Embed Size (px)
DESCRIPTION
Citation preview

RIGID ENDOSCOPIC EVALUATION OF CONVENTIONAL CURETTAGE ADENOIDECTOMY
D REGMI, N N MATHUR, M BHATTARAI Dept.of otolaryngology & head and neck surgery.B P Koirala Institute of Health Sciences, Dharan, Nepal. Introduction By: Dr.Roohia Disscussion By: Dr. Krishna Sumanth

INTRODUCTION Adenoidectomy is a most common
surgical procedure perfomed in childrens.
Conventional curettage commonly used technique in adenoidectomy.

Adenoids is primarily a disease of young
children occurs mainly between the ages of 3 and 5 years.
1994 140,000 U.S. children under the age of 15 had adenoidectomies and 286,000 had adenotonsillectomies
This is down from a peak of over 1 million in the 1970’s

HISTORY1867 Wilhelm Meyer reports removal of “adenoid
vegetations” through the nose with a ring knife. In 1885, Gottstein described the first adenoid
curettePearl & Manoukian had reportedly removed
adenoids viewing it indirectly with a laryngeal mirror. Canon popularized the use of rigid endoscopy in
visualising and removal of adenoid remanants after blind currett.
Wan et al have introduced the transoral adenoidectomy under endoscopic guidance.
In 1992, Becker et al, reported the use of endoscopy assisted adenoidectomy.

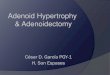
NASOPHARYNGEAL TONSIL
Adenoids is the hypertrophied mass of lymphoid tissue situated at the junction of roof & post. wall of nasopharynx.
The mass of lymphoid tissue is termed as Adenoids only when it is hypertrophied.

Adenoids
The adenoid develops as a midline structure by fusion of 2 lateral primordia.
Adenoids begin forming in 3rd month of fetal development.
Fully formed by 7 month of gestation. Continue to grow up to 5yrs of life.
It usually undergoes atrophy by puberty (13-14 yrs)
Covered by pseudostratified ciliated epithelium.

Adenoids is a nasopharyngeal lymphoid tissue is a part of the Waldeyer’s ring which includes:
Palatine tonsil. Adenoids. Lingual tonsils.Tubal tonsils. Lateral
pharyngeal bands

Extend to the fossa of Rosenmuller and to the eustachian tube orifice as Gerlach’s tonsil.
truncated pyramid. Base- at junc of roof &
post. Wall of nasopharynx.
Apex- towards septum No crypts & capsule. Vertical folds extends
forwars & laterally from midian blind recess(pharyngeal bursa/bursa of luschka)

BLOOD SUPPLY 1. Ascending pharyngeal artery 2. Ascending palatine artery 3. Pharyngeal branch of internal
maxillary artery 4. Artery of pterygoid canal 5. Contributions from tonsillar branch
of facial artery 6. basishpenoid artery Venous drainage from the adenoid
is through the pharyngeal plexus which in turn drain into the internal jugular vein.
Nerve supply: pharyngeal plexus. Lymphatics: in to retropharyngeal
&pharyngo maxillary space L.nodes. Upper deep jugular nodes, Parapharyngeal nodes. there are no afferents.

Immunology
Exposed to ingested or inspired antigens passed through the epithelial layer
Immunologic structure is divided into 4 compartments: reticular crypt epithelium, extra follicular area, mantle zone of the lymphoid follicle, and the germinal center of the lymphoid follicle

Membrane cells and antigen presenting cells are involved in transport of antigen from the surface to the lymphoid follicle
Antigen is presented to T-helper cells
T-helper cells induce B cells in germinal center to produce antibody
Secretory IgA is primary antibody produced
Involved in local immunity


pathophysiology adenoids can contribute to recurrent sinusitis and chronic
persistent or recurrent ear disease because they can harbor a chronic infection.
Recurrent or persistent middle ear effusion Infants have a natural lack of immune function and poorer
eustachian tube function. Bacteria-irritation of the eustachian tube lining, resulting in
dysfunction,/chronic low-grade infection in the middle ear space.
Chronic sinusitis adenoid appears to act as a reservoir of infection. same pathogenic bacteria in the adenoids were cultured from
the middle meatus near the anterior sinus drainage site
Nasal airway obstruction physically blocking the back of the nose. add to sinusitis itself
by blocking normal nasal flow posteriorly,

Predisposing factors:A) General:1) Environmental pollution.2) Allergy.3) Bad Hygiene4) Poor general health
B) Local:1) Recurrent upper respiratory
infections.2) Chronic tonsillitis.

Clinical pictureA) Nasal obstruction,1) Mouth breathing.2) Snoring.3) Difficulty of suckling and
eating.4) Nasal tone of the voice

B) Adenoid facies: Flat expressionless
face due to absence of the nasolabial folds.
Open mouth and dry lips.
Hitched up upper lip, projecting incisors, dry gums, pyorrhea, and dental caries.
Inactive ala nasi. Receding chin. High arched palate .

C) Mucopurulent anterior and posterior nasal discharge. D) Sleep disturbances:1) Snoring.2) Sleep apnea .3) Nocturnal enuresis due to hypercapnia.

E) Respiratory manifestations:1) Irritant cough2) Recurrent pharyngitis, laryngitis, and chest infections. F) Recurrent ear aches and deafness due toobstruction of the eustachian tubes causing recurrentotitis media and middle ear effusions G) Symptoms of throat : due to recurrent pharyngitis,tonsillitis, mouth breathing recurrent sore throat,dysphagia,voice change,poor eaters, ,malnutrition..

