Embed Size (px)
Citation preview

Acoustic schwannoma/ neuroma
Less then 1 cm tumour / no hearing impairment
- Observation
- Yearly MRI scan & audiometry
Early small tumor: (size <2.5 cm)
- Hearing function present: Radiosurgery
- Hearing function not present: Radiosurgery or surgery
Larger tumour (>3.5 cm) / brainstem compression
- Facial Nr preservation not possible: Surgery
- Facial Nr Preservation possible: Surgery only with complication
Safe Surgery + radiosurgery
- Surgery not possible: Fractionated radiotherapy
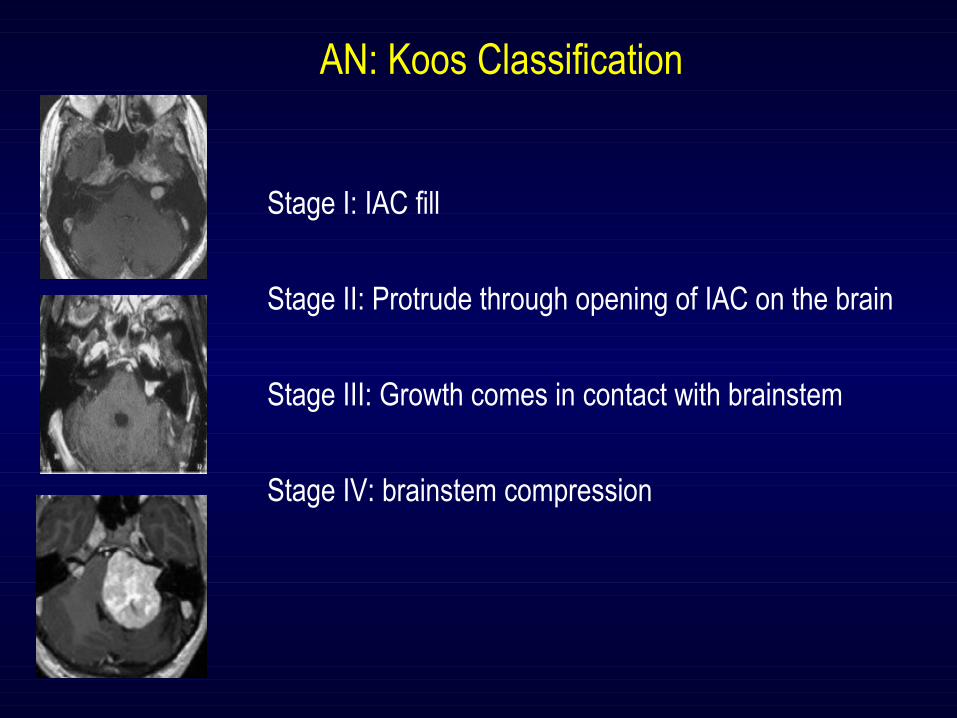
Stage I: IAC fill
Stage II: Protrude through opening of IAC on the brain
Stage III: Growth comes in contact with brainstem
Stage IV: brainstem compression
AN: Koos Classification

