Embed Size (px)
Citation preview
Dr. Bibek raj parajuli

Forensic Toxicology: deals with the medical & legal aspects of the harmful effects of the chemicals on human being.
(Father of Toxicology: Matthew Joseph Orfila– Spanish chemist)
Poison: Any substance, which when introduced into the living body, or brought into contact with any part thereof, will produce ill-health or death by its local or systemic action or both.
“All substances are poisons;
There is no such thing as a non poison”.
Ideal homicidal poison should be: -cheap
-easily available
-colourless, odourless & tasteless
-capable of being easily administered in food/drink without any suspicion
-highly toxic
-s/s resembling natural d/s or delayed
-shouldn’t be detected by chemical tests
-no postmortem changes
-rapidly destroyed or made undetectable by the body
*IDEAL HOMICIDAL POISONS: Organic compounds of Flourine & thallium.
*COMMONLY USED: Arsenic & Aconite.
Ideal suicidal poison should have following
properties:
-cheap
-easily available
-highly toxic
-tasteless/pleasant taste
-capable of being easily taken in food/drink
-capable of producing painless death
*IDEAL SUICIDAL POISONS: Opium & Barbiturates.
*COMMONLY USED: Organophosphorous & Endrin.
3. Stupefying: Dhatura, Cannabis indica, Chloral hydrate.
4. Abortifacient: Calotropins, Oleander, Aconite, Lead, Mercury, Arsenic, Potassium permanganate.
5. Accidental: Household poisons.
6. Cattle poisoning: Oleander, Aconite, Arsenic, Zn-phosphide.
7. Arrow poisons: Snake venom, Aconite, Curare etc.
8. Aphrodisiacs: Opium, Cannabis, Cocaine, Strychnine, Arsenic.

A.CORROSIVES :
1. Strong Acids:
i. Mineral acids: H2SO4, HNO3, HCL
ii. Organic acids: oxalic, carbolic, acetic, salicylic
2. Strong Alkali: hydrates & carbonates of Na, K, NH4
3. Metallic Salts: ZnCl2, CuSO4, KCN, FeCl3
B. IRRITANTS:
1. Agricultural: Organophosphorous, Organochlorines
2. Inorganic:
i. Non-metallic: K, I, Cl, Br, CCl4
ii. Metallic: As, Cu, Pb, Hg, Zn
iii. Mechanical: Powdered glass, Diamond dust
3. Organic:
i. Vegetable: Abrus precatorious, Calotropins
ii. Animal: Snake & Insect venom, Cantharides

C. SYSTEMIC:
1. Cerebral:
i. CNS depressants: Alcohols, Opioids, Sedatives,
Hypnotics.
ii. CNS stimulants: Amphetamines, Caffeine,
Antidepressants
iii. Deliriants: Dhatura, Belladona, Cannabis, Cocaine 2. Spinal: Nux vomica, Gelsemium
3. Peripheral: Conium, Curare
4. Cardiovascular: Aconite, Quinine, Oleander, Aconite,
Tobacco
5. Asphyxiants: CO, CO2, H2S
D. MISCELLANEOUS: - Food poisoning/botulism

1. Fulminating: is produced by a massive dose, death occurs rapidly, sometime without preceding symptoms.
2. Acute: caused by excessive single dose or several smaller doses of poison taken over a short interval of time.
2. Chronic: caused by smaller doses over a period of time, resulting in gradual worsening.
3. Subacute: shows features of both acute & chronic poisoning.

1. Immediate resuscitative measures
A. Airway
B. Breathing
C. Circulation
D. Correction of CNS depression
2. Removal of unabsorbed poison from the body
A. Inhaled poison
B. Injected poison
C. Contact poison
D. Ingested poison- gastric lavage/emesis
“Treat the patient and not the
poison”
Useful within 3 hours after ingestion of poison
By using stomach tube (Ewald’s or Boa’s tube) or ordinary soft, non collapsible rubber tube of L=1.5 m D= 1 cm with a glass funnel attach on one end and a mark at 50 cm from the other end which should be rounded with lateral openings.
Denture must be removed and mouth gag placed.

