Embed Size (px)
Citation preview

Acute Leukemias
Dr. Syed Muhammad Ali Shah
RMO/PGR
Dept. of Medicine

What are leukemias???
• Leukaemias are malignant disorders of the haematopoietic stem cell compartment, characteristically associated with increased numbers of white cells in the bone marrow and/or peripheral blood.
• The course of leukaemia may vary from a few days or weeks to many years, depending on the type.

Epidemiology
• ALL, comprises 80% of the acute leukemias of childhood.
• Peak incidence is between 3 and 7 years of age.
• Appr. 20% of adult acute leukemias is ALL.
• AML - median age at presentation of 60 years


RISK FACTORS
• Environmental factors– Radiation
– Benzene
– Alkylating agents, topoisomerase II inhibitors, and other cytotoxic drugs
– Tobacco smoke
• Acquired diseases– Clonal myeloid diseases
– Chronic myelogenousleukemia
– Primary myelofibrosis
– Essential thrombocythemia
– Polycythemia vera
– Myeloma
• Other disorders– Human immunodeficiency virus
infection
– Thyroid disorders
– Polyendocrine disorders
• Inherited or Congenital Conditions

Signs and Symptoms
GENERAL
• Due to anemia pallor, fatigue, weakness, palpitations, and dyspnea on exertion.
• Weakness, loss of sense of well-being, and fatigue on exertion can be disproportionate to the severity of anemia.
• Easy bruising, petechiae, epistaxis, gingival bleeding, conjunctival hemorrhages, and prolonged bleeding from skin injuries reflect thrombocytopenia.

• Pustules or other minor pyogenic infections of the skin and of minor cuts or wounds are most common.
• The most common pathogens are gram-negative bacteria (Escherichia coli, Klebsiella, Pseudomonas) or fungi (Candida, Aspergillus)
• Major infections, such as sinusitis, pneumonia, pyelonephritis, and meningitis, are uncommon at presentation

• Anorexia and weight loss are frequent findings.
• Fever is present in many patients at the time of diagnosis.
• Palpable splenomegaly or hepatomegalyoccurs in approximately one-third of patients.
• Lymphadenopathy is extremely uncommon except in the monocytic variant of AML.

Systemic Involvement
• Skin involvement may be of three types: – nonspecific lesions– leukemia cutis– granulocytic (myeloid) sarcoma of skin and subcutis
• Sensory organ involvement is very unusual, but retinal, choroidal, iridial, and optic nerve infiltration can occur
• Oral manifestations– Gingival or periodontal infiltration– Dental abscesses may lead to an extraction– Prolonged bleeding of an infected tooth socket

• The respiratory tract can be involved by:– Infiltrates or tumors leading to laryngeal obstruction– Parenchymal infiltrates– Alveolar septal infiltration– Pleural seeding.
• Central or peripheral nervous system - meningealinvolvement is an important consideration in the treatment of the monocytic type of AML.
• Osteoarticular symptoms– Bone pain– Joint pain– Bone necrosis – Crystal-induced arthritis
• Calcium pyrophosphate dihydrate (pseudogout)• Monosodium urate (gout)

LABORATORY FEATURES
BLOOD PICTURE:
• The hallmark of acute leukemia is the combination of pancytopenia with circulating blasts.
• Anemia is a constant feature - inadequate production of red cells
• Thrombocytopenia is nearly always present -inadequate production and decreased survival of platelets.
• The TLC is < 5000/ L (5 x 109 /L) & absolute neutrophilcount is < 1000/ L (1 x 109 /L) in approximately half of patients at the time of diagnosis.

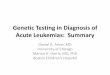
Blood film of AML without maturation (acute myeloblastic leukemia). Five myeloblasts are evident. High nuclear-to-cytoplasmic ratio. Agranularcells.

ALL with large blasts showing prominent nucleoli, moderate amounts of cytoplasm, and an admixture of smaller blasts

Typical lymphoblasts with scanty cytoplasm, regular nuclear shape, fine chromatin, and indistinct nucleoli

Bone Marrow Findings
• The marrow always contains leukemic blast cells
• The bone marrow is usually hypercellular and dominated by blasts.
• More than 20% marrow blasts are required to make a diagnosis of acute leukemia.

• Hyperuricemia
• If DIC is present– the fibrinogen level will be reduced
– the prothrombin time prolonged
– fibrin degradation products or fibrin D-dimerspresent.
• Patients with ALL (especially T cell) may have a mediastinal mass visible on chest radiograph.
• Meningeal leukemia will have blasts present in the spinal fluid, seen in approximately 5% of cases in monocytic types of AML and can be seen with ALL.


