Embed Size (px)
Citation preview

Presentation Presentation Number:Number: 1054-19 1054-19Progress With the Calibration of a 3Fr Near Infrared Spectroscopy Fiber Progress With the Calibration of a 3Fr Near Infrared Spectroscopy Fiber
Optic Catheter for Monitoring the pH of Atherosclerotic Plaque: Optic Catheter for Monitoring the pH of Atherosclerotic Plaque: Introducing a Novel Approach for Detection of Active Vulnerable PlaqueIntroducing a Novel Approach for Detection of Active Vulnerable Plaque
Tania Khan, M.E.†, Babs R. Soller, PhD†; Peter Melling, PhD‡; Mohammad Madjid, M.D.*; Ward Casscells, M.D.*; Morteza Naghavi, M.D.*
†Department of Surgery, University of Massachusetts Medical School, Worcester MA 01655 ; ‡Remspec, Inc. Sturbridge MA; *Center for Vulnerable Plaque Research, University of Texas-Houston, and Texas Heart Institute, Houston TX 77030
BACKGROUND
AAtherosclerotic plaques vary by activityactivity and vulnerable plaques are more active than others. Our approach is based on identifying the different metabolic activities (e.g., tissue pH, temperature, metabolite concentrations) of atherosclerotic lesions using near infrared spectroscopy. Previously we reported pH heterogeneity in human and rabbit atherosclerotic lesions. Preliminary calibration models were derived using a 3Fr optical catheter prototype for plaque tissue pH, using near-infrared (NIR) spectroscopic techniques in the 400-1100 nm region. The tissue lactate concentration, a by-product of anaerobic glycolysis, is possibly another useful vulnerability parameter. Tissue lactate is detectable in atherosclerotic lesions through various destructive methods. In addition, the lactate molecule has known absorbance bands in the near-infrared at ~2250 and 2295 nm, with a shoulder region at approximately 2030 nm, which may facilitate the calibration of the NIR optical catheter.
In this study, we propose a non-destructive method of assessing lactate concentration in the active, living plaque, using a near-infrared spectroscopy based optical catheter.
In addition, macrophages sustain activity through anaerobic metabolism and lactate production. The tissue lactate concentration of atherosclerotic lesions may be an additional indicator of plaque vulnerability.
Morphology vs. Activity Imaging
Inactive and non-inflamed plaque
Active and inflamed
plaqueAppear Similar in
IVUS OCT MRI w/o CM
Morphology
Show DifferentActivity
Thermography, Spectroscopy, immunoscintigraphy, MRI with
targeted contrast media…
TEXAS HEART INSTITUTE
CONCLUSIONS
RESULTS
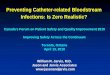
Figure 4: Changes in parameters over ~3.5 hrs of a representative plaque in the plaque viability study. (m = media values)
30
32
34
36
38
40
10:00:00 11:00:00 12:00:00 13:00:00 14:00:00
Temperature
7.00
7.10
7.20
7.30
7.40
7.50pH
temp pH
Plaque Viability Study
0
10
20
30
40
50
60
10:00:00 11:00:00 12:00:00 13:00:00 14:00:00
PCO2
7.00
7.10
7.20
7.30
7.40
7.50
pH
PCO2 m PCO2 pH m pH
sensor in
0
100
200
300
400
500
10:00:00 11:00:00 12:00:00 13:00:00 14:00:00Time
PO2
7.00
7.10
7.20
7.30
7.40
7.50
pH
PO2 mPO2 pH m pH
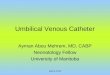
Figure 5: Box-whisker plots for change in pH per hour and change in temperature per hour (respectively) for the control and test plaques in the viability study. Rate of change in controls are significantly different than the test plaques.
Figure 6: Seventeen raw spectra from 5 plaques are shown. The best calibration results used 2030 –2330 nm data. This wavelength region corresponds to the theoretical lactate absorbance spectrum.
Lactate Feasibility Study
HYPOTHESES
The excised human carotid plaques can be maintained at near in-vivo, physiologic conditions using tissue culture techniques for extended periods during the measurements.
Using the same optical catheter as for NIR pH determination, NIR-measured lactate concentration is feasible in living, heterogeneous carotid plaques.
METHODSPlaque Viability
Study
• Minimum Eagle’s Med-ium (MEM), pH 7.4, 5.6 mM glucose, 26.2 mM NaHCO3, with non-essential amino acids was used (Invitrogen).
• Media equilibrated with 75% O2 / 5% CO2 gas mixture prior to tissue addition.
• Seven human carotid plaques were collected and placed immediately in 37°C media enclosed in a humidified incubator at 37°C. Figure 1.
• Two plaques that were not placed in the liquid media, only in the humidified air of the incubator, served as controls.
• Measurements were taken with a multi-parameter, intra-arterial sensor placed in the tissue (Diametrics, MN). Figure 2.
• Changes in tissue pH, temperature, PO2 and PCO2 over time were analyzed.
Lactate Feasibility
Study
• Five additional human carotid plaques were collected in a similar manner. 3-4 areas of each plaque were randomly chosen for total of 17 points.
• Reflectance spectra (1100 – 2500 nm) of each area were taken using Nicolet FTIR 670 spectrometer with a fiber optic probe. (Remspec, MA) Figure 3.
• Tissue biopsies of the same area were taken using a 4-mm punch biopsy and immediately frozen in liquid nitrogen.
• Tissue lactate (LA) was assayed using micro-enzymatic methods (Sigma). Values are reported as micromole LA per gram wet tissue.
• Matching spectra and tissue lactate values modeled by multivariate calibration techniques. R2 and root mean squared deviation (RMSD) used to assess model accuracy.
Figure 2: Plaque in media with multi-parameter sensor in place. The media is oxygenated by bubbling gas.
sensor
Figure 1: Experimental setup for both studies. Incubator maintained at 37°C.
Figure 3: Fiber optic probe used for lactate feasibility study.
The oxygenated media environment allowed the plaques to remain in near in-vivo status for the duration of the data collection.
The near infrared (NIR) measurement of tissue lactate in living carotid plaques is feasible and well correlated with the standard destructive measurement of tissue lactate by micro-enzymatic assay.
This experimental setup may allow us, in the future, to directly translate calibration equations generated in-vitro, to in-vivo validation studies.
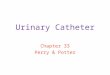
Figure 7: Correlation between the actual tissue lactate values and the NIR determined values is shown. The R2 of the determination was 0.83. The RMSD or estimated accuracy of the model was 1.4 micromole LA /gram tissue.
-2.0
0.0
2.0
4.0
6.0
8.0
10.0
12.0
-2.0 0.0 2.0 4.0 6.0 8.0 10.0 12.0Actual Lactate Concentration
(microle/gram tissue)
NIR-Lactate Concentration
(micromole/gram tissue)