Patient in left lateral position or head hanging over edge of the bed and face supported by assistant.
The end is lubricated with olive oil/glycerine & is slowly passed into mouth & through the pharynx & oesophagus into the stomach till the 50cm marking.(confirm)
About 300ml of lukewarm water should be passed through the funnel held high above the patient’s head.


This 1st stomach contents should be preserved for chemical analysis.
Gastric lavage can be done with-
-water,
-1:5000 potassium permanganate,
-5% Sodium Bicarbonate,
-4% Tannic Acid,
-1% Sodium/Potassium Iodide,
-0.9% Saline.
Repeat the wash with ½ li. suitable solution till
clear & odourless fluid comes out
Contraindications of gastric lavage:
Absolute- corrosive poisoning (except carbolic acid)
Relative-
i.convulsant poisoning,
ii.comatose patient,
iii.volatile poison,
iv.upper GIT disease,
v.patient with marked hypothermia and haemorrhagic diathesis
Caution: In drowsy or unconscious patient, INTUBATE before you attempt gastric lavage.
Should be used only if stomach tube is not available.
Ipecacuanha powder 1-2 grams or 30 ml syrup (10-15ml for children) followed by several glasses of water.
Household emetics :15 grams mustard powder or 2 tsp common salt in 200 ml of lukewarm water (not effective)
Contraindications: i. Severe heart and lung disease
ii. Advanced pregnancy
iii. Same as for stomach wash
3.Administration of antidotes:
A. Mechanical or physical antidotes-
(Neutralize poison by mechanical action or prevent their
absorption)
i. Activated charcoal
ii. Demulcents- (forms coating)
eg. milk, barley-water, starch,
egg white, mineral oil
iii. Bulky food- for glass particles.
iv. Diluents- water
B. Chemical antidotes- (Counteract the action of poison by forming harmless or
insoluble compounds or by oxidizing poison when brought in contact with them)
eg. 1.Common salt for Ag NO3,
2.Egg albumin for HgCl3,
3.Dialysed iron for As,
4.CuSO4 for phosphorous,
5.1:5000 solution of Potassium permanganate,
6.Tannic acid 4% for nicotine, cocaine, aconite etc
7.Weak alkali for acids.
8.Weak vegetable acids for alkalis.
C. Universal Antidote: it is the combination of:
i. Activated charcoal (2 parts)- adsorbs poison.
ii. Magnesium oxide (1 part)- neutralizes acid without gas formation.
iii. Tannic acid (1 part)- precipitates alkaloids & many metals.

D. Physiological or Pharmacological antidotes:
Produce signs & symptoms exactly opposite to those
caused by the poison)
eg. Atropine & Physostigmine.
Barbiturates & Amphetamines,
Strychnine & Barbiturates,
Naloxone & Morphine
E. Chelating Agents: (Metal Complexing Agents)
- are used for heavy metal poisoning.
- have greater affinity for metals as compared to the endogenous enzymes.
- complex of metal & the agent is more water soluble than the metal, so there is higher renal excretion of the complex.
1. B.A.L
2. E.D.T.A
3. Penicillamine
4. D.M.P.S
5. D.M.S.A
6. Desferrioxamine
metal
metal
1. B.A.L ( Dimercaprol )
For As, Pb, Hg, Cu, Au etc.
Dose: 3 - 4 mg/kg
Shouldn’t be used when liver is damaged.
May induce haemolysis in G-6-PD deficient individuals.

2. E.D.T.A For Pb, Hg, Cu, Co, Cd, Fe, Ni etc.
Dose: 25-35mg/kg in 250-500ml 5% dextrose/NS i.v. over a
period of 1-2 hr twice daily for 5 days and may be
repeated after 2 – 3 days.
3. Penicillamine (Cuprimine)
A hydrolysis product of penicillin.
Chelating agent of maximum efficiency for heavy
metals.
Dose: 30mg/kg up to 2gm/day in 4 divided doses
orally for 7 days.