Prospective studies: >100Total number of patient treated with RS: >10,000 Follow up period: ≈20 yrs
In AN <2.5 cm treated with SRS, PFS at 20 years – 95-98% Facial Nr palsy – 0.5% Symptomatic Progression – 2-3% Severe toxicity – 0.1%
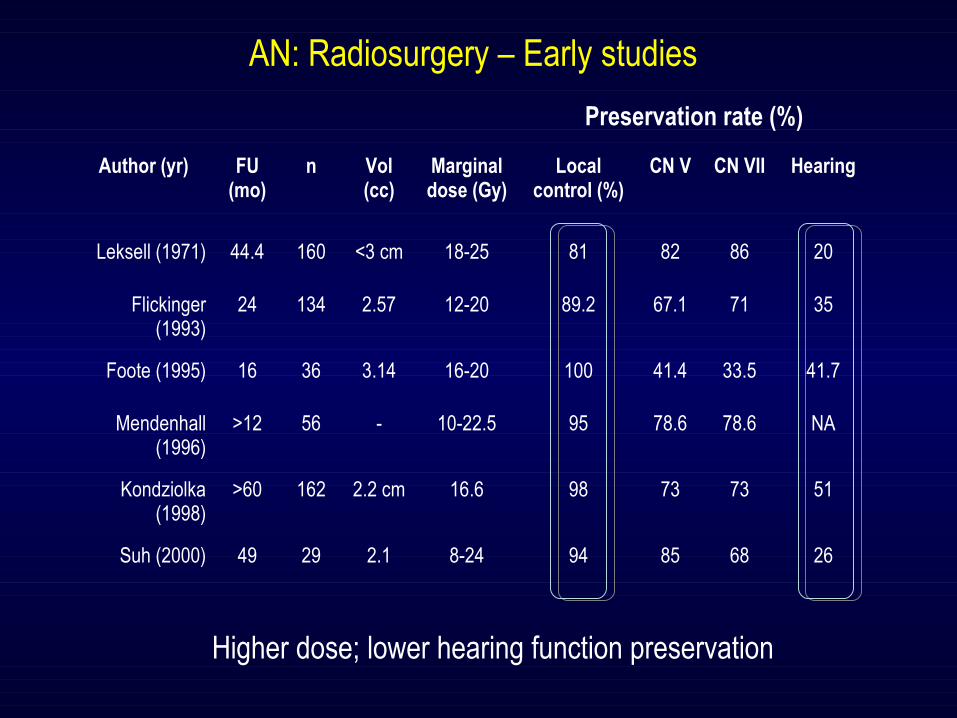
AN: Radiosurgery – Early studies
Higher dose; lower hearing function preservation
Preservation rate (%)
Author (yr) FU(mo)
n Vol (cc)
Marginal dose (Gy)
Local control (%)
CN V CN VII Hearing
Leksell (1971) 44.4 160 <3 cm 18-25 81 82 86 20
Flickinger (1993)
24 134 2.57 12-20 89.2 67.1 71 35
Foote (1995) 16 36 3.14 16-20 100 41.4 33.5 41.7
Mendenhall (1996)
>12 56 - 10-22.5 95 78.6 78.6 NA
Kondziolka (1998)
>60 162 2.2 cm 16.6 98 73 73 51
Suh (2000) 49 29 2.1 8-24 94 85 68 26

AN: Radiosurgery – Dose <13 Gy, long term FU
Author (yr) n FU (yr) Vol (cc)
MedianDose (Gy)
Local control (%)
CN V CN VII Hearing
Prasad (2000) 153 4.27 2.6 13 92 98.3 98.4 58
Unger (2002) 100 6.3 3.4 13 96 100 98 55
Chopra (2007) 216 5.7 1.3 13 93 96 94 68
Hasegawa (2005) 317 >5 - 12 93 100 94 60
Myrseth (2005) 103 >4 - 12.5 93 - 98.3 33.3
Kim (2007) 59 6 3.4 12 93 - 98.3 32
Iwai (2008) 25 7.4 0.27 12 100 100 100 64
Niranjan (2008) 96 3.5 - 13 99 100 100 64.5
Fukuoka (2009) 152 >5 2 12 94 97.4 100 64.5
Murphy (2010) 103 3.6 1.95 13 91.5 92 95 55
Combs (2006) 26 9 2.2 12.5 99 99.3 99.3 NA
Friedman (2006) 295 3.3 1.5 13 91 92 95 55
Kalogeridi (2009) 19 4.6 11 13 99.3 99.3 99.3 NA
Lower dose; Higher hearing function preservation; less toxicity
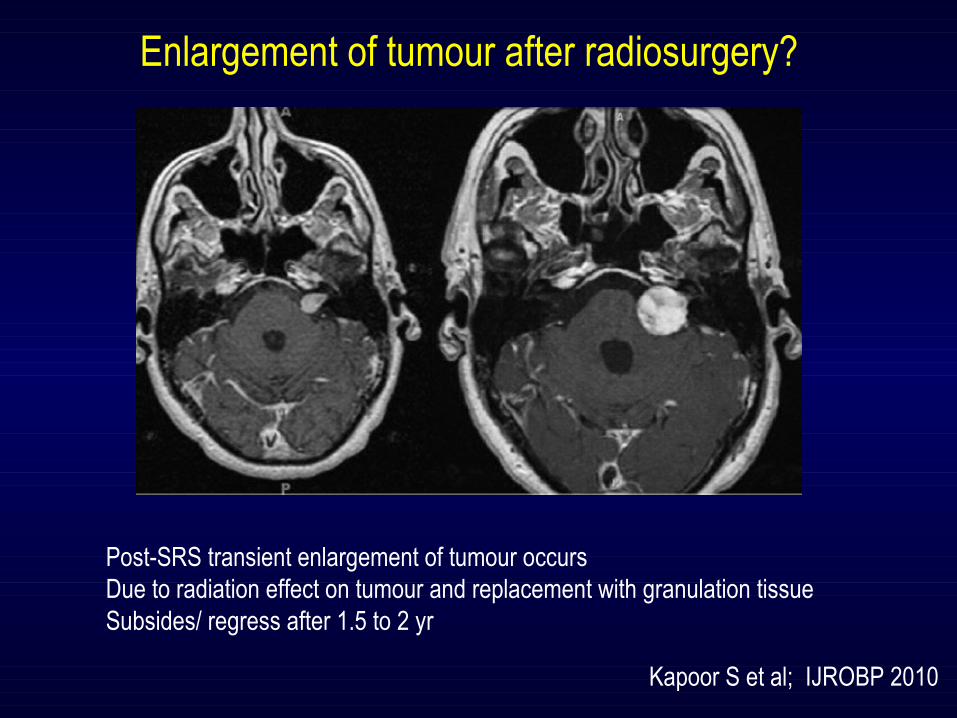
Enlargement of tumour after radiosurgery?
Post-SRS transient enlargement of tumour occursDue to radiation effect on tumour and replacement with granulation tissueSubsides/ regress after 1.5 to 2 yr
Kapoor S et al; IJROBP 2010

