Embed Size (px)
DESCRIPTION
Can ultrasonography diagnose adenomyosis? this talk may present an answer to this
Citation preview

Accuracy of TVUS in Adenomyosis

Introduction
• Adenomyosis is a frequent gynecologic pathology which affects women particularly in the fifth decade complaining of abnormal uterine bleeding.

• Adenomyosis is thought to affect 1% of women.
• The aetiology is unclear.

clinical presentation
• parous, perimenopausal patient with dysmenorrhea and menorrhagia.
• Physical examination may reveal an enlarged, tender uterus,

Adenomyosis
• clinical presentation may suggest adenomyosis • imaging is often used prior to treatment
selected

• but the diagnosis has been difficult to obtain without histologic confirmation.

Invasive

TVUS
• Available• Non invasive• Low cost• Operator dependent• ?? accurate


• asymmetric thickening of the anterior or posterior uterine wall or myometrial cysts which are small anechoic lakes of 2-6 mm in diameter which may represent cystic endometrial implants or focal myometrial hemorrhage, colour doppler can be used to differentiate it from myometrial vessels.




Aim of the study
• to measure the accuracy of the TVUS features in diagnosing adenomyosis
• to determine the diagnostic role of uterine artery Doppler in these cases.

• Study design:a prospective comparative study.• Setting: Cairo University hospital

363 Women
• scheduled for hysterectomy either abdominal, vaginal
• TVUS was done to detect adenomyosis • then compare the results with
histopathological findings• then evaluate if there is any relation of
adenomyosis with uterine artery Doppler indices

352 women
• 11 patients were excluded from the study either because that they diagnosed as being unfit for surgery.
• 198 Patients were premenopausal (56.3 %) while 154 were postmenopausal (43.8 %).

TVUS
• Ultrasound scanning was performed with Accuvix (Medison, Seoul, Korea) scanner using 4-7 MHZ endovaginal probe.
• Scanning was done in early morning to avoid fluctuations due to circadian rhythm of uterine artery blood flow.

Moreover
• There are different ultrasonographic features which are suggested by many studies in order to reach a diagnosis of adenomyosis.
• This lead to different accuracy in transvaginal detection of adenomyosis

Criteria examined
• uterine diameters, outline• myometrial echotexture,• myometrial linear striation,• myometrial cysts (its number if present),• endometrial myometrial junction,• uterine wall asymmetry and if there was any
associated gynecological pathology

Criteria Details
• Myometrial cysts were defined as rounded anechoic area of 2-6 mm in diameter .
• Color Doppler was used to differentiate the myometrial cysts from myometrial blood vessels.
• Heterogenous myometrium was defined by the presence of an indistinctly marginated myometrial area with decreased or increased echogenicity


More details
• heterotopic endometrium extending into the inner myometrium can appear as echogenic linear striations. When these lines are small or indistinct, pseudo-widening of the endometrium or poor delineation of the endomyometrial junctional zone is seen.
• Globular and/or asymmetric uterus was defined as a regular enlarged uterus with possible myometrial asymmetry unrelated to leiomyoma.

Histopathology
• the pathologist was blinded to the US and clinical findings.
• adenomyosis was diagnosed by migration of the endometrial glands from the stratum basale into the myometrium. The ectopic glands tend to be at least 2-3 mm below the endometrial-myometrial junction.

• Adenomyosis was found in 37/352 (10.5 %) patients at the histopathological examination. Other pelvic pathology was associated in 10/37 of the adenomyotic cases (27.77%).

• Leiomyomas were the most commonly associated gynecological pathology with adenomyosis (6/37, 16.2%) then endometrial hyperplasia (3/37, 8.3 %) and ovarian cyst (1/37, 2.7%).

• Transvaginal ultrasound diagnosed adenomyosis in 48 cases out of 352 cases scheduled for hysterectomy, of whom, only 37 cases had a histopathological diagnosis of adenomyosis. (~10%)

• The sensitivity, specificity, negative predictive value, positive predictive value and accuracy of transvaginal ultrasound in the diagnosis of adenomyosis were: 7 5.68%, 90.79%, 49.12%, 96.95% and 89.20 %respectively.

