. ISBN: 978-929-023-2476 (NLM ClassficationClassification:).
18. Bruce Clements. Disaster and Public Health Planning and Response
19 Mohanty, S., Panda, B., Karelia, H. & Issar, R. 2006. Knowledge Management in
Disaster Risk Reduction: The Indian Approach,20 . Tatham, P. & Spens, K. 2011. Towards a Humanitarian Logistics Knowledge
Management System. Disaster Prevention and Management, 20(1), pp. 6-26.
21 . Nonaka, I., Konno, N., and Toyama, R., 2000. Emergence of Ba, In: Nonaka, I., and
Nishiguchi, T. (Eds), Knowledge emergence: Social, technical and evolutionary dimensions
of knowledge creation, Oxford University press, Oxford.

22 . www. Who.int/hac/about/definitions/en/ (assessed August 3,2015.
23 . Nishiura, H. and G. Chowell, Early transmission dynamics of Ebola virus disease
(EVD), West Africa, March to August 2014. Euro surveSillance, 2014. 19(36): p. 5-10.
24 . http://www.pubfact.com/detail/24575870/Ebola-virus-vaccines-an-overview of current
approaches (accessed August 3, 2015).
25 Barrette, R.W., Metwally, S.A., Rowland, J.M., Xu, L., Zaki, S.R., Nichol, S.T. et al.,
2009, 'Discovery of swine as a host for the Reston ebolavirus', Science 325, 204-206.
http://dx.doi.org/10.1126/science.1172705, PMid:19590002.
26 Feldmann, H. &Geisbert, T.W., 2011, 'Ebola haemorrhagic fever', Lancet 2011; 377,
849862. http://dx.doi.org/10.1016/S0140-6736(10)60667-8
27 https:who.int/mediacentre/factsheets/fs103/en/#
28 WHO/
https://www.abdserotec.com/ebola-outbreaks-
research.html?utm_source=shared&utm_medium=referral&utm_campaign=page-copy-
copied-and-pasted
29 . Mari Saez, A., et al., Investigating the zoonotic origin of the West African Ebola epidemic.
EMBO molecular medicine, 2015. 7(1): p. 17-23.
30 . Kuhn JH. Filoviruses, a compendium of 40 years of epidemiological, clinical and
laboratory studies. New york: Springer Wien; 2008.
31 Reference: European Centre for Disease Prevention and Control.
http://ecdc.europa.eu/en/
(accessed on July 15, 2015)

32. Dixon MG, SchaferIJ, Centres for Disease control and prevention (CDC). Ebola Viral
Disease Outbreak West Africa.MMWR morbidity Weekly Report.2014:63(25) 548-51.
33 .WHO\ Ebola virus disease. WHO.http://www.
WWho.int/mediacentre/factsheets/fs103/en/ (accessed August 2, 2015).
34. Leroy, E.M.et al. Fruit bats as reservoirs of Ebola virus. Nature 438,575-576 (2005)
35 . S. F. Dowell, R. Mukunu, T. G. Ksiazek, et al. Transmission of Ebola hemorrhagic fever: a
study of risk factors in family members, Kikwit, Democratic Republic of Congo, 1995
36 .R. Colebunders, M. Borchert Ebola haemorrhagic fever-a review J Infect Dis, Volume 40,
2000, pp. 16-20
37 . Centers for disease control and prevention. Health advisory network 367: CDC Ebola
Response update. No 3, Available at http://emergency.cdc.gov/han/han 00367.asp (accessed
Aug. 4,2015
38 . Tarantola, A.; Abiteboul, D.; Rachline, A. Infection risks following accidental
exposure to blood or body fluids in health care workers: A review of pathogens transmitted
in published cases. Am. J. Infect. Control.2006, 34, 367–375. [Google Scholar] [CrossRef]
[PubMed].
39 Weingartl, H.M.; Embury-Hyatt, C.; Nfon, C.; Leung, A.; Smith, G.; Kobinger, G.
Transmission of Ebola virus from pigs to non-human primates. Sci. Rep. 2012, 2, 811.
[Google Scholar] [CrossRef] [PubMed]40
. Sagripanti, J.L.; Rom, A.M.; Holland, L.E. Persistence in darkness of virulent
alphaviruses, Ebola virus, and Lassa virus deposited on solid surfaces. Arch. Virol. 2010,
155, 2035–2039. [Google Scholar] [CrossRef] [PubMed].
41 . World Health Organization. Ebola response roadmap – situation report. ; December
31st, 2014 ([accessed 07.01.15])http://www.who.int/csr/disease/ebola/situation-reports/en/
(accessed Aug.5,2015).
42. Mike B, Daniel S, Martin SH, Jennifer M (EDS). Epidemiology and pathogenesis of

