Diseases of the breast
Diseases of the breastDr. Mohammed HajhamadMB.ChB. (Egypt) M.S
(Malaysia)Department of SurgeryInternational Medical
SchoolManagement and Science University
1Diseases of the Breast
Contents IntroductionCongenital anomalies Breast traumaMastitis
and breast abscessChronic inflammatory conditionsFibrocystic
disease of the breastCysts of the breastBreast neoplasms Male
breast12 February 20162
Introduction Breasts are modified sweat glandLie between skin
and pectoral fasciaFrom 2nd to 6th ribFrom lateral border of
sternum to anterior axillary line.May extends:upwards till
clavicledownwards till below costal marginmedially to
midlinelaterally to posterior axillary lineBreast tail 12 February
20163
Introduction Components:Epithelia elements:Responsible for milk
secretion and transport.Supporting tissue:Fibrous septa, extend
from pectoral fascia to skin, they divides the parenchyma into
lobes.
12 February 20164
Introduction Arteries:IMALateral thoracic art.Pectoral branch of
acromio-thoracic art.Intercostal perforatorsVeins:Axillary and
internal mammaryIntercostal veins Azygos Vertebral venous plexus.
(importance) 12 February 20165
Breast lymphatics There are about 35 LNThree main groupsAxillary
(75%)Pectoral, subscapular, lateral, interpectoral, central and
apical.Internal mammary3-4 LN along internal mammary vessels.
12 February 20166
Physiology of the breastHormonal controlOestrogen, adrnocortical
steroids and growth hormone development of ducts.Progesterone
growth of lobules.Prolactin formation of alveoli12 February
20167
Physiology of the breastPhysiological changesPuberty: cyclical
hormonal activity growth, branching of the ducts and formation of
ductules.Menstrual changes: there will be cyclical changes with
heaviness, discomfort, increased nodularity.Lactation: -Drop in
oestrogen, increase sensitivity to (prolactin, GH and cortisol)
milk production.- Suckling stimulate prolactin and oxytocin milk
ejection.Menopause: the lobules gradually disappear. 12 February
20168
Congenital anomalies of the breast
12 February 20169
Congenital anomaliesNipple Athelia: absence of the nipple. Rare,
usually associated with (Amazia)Polythelia: supernumerary nipples
occurs anywhere along mammary ridges, from axilla to groin. 12
February 201610
Congenital anomaliesBreast Amazia: absence of breast. Usually
unilateral.Polymazia: supernumerary breasts, due to persistence of
extramammary portions of the mammary ridge.Infantile gynecomastia:
diffuse enlargement of male breast. Bilateral or unilateral. Due to
maternal sex hormones. Usually disappears within six months. 12
February 201611
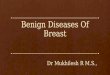
Bilateral athelia and unilateral amazia
12 February 201612
Polythelia and polymazia
12 February 201613
Trauma Results in two sequencesBreast hematomausually deeply
seatedhard massresembles a carcinoma Traumatic fat necrosisdeath of
fat cells fatty acids combine with calcium calcium soap.- cyst
contains thick oily fluid- hard mass resembles carcinoma-
differentiation is by biopsy.12 February 201614
Acute lactational mastitis and breast
abscessAetiology:Staphylococcus aureus clotting of milk in the
ducts obstruction stasis.Organism reaches the ducts from the
suckling infant mouth through a cracked nipples.Predisposing
factors:1- milk engorgement2- abrasions to the nipples by
suckling3- poor hygiene
12 February 201615
Acute lactational mastitis and breast abscessPathology: milk
engorgement diffuse inflammation not treated acute mastitis
abscess. Predisposing factors:1- milk engorgement2- abrasions to
the nipples by suckling3- poor hygiene
12 February 201616
Acute lactational mastitis and breast abscessClinical picture
Dull aching pain, pyrexia, breast in engorged and tender.Acute
mastitis: high fever, sever tenderness and redness.Acute abscess:
throbbing pain, hectic fever, localized signs, pitting edemaChronic
abscess. 12 February 201617
Diffuse mastitis and abscess
12 February 201618
Treatment Before development of abscess:- systemic antibiotics
covering staph. (pencillin, cephalosporin)- breast support, reduces
pain- local heat- advice breast emptying (breast bump) and or
bromocriptine 2.5 mg BD.Abscess: - drainage under anesthesia- US
guided aspiration12 February 201619
Chronic inflammatory conditionsMammary duct ectasiaChronic
abscessTuberculosis 12 February 201620
Mammary duct ectasiaUnknown aetiologyDilatation of major ducts,
filled with creamy secretion with periductal inflammation.May be
asymptomatic, or- nipple discharge (bloody, serous, creamy white or
yellow.- retracted nipple- acute inflammation- recurrent chronic
inflammation with abscess formation.Treatment: surgical excision of
the major duct. Correction of nipple retraction.