BACKGROUNDAAtherosclerotic plaques vary by activityactivity and vulnerable plaques are more active than others. Our approach is based on identifying the different metabolic activities (e.g., tissue pH, temperature, metabolite concentrations) of atherosclerotic lesions using near infrared spectroscopy. Previously we reported pH heterogeneity in human and rabbit atherosclerotic lesions. Preliminary calibration models were derived using a 3Fr optical catheter prototype for plaque tissue pH, using near-infrared (NIR) spectroscopic techniques in the 400-1100 nm region. The tissue lactate concentration, a by-product of anaerobic glycolysis, is possibly another useful vulnerability parameter. Tissue lactate is detectable in atherosclerotic lesions through various destructive methods. In addition, the lactate molecule has known absorbance bands in the near-infrared at ~2250 and 2295 nm, with a shoulder region at approximately 2030 nm, which may facilitate the calibration of the NIR optical catheter.

Morphology vs. Activity Imaging
Inactive and non-inflamed plaque
Active and inflamed
plaqueAppear Similar in
IVUS OCT MRI w/o CM
Morphology
Show DifferentActivity
Thermography, Spectroscopy, immunoscintigraphy, MRI with
targeted contrast media…

• In this study, we propose a non-destructive method of assessing lactate concentration in the active, living plaque, using a near-infrared spectroscopy based optical catheter.
• Macrophages sustain activity through anaerobic metabolism and lactate production. The tissue lactate concentration of atherosclerotic lesions may be an additional indicator of plaque vulnerability.
GOALS

