Embed Size (px)
Citation preview

AIRWAY ANATOMY & ITS IMPLICATION IN
ANAESTHESIA
Dr Ramprasad GoraiPGT-Dept of Anaesthesiology
R.G.Kar Medical College,Kolkata

AIRWAY ANATOMYUPPER AIRWAY(Part above cricoid cartilage)1. Nose & Paranasal sinuses2. Oral cavity3. Pharynx4. LarynxLOWER AIRWAY1. Trachea2. Lt & Rt Principal Bronchi3. Secondary (Lobar) bronchi4. Segmental (Tertiary) bronchi5. Terminal bronchiole6. Respiratory bronchiole7. Alveolar duct & Sacs

NOSE
INTERNAL NOSE1. Lt & Rt Nasal Cavities2. Nasal Septum Collumeller Septum Membranous Septum Septum Proper a. Cartilage 1/3 b. Bone 2/3
NASAL CAVITITY1. Vestibule2. Respiratory Segment3. Olfactory Segment
EXTERNAL NOSE1. Osteo-Cartilagenous 2. Ala Nasi3. Nasal Skin

1.Vestibule Strat column epithelium. Vestibular hair (Vibrissae) filter large particulate matter. Lamina propria a. Hair follicle b. Ecrine gland c. Sebaceous gland2. Respiratory Segment Ciliated Pseudo strat Column Contains Goblet,Basal,Brush, Neuro -endocrine cell3. Olfactory Segment Olfactory epithelium Contains: Bipolar neurosensory cell supporting cell regenerative basal cells

NASAL SEPTUM
• Consist of-1. Septal Cartilage2. Perpendicular plate(Ethmoid)3. Vomer4. Crest of Nasal bone5. Nasal Spine of Frontal bone6. Rostrum of sphenoid bone7. Crest of Palatine bone8. Crest & Ant nasal spine of
Maxilla

PARANASAL SINUSBlind ended air containing Cavity in certain skull bones.2 groups—Anterior Group1. Maxillary2. Frontal3. Ant EthmoidalPosterior Group1. Posterior Etmoidal2. Sphenoid
Functions1.Warm & Humidify Inspired Air
2.Resonance to Voice

PHARYNX
• Musculo-membranous tube extend from base of skull to 6th Cerveical Vertebra.
• Length-12-14 cm• Width- Max 3.5 cm(Naso Pharynx) - Min 1.5 cm(Pharyngo esophageal Jn)* 3 Part---- 1. Naso/Epi-Pharynx 2. Oro/Meso-Pharynx 3. Laryngo/Hypo-Pharynx
At the base of tongue EPIGLOTTIS functionally separate Oropharynx from Laryngopharynx.

LARYNX LARYNX Lies- in front of hypopharynx & opposite to 3rd to 6th Cerveical vertebra. Composition-
1.CARTILAGE-3 Unpaired & 3 Paired(Total 9)
UNPAIRED—Thyroid, Cricoid , Epiglottis PAIRED ---Aretenoid, Corniculate, Cuneiform
2.MUSCLES---Intrinsic & Extrinsic.
3.JOINTS—Cricothyroid & Cricoarytenoid
4.MEMBRANE-Intrinsic & Extrinsic
5.CAVITY- Inlet. Vestibule. Sinus of Lrynx. Infraglottic part.
6.MUCOSA-Ciliated Pseudostratified Columnar except VC--Strat squamnous.

