Embed Size (px)
Citation preview
Moderator : Dr. M. S. SomannavarPresenter : Jay prakash sah
Jawaharlal Nehru Medical college, Belgaum,Karnataka,IndiaEmail:[email protected]
INTRODUCTION
REGULATION OF ACID BASE BALANCE
BLOOD BUFFERS
RESPIRATORY MECHANISM
RENAL MECHANISM
ACID BASE DISORDERS
ABG ANALYSIS
Normal blood PH : 7.35-7.45
Maintenance of blood pH - importanthomeostatic mechanism of the body.
PH less than 7.35 leads to acidosis andpH more than 7.45 leads to alkalosis.
Acids are proton donors.
HA ↔ H+ + A-
HCL ↔ H ++ CL -
Bases are proton acceptors.
NH3+H+ ↔ NH4+
HCO3+H+ ↔ H2CO3
• Weak and strong acids :
HCL → H ++ CL - (COMPLETE) - Strong acid H2CO3 → H+ + HCO3
- ( PARTIAL) - Weak acid
Acid Base

Carbonic acid - Oxidation of c-compounds
Sulphuric acid - Oxidation of sulphur containing amino acids.
Phosphoric acid-metabolism of dietary phosphoproteins ,nucleoproteins, phosphatides .
Organic acid- oxidation of carbohydrates , fats and proteins.e.g. pyruvic acid ,lactic acid , acetoacetic acid etc.
Iatrogenic : - certain medicine like NH4Cl, mandelic acid etc.
NOTE:DIET RICH IN ANIMAL PROTEIN RESULTS IN MOREACID PRODUCTION.
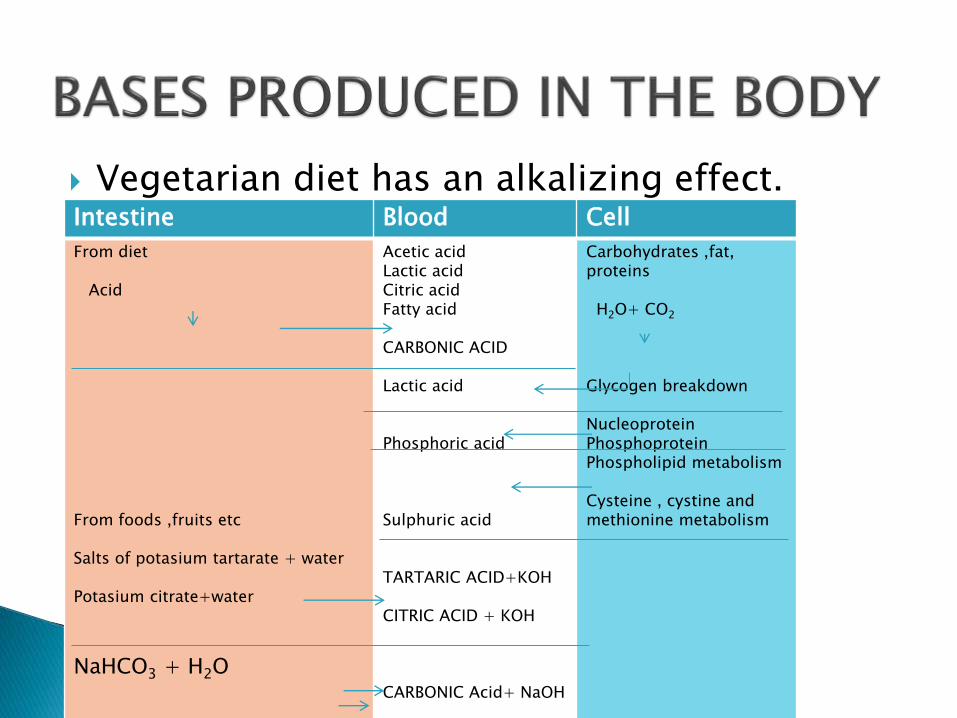
Vegetarian diet has an alkalizing effect.Intestine Blood Cell
From diet
Acid
From foods ,fruits etc
Salts of potasium tartarate + water
Potasium citrate+water
NaHCO3 + H2O
Acetic acid Lactic acid Citric acid Fatty acid
CARBONIC ACID
Lactic acid
Phosphoric acid
Sulphuric acid
TARTARIC ACID+KOH
CITRIC ACID + KOH
CARBONIC Acid+ NaOH
Carbohydrates ,fat, proteins
H2O+ CO2
Glycogen breakdown
NucleoproteinPhosphoproteinPhospholipid metabolism
Cysteine , cystine and methionine metabolism
Buffers - resist change in pH.
Two types
a) Mixture of weak acids with their salt with a strong base.
b) Mixture of weak bases with their salt with a strongacid.
Example1. Bicarbonate buffer (H2CO3 / NaHCO3 )2. Acetate buffer (CH3COOH / CH3COONa)3. Phosphate buffer (Na2HPO4 /NaH2PO4 )
If you go running you build up lactic acid in your muscles.
Therefore your pH will decrease.
Buffer will act to increase the pH.
And vice versa.
So how does it work using chemistry ?
H+ + A- → HA
OH- + HA → A- + H2O
EX;
H+ + HCO3- → H2CO3
OH- + H2CO3 → HCO3- + H2O
Acid add [ H+ ] therefore ↑ [ H+ ] - ↓ pH
Base bind [ H+ ] therefore ↓ [ H+ ] - ↑ pH .
Phosphate buffer
H2PO4 ↔ HPO42- + H+
Protein buffer
Amino acid
If pH ↓
In acidic medium amino acid (NH2) act as a base and absorbs H+.
If pH↑
In alkaline medium amino acid (COOH) act as a acid and release H+.

Acetate buffer
When HCl is added to the acetate buffer, the saltsreact with the acid forming the weak acid , aceticacid and its salts.
CH3COONa + Hcl CH3COOH + Nacl
When NaOH is added, the acid reacts with itsforming salt and water.
CH3COOH + NaoH CH3COONa +Nacl
Thus changes in pH is minimised.
