Embed Size (px)
Citation preview



Airway management :Comparative study between
McGrath VL , Airtraq VL
and
Macintosh laryngoscope
in neutral neck position

Presented by
Alaa Elsayed Goma FalogyM.Sc. of Anaesthesia and surgical intensive care
Faculty of medicine
Zagazig university
2016

Under supervision of
Professor
Ayman Abdel El-Salam
Professor of Anesthesia and surgical
Intensive Care
Faculty of Medicine – Zagazig university

Under supervision of
Professor
Ahmed Abd El-Hakim Balata
Professor of Anesthesia and surgical
Intensive Care
Faculty of Medicine – Zagazig university

Under supervision of
Professor
Khaled Mohammed El-Sayed
Professor of Anesthesia and surgical
Intensive Care
Faculty of Medicine – Zagazig university

Prof. Dr.
Ayman Abdel SalamMy deep gratitude and greatest debt
for his sincere guidance.
Thanks My Dear prof; Ayman

Prof. Dr.
Ahmed Abdel Hakim Balata,
for his kind supervision, valuable
guidance and for being always backing
and supporting.
Thanks Dear Dr, Ahmed

Prof. Dr.
Khaled Mohammed ElsayedReal kindness and deepest support
Thanks Dear Dr, Khaled .

Disclosure & Conflict of interestThe researcher confirm and
stated that:
the manufacturers of the
neither Airtraq nor McGrath
VL, had NO involvement in
the;
concept,
design ,
conduct,
analysis, or
write-up of this clinical trial

Research questionIf……
used by [experienced anesthiologists]
managing a model of a difficult airway in
form of neck immobilization by semi- rigid
neck collar
Do………
[the Airtraq and the McGrath VL]
Are……
[more safe and more effective in tracheal
intubation ] when compared with [Classic
Macintosh laryngoscope]?

Introduction

INTRODUCTION:• Airway management is a major challenge upon
the anaesthesiologists in their everyday
operative practice.
• During direct laryngoscopy, positioning of the
head and neck in
NEUTRAL POSITION
will decrease chance of optimal laryngeal
visualization which derange the line of sight
between laryngeal , pharyngeal and oral axes.

INTRODUCTION:
• patients with cervical spine instability, airway
management implies upon a high risk of
neurological damage related to head and neck
manipulation, so semi-rigid neck collar is applied
in trail to control neck movement during tracheal
intubation.
• Such immobilisation technique can turn
intubation under the direct laryngoscopy into
more difficult situation (corrupted line of sight) .

INTRODUCTION:
• These concerns have aroused the idea to developnumber of alternatives to classical Macintoshlaryngoscope such as Airtraq ®, McGrath® Videolaryngoscope.
• These laryngoscopes do not require the arrangement ofpharyngeal, laryngeal and oral axis in one line of sightand thus do not require modulation of neutral headposition.
• During difficult airway situations, both Airtraq opticallaryngoscope and McGrath Video laryngoscope soundto be better than Macintosh laryngoscope

AIM OF THE WORK• To evaluate the efficacy and safety of :• Airtraq Laryngoscope and
McGrath Video Laryngoscope versusClassical Macintosh Laryngoscope
• in stimulated difficult intubation situations• in patients with their cervical spine kept in
neutral position• by semi-rigid neck collar as an
immobilization techniques.

in stimulated difficult intubation situations
in patients with their cervical spine kept in neutral position
by semi-rigid neck collar as an immobilization techniques.

Concept of line of sight
during direct laryngoscopy :

Idea of Alignment of 3 axes in direct
laryngoscopy


Situation
Stimulated difficult intubation
Patients with their cervical spine kept in neutral neck position
Semi-rigid neck collar