LARYNX


SENSORY NERVE SUPPLY
NASAL CAVITYANT-Anterior ethmoidal N(br of Ophthalmic div-V1)
POST-Sphenopalatine (br of Maxillary div -V2)
TONGUE(GEN SENSATION)ANT 2/3—Lingual Nerve(br of Mandibular div of Trigeminal)POST 1/3-Glossopharyngeal nerve.
PHARYNXGlossophayngeal nerve also innervate - Roof of pharynx Tonsil under surface of soft palate.
LARYNX Below the epiglottis --VAGUS.Above vocal cord-Internal Laryngeal branch Below vocal cord-Recurrent laryngeal branch

NERVE SUPPLY

TRACHEA Membrano cartilaginous tube Lower border(Carina) T4 vertebra- supine & cadaver T6 vertebra- standing & living Length- 10-11 cm Breadth-12 mm in adult. (int diameter) 3 mm (newborn –upto 3 yr) increase by 1mm/year till 12 yr of age. Structure-16-20 C-shaped hyaline cartilage connected by
strong fibroelastic memb & posterior deficit part contain involuntary trachealis muscle
Relation-Thyroid Isthmus-2nd.3rd .4th Ring


ZONE OF AIRWAY(23 generation)Conducting zone-(First 14 gen)TracheaPrincipal BronchiSegmental bronchi-upto Terminal bronchiole
Transitional zone-(15th gen)Terminal bronchiole(3-4 generation)
Respiratory zone-(Last 8 gen)Respiratory bronchioleAlveolar ductsAlveolar sacs.


BRONCHO-PULMONARY SEGMENT Def- The portion of the lungs aerated by each tertiary or segmental bronchus. Features-- an independent respiratory district.- covered by inter-segmental septa through which br of pulmonary vein runs.- the largest sub-divisions of the lobe and is surgically resectable.- supplied independently by segmental brochus and a tertiary branch of pulmonary artery.

Bronchopulmonary segments
Right Lung :
Superior Lobe :ApicalPosteriorAnterior
Middle Lobe :LateralMedial
Inferior Lobe:SuperiorAnterior basalPosterior basalMedial basalLateral
Left Lung :
Superior Lobe :Apico-posteriorAnterior
Lingular Lobe :SuperiorInferior
Inferior Lobe:SuperiorAnterior basalPosterior basalLateral

Left main bronchus and its divisions

Rt BronchousRIGHT BRONCHUS IS WIDER ,SHORTER AND MORE VERTICAL THAN LEFT BRONCHUS
IT IS WIDER B/C IT SUPPLIES MORE VOLUMINOUS RT LUNG
IT IS MORE VERTICAL B/C AT ITS BIFURCATION TRACHEA DEVIATES MORE TO THE RT SIDE

Right main bronchus and its divisions

At a glance…


ACINUS V/S TERMINAL RESPIRATORY UNIT• ACINUS-The ultimate lung unit from each
terminal bronchiole.
• TRU-all alveolar duct & their accompanying alveoli,that stem from the most proximal (first) respiratory bronchiole.
• 1 Acinus contain 10-12 TRU.
• Anatomist & Pathologist –Acinus.
• Physiologist & Pulmonologist-TRU.







ANATOMICAL VARIATION & IMPLICATION IN ANAESTHESIA
Conventional Laryngoscopy – done in -supine position -a slight Neck flexion of 25-35 deg -Head extension of 85deg at atlanto-occipital
joint to align oral,pharyngeal & Laryngeal axes.
In adult a head elevation of 10 cm with a pillow is appropriate for neck flexion.
No such elevation required in pediatric age gr (<8yr age) d/t their large head size.
This position is called OPTIMAL SNIFFING POSITION.

AIRWAY ASSESSMENT• Mouth opening: an incisor distance of 3 cm or
greater is desirable in an adult.• Upper lip bite test: the lower teeth are brought in
front of the upper teeth. The degree to which this can be done estimates the range of motion of the tempero-mandibular joints .
• Mallampati classification: examines the size of the tongue in relation to the oral cavity. The greater the tongue obstructs the view of the pharyngeal structures, the more difficult intubation

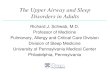
Cont…• ■ Class I: the entire palatal arch, including the
bilateral faucial pillars, are visible down to their bases.
• ■ Class II: the upper part of the faucial pillars and most of the uvula are visible.
• ■ Class III: only the soft and hard palates are visible.• ■ Class IV: only the hard palate is visible.• Thyromental distance: the distance between the
mentum and the superior thyroid notch. A distance greater than 3 finger breadths is desirable.
• Neck circumference: a neck circumference of greater than 27 inch is suggestive of difficulties in visualization of the glottic opening.

