Embed Size (px)
Citation preview

3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
3M™ Tegaderm™ CHGChlorhexidine Gluconate IV Securement Dressing
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
A New Look at CHG: Impact on Clinical Practice
ObjectivesToday we will….•
Review chlorhexidine gluconate (CHG) action and activity on skin
•
Review sources of contamination with central venous catheters (CVCs)
•
Discuss the impact of CHG dressings in clinical practice
•
Review what you asked for in an antimicrobial dressing
•
Answer your questions related to Tegaderm™ CHG dressings
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
CHG Effectiveness•
First synthesized and marketed in 1950s–
Over 55 years of efficacy and safety experience with CHG as a topical antimicrobial
•
Efficacy–
Broad-spectrum activity against gram-positive and gram-
negative bacteria, anaerobes and aerobes, yeasts, and some lipid-envelope viruses
–
Not sporicidal–
Demonstrated effectiveness against S. epi, MRSA, VRE, K. pneumoniae, C. albicans
•
Bacterial susceptibility–
After 50 years of research and experience, still no development of bacterial resistance against CHG
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
CHG Activity
Properties: •
Binds to, and is shed with, the skin’s surface layer
•
No meaningful penetration across the skin barrier into systemic circulation
•
Persistent activity –
remains on skin until shed•
Cumulative activity –
bacteria population
continues to be reduced over time (bacterial regrowth is suppressed)
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
CHG ActivityLandmark Reviews:•
Milstone; Clinical Infectious Disease 2008, Vol 47
•
Denton; Disinfection, Sterilization and Preservation; 2001. CTFA Final Report
•
Safety (Chlorhexidine Safety. Journal of the American College of Toxicology 1993)–
Rare local skin reactions
–
Extremely rare incidence of sensitization–
Isolated reports of allergic and anaphylactic reactions
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
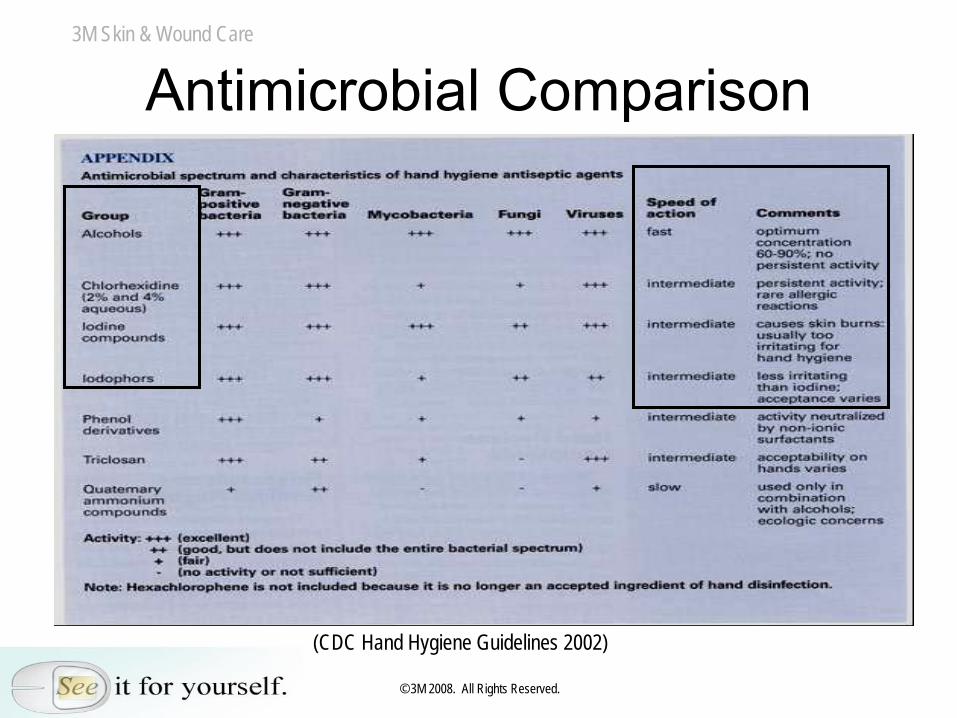
Antimicrobial Comparison
(CDC Hand Hygiene Guidelines 2002)