Cervical spine stability:
Cervical Stability:
is the ability of the
spine to maintain
relationships
between vertebrae,
so as not to
damage the neural
structures contained
within the spinal
column
Cervical instability:
Is defined as over
translational or
rotational motion of
any vertebra and
means that the
odontoid process is
no longer firmly
held against the
back of the anterior
arch of C1.
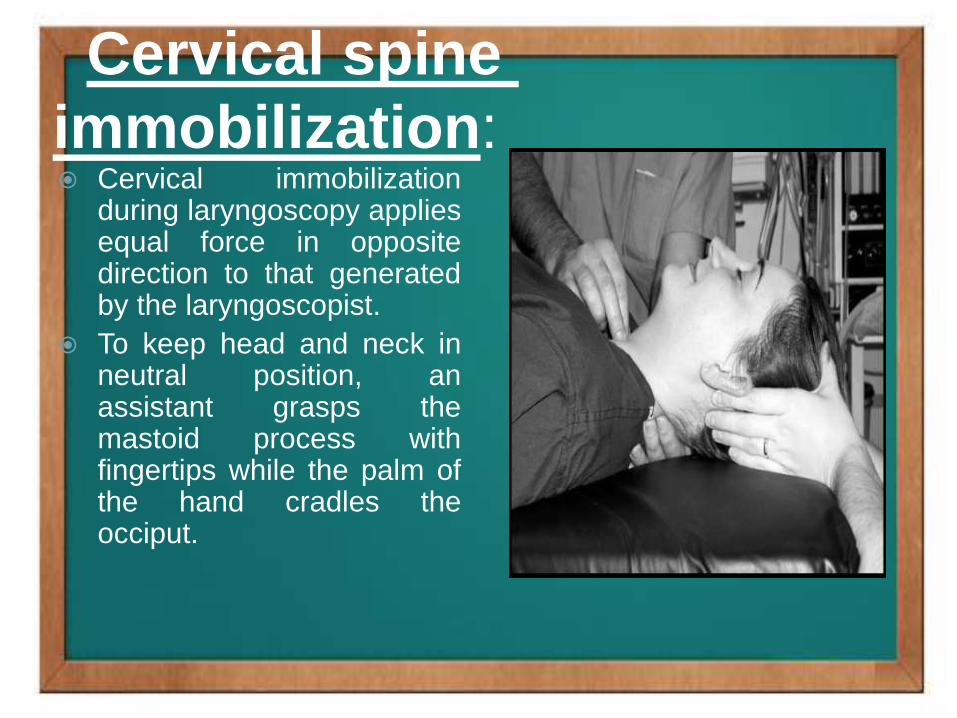
Cervical spine
immobilization: Cervical immobilization
during laryngoscopy appliesequal force in oppositedirection to that generatedby the laryngoscopist.
To keep head and neck inneutral position, anassistant grasps themastoid process withfingertips while the palm ofthe hand cradles theocciput.

Concept of
Videolaryngoscopy: Video laryngoscopy (VL) is an
update of high resolution
micro-cameras systems that
improves the success rate of
intubation.
There is hypothesis improved
lighting and a better view can
increase the intubation
success.
Anaesthesia had used the
miniature camera for many
years but for only bronchial
endoscopy .

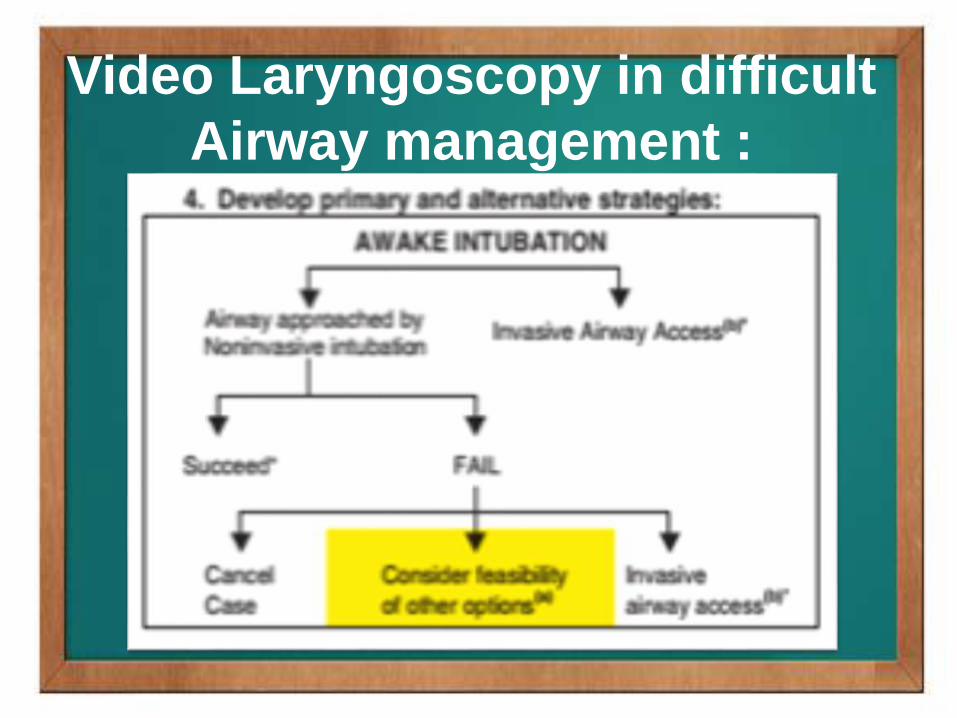
Video Laryngoscopy in difficult
Airway management :
Video Laryngoscopy in difficult
Airway management :