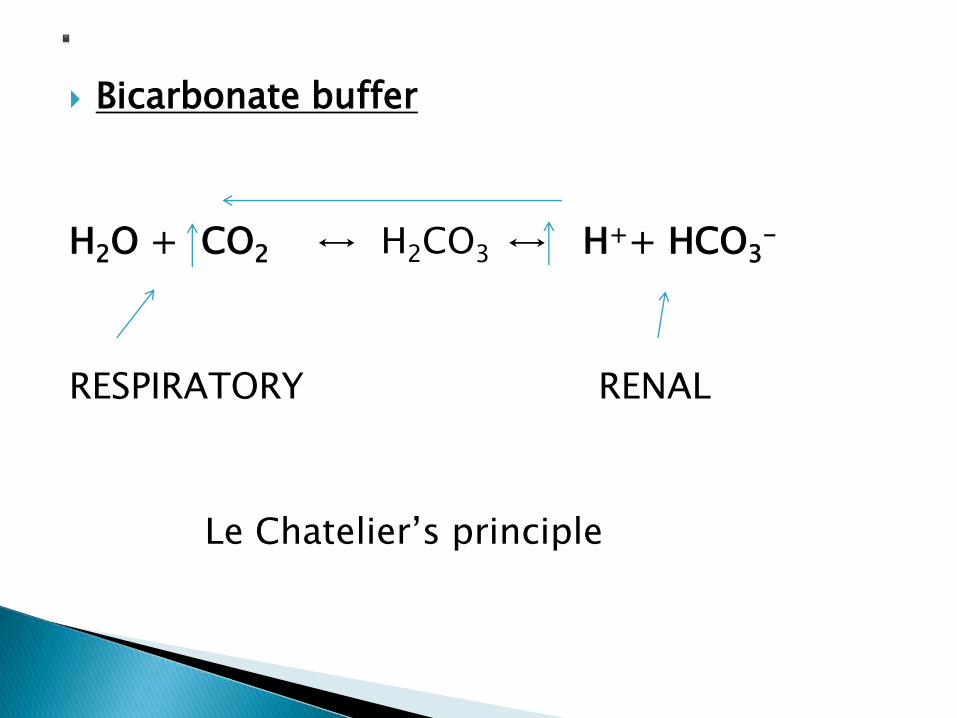
Bicarbonate buffer
H2O + CO2 ↔ H2CO3 ↔ H++ HCO3-
RESPIRATORY RENAL
Le Chatelier’s principle
1. Standard buffer solution are used withindicator for determination of pH.
2. Buffer are used to check the performance ofelectrode used for determination of pH.
3. Used for many chemical reactions includingthose catalysed by enzymes.
4. Used in the pathological laboratory to controlpH of culture media for bacteria tissues.
5. Very important in regulating the pH of bodyfluids e.g. blood, interstitial fluid ,lymph.
Sodium monohydrogen phosphate (Na2HPO4 )
Sodium dihydrogen phosphate ( NaH2PO4 )
Sodium bicarbonate ( NaHCO3 )
Hydrogen carbonate (H2CO3 )
Sodium proteinate
Hydrogen proteinate
.’ ..
erythrocytes
• Potassium bicarbonate
• Carbonic acid
• K2HPO4
• kH2PO4
• Potasium proteinate
• Hydrogen proteinate
Tissue cell
• Potassium proteinate• Hydrogen proteinate• Potasium bicarbonate• Hydrogen bicarbonate• K2HPO4
• kH2PO4
pH = - log [H+] , dimensionless quantity.
[H+] means gm of hydrated H+ ion present asH3O+ per litre of fluid .
E.g. H2O contains 1/1000000gm of hydrogen ionin 1 litre ,means [H+]=10-7.
Decrease of one pH unit represents a ten foldincrease in the H+ activity.
The pH 7.40 corresponds to a hydrogen ionconcentration of 40 nmol/L ( European centre).
Represents the negative logarithm of theionization constant of a weak acid (ka).
Pk is the pH at which an acid is halfdissociated.
Acids have pk value less than 7 and baseshave have more than 7.
Lower pk = stronger acid Higher pk = stronger base
1. Enzyme activity
2. Action potential of myelinated nerve
3. Membrane permeability
4. Control of respiration
5. Heart activity
6. Plain muscle activity
7. Oxygen Hb dissociation curve
8. Nerve excitability
3 mechanism
1. Blood buffers : first line of defence
2. Respiratory regulation :second line of defence
3. Renal regulation : third line of defence
Can not remove H+ ions from the body.
Temporarily acts as a shock absorbant to reduce the free H+ ion.
3 buffer system :
1. Bicarbonate buffer
2. Phosphate buffer
3. Protein buffer
Extracellular buffer system of the body
NaHCO3/H2CO3= [ SALT ] / [ACID]
NORMAL RATIO= 20 : 1
Base constituent (HCO3 ) - regulated by the kidney
(Metabolic component)
Acid (H2CO3) - respiratory regulation ( Respiratory component ).
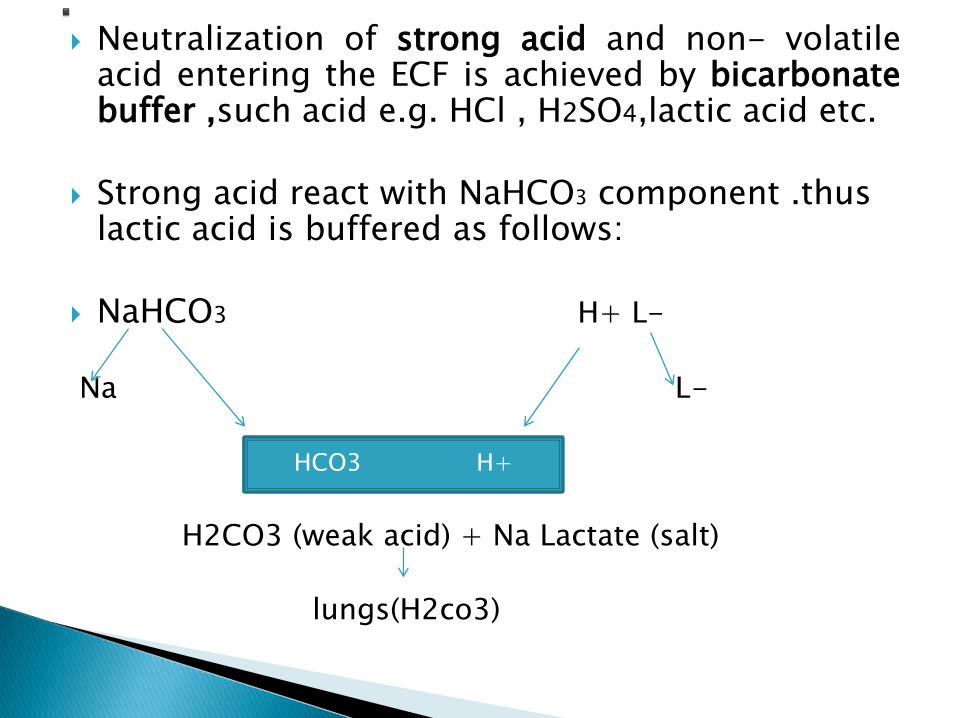
Neutralization of strong acid and non- volatileacid entering the ECF is achieved by bicarbonatebuffer ,such acid e.g. HCl , H2SO4,lactic acid etc.