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
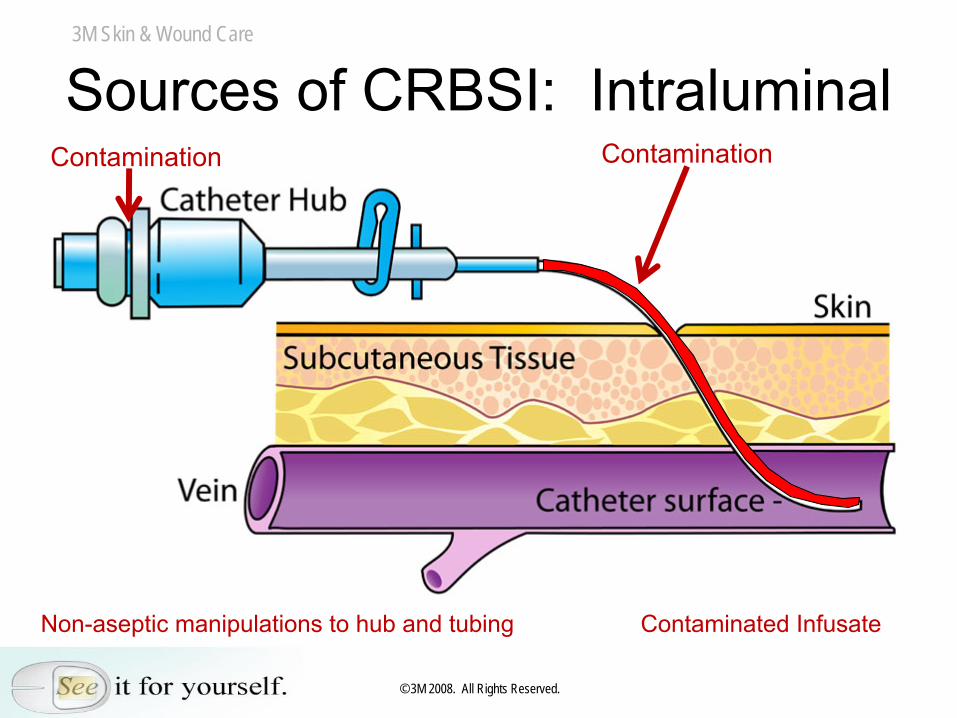
Sources of CRBSI: IntraluminalContamination Contamination
Non-aseptic manipulations to hub and tubing Contaminated Infusate
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
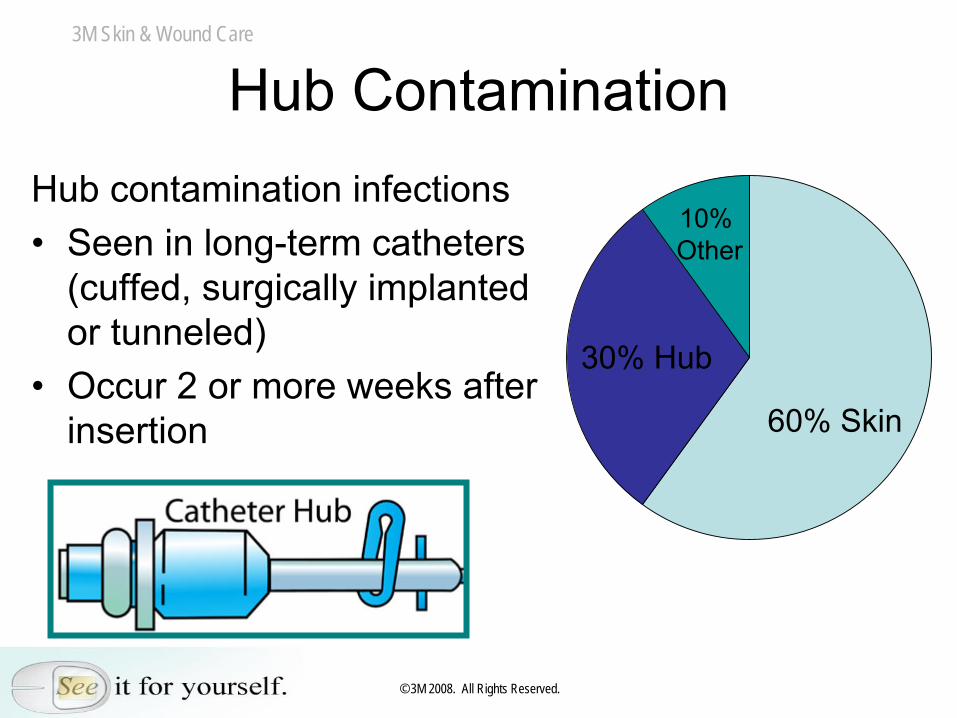
Hub ContaminationHub contamination infections•
Seen in long-term catheters (cuffed, surgically implanted or tunneled)
•
Occur 2 or more weeks after insertion
10%Other
60% Skin
30% Hub
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
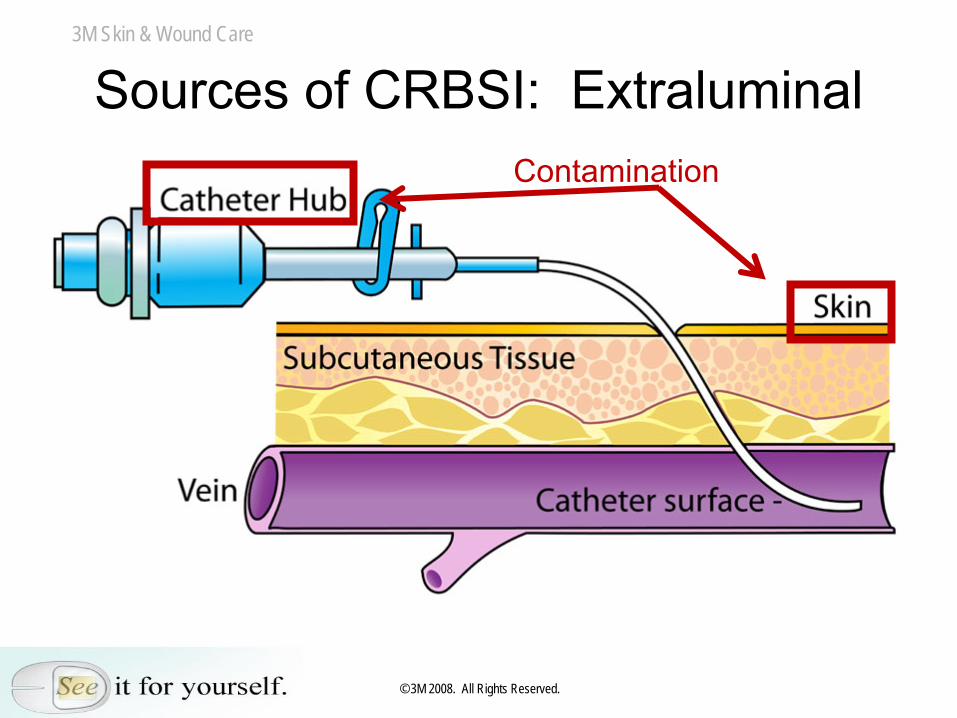
Sources of CRBSI: ExtraluminalContamination
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
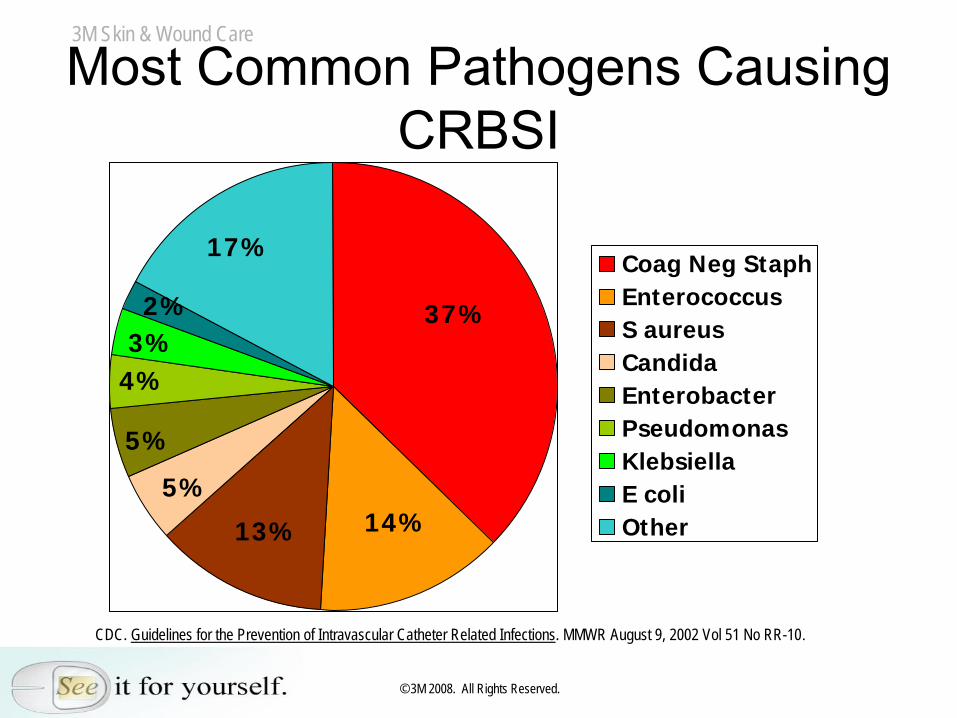
Most Common Pathogens Causing CRBSI
37%
14%13%
5%
5%
4%3%2%
17%Coag Neg StaphEnterococcusS aureusCandidaEnterobacterPseudomonasKlebsiellaE coliOther
CDC. Guidelines for the Prevention of Intravascular Catheter Related Infections. MMWR August 9, 2002 Vol 51 No RR-10.
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
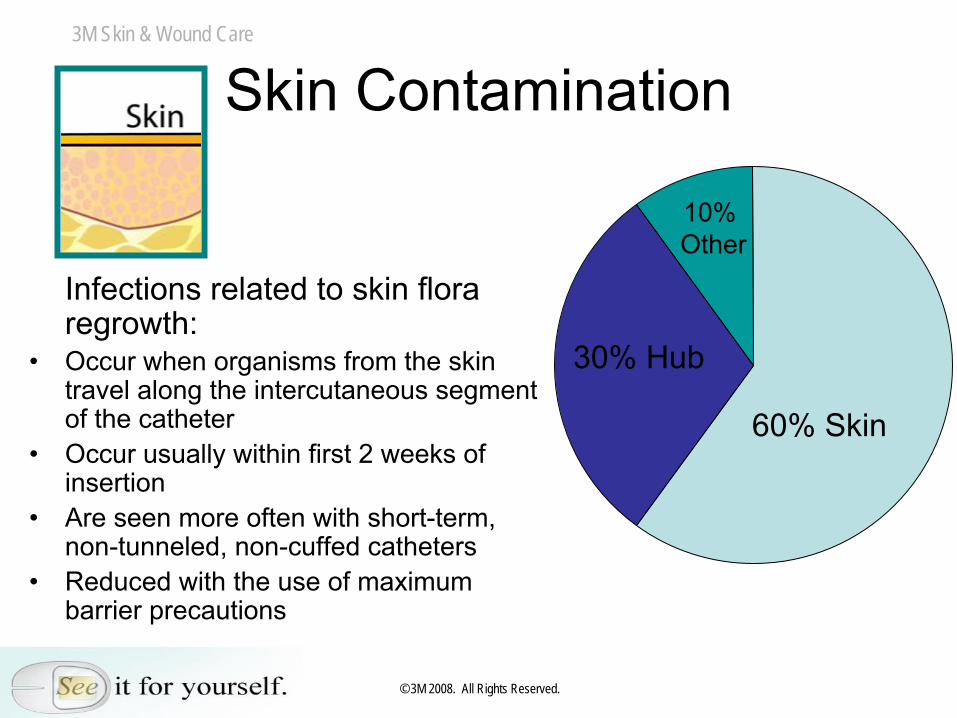
Skin Contamination
Infections related to skin flora regrowth:
•
Occur when organisms from the skin travel along the intercutaneous segment of the catheter
•
Occur usually within first 2 weeks of insertion
•
Are seen more often with short-term, non-tunneled, non-cuffed catheters
•
Reduced with the use of maximum barrier precautions
60% Skin
10%Other
30% Hub
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
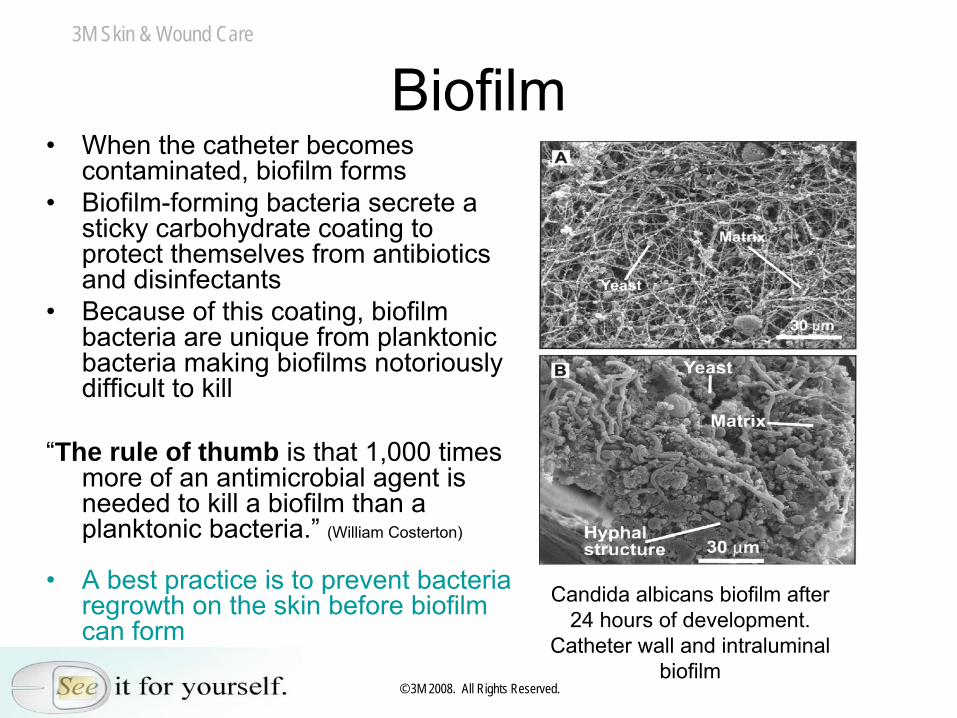
Biofilm•
When the catheter becomes contaminated, biofilm forms
•
Biofilm-forming bacteria secrete a sticky carbohydrate coating to protect themselves from antibiotics and disinfectants
•
Because of this coating, biofilm bacteria are unique from planktonic bacteria making biofilms notoriously difficult to kill
“The rule of thumb is that 1,000 times more of an antimicrobial agent is needed to kill a biofilm than a planktonic bacteria.”
(William Costerton)
•
A best practice is to prevent bacteria regrowth on the skin before biofilm can form
Candida albicans biofilm after 24 hours of development.