Video Laryngoscopy in difficult Airway
management (after unsuccessful attempts) :

McGrath video-laryngoscope

The McGrath Video Laryngoscope:
(Aircraft Medical, Edinburgh, United Kingdom)• a video-based system for tracheal intubation thatutilizes a video camera embedded into a camerastick.
• The unit is powered by a single easily-replaceable1.5 v AA battery
• features a single electronic control; an on/offswitch located on the top of the unit.
• It therefore offers the user an image of the vocalcords and the surrounding airway anatomy on aliquid crystal display (LCD) screen.

McGrath Video Laryngoscope:
• The unit which is used as a part of much thesame way as common as Macintoshlaryngoscope
• with a special case that once it has beenbrought into mouth by a couple centimeters,operator’s attention must be directed to theLCD show.
• In video laryngoscopes we pay attention onthe superior view and access provided byvideo screen show

The McGrath Video Laryngoscope:
• The intubationist uses direct vision to insertthe video laryngoscope in the mouth andthen the video-imaging screen to obtain thebest possible perspective view of the glottis(step 2).
• In step 3, the eyes then returned to theoropharynx to introduce the ETT and thenback to the video image screen toaccomplish the intubation (step 4).

Concept of the improved
glottic view

AIRTRAQ Optical Laryngoscope

AIRTRAQ Optical Laryngoscope
based on refraction prism principle to give an angular
view of the glottic area.
The blade of the Airtraq consists of two side by side
channels.
One channel act as housing for the ETT, and the other
channel terminates in terminal lenses and transmit back
the image.
The viewed image is then been transmitted to a proximal
eye piece viewfinder employing a prisms system and lenses
not as basic concepts of usual fiberoptics.
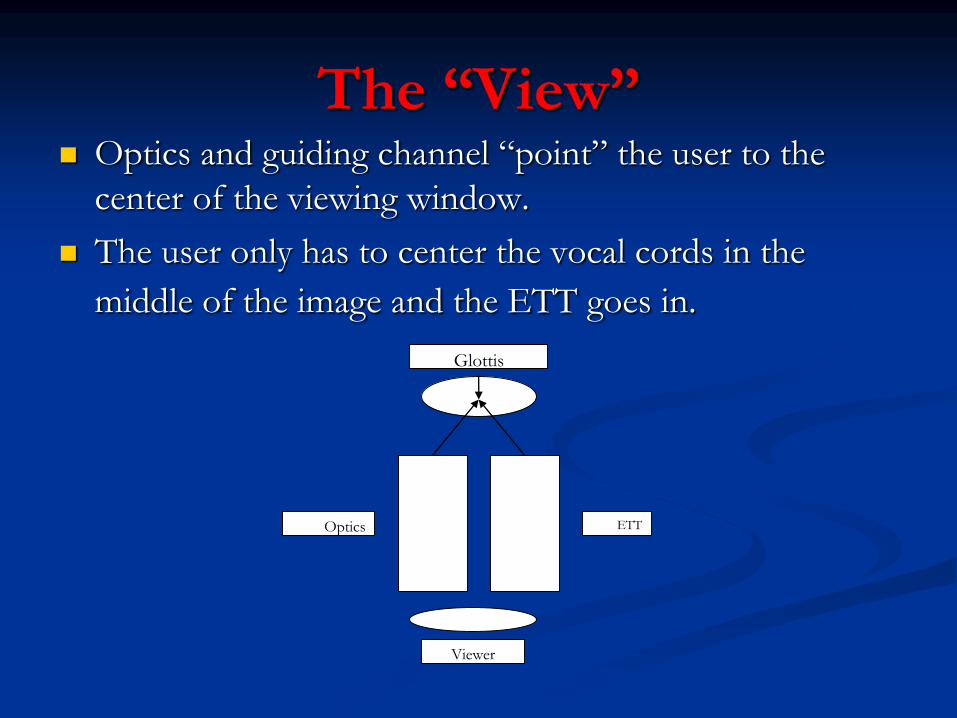
The “View” Optics and guiding channel “point” the user to the
center of the viewing window.
The user only has to center the vocal cords in the
middle of the image and the ETT goes in.
Glottis
Viewer
ETTOptics