Strong acid react with NaHCO3 component .thus lactic acid is buffered as follows:
NaHCO3 H+ L-
Na L-
H2CO3 (weak acid) + Na Lactate (salt)
lungs(H2co3)
HCO3 H+
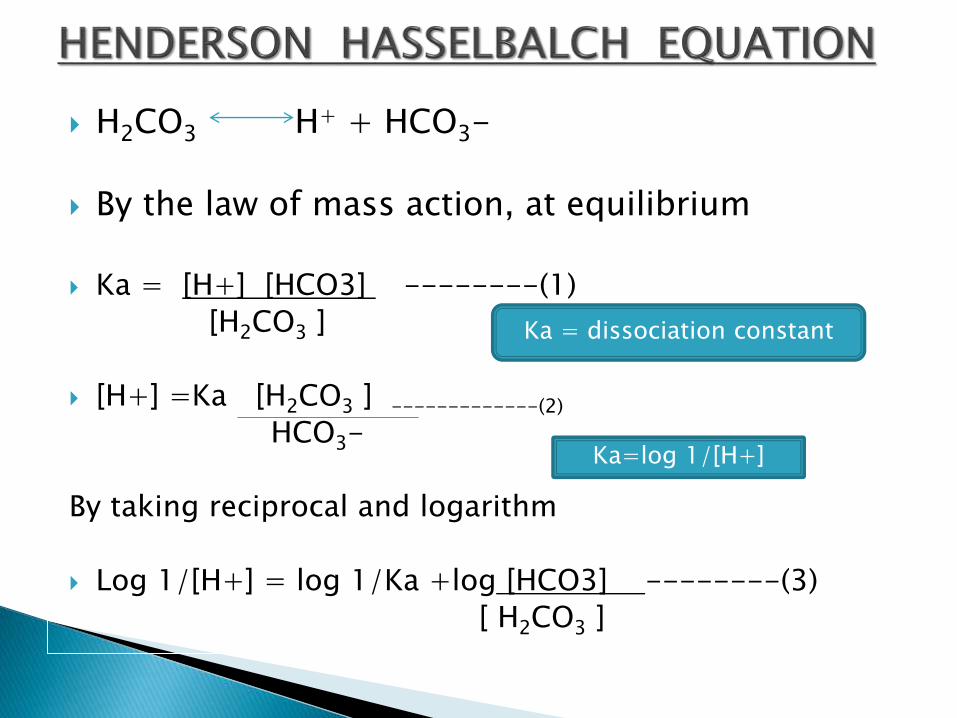
H2CO3 H+ + HCO3-
By the law of mass action, at equilibrium
Ka = [H+] [HCO3] --------(1)
[H2CO3 ]
[H+] =Ka [H2CO3 ] -------------(2)
HCO3-
By taking reciprocal and logarithm
Log 1/[H+] = log 1/Ka +log [HCO3] --------(3)
[ H2CO3 ]
Ka = dissociation constant
Ka=log 1/[H+]
pH = pka + log [ HCO3 ] -------(4)
[H2CO3 ]
USES;
1. It determines the pH of blood.
2. Serve as an index to understand thedisturbance in acid base balance of thebody.
1. High concentration
2. Alkali reserve
3. Very good physiological buffer and act asfront line of defence.
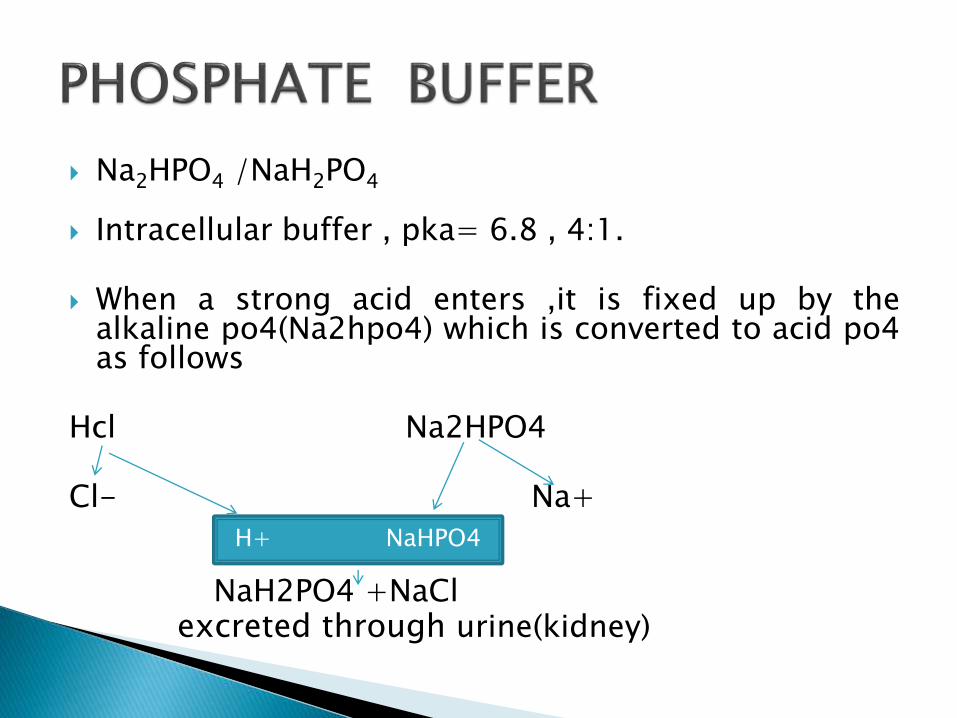
Na2HPO4 /NaH2PO4
Intracellular buffer , pka= 6.8 , 4:1.