Catheter wall and intraluminal biofilm
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
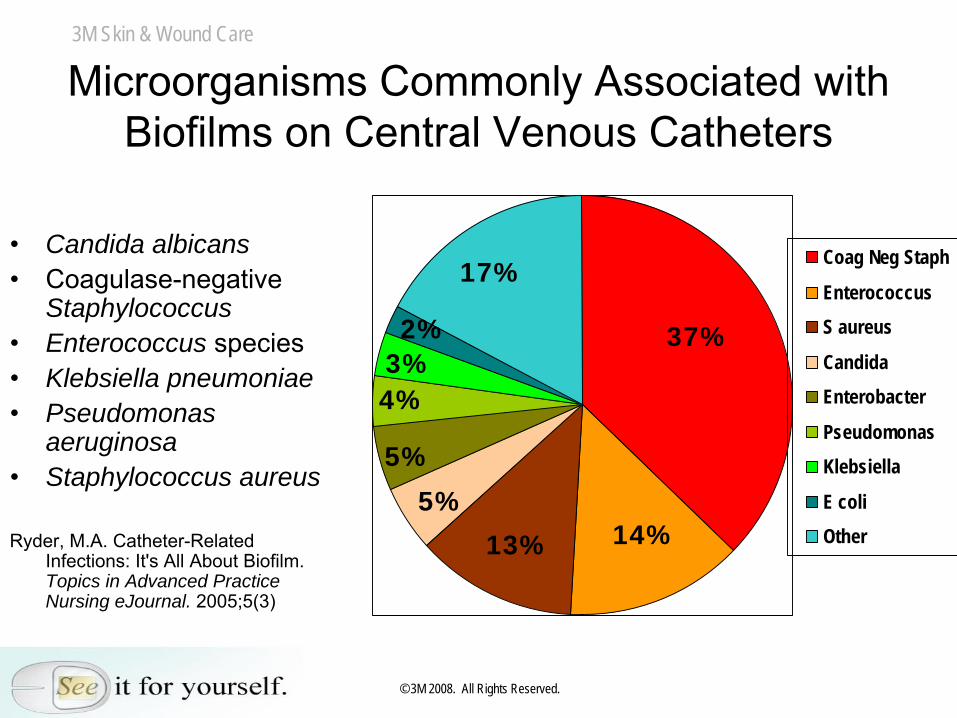
Microorganisms Commonly Associated with Biofilms on Central Venous Catheters
•
Candida albicans•
Coagulase-negative
Staphylococcus
•
Enterococcus species•
Klebsiella pneumoniae •
Pseudomonas aeruginosa
•
Staphylococcus aureus
Ryder, M.A. Catheter-Related Infections: It's All About Biofilm. Topics in Advanced Practice Nursing eJournal. 2005;5(3)
37%
14%13%
5%
5%
4%3%2%
17%Coag Neg Staph
EnterococcusS aureus
CandidaEnterobacter
PseudomonasKlebsiella
E coliOther
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Impact of Skin Flora
•
Location matters–
Skin of the neck and thorax is oily and houses approximately 1,000–10,000 CFUs per site
–
Skin of the antecubital space is dry and cool and houses approximately 10 CFUs per site
•
Even with stringent cleansing and prepping, up to 20% microbes remain on and within the skin after prepping –
the skin can never be sterilized
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Impact of Skin Flora
Greatest Single Source of Catheter Colonization and Infection for CVC’s in Place for 10 Days or Less:
References: Safdar, Kluger, Maki (2002) O’Grady (2002) Weinstein (1991)
Patient’s Own Skin FloraCatheter Surface Contamination
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Skin flora are the biggest concern because:
•
Preps don’t maintain low skin flora•
Skin antisepsis is a continuous activity, not an event
•
Skin flora will regrowSo … what can be done to control skin
flora regrowth longer?
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Clinicians Asked for an Antimicrobial Dressing That …
•
Contains CHG–
Controls skin flora–
Effective immediately•
Transparent to monitor insertion site daily for complications
•
Easy to use correctly•
Doesn’t require a change of practice
•
Has the potential to reduce nursing time and save money
•
Able to use on all patient populations•
Has the potential for fewer products –
integrated design
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Tegaderm™
CHG Dressing•
Gel pad integrated with Tegaderm™
transparent
film dressing •
2% CHG in a gel pad that is: –
Transparent
–
Able to absorb fluids–
Conformable
•
CHG availability–
Immediately available
–
Does not require additional skin moisture to activate
–
Skin flora reduction demonstrates consistent availability up to 10 days
–
CHG migrates to areas not in direct contact with gel
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Tegaderm™
CHG Dressing•
Effective –
Proven to reduce skin flora under the
dressing and prevent regrowth on healthy subjects for 10 days
•
Broad spectrum, long-lasting, fast antimicrobial activity*
•
Barrier to a variety of gram-positive and gram- negative bacteria and yeast*
•
Transparent –
Allows continuous site monitoring•
Integrated Design –
Minimizes application error
•
Clinician Friendly –
As easy-to-use and easy-to- train as Tegaderm™
Transparent Film
Dressings*Based on in vitro studies
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
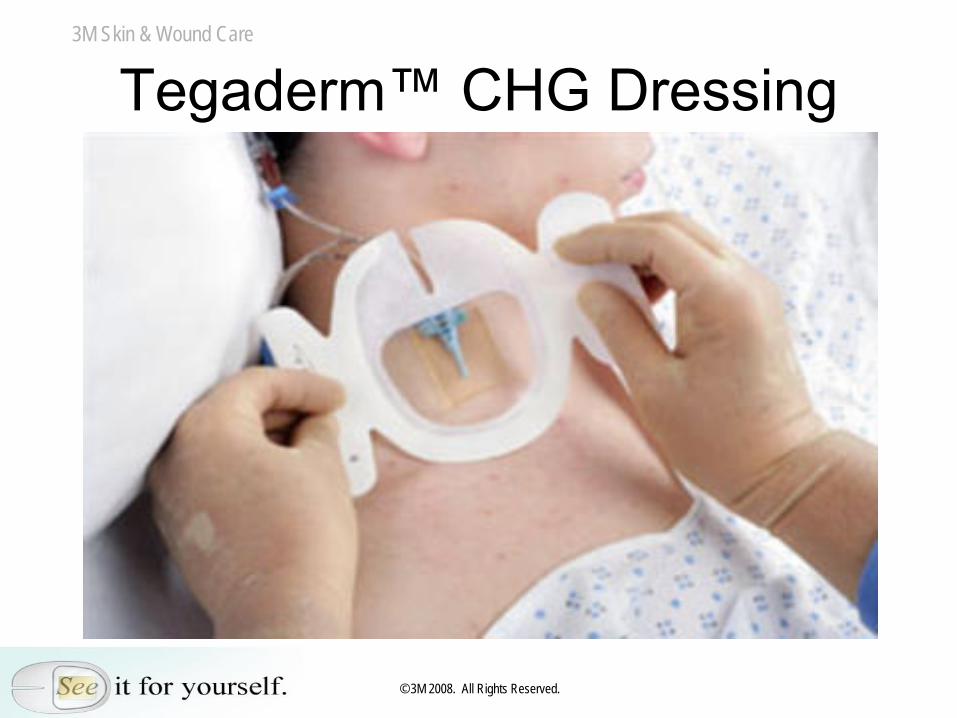
Tegaderm™
CHG Dressing
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
What Did You Ask? •
What “bugs”
does the dressing kill?
•
Does it kill the “bugs”
most commonly associated with CRBSIs?
•
Does CHG get under the catheter?•
Is it safe and effective?
•
How long is the dressing effective? •
How does this compare to other products on the market?
•
What clinical data do you have? Do you have a CRBSI study?
•
What independent studies do you have? •
Does it absorb fluid? And if so, how does it absorb fluid?
•
Can you use it on all devices? What other products can you use it on?
