Embed Size (px)
Citation preview

How to deal with the affordability of oncology drugs?From personalised medicine to personalisedreimbursement modelsJeroen van Dijk, Sales Director, Roche NederlandSeptember 29th 2016

Doing now what patients need next

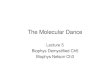
The Netherlands compared to other EU
countries
Source: Healthcare costs of cancer per person in European Union (Luengo-Fernandez et al - Lancet Oncology, 2013)

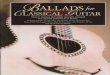
Spending over the last years
Out-patient vs hospital setting
Outpatient drugs
Hospital drugs
Spending in bln €

Drug expenses in 2015
Health care expenses 2015 Increase
Health care budget (Budget Kader
Zorg)€73 billion -
Drugs (total) €5 billion 6%
Inpatient drugs €2.06 billion 6%
‘Expensive’ inpatient drugs €1.62 billion 9%
‘Expensive’ oncology drugs €810 million 15%
Source: Farminform, 2016

Budget cap for hospitals
Maximum growth 1% per annum• Agreement between MoH, NVZ,
NFU, NPCF, ZKN, ZN, OMS.
• Cap on growth rate:
• 2012-2013: 2,5% p.a.
• 2014: 1,5% p.a.
• 2015-2017: 1% p.a.
Healthcare Insurance Act
€ 45,9 billion
Longterm care
€ 19,9 billion
Wmo € 6,7 billion
Other € 0,4 billion
Na
tio
na
l H
ea
lth
ca
re B
ud
ge
t: €
72
,9 b
illio
n
Hospital care
€ 23,0 billion
(Incl. hospital drugs)
Ref: National Budget 2016 (2015); Administrative
Agreement 2012, 2013
Outpatient drugs

Sounding the alarm on drug prices

Pricing by RocheRoche only develops innovative drugs
Population size ValueR&D
• Drug prices depend on economic situation, governmental priorities and health
care system
• Therefore differentiation of drug prices among EU countries is crucial for the
accessibility to drugs for patients in Europe

How to warrant affordability and accessibility in
the future?Are we not able to pay for it or we just don’t know how?• Several measures are used in the NL to maintain affordability and
accessibility in the future, such as:
– Rational pharmacotherapy (‘gepast gebruik’)
• E.g. Start-stop criteria
– Financial arrangements to constrain the budget impact
• Initiated by Ministry of Health (‘buro prijsarrangementen
geneesmiddelen’)
– Value-based health care
• Cost-effectiveness

Is a fixed CE-threshold is appropriate for decision
making?
Metastatic versus early setting
• First introduction of new oncology drugs is in metastatic setting
• According to current models used, the ‘value’ of the drug is always
lower here compared to the early setting*
• Is that right?
• What does a cost per QALY mean in the metastatic setting?
• What does this mean for price setting?
*Dvortsin et al. PLoS ONE 11(1): e0146551. doi:10.1371

How to optimize ‘value’?
• Increase in value
– Personalised medicine
• Biomarker testing
• Rational pharmacotherapy agreements
• How to measure value
– Gather Real World Evidence
• Clinical outcomes
– Value for society
Personalised medicines personalised reimbursement models

Challenge: future combination therapies
• Expected Combination Regimen Launches in Oncology

Drugs of different companies being combined
• Potential Combination Therapies Launching by 2021

From volume to value
Increasing levels of patient based information
Undifferentiated price
per vial
Episode-of-
care
Unit based pricing Personalised Reimbursement Models
Today Future
Combinations+
Reimbursement driven by
volume of therapy used
Reimbursement driven by value therapy delivers to the patient
National registries
Multiple indications
Pay for response
?

Takeaways
• A fixed cost-effectiveness threshold for drugs in the metastatic setting is
not desirable
• Personalised medicine asks for personalised reimbursement models
– Nationwide registries warranted
– How to deal with combination therapies?
• Collaboration between all relevant stakeholders needed in order to
keep the health care system affordable and sustainable

Doing now what patients need next