When a strong acid enters ,it is fixed up by thealkaline po4(Na2hpo4) which is converted to acid po4as follows
Hcl Na2HPO4
Cl- Na+
NaH2PO4 +NaClexcreted through urine(kidney)
H+ NaHPO4
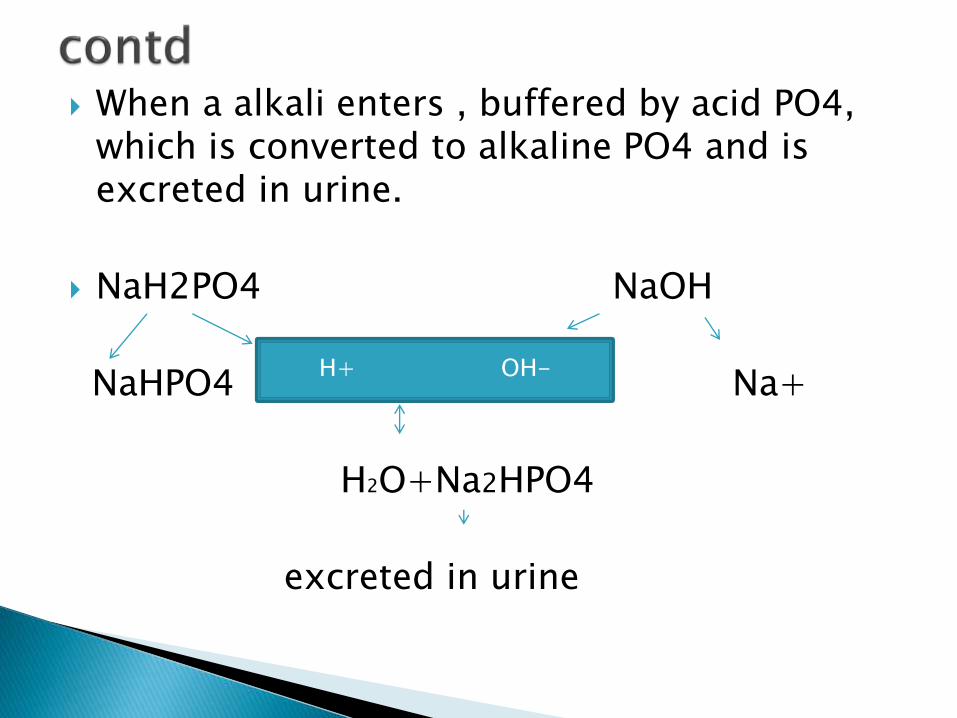
When a alkali enters , buffered by acid PO4, which is converted to alkaline PO4 and is excreted in urine.
NaH2PO4 NaOH
NaHPO4 Na+
H2O+Na2HPO4
excreted in urine
H+ OH-
Advantage
Very effective and better, as pka approaches physiological ph.
Plasma Protein and Hb - most important
Buffering action of protein depends on pk of ionizable group of amino acid
Effective group- imidazole group of Histidine
Pk - 6.7
In acidic medium, protein acts as a base, NH2
group takes up H+ ions from the mediumforming NH3+, proteins becomes positivelycharged.
in alkaline medium , protein act as an acid,
COOH group dissociates and gives H+,forming COO-. H + combines with OH- toproduce molecule of water , proteins becomenegatively charged
The respiratory system helps control theacidity of the blood by regulating theelimination of CO2 and H2O.
These molecules are exhaled with everybreath.
H2CO3 H2O + CO2
carbonic acid
The brain is sensitive to blood CO2 levels andpH.