12 February 201621
Chronic breast abscessResult from improper treatment of an acute
abscess.The abscess is treated with prolonged antibiotics rather
than adequate surgical drainage.Its called antibioma where is
bacteria is killed, but, pus remains in the breast with excess
fibrous tissue formation.The breast will be thickened and
honeycombed with pus. There will nipple retraction and skin
puckering. Treatment is excision (not incision). 12 February
201622
Tuberculosis of the breast Rare diseaseUsually associated with
PTB or cervical TB.Presents as either multiple cold abscess or
sinuses, or nodules.Axillary LN are enlarged and matted.Diagnosis
by biopsy (granulomma)Treatment with antituberculous
drugs.Mastectomy for resistant cases only. 12 February 201623
Fibrocystic disease Also known as mammary dysplasia, ANDI,
fibroadenosis and chronic interstitial mastitis.Aetiology
unknownAge 30-50 years, related to ovarian activity.It represent a
variation or aberration of normal changes during menstrual cycles,
pregnancy, lactation and menopausal involution. Aberration of
Normal Development and Involution ANDI12 February 201624
Pathology Upper outer quadrant One or a mixture of the
following:Adenosis: glandular hyperplasiaEpitheliosis: solid
epithelial hyperplasia within the small ducts. If atypical
hyperplasia noted a higher chance to develop cancer. Fibrosis:
replacement of elastic and fatty tissue with fibrous tissue.Cyst
formation: lined by epithelium and filled with clear yellow or
brown fluid. (late menopausal age). 12 February 201625
Clinical pictureAsymptomaticPalpable lump, may disappear if
patient re-examined one week after menstrual cycle.Painful
nodularity: multiple painful small lumps related to menstrual
cycle.Mastalgia: usually cyclical, premenstrual, accompanied by
enlargement and increased nodularity of the breasts.Nipple
discharge: clear, yellow, brown or green. 12 February 201626
Investigations USG and mammogramCytology of aspirated fluid,
however, not conclusive.If solid mass FNACExcisional biopsy if FNAC
not available or inconclusive.12 February 201627
Treatment It should be individualizedExclusion of malignancy and
reassurance is the most importantCysts: can be treated by
aspiration, if recur, excision.Cyclic Mastalgia: Mild: breast
support, day and night, reduce cafeen.Moderate: prolactin inhibitor
e.g. bromocriptin.Sever: synthetic androgen, e.g. Danazol. 100 200
mg BD. Atypical cells found in biopsy patient should be instructed
to perform monthly SBE and regular follow up. 12 February
201628
Neoplasms of the breast
12 February 201629
Neoplasms of the breastBenignMalignant EpithelialDuct
papillomaEpithelialCarcinomaMixed (epith +
mesenchymal)FibroadenomaMixed (epith +
mesenchymal)LymphomaFibrosarcoma
12 February 201630
Duct papillomaBenign tumor from epithelial lining of main ducts
near the nippleIts can be either a lump or an ulcerated mass with
bleeding discharge and bloody nipple discharge.Can cause a
retention cyst if the duct is totally blocked.