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
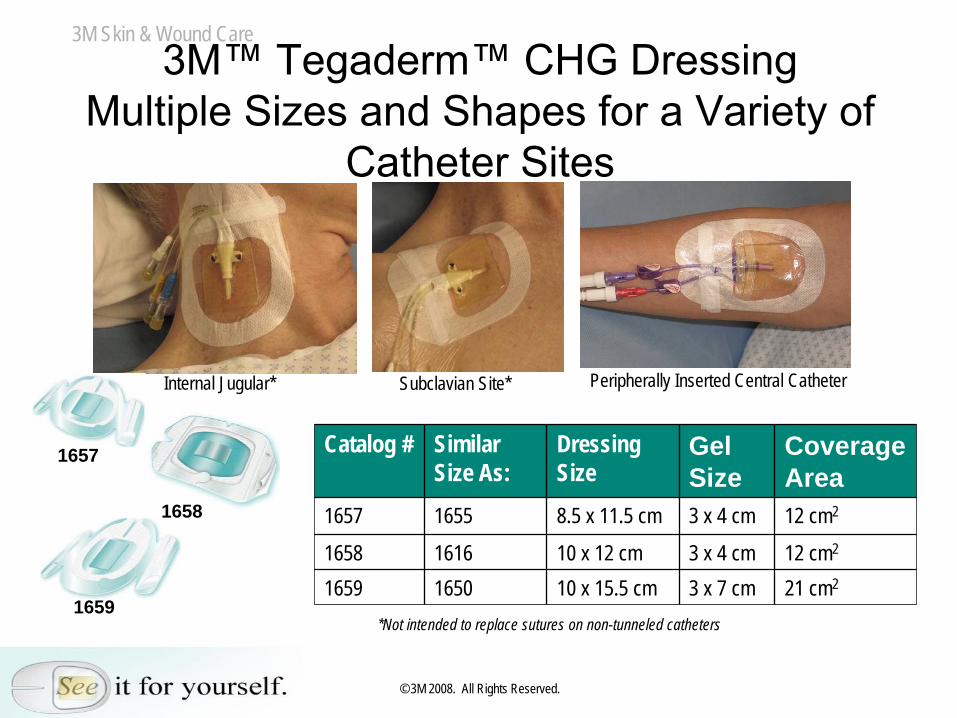
3M™
Tegaderm™
CHG Dressing Multiple Sizes and Shapes for a Variety of
Catheter Sites
Catalog # Similar Size As:
Dressing Size
Gel Size
Coverage Area
1657 1655 8.5 x 11.5 cm 3 x 4 cm 12 cm2
1658 1616 10 x 12 cm 3 x 4 cm 12 cm2
1659 1650 10 x 15.5 cm 3 x 7 cm 21 cm2
Internal Jugular* Subclavian Site* Peripherally Inserted Central Catheter
*Not intended to replace sutures on non-tunneled catheters
1657
1658
1659
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
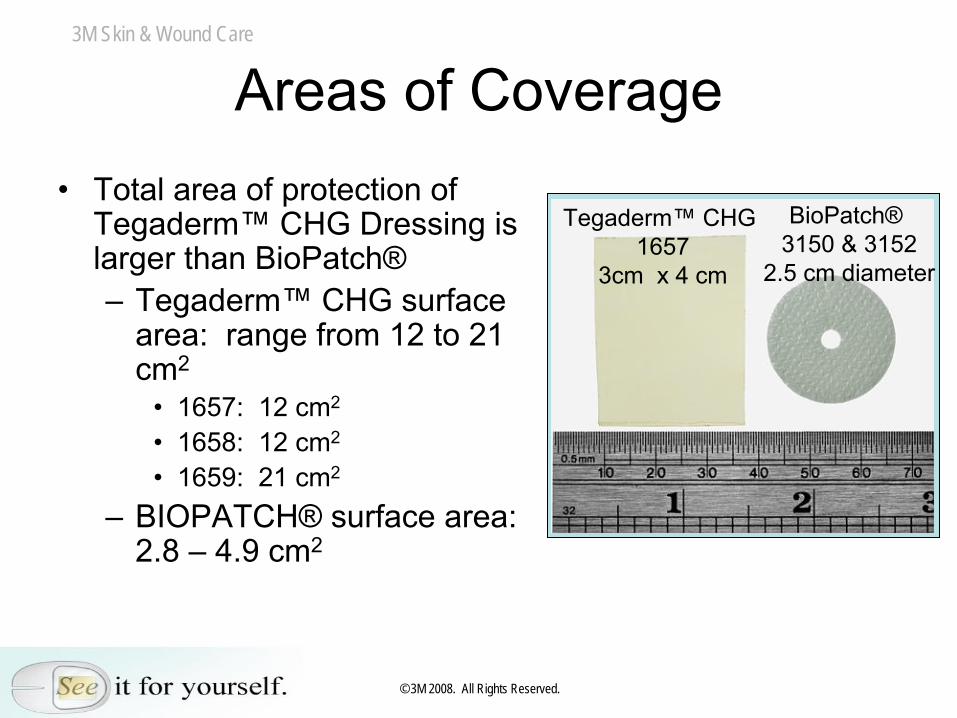
Areas of Coverage•
Total area of protection of Tegaderm™
CHG Dressing is
larger than BioPatch®–
Tegaderm™
CHG surface
area: range from 12 to 21 cm2
•
1657: 12 cm2
•
1658: 12 cm2
•
1659: 21 cm2
–
BIOPATCH®
surface area: 2.8 –
4.9 cm2
Tegaderm™
CHG 1657
3cm x 4 cm
BioPatch®3150 & 3152
2.5 cm diameter
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Tegaderm™
CHG Fluid Absorption
•
The novel technology of the gel pad has high capacity to absorb fluid–
Absorbs fluid slowly
–
Retains fluid in gel pad•
Smallest gel pad can absorb up to 18 mL (~ 3 teaspoons)–
Total absorption capacity is 6 times greater than BioPatch®
•
Presence of blood does not inactivate CHG
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
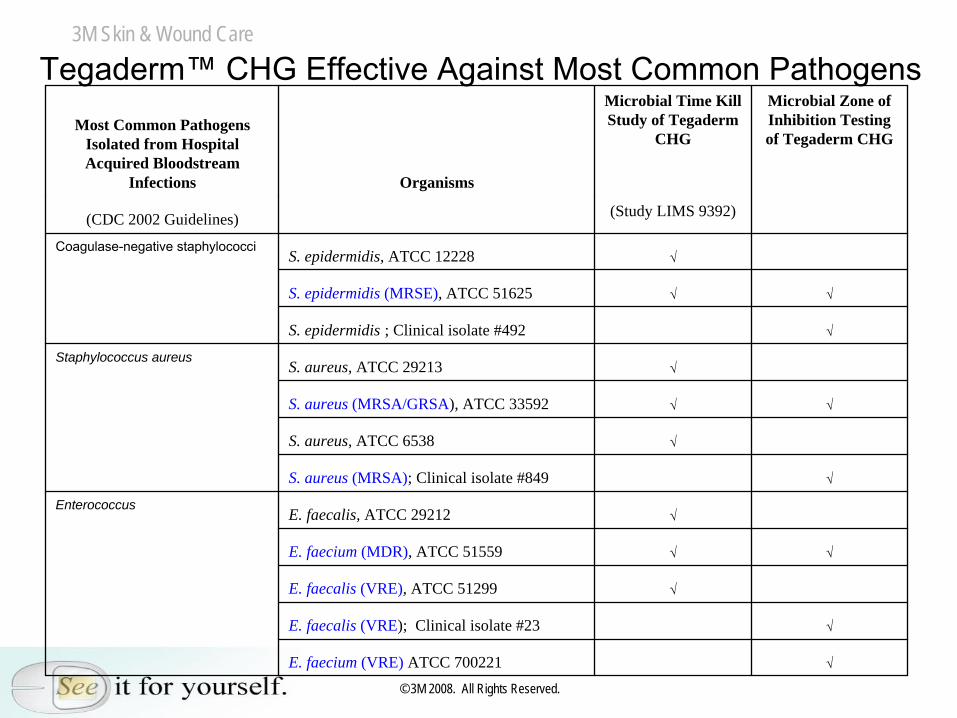
Most Common Pathogens Isolated from Hospital Acquired Bloodstream
Infections Organisms
Microbial Time Kill Study of Tegaderm
CHG
Microbial Zone of Inhibition Testing of Tegaderm CHG
(CDC 2002 Guidelines) (Study LIMS 9392)
Coagulase-negative staphylococciS. epidermidis, ATCC 12228 √
S. epidermidis (MRSE), ATCC 51625 √ √
S. epidermidis ; Clinical isolate #492 √
Staphylococcus aureusS. aureus, ATCC 29213 √
S. aureus (MRSA/GRSA), ATCC 33592 √ √
S. aureus, ATCC 6538 √
S. aureus (MRSA); Clinical isolate #849 √
EnterococcusE. faecalis, ATCC 29212 √
E. faecium (MDR), ATCC 51559 √ √
E. faecalis (VRE), ATCC 51299 √
E. faecalis (VRE); Clinical isolate #23 √
E. faecium (VRE) ATCC 700221 √
Tegaderm™
CHG Effective Against Most Common Pathogens
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
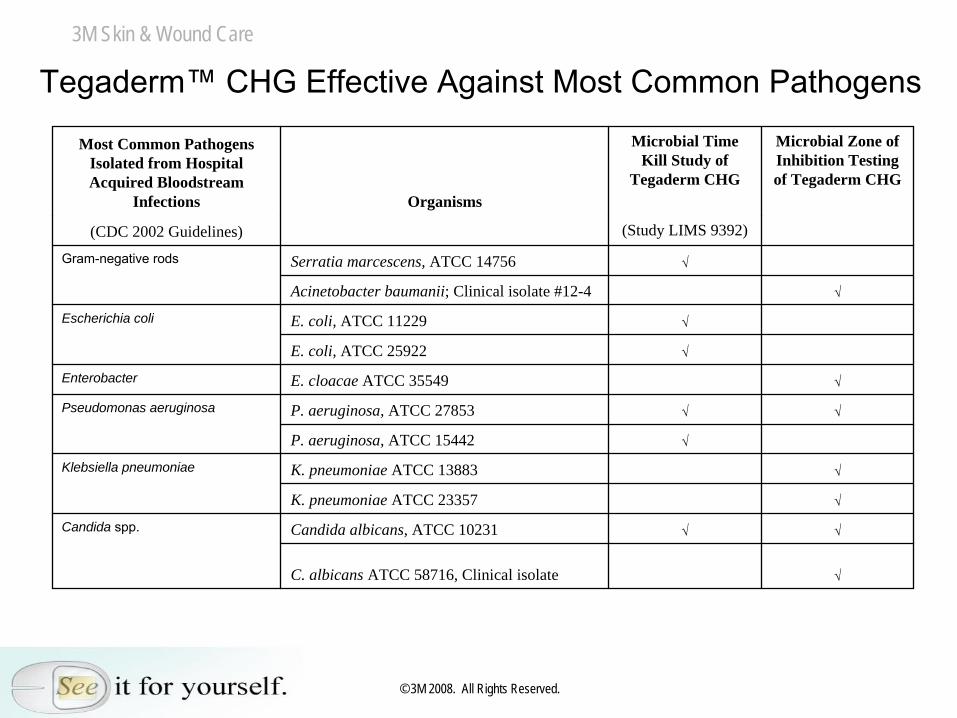
Most Common Pathogens Isolated from Hospital Acquired Bloodstream
Infections Organisms
Microbial Time Kill Study of
Tegaderm CHG
Microbial Zone of Inhibition Testing of Tegaderm CHG
(CDC 2002 Guidelines) (Study LIMS 9392)
Gram-negative rods Serratia marcescens, ATCC 14756 √
Acinetobacter baumanii; Clinical isolate #12-4 √
Escherichia coli E. coli, ATCC 11229 √
E. coli, ATCC 25922 √
Enterobacter E. cloacae ATCC 35549 √
Pseudomonas aeruginosa P. aeruginosa, ATCC 27853 √ √
P. aeruginosa, ATCC 15442 √
Klebsiella pneumoniae K. pneumoniae ATCC 13883 √
K. pneumoniae ATCC 23357 √
Candida spp. Candida albicans, ATCC 10231 √ √
C. albicans ATCC 58716, Clinical isolate √
Tegaderm™
CHG Effective Against Most Common Pathogens
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
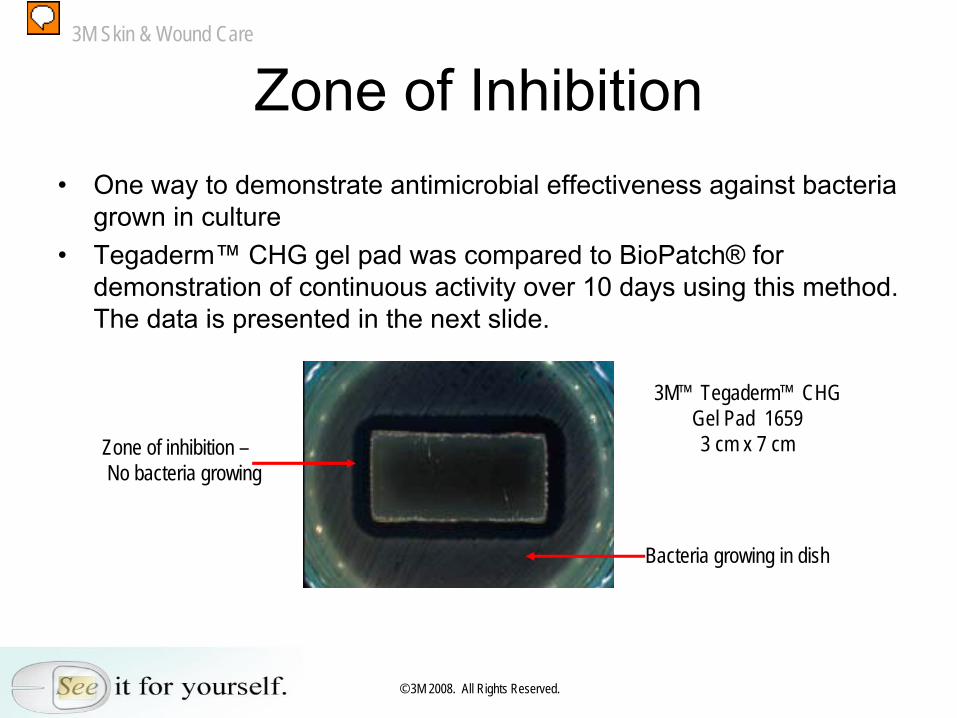
Zone of Inhibition•
One way to demonstrate antimicrobial effectiveness against bacteria grown in culture
•
Tegaderm™
CHG gel pad was compared to BioPatch®
for demonstration of continuous activity over 10 days using this method. The data is presented in the next slide.