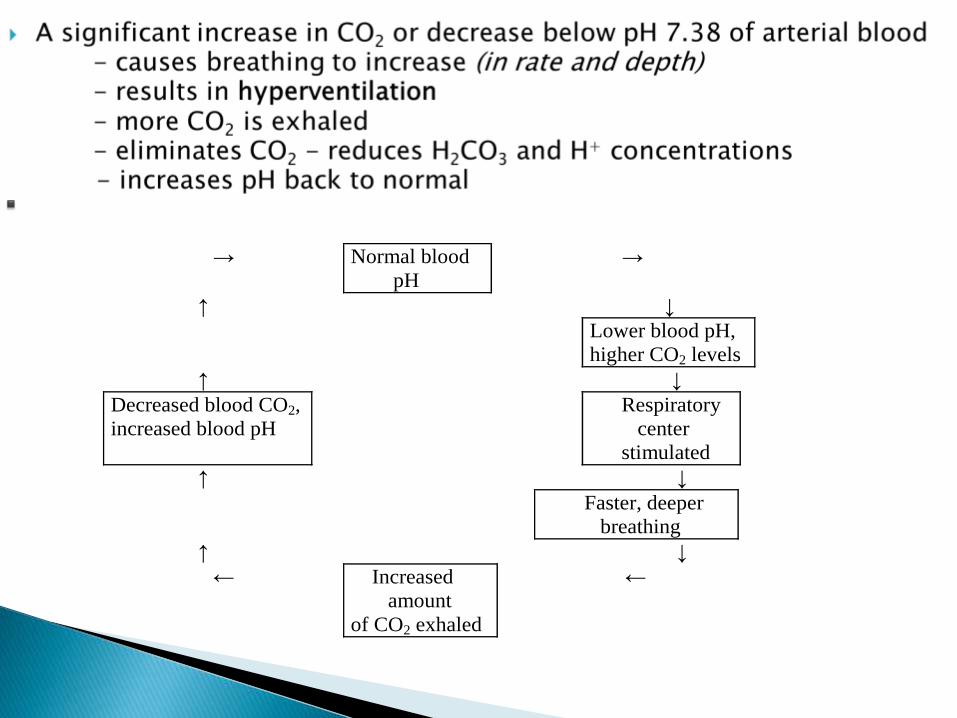
→ Normal blood
pH
→
↑ ↓
Lower blood pH,
higher CO2 levels
↑ ↓
Decreased blood CO2,
increased blood pH
Respiratory
center
stimulated
↑ ↓
Faster, deeper
breathing
↑ ↓
← Increased
amount
of CO2 exhaled
←
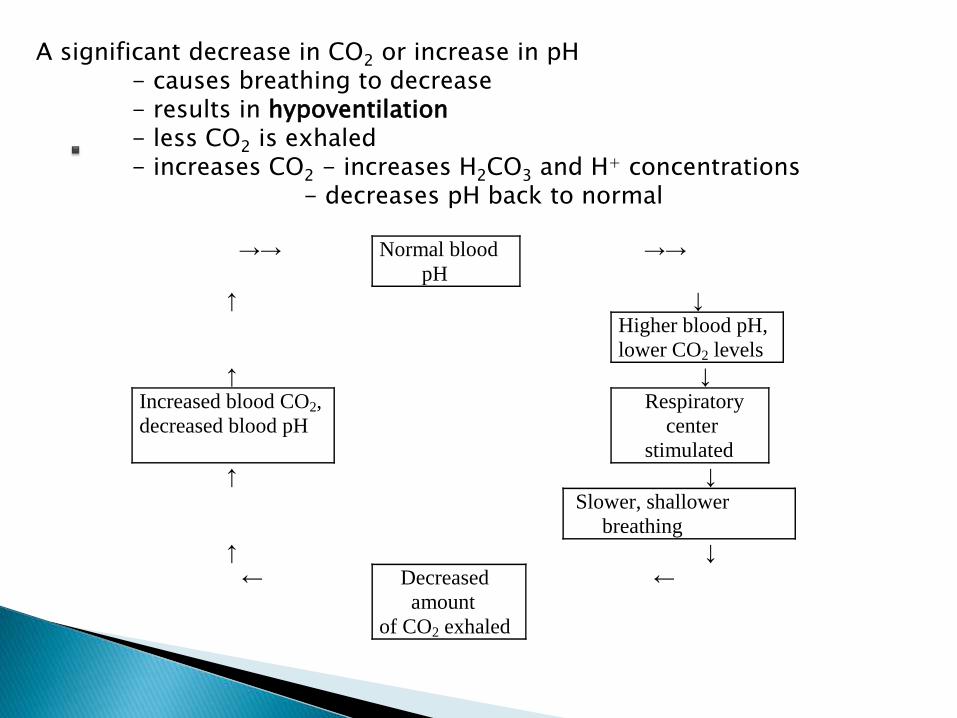
A significant decrease in CO2 or increase in pH- causes breathing to decrease- results in hypoventilation- less CO2 is exhaled- increases CO2 - increases H2CO3 and H+ concentrations
- decreases pH back to normal
→→ Normal blood
pH
→→
↑ ↓
Higher blood pH,
lower CO2 levels
↑ ↓
Increased blood CO2,
decreased blood pH
Respiratory
center
stimulated
↑ ↓
Slower, shallower
breathing
↑ ↓
← Decreased
amount
of CO2 exhaled
←
• Third line of defense against change inhydrogen ion concentration
• permanent solution to the acid basedisturbances.
• Kidneys require hours to days tocompensate for changes in body-fluid pH
1. Excretion of H+.
2. Reabsorption of bicarbonate
3. Excretion of titratable acid
4. Excretion of ammonium (NH4+)
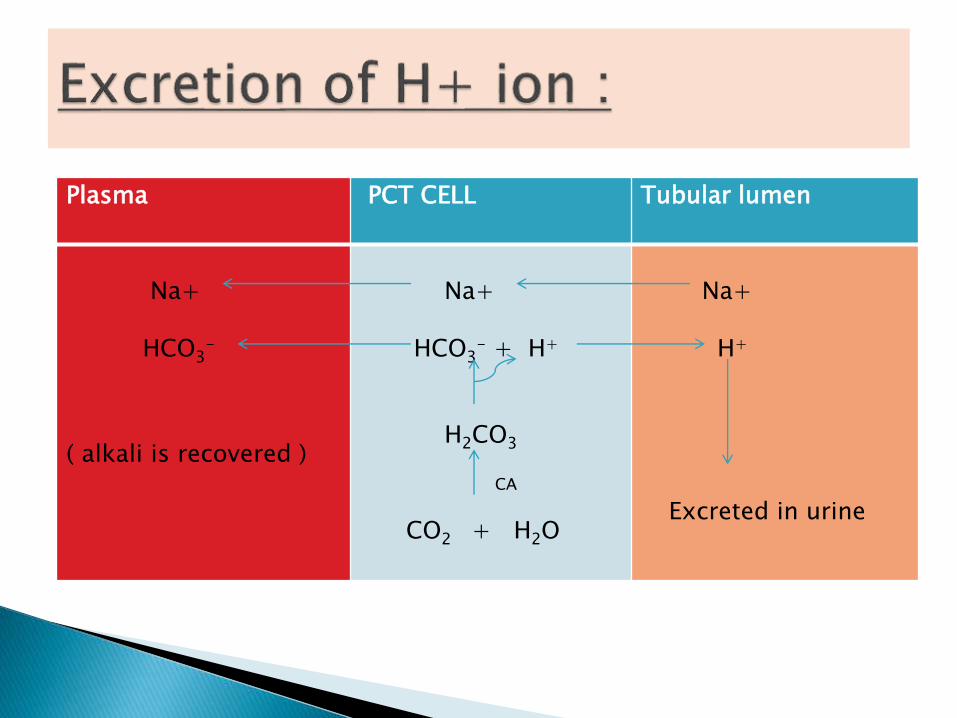
Plasma PCT CELL Tubular lumen
Na+
HCO3-
( alkali is recovered )
Na+
HCO3- + H+
H2CO3
CA
CO2 + H2O
Na+
H+
Excreted in urine