4. Elimination of poison by excretion:
Indications:
i. Severe poisoning.
ii. Progressive deterioration inspite of full supportive
care.
iii. High risk of serious morbidity or mortality.
iv. If normal route of excretion of toxins is impaired.
v. when the poison produces serious delayed toxic
effects.
vi. If the patient has CVS, respiratory or other d/s.
a. Increasing renal excretion:
Large amount of fluid, tea, lemonade orally,
Urinary alkalinisation for salicylates & phenobarbital.
b. Purging:
-30gm Sodium sulphate with large amounts of water hastens poison elimination in stool.
c. Whole-bowel irrigation:
-with polyethylene glycol with electrolyte lavage solution.
d. Diaphoretics:
- increases perspiration.
- 5mg of Pilocarpine nitrate s.c
e. Forced alkaline diuretics:
- achieving urinary pH of 7.5 to 9 promotes excretion of drugs that are weak acids (eg. Salicylates, phenobarbital)
- Sodium bicarbonate 50 to 100 meq added to 1 li of 0.45% saline administered 250- 500ml/hr
f. Peritoneal Dialysis:
- for alcohols, barbiturates, chloral hydrate, lithium etc
g. Haemodialysis:
- for ethanol, methanol, chloral hydrate etc
h. Charcoal Haemoperfusion:
-for barbiturates, salicylates, phenytoin etc
5. Symptomatic treatment:
-symptoms should be treated on general lines.
-adoption of general measures to support the life of the patient.
6. Adequate follow-up:
-to treat complication if any.
-in suicidal cases, psychiatric treatment is needed.

http://www.dda.gov.np/uhn.php

1. Quantity of the poison.
2. Physical form- Gaseous or volatile poisons are rapidly absorbed
and show quick action.
3. Chemical form- Pure metallic arsenic or mercury are not highly
toxic but different compounds of these metals are deadly poisons.
4. Concentration- Usually greater the concentration more will be the
effect except oxalic acid which is more rapidly absorbed in dilute form.
5. Contents of the stomach- Presence of food delays absorption
except phosphorus where fatty food enhances absorption.
6. Route of administration
7. Age of individual – Opium and its alkaloids are better tolerated by elderly whereas belladonna group of drugs are better tolerated by children.
8. Presence of any disease
9. Cumulative action of poisons – leads to chronic toxicity on long term exposure.
10. Idiosyncrasy
11. Tolerance
In Living Subjects
1. History
2. Clinical Examination
3. Laboratory tests – e.g. blood, urine, stool, vomitus,
stomach wash contents.