EVD. Available at http:// www. Update.com/content/epidandpathog September 04, 2014.
(accessed Aug. 10, 2015).
43 . Jahrling, P.B., et al., PRELIMINARY-REPORT - ISOLATION OF EBOLA VIRUS
FROM MONKEYS IMPORTED TO USA. Lancet, 1990. 335(8688):p. 502-505.
44 . Hofmann-Winkler, H., F. Kaup, and S. Poehlmann, Host Cell Factors in Filovirus Entry:
Novel Players, New Insights. Viruses-Basel, 2012. 4(12): p. 3336- 3362.
45 . Alimonti, J., et al., Evaluation of transmission risks associated with in vivo replication of
several high containment pathogens in a biosafety level 4 laboratory. Scientifi c Reports,
2014. 4.
46 . Jahrling, P.B., et al., PRELIMINARY-REPORT - ISOLATION OF EBOLA VIRUS
FROM MONKEYS IMPORTED TO USA. Lancet, 1990. 335(8688): p. 502-505.
47 . Kreuels B, Wichmann D, Emmerich P, et al. A case of severe ebola virus infection
complicated by gram-negative septicemia.NEngl J Med 2014; 371-2394.
48. Feldmann H, Geisbert TW. Ebola hemorrhagic fever. Lancet 2011; 377:849.
49 . Bray M, Geisbert TW. Ebola virus: the role of macrophages and dendritic cells in
pathogenesis of Ebola haemorrhagic fever. Int J Biochem cell Biol 2005; 37: 1560
50 . Hensley LE, Young HA, Jahrling PB, Geisbert TW.Proinflammatory respond during
Ebola virus infection of primate models : Possible involvement of the tumor necrosis factor
receptor superfamily. Immunol let 2002; 80:169.
51 . Hensley LE, Young HA, Jahrling PB, Geisbert TW.Proinflammatory respond during
Ebola virus infection of primate models : Possible involvement of the tumor necrosis factor
receptor superfamily. Immunol let 2002; 80:169.
52 . . Hensley LE, Young HA, Jahrling PB, Mechanisms underlying Coagulation
abnormalities in ebolahaemorrhagic fever: Overexpression of tissue factor in primate
monocytes/macrophages is a key event. J Infect Dis 2003; 188:161853
. Bray M, Murphy FA. Filovirus research: Knowledge expands to meet a groing threat.
J Infact Dis 2007;196Supp 12: S438.

54. Mahanty S, Hutchinson K, Agarwal S, et al. Cutting edge: Impairment of dendritic
cells and adaptive Immunity by Ebola and lassaviruss. J Immunol 2003; 107: 2797.55
. Baize S, Leroy EM, Georges-Courbot MC, et al. Defective humoral response and extensive
intravascular apoptosos are associated with outcome in Ebola virus-Infected Patients. Nat.
Med. 1999, 5:423.
56 . Geisbert TW, Hensly LE, Gibb TR, et al. Apoptosis induced in vitro and vivo during
infection by Ebola anad Marburg viruses. Lab Invest 2000; 80:171.
57. Brandfute SB, Warfield KL, Bavari S. Functional CD8+ T cell response in Lethal
Ebola virus infection.J Immunol 2008; 180-4058.
58. Baylor College of Medicine Ebola Virus (Online).September 2014.Available from:
URL:https://www.bcm.edu/departments/molecular virology andm microbiology/emerging infections
and biodefense/ebola-virus (accessed Aug.18, 2015).
59. WHO/Ebola vaccine, therapies and diagnostics. WHO. http://
www.who.int/cst/disease/ebola/fag-ebola/en (accessed Aug. 20,2015)
60 .http://apps.who.int/ebola/en/status-outbreak/situation-reports/ebola-situation-report-31-
September-2015. (assessed September 6th 2015)61 . WHO | Ebola virus disease. WHO.
http://www.who.int/mediacentre/factsheets/fs103/en/ (accessed Aug. 22, 2014).
62 . WHO, One Year into the Ebola Epidemic: Factors That Contributed to Undetected Spread
of the Ebola Virus and Impeded Rapid Containment, January 2015, p.4-5.
63 . .WHO, WHO Risk Assessment: Human Infections with Zaïre Ebola virus in West Africa,
June 24, 2014.
64 . .WHO, One Year into the Ebola Epidemic: Factors That Contributed to Undetected Spread
of the Ebola Virus and Impeded Rapid Containment, January 2015, p.18.