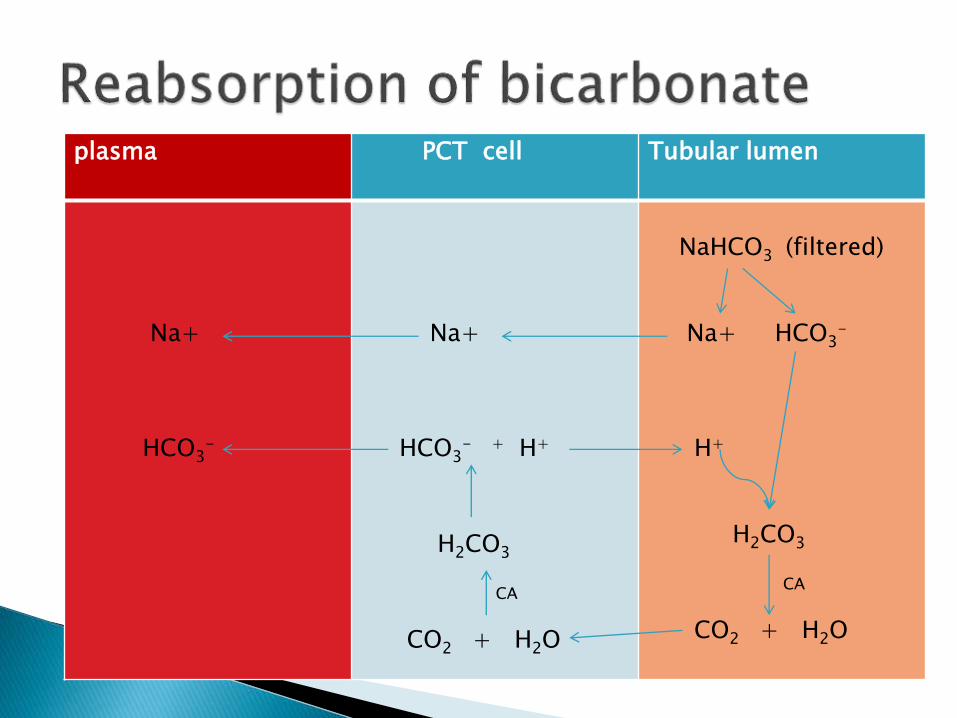
plasma PCT cell Tubular lumen
Na+
HCO3-
Na+
HCO3- + H+
H2CO3
CA
CO2 + H2O
NaHCO3 (filtered)
Na+ HCO3-
H+
H2CO3
CA
CO2 + H2O
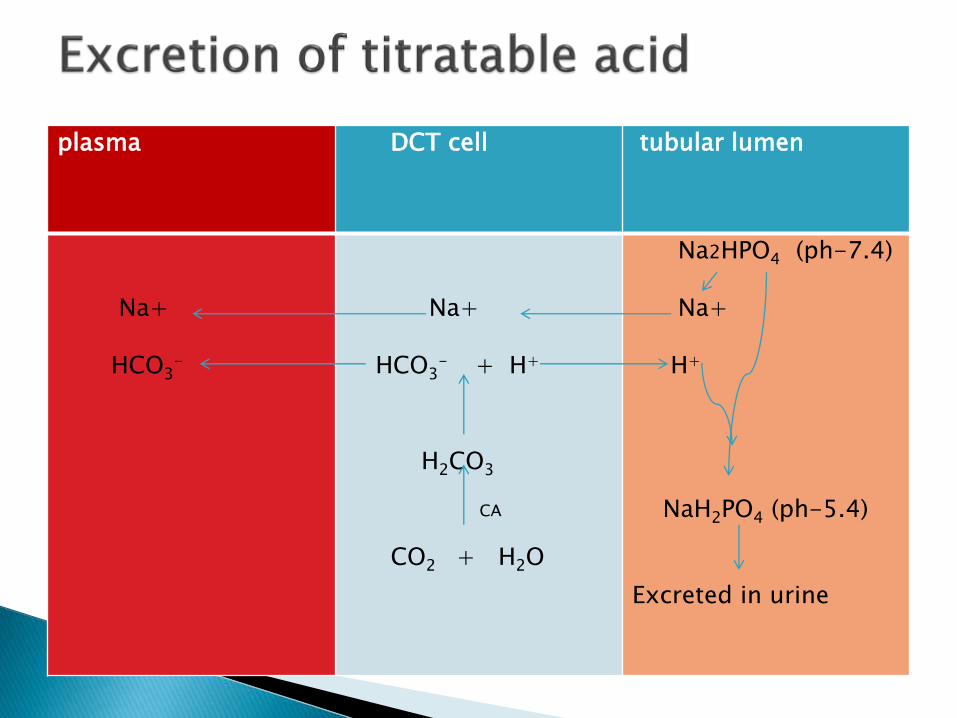
plasma DCT cell tubular lumen
Na+
HCO3-
Na+
HCO3- + H+
H2CO3
CA
CO2 + H2O
Na2HPO4 (ph-7.4)
Na+
H+
NaH2PO4 (ph-5.4)
Excreted in urine
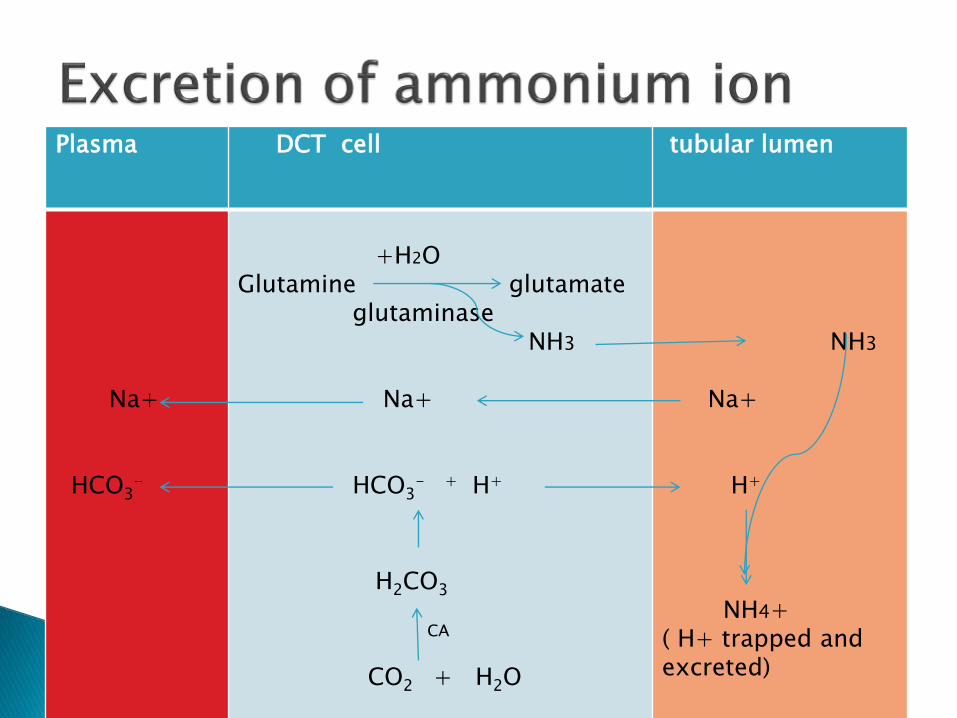
Plasma DCT cell tubular lumen
Na+
HCO3-
+H2OGlutamine glutamate
glutaminaseNH3
Na+
HCO3- + H+
H2CO3
CA
CO2 + H2O
NH3
Na+
H+
NH4+( H+ trapped and excreted)
A 50 year old man came to emergency department after returningfrom foreign travel. His symptom included persistent diarrhoea (overthe past 3 days) and rapid respiration . Blood gases were drawn withfollowing results :
pH- 7.21 ( )
pCO2 - 19 mmHg ( )
pO2 - 96 mmHg
HCO3- 7 mmol/l
Questions:
1. What is the patient acid base status?
2. Why is the HCO3 level is so low?
3. Why does the patient have rapid respiation?
ACIDOSIS: PH <7.35
a ) METABOLIC ACIDOSIS
b ) RESPIRATORY ACIDOSIS
ALKALOSIS : PH >7.45
a ) METABOLIC ALKALOSIS
b ) RESPIRATORY ALKALOSIS
The sum of cations and anions in ECF isalways equal , so as to maintain the electricalneutrality.