In the Dead:
(i) History from relatives and attendants
(ii) Relevant papers
(a) FIR
(b) Inquest report
(c) Hospital documents
(d) Investigation reports
(iii) Post mortem examination
(iv) Toxicological analysis of Viscera.
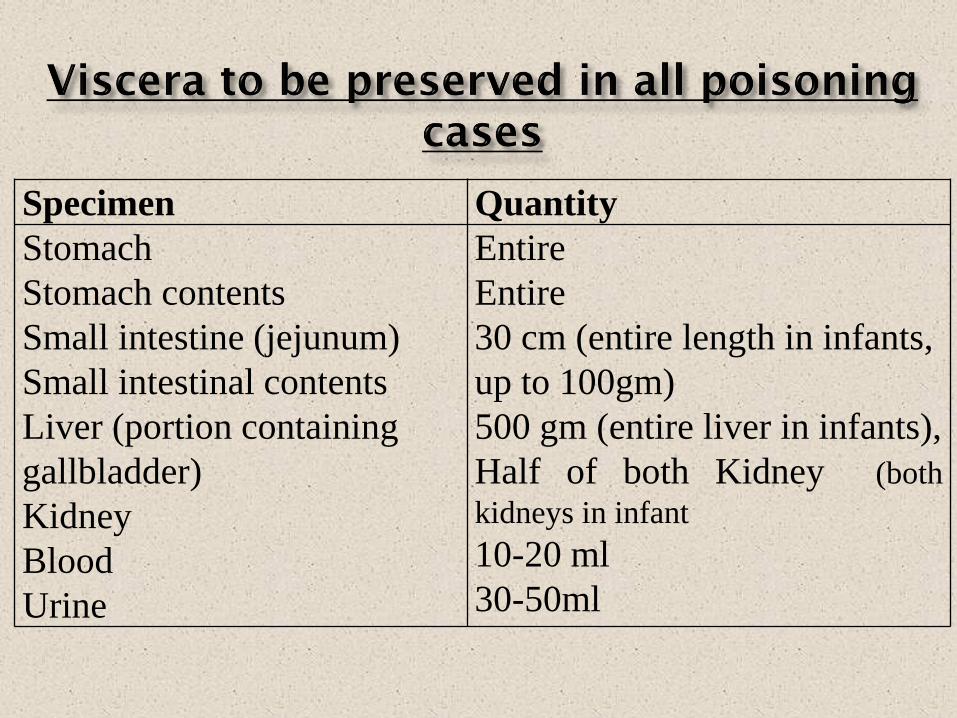
Specimen Quantity
Stomach
Stomach contents
Small intestine (jejunum)
Small intestinal contents
Liver (portion containing
gallbladder)
Kidney
Blood
Urine
Entire
Entire
30 cm (entire length in infants,
up to 100gm)
500 gm (entire liver in infants),
Half of both Kidney (both
kidneys in infant
10-20 ml
30-50ml
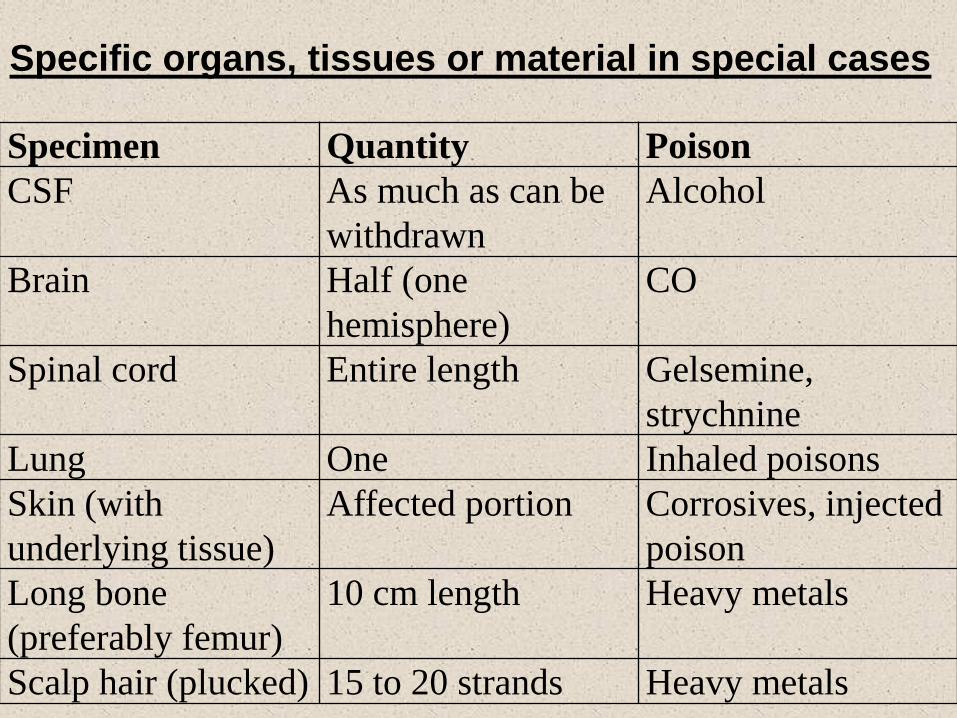
Specimen Quantity Poison
CSF As much as can be
withdrawn
Alcohol
Brain Half (one
hemisphere)
CO
Spinal cord Entire length Gelsemine,
strychnine
Lung One Inhaled poisons
Skin (with
underlying tissue)
Affected portion Corrosives, injected
poison
Long bone
(preferably femur)
10 cm length Heavy metals
Scalp hair (plucked) 15 to 20 strands Heavy metals
Specific organs, tissues or material in special cases
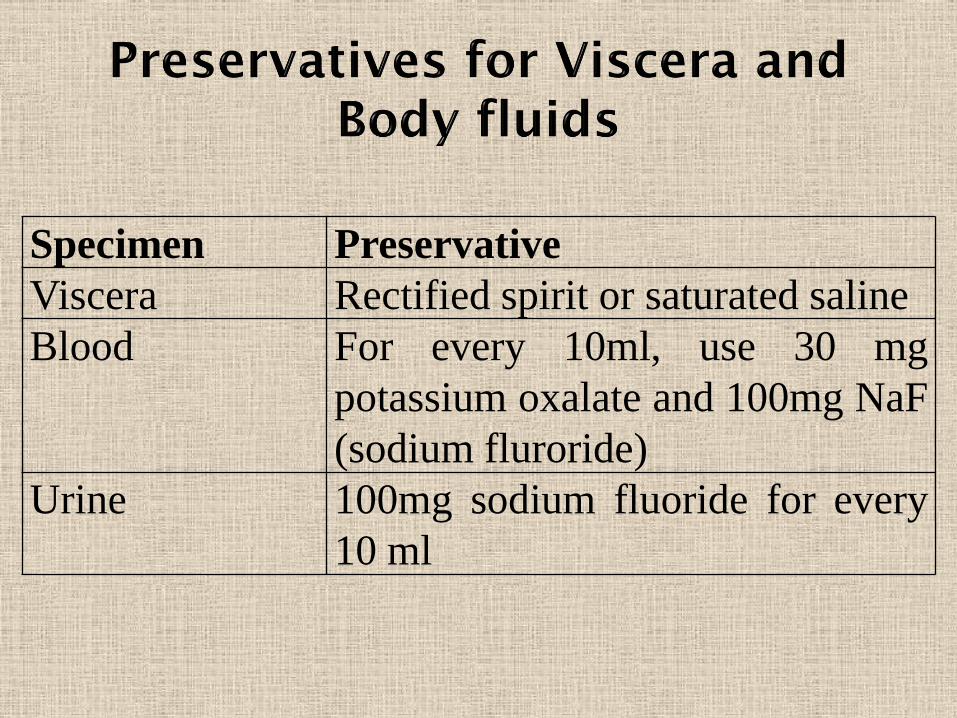
Specimen Preservative
Viscera Rectified spirit or saturated saline
Blood For every 10ml, use 30 mg
potassium oxalate and 100mg NaF
(sodium fluroride)
Urine 100mg sodium fluoride for every
10 ml
1. Delay in examination of viscera
2. Improper preservation of viscera
3. Use of incorrect analytical technique
4. Early disintegration of the poison
5. Complete metabolism of the poison in the body
6. Negligible amount of poison in the viscera
7. Lack of suitable chemical tests for the poison
8. Tampering of the preserved viscera.
1. Save the life of the patient.
2. All the findings including the history, signs and symptoms,
treatment given should be recorded.
3. In every suspected case of poisoning, a medical practitioner
whether in private or government service must preserve all
evidence.
4. If a medical practitioner in private practice is convinced that the
patient is suffering from homicidal poisoning – he is bound to
inform the nearest police station or magistrate.
1.A medical practitioner is not bound to give information
of his own record to the police if he is sure that the
patient is suffering from suicidal poisoning.
2. If death is apprehended then arrangement for
recording of dying declaration should be made.
3. In case of death, the police must be informed and
recommendation for postmortem examination should
be made.