12 February 201631
Clinical featuresBloody or bloody stained nipple discharge.A
lump deep or near the areola. Pressure on it causing nipple
discharge.Sometimes, there is no swellings palpable, only discharge
on pressure.12 February 201632
Management Ductography the lesion will be shown as a filling
defect.Treated by excision of the affected duct (microdochectomy),
send specimen to HPE.12 February 201633
Fibroadenoma Its a benign neoplasm of the breast which affects
both the fibrous and the glandular tissues, but fibrous element
predominates. The most common breast mass in young womenAge from
15-30 yearsIt can be hard (pericanalicular), tend to be small, or
soft (intracanalicular), tend to be large.Solitary or multiple,
smooth surface, lobulated, well circumscribed, never attached to
surrounding tissues.Cut section shows whorled white fibrous tissue
which bulges out of its surface.12 February 201634
Clinical featuresHard type occurs in 20-30 years oldSoft type in
30-50 years oldUsually painless lump(s) which is indecently
discovered.Its small, nontender, spherical, firm, well
circumscribed, with smooth surface.High mobility is characteristic
feature (breast mouse).12 February 201635
Investigations Exclude malignancyUSG or
mammography.FNACTreatment:Excision and HPE to confirm diagnosis.12
February 201636
12 February 201637
Phylloides tumor Its a high cellular type of fibroadenoma which
tends to grow rapidly.Its named like that because the cut surface
resembles a leaf or fern.Its rarely malignant.Can grow as big as
20-30 cm.Its not attached to skinTreatment is wide local
excisionMastectomy for huge tumor occupying the whole breast.
12 February 201638
12 February 201639
Carcinoma of the breast
12 February 201640
Carcinoma of the breast1 out of 8 women is expected to develop
breast cancer sometime in her life.Its the most common cancer in
women.Risk increases with age60 is the mean age of occurrence.
12 February 201641
Aetiology Genetic factors: 5-10%BRCA 1 (chrom 17)BRACA 2 (chrom
13)Mother or sister BC 2.3 times riskMother and sister BC 14 times
riskEndocrine factors: - early menarche 30- late menopause >50-
contraceptive pills, Unsure relationship.12 February 201642
Aetiology Precancerous lesions:- epithelial hyperplasia and duct
papilloma 1.5-2 times- atypical epithelial hyperplasia 2-5 times-
lobular or ductal carcinoma insitu 5-10 times.Obesity: - high fatty
diet- steroidsPrevious affection of breast cancer in one side.12
February 201643
Pathology 12 February 201644
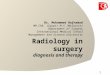
Gross typesSchirrhous carcinoma (hard), 75%Encephaloid carcinoma
(brain-like), large, soft and brain-like.Inflammatory carcinoma:
rare, most malignant, infiltrating duct carcinoma resembles
mastitis.Pagets disease: rare, intraductal carcinoma at the
epithelium of a main lactiferous duct which then spreads to both
skin and breast. There is nipple erosion. Mimics eczema. Carcinoma
of the ductsCarcinoma of the lobulesPagets diseaseNon-infilitrating
(in situ)Non-infilitrating (in situ)Intraductal carcinoma (1%)IDC
(75%)ILC (25%)
12 February 201645
SchirrhousinflammatoryPagets
Spread Local spread: inside the breast, skin, muscles of chest
wall and chest wall.Lymphatic spread: - by embolism or permeation.