Commonly measured electrolytes in plasmaare Na+, K+,Cl-,HCO3- .
Unmeasured anion in the plasma constitutesthe anion gap.
This is due to presence of protein anions ,sulphate , phosphate and organic acids.
Anion gap = (Na + k) - ( HCO3+ Cl- ) .
Normally anion gap is about 15 mEq/l
Normal range = 8-18 mEq/l.
High anion gap acidosisI. Renal failureII. Diabetic ketoacidosisIII. Lactic acidosis
Normal anion gap acidosisI. DiarrhoeaII. Hyperchloremic acidosis
Low anion gapI. Multiple myeloma
Primary deficit of bicarbonate.
Due to its utilization in buffering H+ ions,loss in urine or GIT .
Important cause-excessive production oforganic acids which combine with sodiumbicarbonate and deplete alkali reserve .
NaHCO3+organic acids Na salts of o organic acids + CO2

Severe uncontrolled diabetes mellitus(ketoacidosis)- production of organic acids
Renal failure
Lactic acidosis
Severe diarrhoea
Renal tubular acidosis
Increased production and accumulation of organic acid causes an elevation in anion gap.
This type is seen in ketoacidosis
COMPENSATION• Hyperventilation of lungs(elimination of co2)
• Renal compensation-(3-4days) H+ ions excreted as NH4+
Primary excess of carbonic acid .
Causes
• Severe asthma
• Pneumonia
• Cardiac arrest
• Depression of respiratory centre
• COPD
Compensation
H2O + CO2 ↔ H2CO3 ↔ H++ HCO3-
renal mechanism-
• Increase in renal reabsorption of bicarbonate
• excretion of titrable acidity and NH4+ iselevated in urine
Primary excess of bicarbonate
Causes• Severe vomiting
• Hypokalemia
• Intravenous administration of bicarbonate.
• Cushing syndrome
M. alkalosis is commonly associated withhypokalemia .
In severe k+ deficiency ,H+ ions are retainedinside the cells to replace missing k+ ions.
In the tubular cells, H+ions are exchanged(instead of k+) with the reabsorbed Na+.
Paradoxically , the patient excretes acid urinedespite alkalosis.
COMPENSATION
H2O + CO2 ↔ H2CO3 ↔ H++ HCO3-
HYPOVENTILATION- to retain co2
Renal mechanism-
excretes more bicarbonate and retains H+