Zone of inhibition –No bacteria growing
Bacteria growing in dish
3M™ Tegaderm™ CHG Gel Pad 16593 cm x 7 cm
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
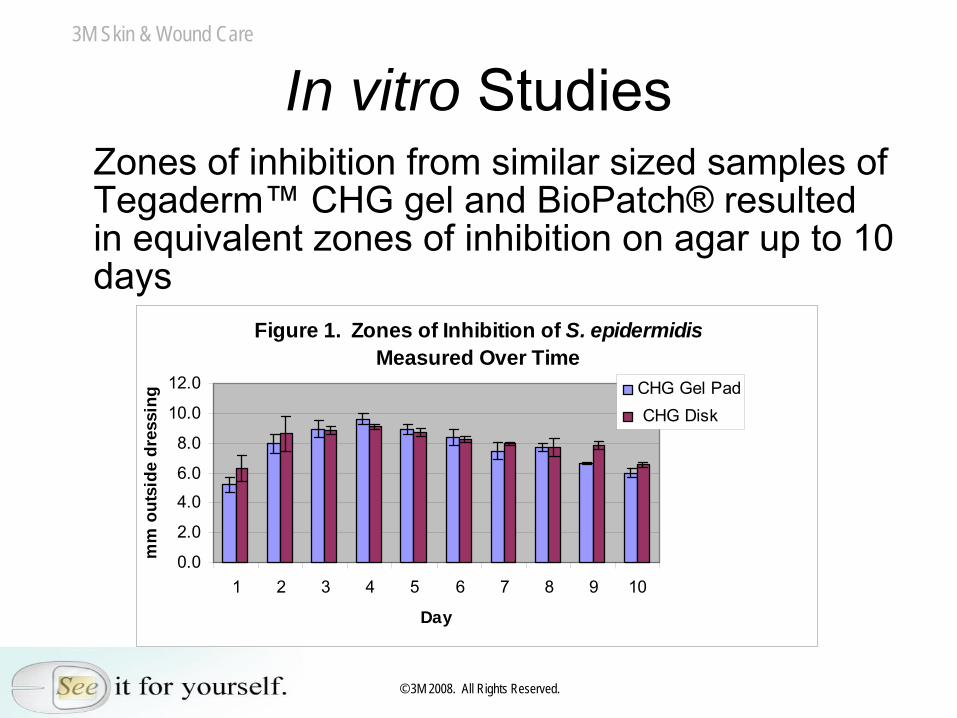
In vitro StudiesZones of inhibition from similar sized samples of Tegaderm™
CHG gel and BioPatch®
resulted
in equivalent zones of inhibition on agar up to 10 days
Figure 1. Zones of Inhibition of S. epidermidis Measured Over Time
0.0
2.0
4.0
6.0
8.0
10.0
12.0
1 2 3 4 5 6 7 8 9 10
Day
mm
out
side
dre
ssin
g CHG Gel Pad CHG Disk
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
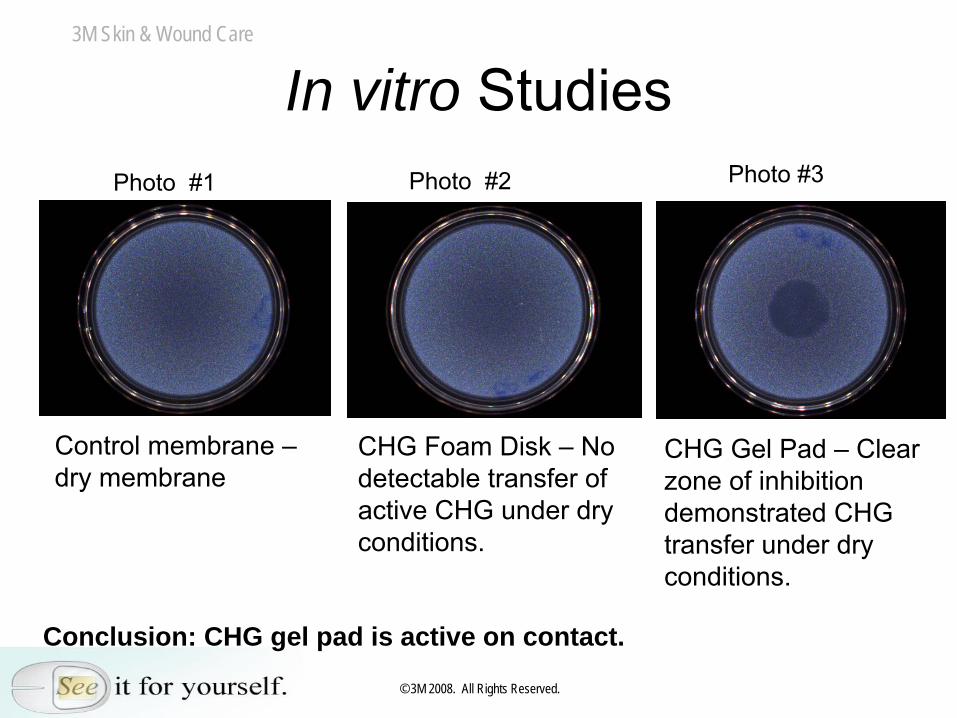
Control membrane –
dry membraneCHG Foam Disk –
No detectable transfer of active CHG under dry conditions.
CHG Gel Pad –
Clear zone of inhibition demonstrated CHG transfer under dry conditions.
In vitro StudiesPhoto #2Photo #1 Photo #3
Conclusion: CHG gel pad is active on contact.