•The excised human carotid plaques can be maintained at near in-vivo, physiologic conditions using tissue culture techniques for extended periods during the measurements.
•Using the same optical catheter as for NIR pH determination, NIR-measured lactate concentration is feasible in living, heterogeneous carotid plaques.
HYPOTHESES

Plaque Viability Study
•Minimum Eagle’s Medium (MEM), pH 7.4, 5.6 mM glucose, 26.2 mM NaHCO3, with non-essential amino acids was used (Invitrogen).
•Media equilibrated with 75% O2 / 5% CO2 gas mixture prior to tissue addition.
•Seven human carotid plaques were collected and placed immediately in 37°C media enclosed in a humidified incubator at 37°C. Figure 1.
•Two plaques that were not placed in the liquid media, only in the humidified air of the incubator, served as controls.
Figure 1: Experimental setup for both studies. Incubator maintained at 37°C.
METHODS

• Measurements were taken with a multi-parameter, intra-arterial sensor placed in the tissue (Diametrics, MN). Figure 2.
• Changes in tissue pH, temperature, PO2 and PCO2 over time were analyzed.
sensor
Figure 2: Plaque in media with multi-parameter sensor in place. The media is oxygenated by bubbling gas.
Plaque Viability Study (Con’t)

Lactate Measurement Study
•Five additional human carotid plaques were collected in a similar manner. 3-4 areas of each plaque were randomly chosen for total of 17 points.
•Reflectance spectra (1100 – 2500 nm) of each area were taken using Nicolet FTIR 670 spectrometer with a fiber optic probe. (Remspec, MA) Figure 3.
Figure 3: Fiber optic probe used for lactate feasibility study.

• Tissue biopsies of the same area were taken using a 4-mm punch biopsy and immediately frozen in liquid nitrogen.
• Tissue lactate (LA) was assayed using micro-enzymatic methods (Sigma). Values are reported as micromole LA per gram wet tissue.
• Matching spectra and tissue lactate values modeled by multivariate calibration techniques. R2 and root mean squared deviation (RMSD) used to assess model accuracy.
Lactate Measurement Study (Con’t)

Figure 4: Changes in parameters over ~3.5 hrs of a representative plaque in the plaque viability study. (m = media values)
30
32
34
36
38
40
10:00:00 11:00:00 12:00:00 13:00:00 14:00:00
Tem
pera
ture
7.00
7.10
7.20
7.30
7.40
7.50
pH
temp pH
Plaque Viability Study
0
10
20
30
40
50
60
10:00:00 11:00:00 12:00:00 13:00:00 14:00:00
PCO
2
7.00
7.10
7.20
7.30
7.40
7.50
pH
PCO2 m PCO2 pH m pH
sensor in
0
100
200
300
400
500
10:00:00 11:00:00 12:00:00 13:00:00 14:00:00Time
PO2
7.00
7.10
7.20
7.30
7.40
7.50pH
PO2 mPO2 pH m pH
RESULTS

Figure 5: Box-whisker plots for change in pH per hour and change in temperature per hour (respectively) for the control and test plaques in the viability study. Rate of change in controls are significantly different from the test plaques.

Figure 6: Seventeen raw spectra from 5 plaques are shown. The best calibration results used 2030 –2330 nm data. This wavelength region corresponds to the theoretical lactate absorbance spectrum.
Lactate Measurement Study
-2.0
0.0
2.0
4.0
6.0
8.0
10.0
12.0
-2.0 0.0 2.0 4.0 6.0 8.0 10.0 12.0Actual Lactate Concentration
(microle/gram tissue)
NIR
-Lac
tate
Con
cent
ratio
n (m
icro
mol
e/gr
am ti
ssue
)
Figure 7: Correlation between the actual tissue lactate values and the NIR determined values is shown. The R2 of the determination was 0.83. The RMSD or estimated accuracy of the model was 1.4 micromole LA /gram tissue.

The oxygenated media environment allowed the plaques to remain in near in-vivo status for the duration of the data collection.
The near infrared (NIR) measurement of tissue lactate in living carotid plaques is feasible and well correlated with the standard destructive measurement of tissue lactate by micro-enzymatic assay.
This experimental setup may allow us, in the future, to directly translate calibration equations generated in-vitro, to in-vivo validation studies.
CONCLUSIONS