Adenomyosis
(n = 37)
No adenomyosis
(n = 315)
P
Globular uterus
Yes
No
25(67.6)
12(32.4)
228(72.4)
87(27,6)
0.538
Asymmetrical anterior-posterior uterine wall
Yes
No
12(32.4)
25(67.6)
86(27.3)
229(72.7)
0.510
Heterogeneous myometrial echotexture
Yes
No
35(94.6)
2(5.4)
175(55.6)
140(44.4)
< 0.001
Poor Endometrial Delineation
Yes
No
28(75.7)
9(24.3)
144(45.7)
171(54.3)
< 0.001
Linear myometrial striation
Yes
No
18(48.6)
19(51.4)
29(9.2)
286(90.8)
< 0.001
The Presence of myometrial cysts
Yes
No
26(70.3)
11(29.7)
144(45.7)
171(54.3)
0.005

Accuracy of different ultrasonographic features for diagnosing adenomyosis
Sensitivity Specificity PPV NPV accuracyHeterogeneous myometrial echotexture
94.59 44.44 16.67 98.59 49.72
Poor Endometrial Delineation 75.68 54.29 16.28 95.00 56.53
Linear myometrial striation 48.65 90.79 38.30 93.77 86.36
The Presence of myometrial cysts 70.27 54.29 15.29 93.96 55.97
Myometrial cysts > 2 96.15 100.00 100.00 99.31 99.41

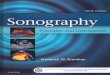
ultrasonographic features(myometrial cysts (arrows) and linear striations

Doppler study of the uterine artery in a case documented to have adenomyosis.

Comparison of uterine artery Doppler indices (RI and PI)
Adenomyotic cases
(n = 37)
Non adenomyotic cases
(n = 315)
P value
Uterine artery RI:
- Min- Max- Mean- SD
0.72
0.93
0.865
0.051
0.75
0.94
0.847
0.063
0.107
Uterine artery PI:
- Min- Max- Mean- SD
1.35
3.10
2.473
0.472
1.65
3.01
2.317
0.539
0.093

• no previous study measure the uterine artery Doppler in cases of adenomyosis and compare them with those who are not documented histopathologicaly to have it ,
• Also there was no other study specify the number of myometrial cysts in cases of adenomyosis

Other studies
Prevalence Sensitivity Specificity PPV NPV
Siedler et al. 8/80(10) 63 97 71 _
Fedele etal 22/43 (51) 80 74 73 81
Asher etal 17/20 (85) 86 50 90 20
Reinholdet al. 29/100 (29) 86 86 71 94
Brosen et al 28/56 (50) 53 75 86 77
Reinhold et al. 18/119 (`15) 89 89 71 96
Atzori et al. 15/175 (8.6) 86 96.2 68.4 98
Vercelini et al. 29/102(28) 82.7 67 50 90.7
Atri et al. 30/102(29.4) 81 71 54 90
Bazot et al. 40/120(33) 65 97.5 92.8 88.8
Bazot et al. 23/106(21.7) 80.9/38.4 100/97.5 100/83.3 40/82.9
Kepkek et al. 26/70(37.1) 80.8 61.4 55.3 84.4
Our study 37/352(10.5) 75.6 90.79 49.12 96.95

• This study had the privilege of including a large sample volume but still there may be a need of further studies with larger sample volume to put a scoring system including both the clinical and ultrasonographic criteria for diagnosis of adenomyosis with a high accuracy.

• We try to find if we can add uterine artery Doppler in the ultrasound features for adenomyosis but there was no statistical difference in either uterine artery Doppler indices (RI,PI) in both adenomyotic cases and non adenomyotic ones.

Limitations
• different pathologists examine the hysterectomy specimens
• in cases where there is focal adenomyosis • the inclusion of only hysterectomized cases

Conclusion
• subendometrial linear echogenic striations showed the highest specificity and accuracy .
• The myometrial cysts show a high negative predictive value and their number (if more than 2) represent the highest accuracy.
• Uterine artery Doppler study can't be used to diagnose adenomyosis.