Kondziolka et al NEJM 1998
Prospective evaluation of AN pts (n=162)
Regression of tumour in majority of ptsRegression is slow & occurs over years

Mar
gina
l Dos
e (G
y)
Year
7-45 Gy
20 Gy
15 Gy12 Gy
Local control maintained (>95% at 10 years)Toxicities have come downHearing preservation increased
RT dose (Gy) Complication rate (%)
10-12.5 13
15-17.5(TV<5.5 cm3)
9
15-17.5 (TV>5.5 cm3)
71
20-22.5 100
Dose reduction have reduced toxicity without compromise on local control
Mendenhal et al 2000

Hydrocephalus
Vertigo/ tinnitus
Cranial Nr Palsy
Complications depends upon dosage schedule

Surgery possible after SRS ?
After SRS only few patients progress, they need surgery
SRS causes regression of blood supply, hence should be easy for resection
In a study, 8/13 pts with progression after SRS had difficult surgery !!
No clear contraindication of surgery after RS
Pollock et al; J Neurosurg 1998

Higher risk of second malignancy after SRS ?
After radiosurgery risk of second malignancy is very low
No report of any second malignancy after 7500 AN pt treatment in 18 yrs
Estimated risk 1: 1000 (0.001%)
Only two reported case of second malignancy
1. In Japan 4 yrs after surgery
2. Temporal lobe GBM 7.5 yrs after radiosurgery
Kondziolka et al 2000
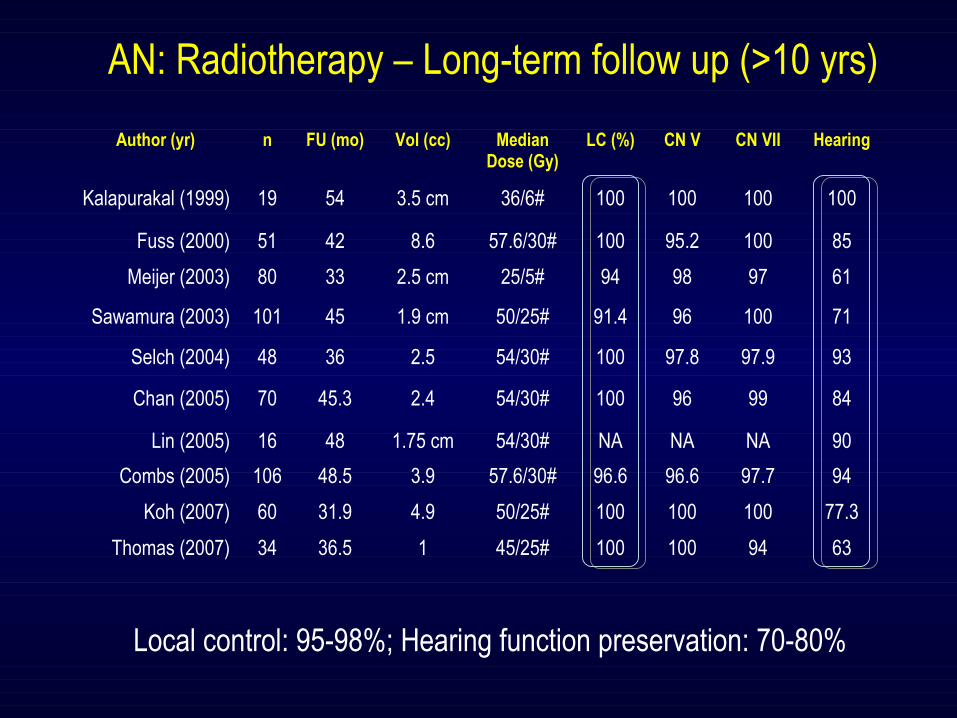
AN: Radiotherapy – Long-term follow up (>10 yrs)
Local control: 95-98%; Hearing function preservation: 70-80%
Author (yr) n FU (mo) Vol (cc) MedianDose (Gy)
LC (%) CN V CN VII Hearing
Kalapurakal (1999) 19 54 3.5 cm 36/6# 100 100 100 100
Fuss (2000) 51 42 8.6 57.6/30# 100 95.2 100 85
Meijer (2003) 80 33 2.5 cm 25/5# 94 98 97 61
Sawamura (2003) 101 45 1.9 cm 50/25# 91.4 96 100 71
Selch (2004) 48 36 2.5 54/30# 100 97.8 97.9 93
Chan (2005) 70 45.3 2.4 54/30# 100 96 99 84
Lin (2005) 16 48 1.75 cm 54/30# NA NA NA 90
Combs (2005) 106 48.5 3.9 57.6/30# 96.6 96.6 97.7 94
Koh (2007) 60 31.9 4.9 50/25# 100 100 100 77.3
Thomas (2007) 34 36.5 1 45/25# 100 100 94 63

Comparative study: Fractionated RT Vs SRS
Author (yr) RT type n FU (mo) Dose (Gy)
LC (%) CN V CN VII Hearing
Andrews Philadelphia
(2001)
FSRT 56 115 Wk 50/25# 97 93 98 81
SRS 69 115 Wk 12 98 95 98 33
CombsHiedelburg
(2010)
FSRT 172 75 mo 57.6/33# 96 97 98 78
SRS 19 75 mo <13Gy 96 100 95 78
SRS 11 75 mo >13Gy 96 93 88 NA
Kopp Germany (2011)
FSRT 47 32.1 54/30# 97.9 NA 100 79
SRS 68 30.1 12 98.5 NA 100 85
Collen Belgium (2011)
FSRT 78 62 50/25# 95 NA 88 68
SRS 41 62 12.5 95 NA 88 59
No difference in local control, hearing preservation & toxicity profile

Fractionated RT Vs SRS (n=202)
Local Control: FSRT vs SRS ( FU= 75 mo)
Coumb et al IJROBP 2000
FSRT vs SRS: No difference in local control
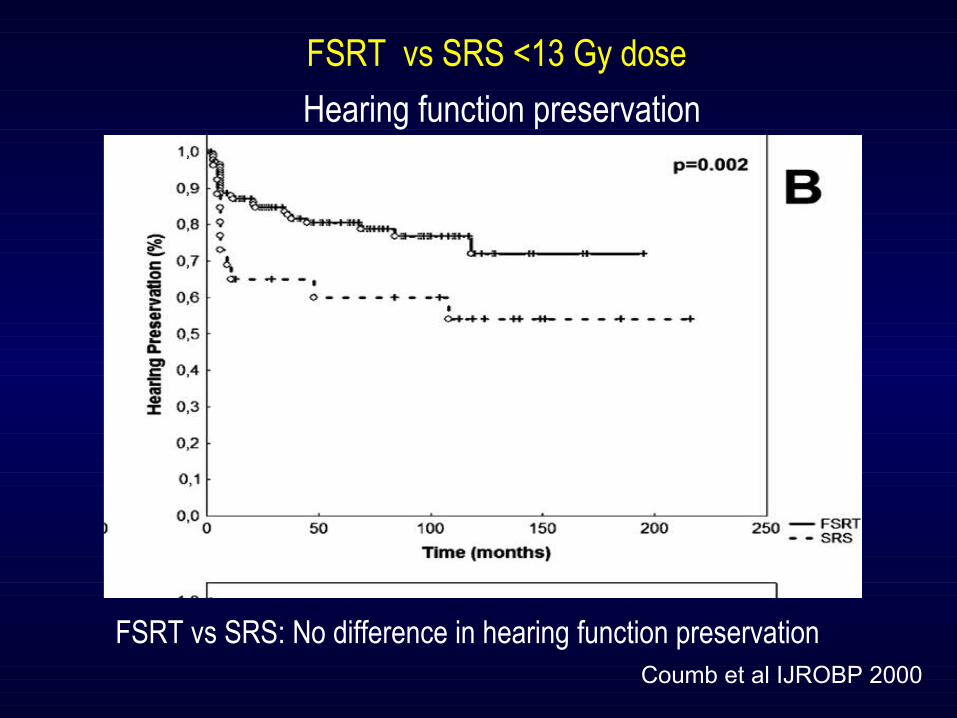
FSRT vs SRS <13 Gy dose
Coumb et al IJROBP 2000
FSRT vs SRS: No difference in hearing function preservation
Hearing function preservation
CLINICAL INVESTIGATION
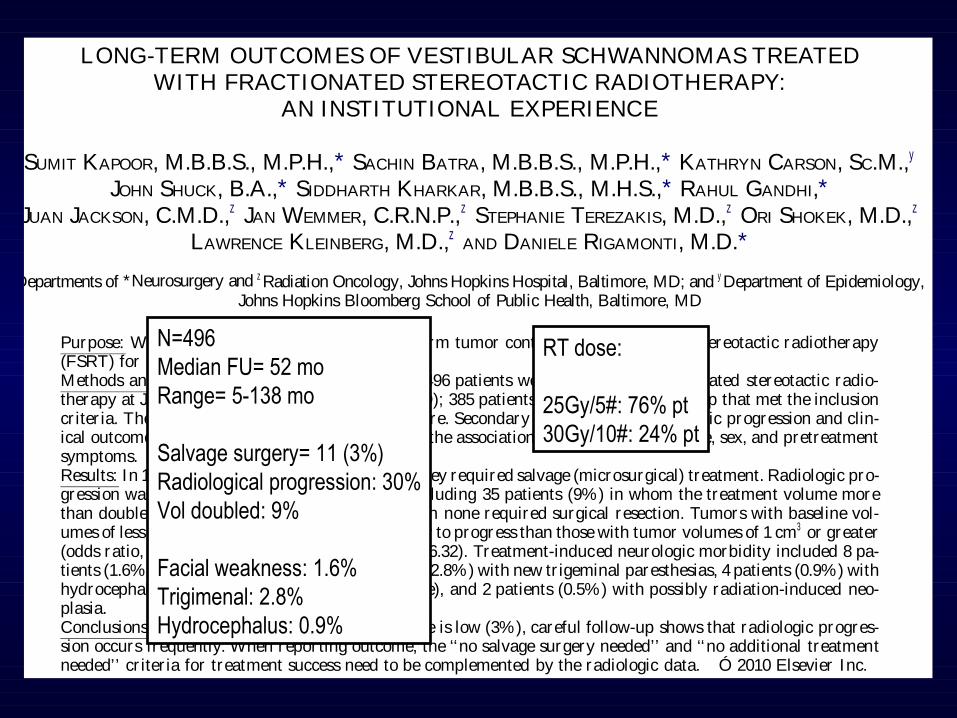
LONG-TERM OUTCOMESOF VESTIBULAR SCHWANNOMASTREATEDWITH FRACTIONATED STEREOTACTIC RADIOTHERAPY:
AN INSTITUTIONAL EXPERIENCE
SUMIT KAPOOR, M.B.B.S., M.P.H.,* SACHIN BATRA, M.B.B.S., M.P.H.,* KATHRYN CARSON, SC.M.,y
JOHN SHUCK, B.A.,* SIDDHARTH KHARKAR, M.B.B.S., M.H.S.,* RAHUL GANDHI,*JUAN JACKSON, C.M.D.,z JAN WEMMER, C.R.N.P.,z STEPHANIE TEREZAKIS, M.D.,z ORI SHOKEK, M.D.,z
LAWRENCE KLEINBERG, M.D.,z AND DANIELE RIGAMONTI, M.D.*
Departmentsof *Neurosurgery and zRadiation Oncology, JohnsHopkinsHospital, Baltimore, MD; and yDepartment of Epidemiology,Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
Purpose: Weassessed clinical outcome and long-term tumor control after fractionated stereotactic radiotherapy(FSRT) for unilateral schwannoma.Methods and Mater ials: Between 1995 and 2007, 496 patients were treated with fractionated stereotactic radio-therapy at JohnsHopkins Hospital (Baltimor e, MD); 385 patients had radiologic follow-up that met the inclusioncr iter ia. Thepr imary endpoint was treatment failure. Secondary endpoints were radiologic progression and clin-ical outcome. Logistic regression analysis assessed the association of age, race, tumor side, sex, and pretreatmentsymptoms.Results: In 11patients (3%) treatment failed, and they required salvage(microsurgical) treatment. Radiologic pro-gression was observed in 116 patients (30.0%), including 35 patients (9%) in whom the treatment volume morethan doubled dur ing the follow-up per iod, although none required surgical resection. Tumors with baseline vol-umesof lessthan 1 cm3 were18.02 timesmore likely to progressthan thosewith tumor volumesof 1 cm3 or greater(odds ratio, 18.02; 95% confidence interval, 4.25–76.32). Treatment-induced neurologic morbidity included 8 pa-tients (1.6%) with new facial weakness, 12patients (2.8%) with new tr igeminal paresthesias, 4patients (0.9%) withhydrocephalus (1 communicating and 3 obstructive), and 2 patients (0.5%) with possibly radiation-induced neo-plasia.Conclusions: Although the rate of treatment failure is low (3%), careful follow-up shows that radiologic progres-sion occurs frequently. When repor ting outcome, the ‘‘no salvage surgery needed’’ and ‘‘no additional treatmentneeded’’ cr iter ia for treatment success need to be complemented by the radiologic data. Ó 2010 Elsevier Inc.
Vestibular schwannoma, Fractionated stereotactic radiotherapy, Tumor progression, Clinical outcomes.
INTRODUCTION
The vestibular schwannoma (VS) is a benign tumor arisingfrom the Schwann cells of the vestibulocochlear nerve. Theoverall incidence of VS is about 1 per 100,000 person-years, and it appears to be increasing (1, 2). The prevalenceof incidental VS is reported to be between 2 and 7 in10,000 people (3, 4), implying that the numbers ofasymptomatic VS may be larger than previously suspected.Patients with VSs most commonly present with unilateralhearing problems, hearing loss, or tinnitus, which is usuallyprogressive. Other less common symptoms are vertigo, gaitimbalance, facial numbness, and facial tingling.
Magnetic resonance imaging (MRI), enabling detection oftumorsassmall as1 to 2mm in diameter, hasmadepossibleearlier diagnosis (5) and easy follow-up of these tumors.Measurements from MRI scans can reliably detect changesassmall as1.1 mm in tumor diameter and 0.15 cm3 in tumorvolume (6).Surgical resection hasbeen thepreferred treatment modal-
ity for thepast 50 years, but nowmany centersoffer radiation(4) as the first treatment. The rationale for this choice is thattotal removal is not always feasible without significant mor-bidity (7), whereasradiation aimed at arresting tumor growthseems to be associated with fewer complications (8, 9).
Reprint requests to: DanieleRigamonti, M.D., Phipps126, 600NWolfe St., Baltimore, MD 21287. Tel: (410) 955-2259; Fax: (410)955-9126 E-mail: [email protected] work was supported by grants from the Salisbury Founda-
tion, theMonicaandHermenGreenberg Foundation, and theSwen-son Foundation. These grants supported design and conduct of the
study; collection, management, analysis, and interpretation of thedata; and preparation, review, or approval of themanuscript.Conflict of interest: none.Received Feb 15, 2010, and in revised form April 20, 2010.
Accepted for publication June 7, 2010.
1
Int. J. Radiation Oncology Biol. Phys., Vol. - , No. - , pp. 1–7, 2010Copyright Ó 2010 Elsevier Inc.
Printed in theUSA. All rights reserved0360-3016/$–see front matter
doi:10.1016/j .ij robp .2010.06.006
ARTICLE IN PRESS
N=496Median FU= 52 moRange= 5-138 mo
Salvage surgery= 11 (3%)Radiological progression: 30%Vol doubled: 9%
Facial weakness: 1.6%Trigimenal: 2.8%Hydrocephalus: 0.9%
RT dose:
25Gy/5#: 76% pt30Gy/10#: 24% pt

Larger volume tumour treated with high dose have radiological progression
Radiological progression with fSRT

Gender (M:F) 7:9
Age Median (range) (yrs) 51(19-74)
Side (R:L:BL) 9:21:2
Pre-SRS hearing function
Serviceable HL 20 (63%)
Non-Serviceable HL 12 (37%)
Pre-SRS facial function status
H-B Scale I 22(69%)
H-B Scale II 3 (9%)
H-B Scale III 5 (15%)
H-B Scale IV -
H-B Scale V 2 (7%)
SRS TechniqueFrameless
Framebased19 (59%)13 (41%)
Dose Median (range) (Gy) 14 (12-26.2)
FU Median (range) (mo) 6.5 (6-8)
ASH Experience: (n=32)
Balaji, Mahadev, Dutta et al, AROICON 2011
N=32CyberKnife: 19 ptBrainLAB: 13 pt
Serviceable hearing function : 20 pt
N=32CyberKnife: 19 ptBrainLAB: 13 pt
Serviceable hearing function : 20 pt
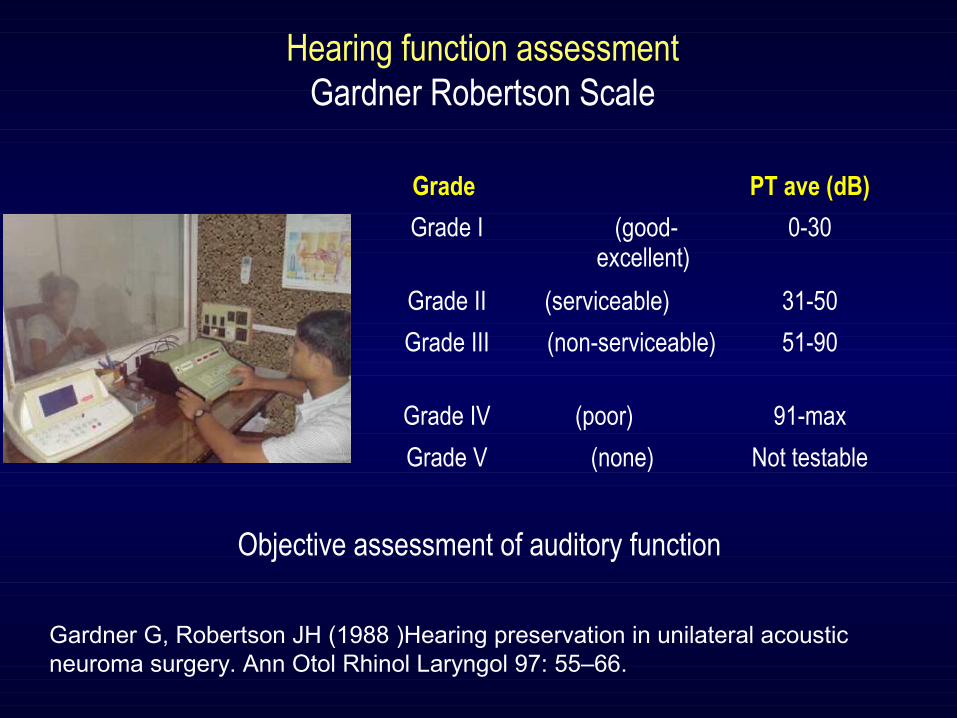
Grade PT ave (dB)
Grade I (good-excellent)
0-30
Grade II (serviceable) 31-50
Grade III (non-serviceable)
51-90
Grade IV (poor) 91-max
Grade V (none) Not testable
Hearing function assessmentGardner Robertson Scale
Gardner G, Robertson JH (1988 )Hearing preservation in unilateral acoustic neuroma surgery. Ann Otol Rhinol Laryngol 97: 55–66.
Objective assessment of auditory function

Grade Description Measurement Function %
I Normal 8/8 100
II Slight 7/8 76 - 99
III Moderate 5/8 - 6/8 51 - 75
IVModerately
Severe3/8 - 4/8 26 - 50
V Severe 1/8 - 2/8 1 – 25
VI Total 0/8 0
House Brackman Scale
"Measurement" is determined by measuring the superior movement of mid-portion of the superior eye brow and the lateral movement of oral commissure. A scale point of 1 is assigned for each 0.25 cm of motion up to 1 cm for both eye brow and commissure movement. The points are then added together.
Facial function assessment

Post-SRS Pre SRS
Total**I II III IV
I 3 0 0 0 3
II 4 6 0 0 10
III 1 6 5 0 12
IV 0 0 6 1 7TOTAL* 8 12 11 1 32
*Total number of pts with corresponding GR scale in column pre-SRS; ** Total number of pts with corresponding GR scale in the row post-SRS; Group of pts, hearing improved or remained within 20-dB considered hearing preservation
Gardner Robertson scale: Hearing functionPre & post-SRS (6 month) evaluation
(n=32)
Post- SRS
Pre-SRSTotal**
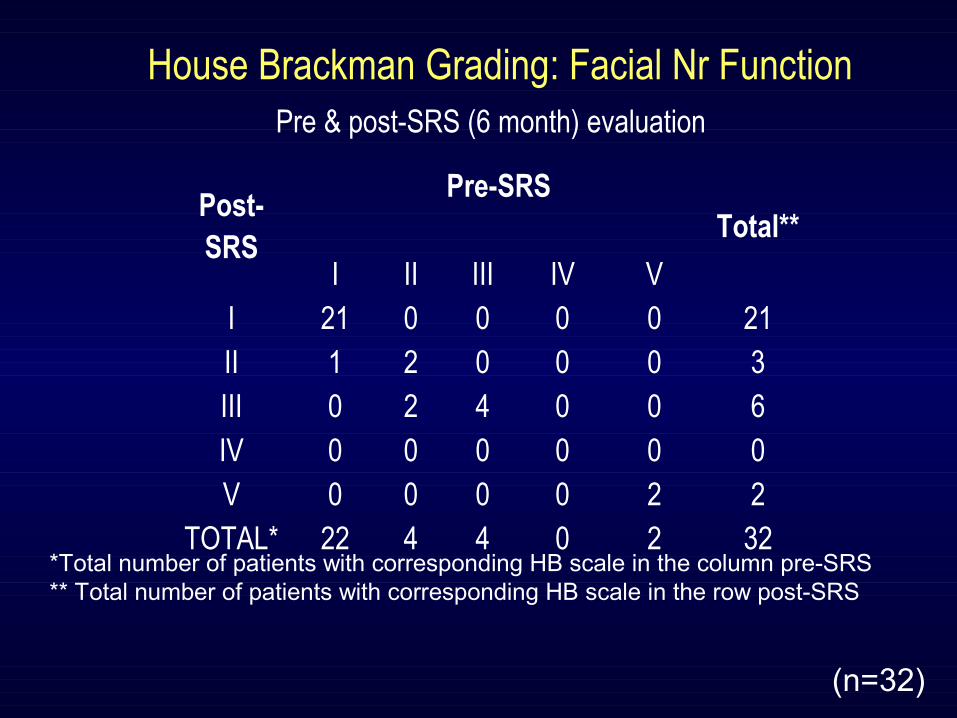
I II III IV VI 21 0 0 0 0 21II 1 2 0 0 0 3III 0 2 4 0 0 6IV 0 0 0 0 0 0V 0 0 0 0 2 2
TOTAL* 22 4 4 0 2 32*Total number of patients with corresponding HB scale in the column pre-SRS** Total number of patients with corresponding HB scale in the row post-SRS
House Brackman Grading: Facial Nr FunctionPre & post-SRS (6 month) evaluation
(n=32)


Dosimetric comparison between BrainLAB & CyberKnife
Unilateral AN ptServiceable hearing functionAge <25 yearsSize <3 cm
Contouring done with CT scan & MRIGTV = post-contrast enhancementPTV margin = 2 mm Dose= 13-15 Gy single fractionOARs (Choclea, Brainstem, Mesial temporal lobe)
Planning & calculation was done with appropriate calculation algorithms. Isodose plans & DVHs generated by the two systems were comparedPrescribed isodose in both the systems were considered adequate to cover at least 95% of PTV
Planning with BrainLAB systemForward planningArc no: 5-9
Planning with CyberKnife systemInverse planningBeamlet no: 70-150
(n=7)

CK BrainLAB p-value*
Mean tumour Vol (cc) 1.2±0.9 1.3±1 0.917
Conformity Index (CI) 0.53±0.06 0.58±0.07 0.225
10Gy Vol (cc) 3.2±1.1 5.2±1.6 0.017
5Gy Vol (cc) 11.8±4.9 16.8±6.2 0.129
2.5Gy Vol (cc) 39.9±17.2 52.3±19.8 0.238
Max dose brainstem (Gy) 4.9±3.1 4.7±2.6 0.935
Mean cochlea dose (Gy) 5.4±0.6 6.9±0.7 0.001
Mean mesial temporal lobe dose (Gy) 1.7±0.9 2.6±0.9 0.07
Dutta et al, J Neurooncol 2012
Comparison BrainLAB & CyberKnife plan
No difference in target coverageHigh dose spillage significantly less with CKDose to critical structures (cochlea & temporal lobe) significantly less with CK
*Non parametric test

Pt survey: Sx vs SRS (n=1553)
Issues Surgery^ RS*
Mean tumour size 25 mm 22 mm
Offers positive recommendation
74% 95%
No change in employment 68% 69%
New balance problem 78% 7%
New onset tinnitus 57% 3%
New facial Nr Dysfunction 63% 10%
^ Martin etal Skull Base Surg 1996* Kondziolka et al J Neurosurg 2001
Patient acceptance & toxicity profile better with radiosurgery
(n=1553)
New symptoms
Hearing function preservation is possible with SRS

SRS for AN FU >5 yrs ; <10 yrs
Q. Radiosurgery met your expectation? YES 92%
Q. Was radiosurgery good treatment? YES 95%
Q. Will you recommend radiosurgery to any one? YES 95%
(n=115)
Patient satisfaction survey*
Kondziolka et al NEJM 1998

Conclusions
Koos I&II: (AN <2.5 cm)
Serviceable hearing function: SRS preferred
Non-serviceable hearing function: SRS or surgery
Koos III&IV: (Larger tumour/ brainstem compression)
Facial Nr preservation not possible: Surgery
Facial Nr Preservation possible: Surgery / Safe Surgery + SRS
Surgery not possible: FSRT

Practice survey: Neurosurgeons choice*37 yr male, 2.5 cm AN Unilateral symptomatic, serviceable hearing function
*Congress of Neurological Surgeons July 2002
Neurosurgeon’s age
(n=663)