- Mostly to axillary LN then internal mammary LN. - Supraclavecular
LN involvement considered advanced disease. - Blockade of cutaneous
lymphatics causes edema and pitting of breast skin, i.e. peau
dorange12 February 201646
12 February 201647
Spread Blood stream spread: lungs, liver, bones, brain and bones
(axial skeleton) (posterior intercostal vein and paravertiberal
plexus of veins)
12 February 201648
Hormonal receptor statusOestrogen-positive (ER-positive): 60% of
tumors have a receptors for oestrogen, they get more active under
its influence. Can be suppressed by reduced estrogen or giving an
anti-estrogen agents.Progesteron-positive PR-positive tumorsER-PR-
negative, 10 % 12 February 201649
Clinical featuresSymptoms: Accidental painless lumpPricking
pain, nipple retraction or bloody nipple discharge.Presents with
metastasis, axillary lump, backache, pathological fractures,
dysponea, pleuritic pain, jaundice or mental changes.During
screening programs12 February 201650
Clinical featuresSigns Examination should be done while upper
half of the patient exposed, both breasts, axillae, arms,
supraclavicular regions all examined. Breast: - asymmetry-
enlargement- skin dimpling- skin puckering- peau dorange- skin
nodule- skin ulceration12 February 201651
Clinical featuresMass:- hard- irregular- ill-defined- restricted
mobility within breast substance- fixation to skin, muscles, chest
wallNipple:- recent retraction- change of direction12 February
201652
Clinical featuresAxillary and supraclavicular nodes- number and
mobility of nodesDistant metastasis:- chest examination-
hepatomegaly- ascitis- pelvic examination for hard deposits or
Krukenberg tumor. 12 February 201653
Clinical featuresPagets disease:- pricking sensation of the
nipple- superficial erosion- a tumor mass may not be palpable-
commonly mistaken for eczema- biopsy is mandatory to differentiate.
Inflammatory carcinoma:- usually occurs during pregnancy or
lactation- rapidly growing, sometimes painful breast swelling.-
overlying skin is reed, edematous and warm.- resembles acute
mastitis- poor prognosis12 February 201654
Clinical featuresCarcinoma in situ- LCIS: found by mammogram and
confirmed by biopsy. Doesnt progress to invasive type.- DCIS:
present as a mass or in mammogram, should be treated by surgery.12
February 201655
Differential diagnosis
CarcinomaCystFibro-cysticfibroadenomaAge>3535-5535-5515-30PainPainlessOccasionallyOccasionallyPainlessSurfaceIrregularSmoothIndistinctSmooth,
lobulatedConsistencyHardSoft to hardFirmFirm, highly mobileLN+/-
axillay LN+Free axillaFree axillaFree axilla
12 February 201656
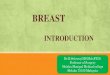
Staging TNM stagingManchester staging12 February 201657
TNM Staging
12 February 201658
13 February 201659
Investigation Aims:Diagnosis (USG, mammogram + HPE)Staging
(CXR+USG abdomen), CT scan, alkaline phosphatase.Special situation:
bone scan (bone pain) and brain CT scan. 12 February 201660
Investigations Tools Mammography: 95% accurate. Usually combined
with tru cut biopsy or FNAC. - dense opacity with indefinite
outlines- clustered microcalcifications.- less effective below age
of 35Ultrasonography: can differentiate between solid and cystic.
Used in young women where mammogram is not helpful.Biopsy:-
Excisional - frozen section biopsy- tru-cut biopsy- FNAC12 February
201661
Early detectionBreast self examination (BSE)Screening programs.-
Clinical examination and a mammogram. - Proven to reduce mortality,
early detection and more conservative surgery. 12 February
201662
Treatment Provided through an MDTDepends on stage of the
diseaseEarly vs. AdvancedEarly: any T2 N1 M0 or below, stage
I&II(localized disease +/- micrometastasis)Primary treatment:
Surgery +/- radiotherapyAdvanced: more than T2 N1 M0, stage
III&IV (systemic disease)Primary treatment: Chemotherapy and
endocrine therapy12 February 201663
Early cases
12 February 201664
Surgical optionsRadical mastectomy (Hasted mastectomy), whole
breast tissue pectoralis muscles+ all axillary LN are
cleared.Modified radical mastectomy (Patey), preserve the
pectoralis muscles, usually followed by radiotherapy.Breast
conservative surgery: combined surgery and radiotherapy: