Embed Size (px)
DESCRIPTION
Citation preview

Caring in Devon

Caring in Devon
Who’s who?

Caring in Devon
0 5 10
Where are you?

Caring in Devon

Caring in Devon
Aims
• To raise your awareness and understanding of advance care planning (ACP) and to promote its PRINCIPLES as part of the solution to improving end of life care. This will include elements of advance decisions (ADRT), LPA’s, PPC’s, conversations
• To consider how to apply ACP to your workplace and the skills and competencies required to do so.
• To refer you to further tools, documents and resources about ACP that can assist you
• To look after you while you are here...

Caring in Devon

Caring in Devon
3 key messages about advance care planning
1. It’s not new, its out there….be ready and open and a little cautious too
2. You are not on your own
3. It is rarely a one off event- but a series of conversations held over time

Caring in Devon
Advance care planning

Caring in Devon
Continuing the conversation......
Mental Capacity Act

Caring in Devon

Caring in Devon
Why Advanced Care Planning?(ACP)
• Around half a million people die each year.• 2/3rds are over 75yrs & die from chronic
illnesses such as heart disease, cancer, CVA, COPD, neurological disease & dementia.
• 58% of deaths occur in Hospital, 18% at home, 17% in Care homes, 4% Hospices, 3% elsewhere. (DoH, 2008)

Caring in Devon
Why Now?
• End of Life Care Strategy
Alice Pyne
• Drive to reduce acute hospital admissionsHealth policy over last 10 years moving towards reducing hospital deaths (DoH, 2007, 2008).

Caring in Devon
Why Now?
• Public surveys demonstrate most people wish to die at home (DoH, 2000).
• Many receive good care & their preferences & wishes at End of Life (EoL) are met.
However, many do not & do not die where they would choose.
• SW SHA funding for education in ACP- Hospiscare commissioned by NHS Devon to roll out 2010/2011

Caring in Devon
Why bother? Where is the evidence?• Evidence to support that pre planning and using
ACP is of benefit to most patients and families.• Used extensively across the world.• Can enable better service provision related to
patient need• May increase realistic hope and resilience• Improve patient and carer satisfaction with care
(greater control, empowerment and confidence in care giving)
• May reduce anxiety, depression and post traumatic stress in surviving relatives

Caring in Devon
ACP both an elephant and Bambi?

Caring in Devon
ACP is like a road map with a journey planned.
Remember: the map is not always the territory!

Caring in Devon
How are you doing so far?
How are you doing so far?

Caring in Devon
Advance Care Planning
“ Caring for people at the end of their lives is an important role for many health and social care professionals. One of the key aspects of this role is to discuss with individuals their preferences regarding the type of care they receive and where they wish to be cared for”
(Mike Richards 2007)

Caring in Devon
What is Advanced Care Planning?
• ACP is a voluntary process to which the patient must agree to and to sharing the information.
• It is a discussion about future care between an individual and their care providers(irrespective of discipline).
• The discussion is to make clear an individual’s wishes and will usually take place in the context of an anticipated deterioration in the future.

Caring in Devon
What is ACP?
It may include or clarify: 1.Their understanding of their illness and
prognosis, treatment options and availability of these.
2. Their wishes, values, beliefs and preferences or goals for care.
3.Any concerns they may have.4.Goals of care when a person has lost
capacity.5. Family and friends if person so wishes.

Caring in Devon
What is ACP?
• Conversations and requests should be clearly documented and then...
• Communicated to others in the care team including Out of hours teams.
• Be reviewed regularly and if the patient should change their mind in between reviews.
• ACP usually involves more than one team/discipline.
• Preferred Priorities for care (PPC) is the documentation used to record advanced care plans.

Caring in Devon
Preferred Priorities of Care (PPC)
• What is this document?• What is its purpose?• Who completes it?• What is done with it?• What if, after completing the PPC, the
person becomes unable to make decisions?• Is this document used to refuse treatment?

Caring in Devon
“Contrary to concerns by GP’s about patients becoming distressed or rejecting the conversation, the study found 90% choose to continue the conversation when initiated by their GP. Patients who talked about their preferences with their GP were more likely to be placed appropriately on the EoL register, and have their preferred place of death & core preferences added to their medical records.”
NCPC Project (2010) - ”dying to talk to your GP?”