• The phenotype of leukemia cells is usually demonstrated by flow cytometry or immunohistochemistry.
• AML cells usually express myeloid antigens such as CD 13 or CD 33 and myeloperoxidase.
• ALL cells of B lineage will express CD19, common to all B cells, and most cases will express CD10, formerly known as the “common ALL antigen.”
• ALL cells of T lineage will usually not express mature T-cell markers, such as CD 3, 4, or 8, but will express some combination of CD 2, 5, and 7 and do not express surface immunoglobulin.
• Almost all ALL cells express terminal deoxynucleotidyl transferase (TdT).


Management
Supportive therapy• Anaemia - red cell concentrate transfusions.• Bleeding
– Thrombocytopenic bleeding requires platelet transfusions, unless the bleeding is trivial.
– Prophylactic platelet transfusion should be given to maintain the platelet count above 10 × 109/L. Coagulation abnormalities
• Infection – Fever (> 38°C) lasting over 1 hour in a neutropenic
patient indicates possible septicaemia

• Empirical therapy - combination of an aminoglycoside (e.g. gentamicin) and a broad-spectrum penicillin (e.g. piperacillin/tazobactam) or a single-agent beta-lactam (e.g. meropenem)
• The organisms most commonly associated with severe neutropenic sepsis are:– Gram-positive bacteria
• Staphylococcus aureus
• Staph. epidermidis,
– Gram-negative bacteria• Escherichia coli
• Pseudomonas
• Klebsiella spp.

• Gram-positive infection may require vancomycin therapy.
• If fever has not resolved after 3–5 days, empirical antifungal therapy (e.g. a liposomal amphotericin B preparation, voriconazole or caspofungin) is added.
• Oral and pharyngeal candida infection –fluconazole, itraconazole
• Reactivation of herpes simplex infection
• Herpes zoster– Chickenpox
– Shingles

• Metabolic problems– Frequent monitoring of fluid balance and renal,
hepatic and haemostatic function is necessary.
– Renal toxicity occurs with some antibiotics (e.g. aminoglycosides) and antifungal agents (amphotericin).
– Cellular breakdown during induction therapy (tumourlysis syndrome)• Hyperkalaemia
• Hyperuricaemia,
• Hyperphosphataemia
• Hypocalcaemia.
– Allopurinol and intravenous hydration are given to try to prevent this

Specific Treatment
• Remission induction – In this phase, the bulk of the tumour is destroyed by
combination chemotherapy.– The patient goes through a period of severe bone marrow
hypoplasia
• Remission consolidation– If remission has been achieved, residual disease is attacked by
therapy during the consolidation phase. – This consists of a number of courses of chemotherapy, again
resulting in periods of marrow hypoplasia.
• Remission maintenance– If the patient is still in remission after the consolidation phase
for ALL, a period of maintenance therapy is given, with the individual as an outpatient and treatment consisting of a repeating cycle of drug administration.


Haematopoietic Stem Cell Transplantation
• Transplantation of haematopoietic stem cells (HSCT) has offered the only hope of ‘cure’ in a variety of haematological and non-haematological disorders
• The type of HSCT is defined according to the donor and source of stem cells into:
– Allogenic HSCT
– Autologus HSCT

• In allogeneic HSCT, the stem cells come from a donor either related (usually an HLA-identical sibling) or a closely HLA-matched volunteer unrelated donor (VUD).
• In an autologous transplant, the stem cells are harvested from the patient and stored in the vapour phase of liquid nitrogen until required.

![The Effect of Chromosomal Translocations in Acute ... · [CANCER RESEARCH (SUPPL.) 59, 1794s-1798s, April 1, 1999] The Effect of Chromosomal Translocations in Acute Leukemias: The](https://img.pdfslide.net/doc/110x75/5e6958cecc3d9a570329abd8/the-effect-of-chromosomal-translocations-in-acute-cancer-research-suppl.jpg)


![New Application · Web viewLeukemias, to include acute lymphoblastic leukemia, acute and chronic myeloid leukemias, and myelodysplastic syndromes [PR IV.B.1.b).(1).(h).(x)] Hodgkin’s](https://img.pdfslide.net/doc/110x75/5f05bca47e708231d4147300/new-application-web-view-leukemias-to-include-acute-lymphoblastic-leukemia-acute.jpg)