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
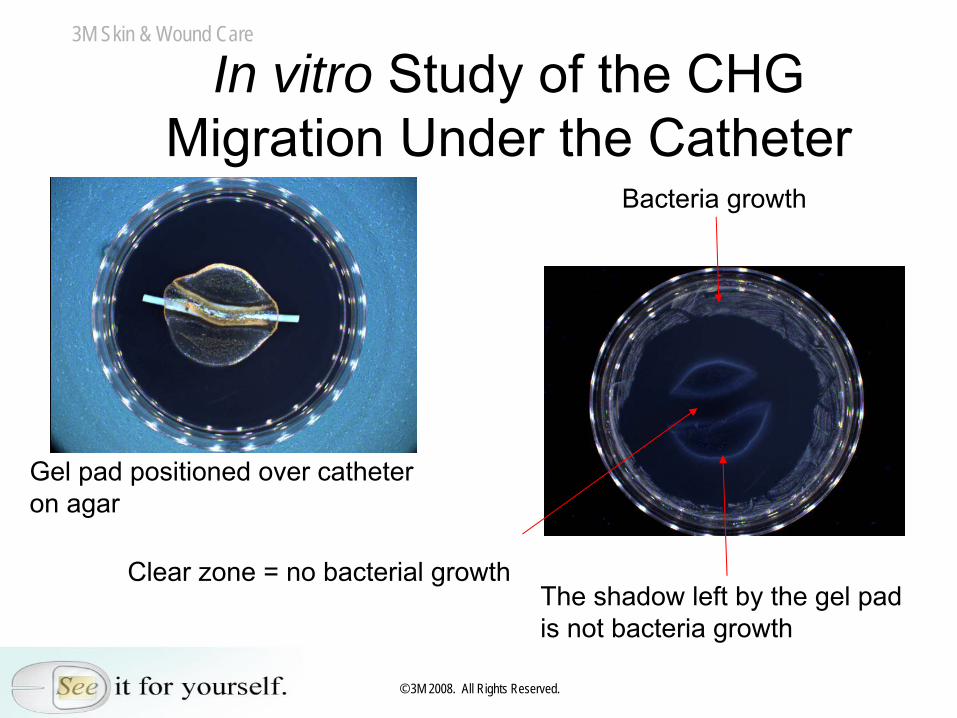
In vitro Study of the CHG Migration Under the Catheter
Gel pad positioned over catheter on agar
Bacteria growth
Clear zone = no bacterial growthThe shadow left by the gel pad is not bacteria growth
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
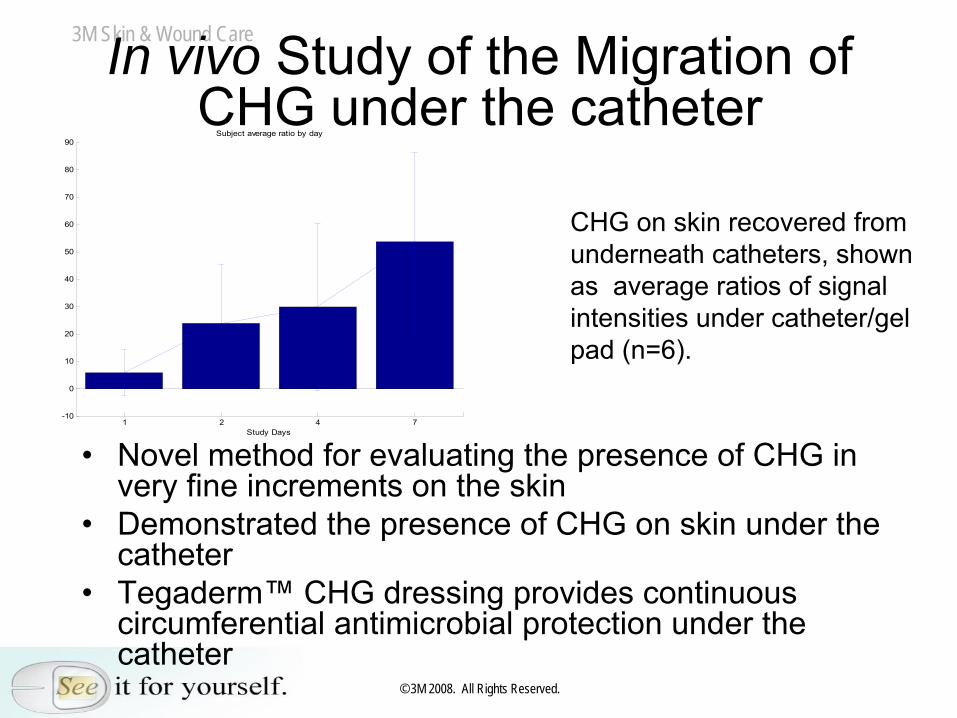
In vivo Study of the Migration of CHG under the catheter
1 2 4 7-10
0
10
20
30
40
50
60
70
80
90Subject average ratio by day
Study Days
CHG on skin recovered from underneath catheters, shown as average ratios of signal intensities under catheter/gel pad (n=6).
•
Novel method for evaluating the presence of CHG in very fine increments on the skin
•
Demonstrated the presence of CHG on skin under the catheter
•
Tegaderm™
CHG dressing provides continuous circumferential
antimicrobial protection under the
catheter
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
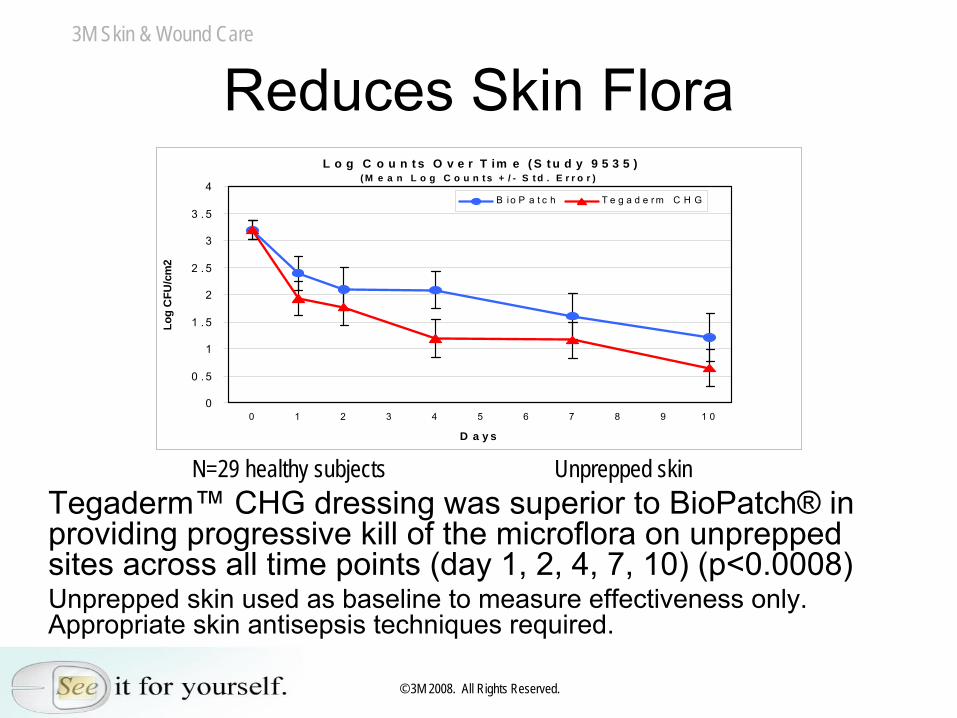
Reduces Skin Flora L o g C o u n t s O v e r T im e ( S t u d y 9 5 3 5 )
( M e a n L o g C o u n t s + / - S t d . E r r o r )
0
0 . 5
1
1 . 5
2
2 . 5
3
3 . 5
4
0 1 2 3 4 5 6 7 8 9 1 0
D a y s
Log
CFU
/cm
2
B i o P a t c h T e g a d e r m C H G
N=29 healthy subjects Unprepped skinTegaderm™
CHG dressing was superior to BioPatch®
in
providing progressive kill of the microflora on unprepped sites across all time points (day 1, 2, 4, 7, 10) (p<0.0008)Unprepped skin used as baseline to measure effectiveness only. Appropriate skin antisepsis techniques required.
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
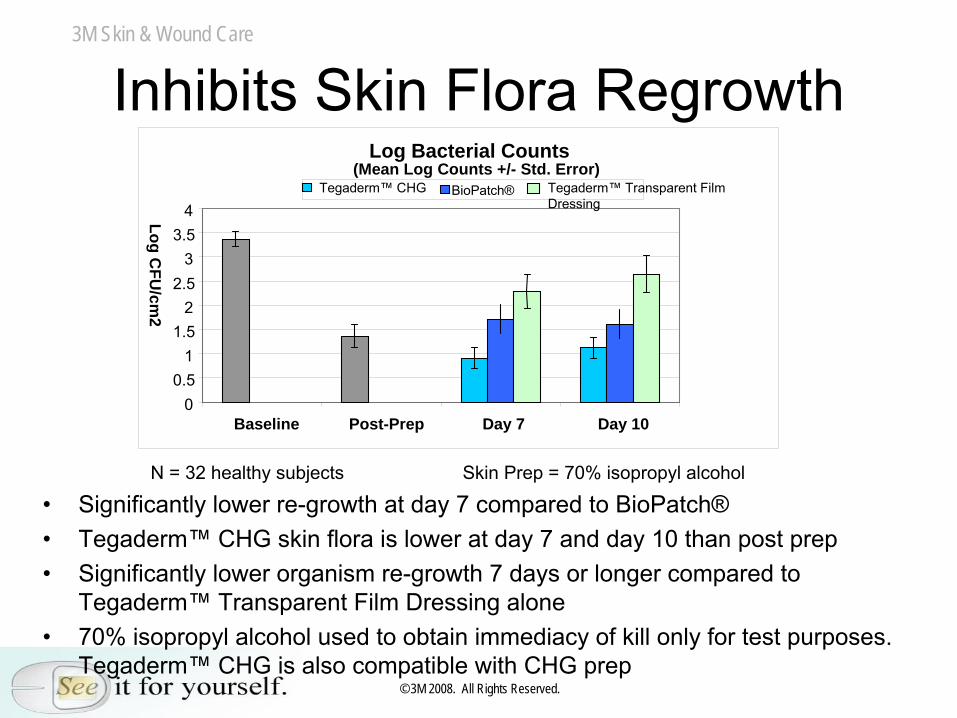
Inhibits Skin Flora RegrowthLog Bacterial Counts
(Mean Log Counts +/- Std. Error)
00.5
11.5
22.5
33.5
4
Baseline Post-Prep Day 7 Day 10
Log CFU
/cm2
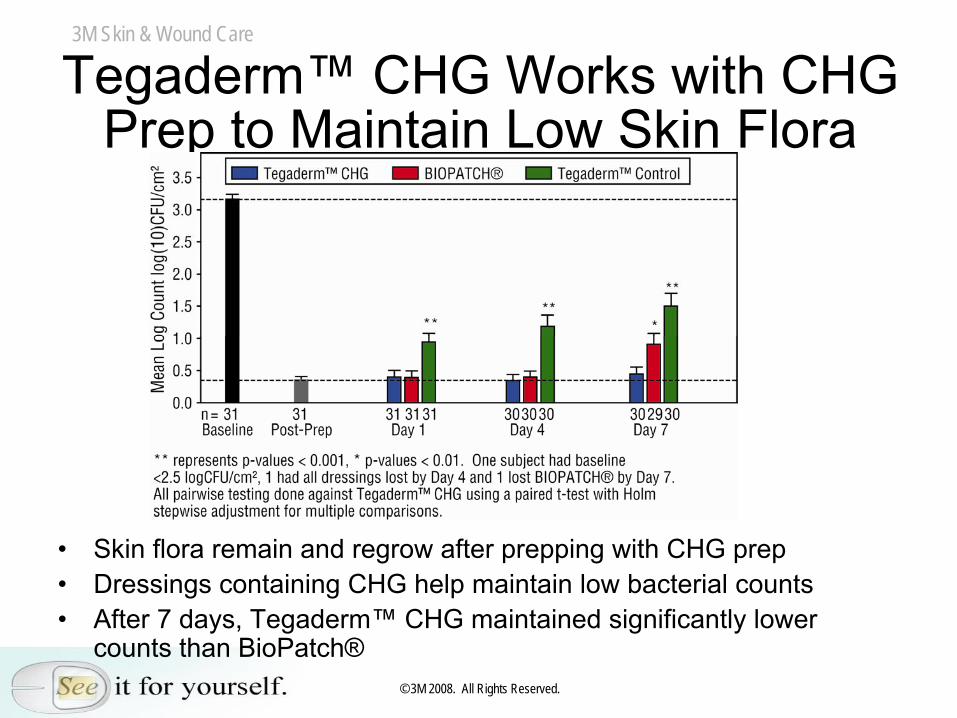
Tegaderm™ CHG BioPatch® Tegaderm™ Transparent Film Dressing
N = 32 healthy subjects Skin
Prep = 70% isopropyl alcohol
•
Significantly lower re-growth at day 7 compared to BioPatch®•
Tegaderm™
CHG skin flora is lower at day 7 and day 10 than post prep•
Significantly lower organism re-growth 7 days or longer compared to Tegaderm™
Transparent Film Dressing alone•
70% isopropyl alcohol used to obtain immediacy of kill only for test purposes. Tegaderm™
CHG is also compatible with CHG prep
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Tegaderm™
CHG Works with CHG Prep to Maintain Low Skin Flora
•
Skin flora remain and regrow after prepping with CHG prep•
Dressings containing CHG help maintain low bacterial counts•
After 7 days, Tegaderm™
CHG maintained significantly lower counts than BioPatch®
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Impact Of CHG Dressings In Clinical Practice
•
Use of CHG dressings suppress skin flora regrowth around catheter insertion site–
We can never sterilize skin, but we can reduce risk
–
Bacteria is always present and will regrow without continuous antimicrobial protection
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Clinical StudiesAbbott Northwestern, Carol Olson, RN-BC•
Randomized, prospective trial (n=63)
•
Key findings: –
Fits into clinical practice as easily as Tegaderm™
Transparent Dressings–
As easy to use as Tegaderm™
Transparent
Dressings–
Easy to use correctly
–
Site remains visible after moderate absorption of blood
–
No device-related adverse events
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Clinical Studies
Nebraska Medical Center, Dr. Mark E. Rupp•
Prospective, randomized study (n=60)– (20 PICC, 20 IJ, 20 Subclavian)
•
Conclusions: –
Tegaderm™
CHG dressing provides an innovative
method to potentially minimize CR-BSI–
The dressing is well-tolerated and judged to be superior to the comparator dressing (IV 3000®) with regard to catheter securement and overall satisfaction
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Professional Nurse Evaluation•
Tegaderm™
CHG rated as significantly better
than BioPatch®* in:–
Overall performance
–
Ease of application –
Ease of applying correctly
–
Ease of removal –
Ability to see IV site
–
Ease of training –
Intuitive application
•
12 out of 12 experienced vascular access nurses favored Tegaderm™
CHG over
BioPatch®