Caring in Devon
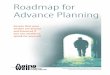
Identification of EoL patients that may benefit- the when do we start?
• Many with chronic illness(s) reach a point where it is evident they are going to die from their condition.
• Other conditions can be difficult to accurately predict.
• Gold Standards Framework Prognostic indicators (GSF 2008) provides guidance.

Caring in Devon
High
Low
Func
tion
Time
Cancer
High
Low
Func
tion
Time
Fraility/Dementia
High
Low
Func
tion
Time
Organ Failure
GP’s Workload
Ave 20 Deaths per GP per year
Taken from GSF Prognostic Indicator guide 2008

Caring in Devon

Caring in Devon
The ‘triggers’
• The surprise question: would you be surprised if this individual were to die within 6 – 12months? - ‘gut instinct’
• Clinical Indicators of Advancing Disease , i.e. Reduced physical performance, frequent admissions to hospital/out of hours services.
• An individual opts for comfort measures /opts out of curative treatment

Caring in Devon
Triggers to consider
• Referral to Specialist Palliative Care team. • Following diagnosis of a life limiting
condition ie. MND, advanced cancer, dementia.
• At instigation of DS1500 for AA/DLA.• At an assessment of an individuals needs,
complex care package, carer distress, respite care.
• Admission to a care home.

Caring in Devon
Starting a conversation
What might you say?

Caring in Devon
Initiating Discussions
• Timing & setting need to be right, privacy. • Non-verbal Communication, eye contact,
attentive listening.• An open style of dialogue..
How do you feel things are with you?How do you see things going from here? Can you tell me how you would like to be best supported if
you do not recover?/get less well?Have you thoughts/feelings about becoming less well?Are there things that would concern you should this happen?Go wish

Caring in Devon
Addressing Family & Friends
• How do you think he/she is compared to last time I came/last week?
• I feel he is less well and it concerns me....• Are there things you would like to discuss?• Respond to cues/not to outside pressures;
Listening is important.• Summarise back the main points; check
your understanding.

Caring in Devon
To Summarise
• Predicting prognosis is difficult – ‘gut instinct’ is important!
• Take the lead from the individual but may need to initiate; listen for the cues.
• Has to be a voluntary process. • Check your understanding; Reflect back.• Conclude and document; may change
their mind later….REVIEW

Caring in Devon
Advanced Decision to Refuse Treatment (ADRT)

Caring in Devon
Core Competencies for ACP

Caring in Devon
Mental Capacity Act - 2005
• Empowerment for adults who lack capacity
• Protection for adults who lack capacity and those who care for them
• Choice - by allowing people to appoint those they trust to make decisions for them
• Clarification of the law in relation to advance decisions to refuse treatments

Caring in Devon
Four tests
• Can they understand the information?
• Can they retain and believe the information? (only needs to be for long enough to allow them to use and weigh up the information)
• Can they use and weigh up the information? (i.e. can they consider benefits and
burdens?)
• Can they communicate their decision by whatever means?

Caring in Devon
Points to remember
• Capacity is Decision Specific• You must presume capacity unless
evidence exists otherwise• People should be supported to make their
decisions• Anything done for or on behalf of a person
who lacks capacity should be the least restrictive of their basic rights and freedoms
• People are allowed to make “unwise or eccentric decisions”

Caring in Devon
•Court appointed Deputies•Independent Mental Capacity Advocates

Caring in Devon
Advance Decision to Refuse Treatment(ADRT)• Made when a person over 18 has capacity.• Will come into effect only when the individual has
lost capacity to give or refuse consent.• A decision relating to a specific treatment in
specific circumstances.• If it includes refusal for life sustaining treatments
they must be in writing, be signed and witnessed and state clearly that “ the decision applies even if my life is a t risk”

Caring in Devon
ADRT
• Advance decisions that meet all the requirements of the MCA are legally binding (guidance available in code of practice for MCA)
• To be binding it must be both Valid and applicable.
• If binding, the person has taken responsibility for the decision
• If not binding, must still be considered when assessing best interests.