Macintosh
laryngoscope

PATIENTS AND METHODS

METHODOLOGY
This was a prospective, randomized clinical trial.
group assignments (C, A and M)
age group of 20-50 years, ASAps Grades I or II
undergoing elective surgery requiring general
Anaesthesia
three groups of 50 patients each.

Inclusion criteria
Of either sex
Within the age group of 20-50 years,
ASAps Grades I or II
Undergoing elective surgery
Requiring general Anaesthesia and endotracheal
intubation

Exclusion criteria
Include:
Anticipated Difficult Airway (Mallampati Class III
And IV)
Thyromental Distance <6 Cm)
BMI>35
Cardiovascular Disease
Endocrine Disease,
Presence Of Risk Factors For Gastric Aspiration
E.G. Pregnancy, Diabetes, Etc.

Standard monitoring
All patients received standard monitoring included
electrocardiography,
non-invasive arterial blood pressure,
pulse oximeter,
end-tidal carbon-dioxide.
Heart rate (HR), mean arterial blood pressure (MAP)
and Oxygen saturation were recorded pre and post-
intubation.

INTUBATION PROCEDURE
Pre-oxygenation
Induction of anesthesia, administration of
fentanyl 1.5μg/kg (i.v.) then propofol 2 mg/kg
followed by rocuronium bromide 1 mg/kg.
Then neck was immobilized using semi-rigid
neck collar of appropriate size (Zola Collar, Egypt)
and was kept in place throughout airway
management process.

INTUBATION PROCEDURE
Tracheal intubation was then undertaken using
one of the study devices.
Intubation was performed by an experienced
anesthesiologist with accepted experience in two
recent video laryngoscopes under study.
A malleable stylet was used in both groups
(Classical Macintosh and McGrath VL).

INTUBATION PROCEDURE
The technique was considered failed if tracheal
intubation was not achieved within 120 seconds
or
within a maximum of three intubation attempts.
Mucosal damage was defined as the presence of
blood on the devices following intubation
process.

INTUBATION PROCEDURE
The glottic view was assessed and recorded
using Cormack and Lehane grading (C&L grade)
system.

CORMACK & LEHANE SCORE
Grade I Grade II
Grade III Grade IV

INTUBATION PROCEDURE
Intubation time was separated into T1 and T2.
T1 is the time between insertions of the allocated
laryngoscope in the mouth until optimal glottic view
including optimization maneuvers.
T2 is the time from optimal glottic view till
confirmation of tracheal intubation (by vision)
including removal of the device.

Intubation sequence by McGrath VL
With the patient in neutral position, Use left hand to
introduce the VL into the midline of the oropharynx.
Push the blade tip till the tip is past the posterior portion
of the tongue.
Now, move eyes to the video screen in order to
manipulate the video scope and obtain the best view of the
glottis.
Advance and withdraw the laryngoscope slightly while
changing the tilt of the blade along with the camera and
seat the device in the vallecula

Intubation sequence by McGrath VL
The video image of the glottis now is
representing Cormack – Lehane view.
The styletted ETT is then inserted under direct
vision. Using video visualization, the ETT is
then advanced on a smooth curve through the
glottis.