in overall performance*All P values ≤
than 0.0002
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
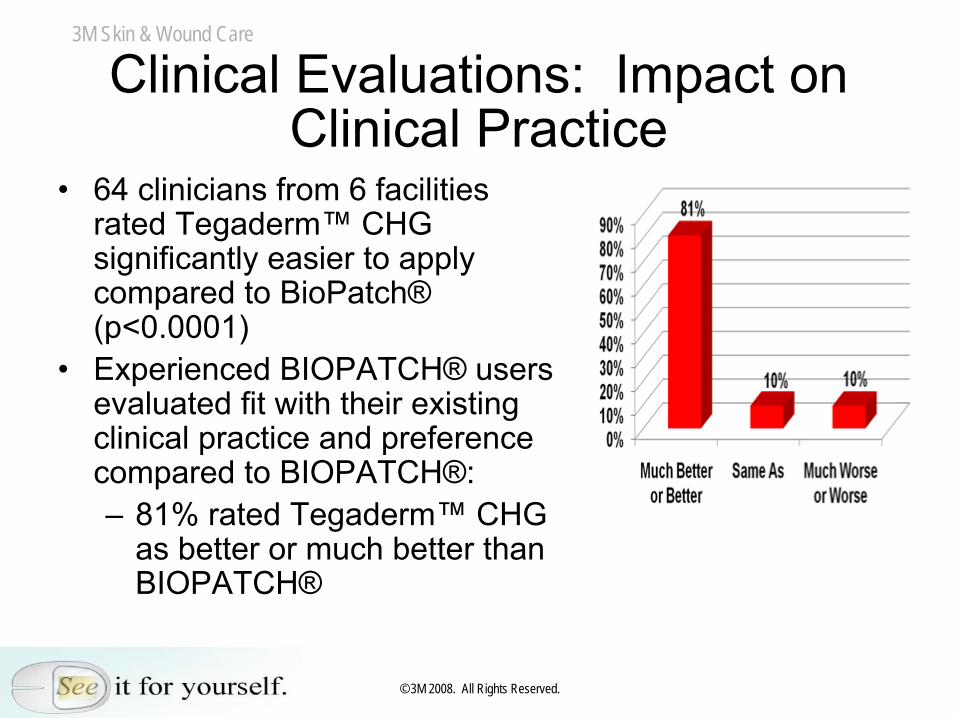
Clinical Evaluations: Impact on Clinical Practice
•
64 clinicians from 6 facilities rated Tegaderm™
CHG
significantly easier to apply compared to BioPatch®
(p<0.0001)•
Experienced BIOPATCH®
users
evaluated fit with their existing clinical practice and preference compared to BIOPATCH®: –
81% rated Tegaderm™
CHG
as better or much better than BIOPATCH®
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Is There Currently a CR-BSI Study on Tegaderm™
CHG?
•
No. Tegaderm™
CHG has not been studied as to it’s effectiveness in preventing CR-BSI in randomized clinical studies
•
High quality infection prevention studies require years to perform
•
Tegaderm™
CHG has been available for less than 1 year–
BioPatch®
has been available for more than
15 years
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
EVIDENCE BASED PRACTICE“Evidence Based Practice is the conscious explicit
and judicious use of the best available evidence in making decisions about the care of patients”
(Sackett et al 1996)
–
The value of CHG in a dressing has already been demonstrated
–
Skin flora’s correlation to CR-BSI is well established (Pathogenesis; CDC 2002; Maki, et. al.)
–
Tegaderm™
CHG has been shown to be superior to suppressing skin flora than other CHG dressings on the market
–
Tegaderm™
CHG is the next generation of antimicrobial dressings designed to meet the needs of clinicians
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
The Dressing Designed with You in Mind
•
Transparent to monitor insertion site daily for complications
•
Contains CHG–
Effective immediately
•
Advantages of Integrated design:–
Allows you to use fewer products
–
Easy to use correctly–
Doesn’t require a change of practice
–
Potential to reduce nursing time and save money–
Potential to secure and stabilize the catheter
•
Able to use on all patient populations
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
Thank You!
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-1Slides 3, 4, 5 (CHG)(Milstone (2008), Denton (1991), CTFA (1993), O’Sullivan (2003)
–
Milstone AN, Passaretti CL, Perl TM (2008) Chlorhexidine; expanding the armamentarium for infection control and prevention. Clinical
Infectioous Diseases 2008 Vol 47; 274-281)
–
Denton, GW: Chlorhexidine. In Disinfection, Sterilization and Preservation, ed. Seymour S. Block. Lippincot Williams & Wilkins, Philladelphia, PA, 2001. p. 321-336. .
–
Cosmetic, Toiletry and Fragrance Association Final report on the
safety assessment of chlorhexidine/chlorhexidine diacetate/chlorhexidine dihydrochloride/chlorhexidine digluconate. J.Am.Coll.Toxicol. 12:201-
223, 1993
–
O'Sullivan, D, Qiu,Y, Glasner, JD, Blattner, FR, and Parks, PJ Antiseptic shock: surverying Escherichia coli K12's transcriptional response to chlorhexidine gluconate treatment. Am.Soc.Microbiol. 18-22, May 2003 and Assn. Pract. Inf. Control and Epidemiology. 8-13 Jun 2003.
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-2Slide 6 (Antimicrobial Comparison)Larson (1995)
-
Larson E. APIC Guideline for Handwashing and Antisepsis in Health Care Settings. American Journal of Infection Control. 1995; 23(4):251-269.
Slide 7, 9 (Sources of CR-BSI)Crnich (2002)
Crnich C, Maki D. The promise of novel technology for the prevention of intravascular device-
related bloodstream infections. II Long-term devices Clin Infect Dis, 2002;34: 1362-1368
Slide 8,11 (Sources of CR-BSI)Ryder (2006), Safdar (2004), Eliott (1997)
-
Ryder, M. Evidence-based practice in the management of vascular access devices for home parenteral nutrition therapy. Journal of Parenteral and Enteral Nutrition. 2006;30 (SUPPL. 1), pp. S82-S93.-
Safdar N, Kluger D, Maki D. A review of risk factors for catheter-related bloodstream infections caused by percutaneously inserted, noncuffed central venous catheters: implications for preventative strategies. Medicine 2002; 81; 466-79-
Elliott, T.S.J. "Novel approach to investigate a source of microbial contamination of central venous catheters". European journal of clinical microbiology & infectious diseases (0934- 9723)1997;16 (3),
p. 210.