Caring in Devon
Useless ADRT
“If I go completely dotty just let me go and stop feeding me”
• Feeding is basic care which cannot be refused by an ADRT
• Too vague• Still worth taking into account when
planning a person’s treatment in their ‘best interest’

Caring in Devon
Valid ADRT
• I now have MND and benefit from PEG feeding. As my condition deteriorates, if I should lose consciousness and am not expected to recover after 24hrs, I wish feeding, hydration and any other life prolonging treatment such as antibiotics to be withdrawn or withheld although medication such as painkillers for my immediate comfort can be used. This decision to apply even if my life is at risk”

Caring in Devon
Valid ADRTs
I wish to refuse the following specific treatments:-
In these circumstances:-
Artificial (mechanical) breathing machine
If I have had a severe stroke with little chance of recovering consciousness
Antibiotics If my dementia means that I cannot not make the decision, in the event that I have a severe chest infection that might threaten my life.
Artificial feeding (via a tube or drip)
When my dementia has deteriorated to the point that I cannot swallow safely, even with the help of others

Caring in Devon
When is an ADRT not valid?
• If medical treatment has changed significantly since the ADRT was made
• If it is not specific enough to include current circumstances – home, family and health
• If ‘out of date’ - good practice to update every 2 years
• If a LPA has been drawn up covering the same treatment
• If a person has recently behaved in a way to suggest they have changed their minds
• If there is any evidence of duress• If there is any evidence the patient has
withdrawn the ADRT

Caring in Devon
What can an ADRT not do?
An ADRT cannot:-
• Request specific treatment• Stop basic care
• nutrition/hydration by mouth• basic cleanliness
• Ask a HCP to end or intentionally shorten a patients life

Caring in Devon
Lasting power of Attorney (LPA)
• An LPA is a statutory form of power of attorney is created by the MCA. A person with capacity can choose a person (an ‘attorney’) to take decisions on their behalf if they subsequently loose capacity.
• Two separate documents: Property and Financial Affairs Health and Welfare
• Must be registered with the Office of the Public guardian. (Therefore this may take time to put in place)

Caring in Devon
Resuscitation

Caring in Devon

Caring in Devon
Resuscitation- allow natural death (AnD)
• Are not obliged to offer treatment to pts that we think are futile.
• It is good practice to discuss this with patients wherever possible but..not if it is going to cause them distress and do them harm.

Caring in Devon
ACP and DNAR
• Success rates poorly understood• Inappropriate resuscitations can lead to
distressing, undignified deaths• May result in transfer to hospital when death
requested at home/care home ect• May be part of a PPC/LCP which is not
clarified/respected• DNAR requests within an ADRT are not always
accessible- and paramedic crews need to see a signed document to withhold resus attempt if responding to a 999 call.

Caring in Devon
Core Competencies for ACP

Caring in Devon
Questions to think about…
• Are you ready to be asked?• If planning to instigate with someone….who
might be best placed to do so?• Is now the right time?• Which aspects do I raise and which do I feel
competent to respond to?• Who else might need to be involved?• Which documents/tools (if any) might be
useful for this patient/client/user/carer?• What support is there for me?

Caring in Devon
Summary points
• The process of ACP can enable people to think about, discuss and have their wishes recorded in advance of an anticipated decline in their health.
• ACP conversations and documents can be referred to if/when a person lacks the capacity to make a decision about their care and treatment. However, it also guides and can instruct loved ones, health and social care staff to plan and deliver appropriate and realistic care for each individual.
• Not desirable for everyone. We need to think critically about if, how and when we implement ACP into practice and our assessments.

Caring in Devon
So..ACP is more likely to benefit people when it takes place:-
• At the right time• Within the right environment• Using the right skills• For the right reasons

Caring in Devon
My ADRTLast night my husband and I were in our sitting room. I said to him “I never want to live in a persistent vegetative state, dependent on some machine..and fluids from a bottle”
He got up, unplugged the computer and threw out my wine

Caring in Devon
What's happening in Devon?
• End of life register is now live (Adastra)• Preferred priorities of care (PPC) and Advanced
decision to reuse treatment (ADRT) documents are approved for NHS Devon
• Just in Case bags are in all GP practices across Devon
• GSF in practices and nursing homes• New community worker in EOL care pilot• Working to develop a Devon wide DNAR policy
probably a treatment escalation plan (TEP)