Primary deficit of carbonic acid
causes
• Hyperventilation
• High altitude
• Salicylate poisoning
Compensation
H2O + CO2 ↔ H2CO3 ↔ H++ HCO3-
Renal mechanism –
by increasing excretion of bicarbonate by decreasing reabsorption
secretion of H+ decreases
Potassium- affects contractility of heart
Hypokalaemia - life threatening
Insulin – increases K+ uptake by cells
Measurement of plasma k+ concentration
assumes significance in acid-base disorders.
Patients with severe uncontrolled DM (M.acidosis) is usually with hypokalemia.
When such a patient is given insulin , itstimulates k+ entry into cells.
The result is that plasma k+ level is furtherdepleted.
Hypokalemia affects the heart functioningand is life threatening.
Therefore in the treatment of diabetic ketoacidosis,
k+ has to be given.
K+ and alkalosis
Hypokalemia leads to increased excretion of hydrogen
ions, and thus may cause M. alkalosis.

Assessment of acid base status.
Arterial blood
Radial artery – in the Wrist
Brachial artery - in the arm
Femoral artery - in the groin

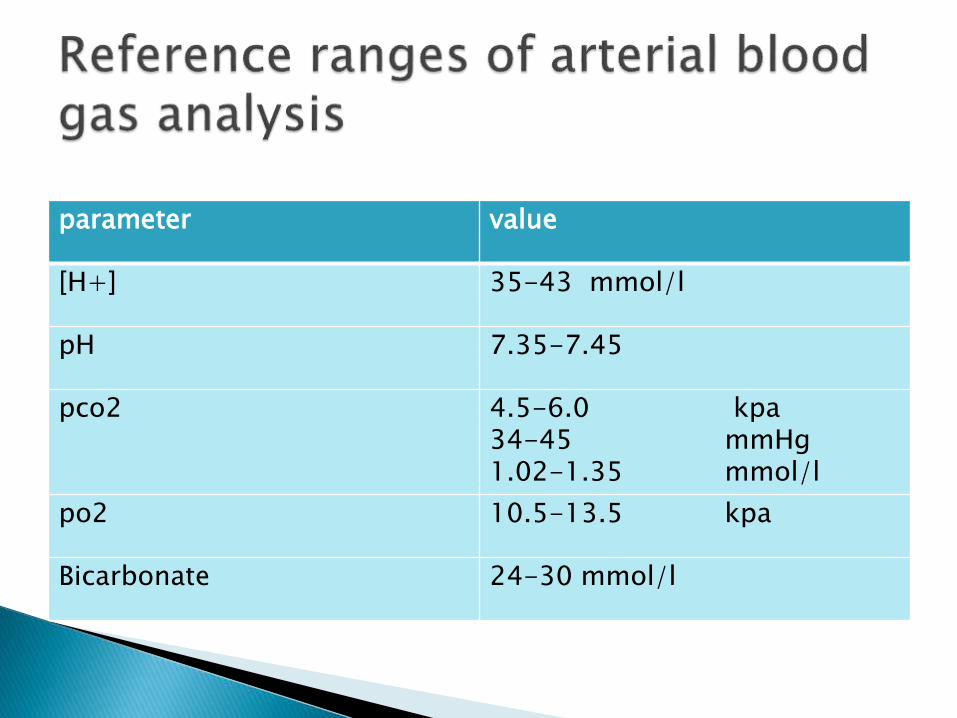
parameter value
[H+] 35-43 mmol/l
pH 7.35-7.45
pco2 4.5-6.0 kpa34-45 mmHg1.02-1.35 mmol/l
po2 10.5-13.5 kpa
Bicarbonate 24-30 mmol/l
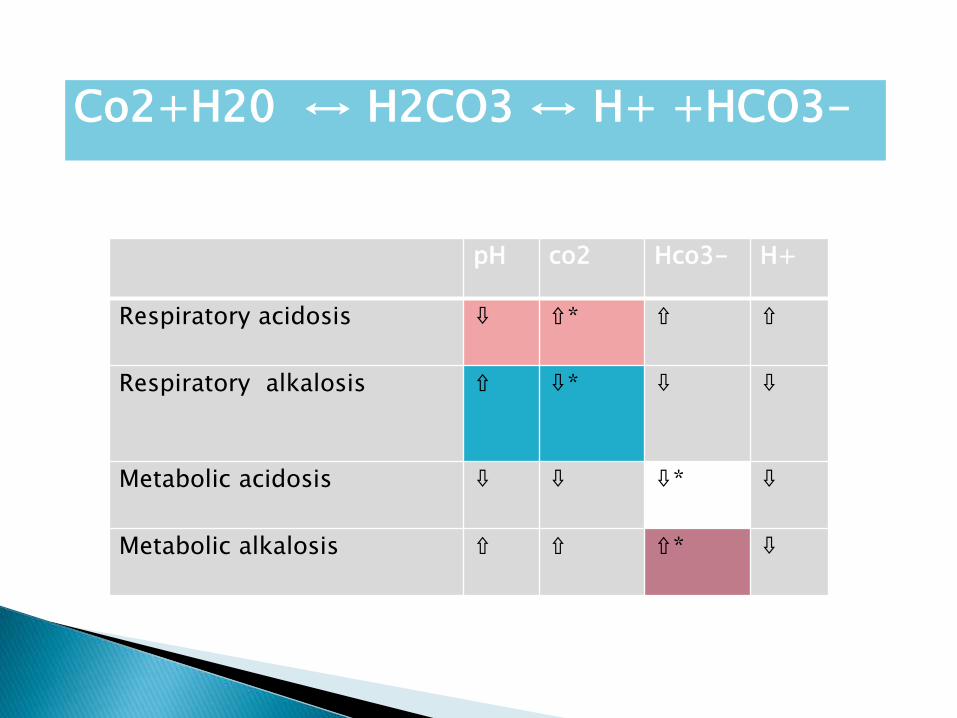
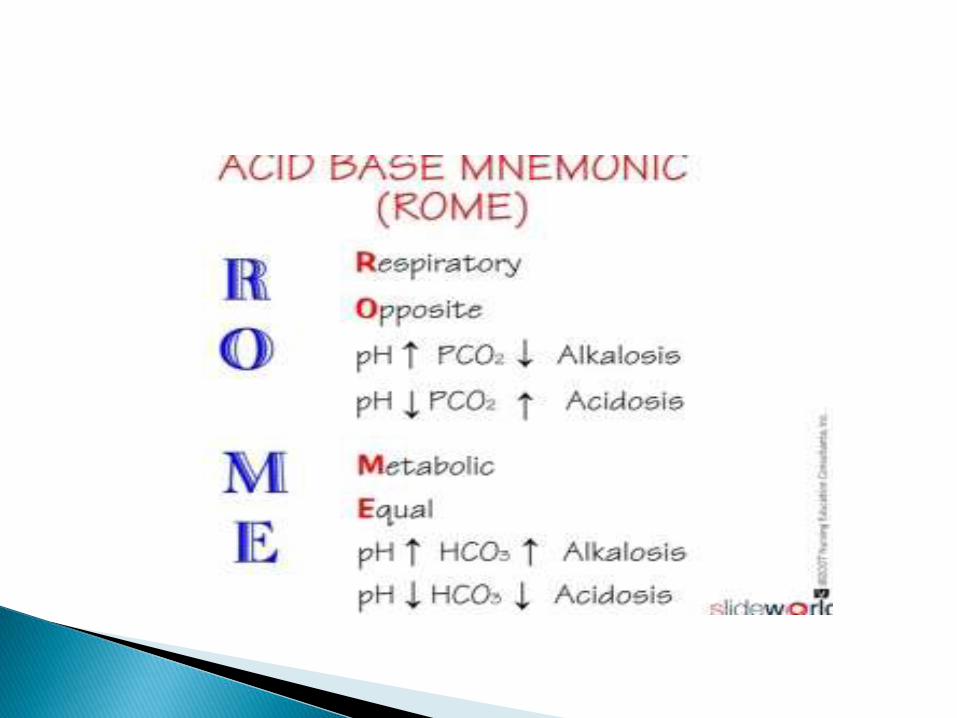
pH co2 Hco3- H+
Respiratory acidosis ⇩ ⇧* ⇧ ⇧
Respiratory alkalosis ⇧ ⇩* ⇩ ⇩
Metabolic acidosis ⇩ ⇩ ⇩* ⇩
Metabolic alkalosis ⇧ ⇧ ⇧* ⇩
Co2+H20 ↔ H2CO3 ↔ H+ +HCO3-
A) Arterial blood gas analysis
PH- 7.31 ( ↓) ,
Pco2-55 mmHg (↑) ,
HCO3-28 mmol/l (Normal)
respiratory acidosis w/o compensation.
B)ABG
Ph-7.31
Pco2-55mmhg
Hco3-35mmol/l (abnormal)
Respiratory acidosis with compensation
TIETZ TEXT BOOK OF CLINICAL CHEMISTRY
VARLEY’S CLINICAL CHEMISTRY
MICHAEL L. BISHOP, CLINICAL CHEMISRY ,SEVENTH EDITION.
DM VASUDEVAN TEXTBOOK OF BIOCHEMISTRY
U. SATYANARAYANA TEXTBOOK OF BIOCHEMISTRY
LAWERENCE A. KAPLAN A TEXT BOOK OF CLINICAL CHEMISTRY
DR. R. N. ROY A TEXT BOOK OF BIOPHYSICS