65 . .CDC, Morbidity and Mortality Weekly Report: Estimating the Future Number of Cases in
the Ebola epidemic—Liberia and Sierra Leone, 2014 – 2015, September 26, 2014.
66 . .UN News Centre, West Africa ‘on brink’ of major food crisis in the wake of Ebola
outbreak – UN expert, November 11, 2014
67 . http://apps.Who.int/iris/bitstream/1065/1315961/Ebola Response Roadmap.pdf (accessed
September 10, 2015).
68 . . Cdc and prevention. Ebola virus disease outbreak. Nigeria, July to September 2014.
http:// www.cdc.gov/mmwr. October 2014.
69 . .Mwesiga A. Reporting epidemics: newspapers, information dissemination and the story of
Ebola in the Ugandan district of Luweero. Pan Afr Med J 2011; 9: 43.
70 .WHO/ Ebola Virus disease. WHO.
http://intranet.who.int/sites/evd/documents/ecrecommendations prearedness.pdf
71 Landesmann LY. Public Health Management of Disasters: The Practice Guide.
Washington, DC: APHA, 2001.
72 . . WHO, 2007. Standard precautions in health care AIDE-MEMOIRE. World Health
Organization, Geneva, 2007; Available from:
http://www.who.int/csr/resources/publications/standardprecautions/en/ (accessed September
03, 2015).
73. International Health Regulations. (2005), Second edition. Geneva, World Health
Organization, 2008 (http://www.who.int/ ihr/9789241596664/en/, accessed September 5th,
2014).
74 .Tierney K, Lindell MK and Perry RW (2001) Facing the Unexpected: Disaster
preparedness and response in the United States. Washington, DC: Joseph Henry Press75
Centers for disease control and prevention. Outbreaks Chronology : Ebola virus
Disease, Known cases’ and outbreak of Ebola virus Disease in Disease in revers
chronological order: Available at
http://www.cdc.gov/vhf/ebola/outbreaks/history/chro nology.html . (accessed September 03,

2015).
76 Monasch R. Public Knowledge, Attitudes, and Practices study relating to Ebola Virus Disease Prevention and medical care in Sierra Leone 2014.
77 UNICEF, CRS, FOCUS 1000. Study on Public Knowledge, Attitude and practice
relating to EVD prevention and medical care in Sierra-Leone. Available at
http://newwire. crs.org/wp-content/uploads/2014/no/ebola-virus-di sease-national-kap-study-
final-report-final.pdf. (assessed October 30th 2014).
78 Fisher M, Kietzing M. Is sensitization effective in changing behavior to prevent Ebola
transmission. Available at www.start-network.org (assessed November 3rd 2015).
79 National Knowledge, Attitudes And Practices Study On Ebola Virus Disease In
Liberia.
Available at www.unicef.org/cbsc/file /KAP-study-Liberia -March 2015-pdf (assessed
November 5th 2015)
80 Vailaya CGR, Kumar S, Moideen S, Ebola virus disease; knowledge, attitude and
practices of health care professionals in a tertiary care hospital.; J Pub health med res
2014;2(12):13-18. (assessed 30th October, 2015).
81 .Lagos State Government. 2013; published online Sept 1. http://www.lagosstate.gov.ng.
82 . Oyeyemi A, Ogunnowo B, Odukoya O. Patent Medicine Vendors in Rural Areas of
Lagos Nigeria: Compliance with Regulatory Guidelines and Implications for Malaria
Control. Trop J Pharm Res 2014; 13: 163–9.
83 . Lagos State Bureau of Statistic 2005
84 . Miaoulis, George, and R. D. Michener. (1976). An Introduction to Sampling. Dubuque,
Iowa: Kendall/Hunt Publishing Company.
85 . Gidado S, Oladimaji AM, Roberts AA, Nguku P, Nwangwu IG, Waziri NE, “et al”.
Public Knowledge, Perception and Source of Information on Ebola Virus Disease.
86 .. Kriger N, Williams DR, Moss NE. Mesuring social class in US public health research.
Annu Rev Public Health 2005; 18:341-78.

87 . ES Hwang. Preparedness for Preveventation of Ebola Virus Disease. J Korean Med Sci.
2014;29(9):1185 [PMC free articule] [PubMed].
88 .M Ki. What do we really fear? The epidemiological Characteristics of Ebola and our
preparedness. Epi Heal. 2014;36 doi.10.4178/epih/2014 [PMC free articule] [PubMed]89
. International Federation of Red Cross and Red Crescent Societies. Emergency Plan of
Action (EPoA) Liberia: Ebola Virus Disease; April, 2014.
90ES Hwang. Preparedness for Preveventation of Ebola Virus Disease. J Korean Med Sci.
2014;29(9):1185 [PMC free articule] [PubMed]91.M Ki. What do we really fear? The epidemiological Characteristics of Ebola and our
preparedness. Epi Heal. 2014;36 doi.10.4178/epih/2014 [PMC free articule] [PubMed]92 . International Federation of Red Cross and Red Crescent Societies. Emergency Plan of Action
(EPoA) Liberia: Ebola Virus Disease; April, 2014.93. Bourque,L.B.,D.S. Mileti, M. Kano, and M.M. Wood. 2012. Who prepares for
terrorism? Environment and Behavior 44:374-409.
http://dx.doi.org/10.1177/0013916510390318 (assessed Sept. 26th, 2015).
94 . Menard, L. A., R. O. Slater, and J. Flaitz. 2011. Disaster preparedness and education
attainment. Journal of Emergency Management 9:45-52.
95 . Frankenberg, E., B. Sikoki, C. Sumantri, W. Suriastini, and D. Thomas. 2013. Education,
vulnerability, and resilience after a natural disaster. Ecology and Society 18(2): 16.
http://dx.doi.org/10.5751/ES-05377-180216.

Figure 41: Overview of Ebola virus pathogenesis