Intubation sequence by McGrath VL

Intubation sequence by McGrath VL

Intubation sequence by McGrath VL

Intubation sequence by McGrath VL
55

Intubation sequence by McGrath VL
56

Intubation sequence by Airtraq OL
Add lubricant to outer surface of the
endotracheal tube.
Embed the tube into the side holding channel of
the Airtraq so that the tip of the endotracheal
tube is at the tip margin of the side channel.
Turn on the light for about 30-60 seconds
before the procedure.
57

Intubation sequence by Airtraq OL
Hold the device in the mouth in the midline.
advance by sliding the device over the tongue.
check the image on view finder to optimize the
view by moving the blade right and left as
necessary.
Be sure that the laryngeal inlet is in the centre of
viewfinder just before pushing forward the
ETT.
58

Intubation sequence by Airtraq OL

Intubation sequence by Airtraq OL

Intubation sequence by Airtraq OL

Intubation sequence by Airtraq OL

Intubation sequence by Airtraq OL

Intubation sequence by Airtraq OL
RESULTS
OF
THE
STUDY

Comparison between groups are done
according to:
INTUBATION CONDITIONS
NUMBERS OF ATTEMPTS
Optimization Procedures
Cormack and Lehane score
IDS
SUCCESS RATE OF INTUBATION
TIME TO INTUBATION
HEMODYNAMICS
COMPLICATIONS

DEMOGRAPHIC DATA
NO significant differences in demographic data
regarding
Age,
Gender,
Height,
Weight,
Body mass index and
ASAps among the studied groups

DEMOGRAPHIC DATA
68
Demographic data Group C Group A Group M p-value (Sig.)
(N=50) (N=50) (N=50)
Age (in years) 35.90±7.65 35.92±7.70 35.16±7.72 0.856** (NS)
Male / Female 62 / 38 % 66 / 34 % 60 / 40 % 0.892* (NS)
Height (cm) 171.48±3.71 171.62±3.54 171.6±3.8 0.981** (NS)
Weight (Kg) 77.96±7.22 77.62±6.25 76.86±6.93 0.619** (NS)
BMI (Kg/m2) 26.84±2.29 27.06±2.05 26.14±2.13 0.095** (NS)
ASAps I / II 14 / 86 % 16 / 84 % 10/ 90 % 0.668* (NS)
MS I / II 56 / 44 % 48 / 52 % 62 / 38 % 0.369* (NS)
TMD (cm) 7.18±0.34 7.12±0.34 7.17±0.32 0.766** (NS)

DEMOGRAPHIC DATA

INTUBATION PROCESS
PARAMETERS
Parameters p-value (Sig.)
Numbers of attempts (<0.001)*(HS)
1st
/2nd
/3rd
(0.002)* (HS)
Optimization: No/YES (<0.001)* (HS)
ID score (<0.001)**(HS)
Successfulness (0.068)* (NS) C&L I/ II / III <0.001)*(HS))
Complications: No / YES (0.135)* (NS)

INTUBATION PROCESS
PARAMETERS SUMMARY
Numbers of attempts
Videolaryngoscope WINS
HS

INTUBATION PROCESS
PARAMETERS SUMMARY
OPTIMIZATION
Videolaryngoscope WINS with less
maneuvers
HS72

INTUBATION PROCESS
PARAMETERS SUMMARY
IDS
Videolaryngoscope WINS with less
than 1 score
HS73

INTUBATION PROCESS
PARAMETERS SUMMARY
CORMACK-LEHANE GRADE
Videolaryngoscope WINS with more
% of grade I
HS74

INTUBATION PROCESS
PARAMETERS SUMMARY
SUCCESSFULNESS
NS?

INTUBATION PROCESS
PARAMETERS SUMMARY
COMPLICATIONS
NS?

AND HERE IS THE ANSWER?
FAMILAR
ITY

Post-hoc inter-group analysis
Analyzed data represent high statistical significance
difference between groups (C and A) as regard
Number of attempts (p = 0.002),
Optimization (p = 0.001),
ID score (p = 0.001) and
only significant difference regarding
successfulness (p = 0.041).