H) Decreased mental performance due tosleep disturbances, hypoxia, defective hearing, andrecurrent respiratory infections causing long periods of absences from school. I) Feeding problems: loss of appetite, indigestion,and vomiting due to swallowed secretions.J) Skeletal changes :including pigeon chest,Harrison’s sulci, and depressed xiphisternum.

DiagnosisClinical picture.Investigations may
be done: Posterior
rhinoscopy Digital palpation Endoscopic exam Lateral x-ray of the
Nasopharynx.CT MRI

ENDOSCOPY
RIGID ENDOSCOPY
FLEXIBLE ENDOSCOPY

Types of rigid endoscopesAdults: 4mm
Children: 2.7mm
Viewing angles: 0 degree,30,45,70,90,120
Length: 10 cm,17 cm,24 cm


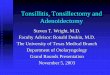
Grading Clemens &mcmurray GRADE I- adenoid tissue filling
1/3rd the vertical ht of choana
GRADE II-upto 2/3rd GRADE III- from 2/3rd to nearly all
but not completely filling of choana
GRADE IV-with complete choanal obstruction

Modified josephson et al Airway , Choana, Eustachian tube A0- no adenoids C0- no obstruction A1-25% airway block C1-50%A2-26-50% C2-100%A3-51-75% A4-75-100% E0-no ET block E1-ET block

Differential diagnosis Choanal atresia Chr.hypertrophic rhinitis,septal
deviation,nasal polyposis Juvenile angiofibroma Thornwald’s cyst,malignant
lymphoma,chordoma,lyphoepithelial carcinoma

Complications1. Middle ear effusions and otitis
media.2. Recurrent respiratory infections.3. Disturbed learning, easy fatigue, and genaral poor health 4.older children; increased ventilatory
resistance leads to moderate cardiac enlargement RVH to Corpulmonale pulm.oedema &pco2

MANAGEMENTMedical: for mild/infrequent symp Adequate nutrition, Antibiotics, Anti inflammatory analgesics,Nasal decongestant drops,steroid sprays like mometasone.These children must undergo a complete
course of medical treatment. (2wks)The ideal drug of choice is penicllin group. Ampicillin or Amoxycillin can
be administered in doses ranging 40 - 50 mg /kg body weight.
Erythromycin & cefalosporins can be used.

Surgical Adenoidectomy Current clinical indicators from
AAO-HNS:◦ 4 or more episodes of recurrent purulent
rhinorrhea in prior 12 months in a child <12. One episode documented by intranasal examination or diagnostic imaging.
◦ Persisting symptoms of adenoiditis after 2 courses of antibiotic therapy. One course of antibiotics should be with a beta-lactamase stable antibiotic for at least 2 weeks.
◦ Sleep disturbance with nasal airway obstruction persisting for at least 3 months

◦ Hyponasal or hypernasal speech◦ Otitis media with effusion >3 months or
second set of tubes◦ Dental malocclusion or orofacial growth
disturbance documented by orthodontist◦ Cardiopulmonary complications including
cor pulmonale, pulmonary hypertension, right ventricular hypertrophy associated with upper airway obstruction
◦ Otitis media with effusion over age 4

Contraindications: Age <3yrs. Bleeding disorders. Acute infections. Epidemics of polio. Cleft palate, short palate Velopharyngeal insufficiency.

Types of adenoidectomy Conventional curettage:

Nasal endoscopic adenoidectomy

Oral endoscopic adenoidectomy

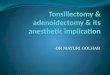
Micro debrider Micro debrider Micro debrider-
tip blade

Microdebrider adenoidectomy

Mirror asissted microdebrider adenoidectomy

Coblation adenoidectomy


The Nd: YAG laser :has additionally been accustomed to take away the adenoids. However, this method is responsible for scarring of tissue and it is generally avoided.
Adenoid punch device: An adenoid punch is really a curved device having a chamber that's placed within the adenoids. The chamber includes a knife blade sliding-door to section from the adenoids which are then housed within the chamber and removed using the instrument.

BOVIE SUCTION COAGULATOR

POST OP CARE1. Immediate general care (a) Keep the patient in coma position until fully
recovered from anaesthesia.(b) Keep a watch on bleeding from the nose and
mouth.(c) Keep check on vital signs, e.g. pulse,
respiration and blood pressure.
2. Diet When patient is fully recovered he is to take
liquids, e.g. cold milk or ice cream. 3. Nasal saline drops

4. Analgesics Pain, locally in the throat and referred
to ear, can be relieved by analgesics like paracetamol. There is no dysphagia and patient is up and about early.
5. Antibiotics A suitable antibiotic can be giv en orally or by injection for a week.
Patient is usually sent home 24 hours after operation unless there is some complication. Patient can resume his normal duties within 2 weeks

POST OP COMPLICATIONS 1. Haemorrhage, usually seen in immediate post-
operative period. 2. Injury to eustachian tube opening. 3. Injury to pharyngeal musculature and vertebrae.
Care should be taken when operating patients of Down's syndrome as 10-20% of them have atlanto-axial instability.
4. Griesel syndrome. Patient complains of neck pain and develops torticollis. Mostly it is due to spasm of paraspinal muscles, but can be due to atlanto-axial dislocation requiring cervical collar and even traction.
5. Velopharyngeal insufficiency. 6. Nasopharyngeal stenosis due to scarring. 7. Recurrence. This is due to regrowth of adenoid tissue
left behind

THANK YOU