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-3Slide 10 (Common pathogens)Slide from Rupp Presentation
-
CDC Guidelines for the prevention of intravascular catheter-related infections MMWR Aug 9, 2002 Vol.51/No. RR-10
Slide 11 (Skin contamination)Mermel L (1991), O’Grady (2002), Tanzer (1994), Bjornson (1982), Maki (1976)+ Ryder (2006), Safdar (2004), Eliott (1997)
-
Mermel L (1991) The pathogenesis and epidemiology of catheter-related infection with pulmonary artery Swan-Ganz catheters: A prospective study utilizing molecular sub-typing. Am H of Med 1991 91 (3B) 197S-205S-
O’Grady, Alexander , Dellinger E, et al Guidelines for the prevention of intravascular catheter-
related infections CDC Morbidity and mortality weekly report Aug
9, 2002 Vol.51/No. RR-10-Tanzer M, Miller J, Richards GS, Preoperative assessment of skin
colonization. Clin Orthop 1994; 299: 163-168-Bjornson HS (1982) Association between microorganism growth at the catheter insertion site and colonization of the catheter in patients receiving total parenteral nutrition. Surgery. 1982. 92:720-
727.-Maki D (1976) Sepsis arising from extrinsic contamination of the
infusion and measures for control. Chapter 7 in Microbiological hazards of Infusion Therapy Ed Phillips I, Meers PD, Arcy PFD. 1976 Publishing Sciences Group Littleton Mass. 99-143
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-4Slides 12, 13 (Biofilm)Ryder (2005)
-
Ryder, M.A. (2005). "Catheter-related infections: It's all about biofilm". Topics in advanced practice nursing (1535-2250), 5 (3).
Slide 14 (Impact of Skin Flora)Hadaway (2003), Ryder (2001), Richardson (2006)
-
Hadaway L. Skin Flora and Infection. 2003 Journal of Infusion Nursing. 26(1):44-48.-Ryder, M. The role of biofilm in vascular catheter-related infections. New Dev Vascular Dis. 2001;2:15-25.-Richardson DK. Vascular Access Nursing Practice, Standards of Care, and Strategies to Prevent Infection: A Review of Skin Cleansing Agents and Dressing Materials (Part 1 of a 3-Part Series). J Assoc Vasc Access 2006 Vol 11 No 4.
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-5Slide 15 (Impact of Skin Flora)Safdar (2002), O’Grady (2002), Weinstein (1991)
-
Safdar N, Kluger D, Maki D. A review of risk factors for catheter-related bloodstream infections caused by percutaneously inserted, noncuffed central venous catheters: implications for preventative strategies. Medicine 2002; 81; 466-79.
-
O'Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002 Aug 9;51(RR-10):1-29.
-
Weinstein, R.A.
Epidemiology and control of nosocomial infections in adult intensive care units. American Journal of Medicine. 1991; 91 (3 SUPPL.2), pp. 3B-179S-3B-184S5.
Slide 17 (Clinicians want)Voice of Customer (VOC); Data on File
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-6Slide 18 (Tegaderm CHG)Maki (2008), Schwab (2008) Schwab (2008)
- Maki, DG (2008) A Novel Integrated Chlorhexidine-Impregnated Transparent Dressing for Prevention of Vascular Catheter-related Bloodstream Infection: A Prospective Comparative Study In Healthy Volunteers. SHEA, April 2008 -
Schwab, D (2008) Migration of Chlorhexidine Gluconate Under Antimicrobial Gel Pad of IV Securement Dressing to Provide Continual Antimicrobial Protection. Association for Vascular Access (AVA), Sept. 2008 -
Schwab, D (2008) Antimicrobial Activity of a CHG-Impregnated Gel Pad for IV Site Protection. Infusion Nurses Society (INS), May 2008
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-7Slide 19 (Tegaderm CHG)Maki (2008), Olson (2008) Eyberg (2008), Rupp (2008)
-
Maki, DG (2008) A Novel Integrated Chlorhexidine-Impregnated Transparent Dressing for Prevention of Vascular Catheter-related Bloodstream Infection: A Prospective Comparative Study In Healthy Volunteers. SHEA, April 2008 -Olson C, (2008) Clinical Performance of a New Transparent Chlorhexidine Gluconate Central Venous Catheter Dressing. Journal of the Association for Vascular Access (JAVA) March 2008 Vol 13 No. 1 13-19 -
Eyberg, C. (2008) A Controlled Randomized Prospective Comparative Study to Evaluate the Ease of Use of a Transparent Chlorhexidine
Impregnated Gel Dressing Versus A Chlorhexidine Disk in Healthy Volunteers. Journal of the Association for Vascular Access (JAVA), Fall 2008 Vol. 13 No 3 -
Rupp, ME (2008) Prospective, Randomized, Controlled Trial Assessing the Clinical Performance of a Transparent Chlorhexidine
Gel Pad Intravascular Catheter Dressing. SHEA, April 2008
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-8Slide 21 (What Data)
Voice of Customer (VOC); Data on File
Slide 24 (Fluid Absorption)Data on File: Study 05-010658; Asmus, B. Fluid absorption study
Slides 25, 26 (Broad Spectrum Antimicrobial)
-O’Grady (2002), In-vitro Time Kill LIMS 9392, Schwab (2008) O’Grady, Alexander , Dellinger E, et al Guidelines for the prevention of intravascular catheter-related infections CDC Morbidity and mortality weekly report Aug 9, 2002 Vol.51/No. RR-10 -In-vitro Time Kill LIMS 9392; Data on file-Schwab, D (2008) Migration of Chlorhexidine Gluconate Under Antimicrobial Gel Pad of IV Securement Dressing to Provide Continual Antimicrobial Protection. Association for Vascular Access (AVA), Sept. 2008
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-9Slides 27, 28, 29, 30 (Agar, Zones of Inhibition)
-
Schwab, D (2008) Antimicrobial Activity of a CHG-Impregnated Gel Pad for IV Site Protection. Infusion Nurses Society (INS), May 2008
Slide 31 (Migration of CHG under Catheter; MALDI)
-
Schwab, D (2008) Migration of Chlorhexidine Gluconate Under Antimicrobial Gel Pad of IV Securement Dressing to Provide Continual Antimicrobial Protection. Association for Vascular Access (AVA), Sept. 2008
Slides 32, 33 (Reduction of Skin Flora)
- Maki, DG (2008) A Novel Integrated Chlorhexidine-Impregnated Transparent Dressing for Prevention of Vascular Catheter-related Bloodstream Infection: A Prospective Comparative Study In Healthy Volunteers. SHEA, April 2008
Slide 34 (Use with ChloraPrep)
-
Olson L Suppression of Regrowth of Normal Skin Flora under Chlorhexidine Gluconate Dressings Applied to CHG-Prepped Skin ICAAC IDSA Oct 2008
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-10Slide 36 (Abbott Northwestern Clinical Use Study)
Olson C, (2008) Clinical Performance of a New Transparent Chlorhexidine Gluconate Central Venous Catheter Dressing. Journal of the Association for Vascular Access (JAVA) March 2008 Vol 13 No. 1 13-19
Slide 37 (University of Nebraska Clinical Use Study)
Rupp, ME (2008) Prospective, Randomized, Controlled Trial Assessing the Clinical Performance of a Transparent Chlorhexidine
Gel Pad Intravascular Catheter Dressing. SHEA, April 2008
Slide 38Eyberg, C. (2008) A Controlled Randomized Prospective Comparative Study to Evaluate the Ease of Use of a Transparent Chlorhexidine
Impregnated Gel Dressing Versus A Chlorhexidine
Disk in Healthy Volunteers. Journal of the Association for Vascular Access (JAVA), Fall 2008 Vol. 13 No 3
Slide 39Data on File: Evaluation 00040 CVE Deschneau, M 2008 A Multicenter prospective open label evaluation of the clinical performance of a chlorhexidine
gluconate
antimicrobial transparent dressing. Manuscript submitted
3M Skin & Wound Care
© 3M 2008. All Rights Reserved.
References-11Slide 40, 41 (CR-BSI Studies)Infection Rate Studies
- Pronovost, P. (2006). "An intervention to decrease catheter-related bloodstream infections in the ICU". 2006 New England Journal of Medicine 355 (26), pp. 2725-2732 (65 facilities, 103 ICUs, 1 ½
years)- Warren, D.K. (2006). Cosgrove Perl "A multicenter intervention to prevent catheter-associated bloodstream infections". Infection control and hospital epidemiology (0899-823X), 27 (7),
p. 662. (6 facilities, 13 ICUs, 2years)-
Berenholtz S, Pronvost P, Lipsett P Trish Perl. Eliminating catheter related bloodstream infections in the intensive care unit. Crit Care Med 2004 32 (10) 2014-2020 (2 ICUs, 5 years)
BioPatch Studies-
Levy, I., J. Katz, et al. (2005). "Chlorhexidine-impregnated dressing for prevention of colonization of central venous catheters in infants and children: a randomized controlled study." Pediatr Infect Dis J 24(8): 676-9-
Garland J, Harris M, Alex C, et al A randomized trial comparing povidone-iodine to chlorhexidine gluconate impregnated dressing for prevention of central venous catheter infections in neonates. Pediatrics 2001 107: 1431-
1437-Ho K M, Litton (2006) Use of chlorhexidine-impregnated dressing to prevent vascular and epidural catheter colonization and infection: A meta-analysis
2006 Journal of Antimicrobial Chemotherapy 58 (2), pp. 281-287Skin Flora’s Correlation
-
O’Grady, Alexander , Dellinger E, et al Guidelines for the prevention of intravascular catheter-related infections CDC Morbidity and mortality weekly report Aug 9, 2002 Vol.51/No.
RR-10- Mermel L (1991) The pathogenesis and epidemiology of catheter-related infection with pulmonary artery Swan-
Ganz catheters: A prospective study utilizing molecular sub-typing. Am H of Med 1991 91 (3B) 197S-205S-
Maki D (1976) Sepsis arising from extrinsic contamination of the infusion and measures for control. Chapter 7 in Microbiological hazards of Infusion Therapy Ed Phillips I, Meers
PD, Arcy PFD. 1976 Publishing Sciences Group Littleton Mass. 99-143
Tegaderm CHG Skin Flora- Maki, DG (2008) A Novel Integrated Chlorhexidine-Impregnated Transparent Dressing for Prevention of Vascular Catheter-related Bloodstream Infection: A Prospective Comparative Study In Healthy Volunteers. SHEA, April 2008
Evidence Based PracticeSackett, D.L. (1996). "Evidence based medicine: What it is and what it isn't. It's about integrating individual clinical expertise and the best external evidence". BMJ. British medical journal (International ed.) (0959-8146), 312 (7023),
p. 71.





