Post-hoc inter-group analysis
By comparison of group (C vs M) there was
high statistical significance difference as regard
Number of attempts, Optimization, and ID
score (p values was 0.009, <0.001, and <0.001
respectively)
but there was NO significant difference as
regard successfulness between these two groups
(C vs M) (p = 0.169).

Post-hoc inter-group analysis
No statistical significance detected between groups
(A vs M) as regarding
Number of attempts (p = 0.842),
Optimization (p = 0.137),
ID score (p = 0.229)
successfulness (p = 0.315).

Post-hoc inter-group analysis
81

RESULTS OF THE STUDY
IDS DISTRIBUTION
Group C showed highest Mean±SD (3.38±2.14)
versus (0.14±0.35) and (0.32±0.68) in group A
and group M respectively.
Group C showed highest median among other
groups (3) versus (0) in groups M and A.
There was high significance difference in
distribution of IDS among three groups
(p<0.001).

RESULTS OF THE STUDY
IDS DISTRIBUTION

RESULTS OF THE STUDY
Cormack-Lehane score in each group
C&L of I; was highest in group A (98%)
followed by (12% and 74%) in groups C and M
respectively.
C&L of II; it was highest in group C (62%)
followed by (2% and 24%) in groups A, and M
respectively.
C&L of III; it disappeared in group A and
represented by (26% and 2%) in groups C and
M respectively.

RESULTS OF THE STUDY
Cormack-Lehane score in each group
85

RESULTS OF THE STUDY
numbers of attempts
Group A showed highest percentage of patients
that intubated in first attempt in comparison to
other groups (90%), versus (88%) and (62%) in
groups M and C respectively.
Group C had the highest percentage of patients
intubated from second attempt (28%) versus
(10% and 10%) when compared to groups A
and M respectively.
86
RESULTS OF THE STUDY
numbers of attempts
NO patients intubated by third attempt in group
A when compared to other groups
Group C showed highest Mean±SD (1.48±0.67)
vs ((1.1±0.3) (1.14±0.4)) in group A and group
M respectively, with highly significant data
difference among groups (p<0.001).
There was high significant data difference in
distribution of numbers of attempts in between
groups (p<0.002).

RESULTS OF THE STUDY
numbers of attempts

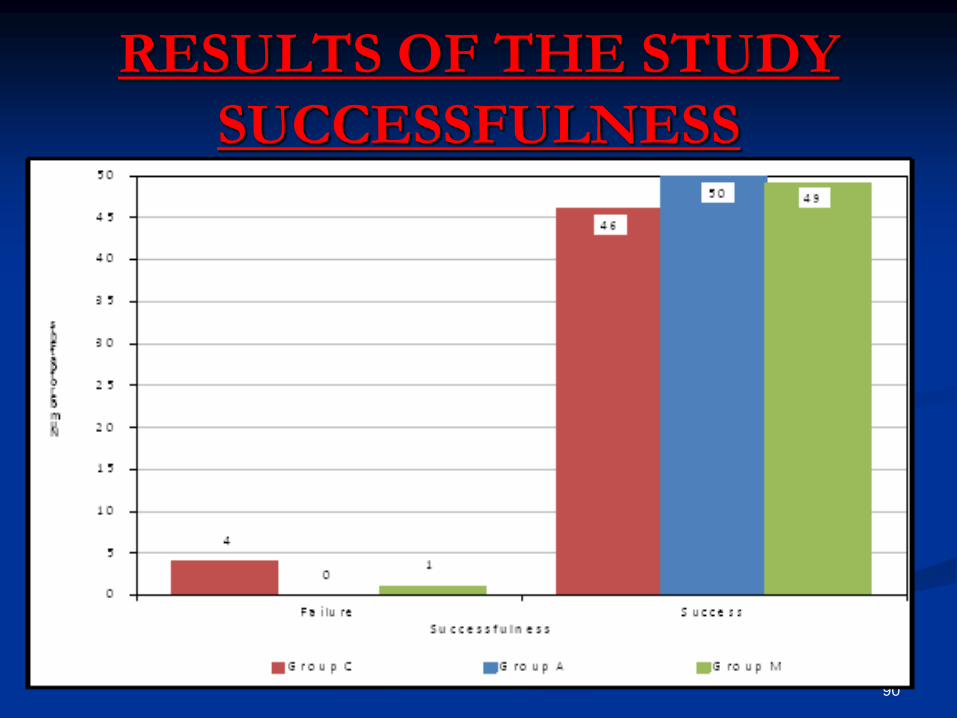
RESULTS OF THE STUDY
SUCCESSFULNESS
number of patients who were successfully
intubated in three groups which was highest in
group A (100%) followed by (98% and 92%) in
group M and group C respectively.
These data was of non-statistical significant.
89
RESULTS OF THE STUDY
SUCCESSFULNESS
90