Mallampati Classification of oral openingLaryngoscopic grade of Cormac & Lehane

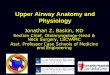
Airway of Neonates and infants
• Relatively larger head and tongue• Narrower nasal passages• Anterior and cephalad larynx• Relatively longer epiglottis• Shorter trachea and neck• More prominent adenoids and tonsils• Weaker intercostal and diaphragmatic
muscles• Greater resistance to airflow• Adult larynx is cylindrical but • Childs larynx is Conical.

Cont…..narrowest point of the airway- cricoid cartilage (children younger than 5 years of age) glottis ( in Adult)
One millimeter of mucosal edema will have a proportionately greater effect on gas flow in children because of their smaller tracheal diameters.
The presence of fewer, smaller airways produces increased airway resistance.The alveoli are fully mature by late childhood(about 8 years of age). The work of breathing is increased and respiratory muscles easily fatigue.

Pediatric Airway

Anatomical change during Pregnancy.• Most of the changes during pregnancy are
Physiological.• Capillary engorgement of the respiratory
mucosa during pregnancy predisposes the upper airways to trauma, bleeding, and obstruction.
• Gentle laryngoscopy and smaller endotracheal tubes (6–6.5 mm) should be employed during general anesthesia.


EMERGENCY TRACHEOSTOMY
• 4 Step• Horizontal skin incision• Expose investing layer
of Deep Fascia• Divide/Displace
Isthmus.• Vertical incision in
trachea.



Aspiration, pneumonia and lung abscessRight lung is most frequently involved as the right main bronchus directly takes off from principle bronchus.
In the recumbent position, superior segment of the right lower lobe and posterior segment of the right upper lobe are the most dependent segment of the lung &in standing position, basilar segment of the lower lobe is most dependant.
Aspiration pneumonia involving apical segments of the lower lobe is known as mendelson’s syndrome

Postural DrainageIt consist of positioning the patient to allow gravity to assist the drainage of secretions from specific areas of the lungs
Segments receiving drainage should be uppermost
Treat the lower lobe segments first and upper lobe last
Aerosol therapy with humidification prior to PD
Worst area should be drained firstOn average 15-20 mins is spend in each position
During PD :
Chest manipulations like(Vibration, clapping/percussion, shaking )-Tappotment massage are performed in postural drainage position.
Should be done in order.
Vibrations and clapping first .
Shaking next

Upper lobe-apical segments (bilateral)
Half lying

Upper lobe-posterior segment-right
left side lying 45 degree turn towards face side

Upper lobe-posterior segment-Left
Right side lying45 degree turn towards face sideThree pillow

Middle lobe –lateral and medial segments right
From supine 45 degree turn towards leftpillow from shoulder to hip
foot end raised 14”

Left Lingula –superior and inferior segments
From supine 45 degree turn towards rightpillow from shoulder to hip
foot end raised 14”
14”

Lower lobe-apical segments(bilateral)
Prone lying pillow under hip

Lower lobe-anterior basal segments(bilateral)
supine lying pillow under hip
foot end elevated to 18”
18”

Lower lobe-posterior basal segments(bilateral)
prone lying pillow under hip
foot end elevated 18 inches
18”

Lower lobe- Medial basal of right& lateral basal of left
Right Side lying pillow under hip
foot end elevated 18”
18”

Lower lobe-lateral basal segment-rightLeft side lying
pillow
18”

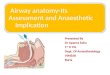
Technique for airway management of a patient with suspected spinal cord injury.
One individual holds the head firmly with the patient on a backboard, the cervical collar left alone if in place, ensuring that neither the head nor neck moves with direct laryngoscopy. A second person applies cricoid pressure and The third performs laryngoscopy and intubation.BUT Gold standard is FLEXIBLE FIBEROPTIC INTUBATION .
laryngoscopy with in-line stabilization

•
Thank you