RESULTS OF THE STUDY
HEART RATE
As regard Heart Rate:
non statistical significance between all groups
regarding change in heart rate in pre-intubation
time, or after intubation (at immediate post-
intubation, 1 and 5 minutes post-intubation).
But there were statistical significance upon
comparison of post-intubation with pre-
intubation data.
91

RESULTS OF THE STUDY
HEART RATE
92

AIRTRAQ LEAST
MACINTOSH MOST

As regard hemodynamics?
Heart rate:
AIRTRAQ
was less than other two laryngoscopes in
stimulation of heart rate
MAP:
Same distribution
No upper hand for any


Definition of intubation time
T1;from insertion of the device into the mouth till
optimal glottic view.
T2;from optimal glottic view till confirmation of
tracheal intubation (by vision).
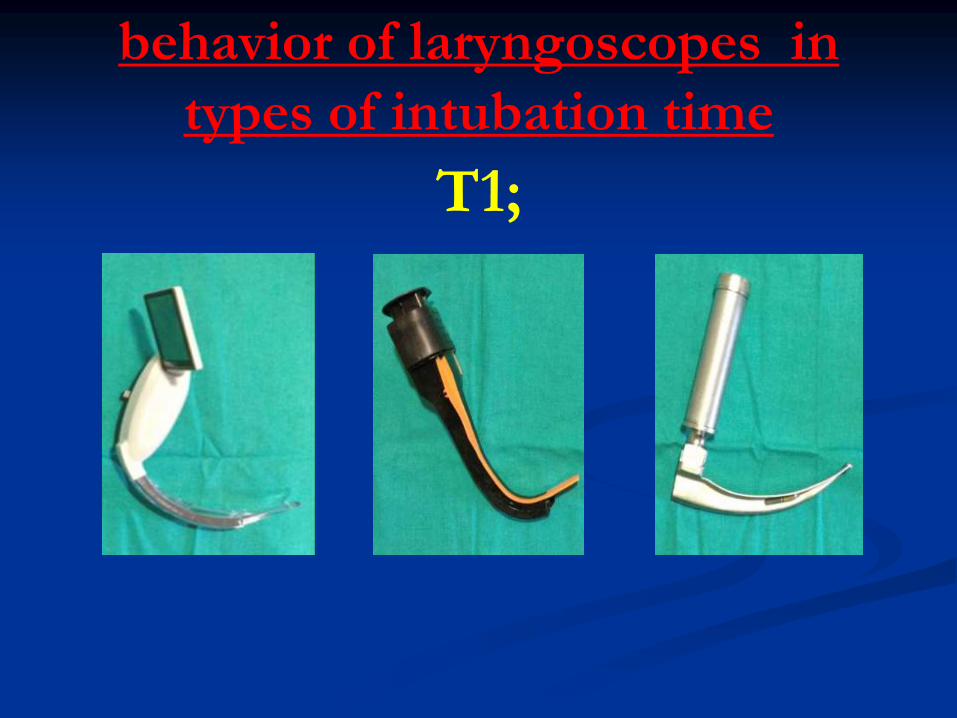
behavior of laryngoscopes in
types of intubation time
T1;

behavior of laryngoscopes in
types of intubation time
T2;

When it comes to intubation
time?
THE RESULTS ARE:
HSEXCEPT SMALL
NS

When it comes to intubation
time?
100

RESULTS OF THE STUDY
Complications Occurrence
As regard frequency of complications :
non statistical significance between all groups
regarding presence or absence of complications
(p=0.135).
However there was high statistical significance
difference between occurrences of primary and
secondary complications between all groups (p=
0.006).

RESULTS OF THE STUDY
Complications Occurrence
As regard occurrence frequency of 1ry and 2ry
complications:
There was high statistical significance between
groups A versus M (p< 0.003),
Statistical significant difference between groups
C versus M (p= 0.013),
But NO statistical significant difference between
groups C versus A (p=0.711).

RESULTS OF THE STUDY
Complications Occurrence

RESULTS OF THE STUDY
Complications Occurrence

SIMILAR RESULTS
ON SAME TOPIC






SYSTEMIC META-ANALYSIS
DISCUSSING VIDEOLARYNGOSCOPES

SYSTEMIC META-ANALYSIS
DISCUSSING VIDEOLARYNGOSCOPES

ARTICLES…….


LIMITATIONSDESIGN
operator knows the devices, which may also introduce bias.
(solved by closed envelopes basis).
STIMULATIVE
not on real cervical trauma patients.
FURTHERMORE………
inter-incisor distance may be added in airway assessment
parameters as pre and post insertion of neck collar especially
because it affects primary insertion of Airtraq VL.

RECOMMENDATIONS

This study recommends the use of
videolaryngoscopes in our daily practice to
increase its familiarity to users and specially
in difficult airway scenarios such as neck
immobilization situations because it
provide better airway management even
without extensive training, and it is needed
to conduct similar studies upon real cervical
trauma patients for better assessment of its
advantages and disadvantages.

TAKE HOME MESSAGE
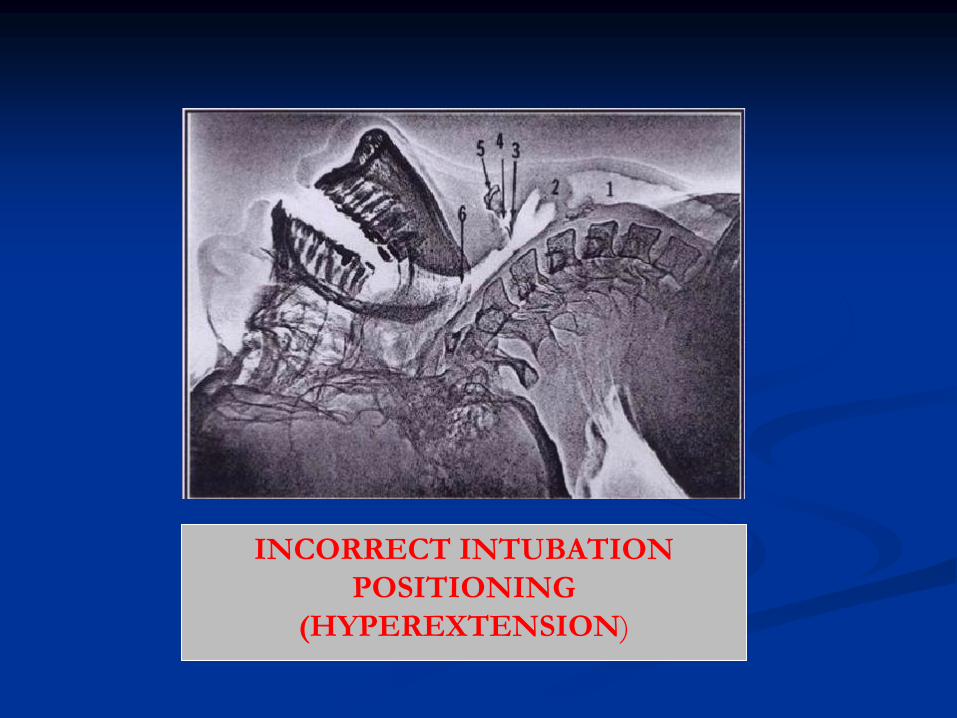
INCORRECT INTUBATION
POSITIONING
(HYPEREXTENSION)

CORRECT INTUBATION
POSITION (NEUTRAL
POSITION)

THANK YOU





























