Embed Size (px)
Citation preview

AlopeciaAlopecia
Nastaran tavakoliNastaran tavakoliGuilan University of Medical sciencesGuilan University of Medical sciences

Anatomy of HairAnatomy of Hair


• Launugo
• Vellus hair
• Terminal hair

• The life cycle of a hair is divided into three phases.
• The actively growing (Anagen)phase• the transitional(Catagen) phase• the resting (Telogen) phase.

Hair Growth CycleHair Growth Cycle

Hair pull testHair pull test

TrichogramTrichogram

Anagen Catagen
Telogen

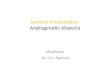
• A physiologic reaction• Genetic• DHEA-S• Norwood-Hamilton Classification• Family history: Commonly positive
Androgenic Alopecia in menAndrogenic Alopecia in men(male pattern baldness)(male pattern baldness)

Norwood-Hamilton Norwood-Hamilton ClassificationClassification



TreatmentTreatment
• Minoxidil(Rogaine)• Finasteride(Propecia)• Autotransplantation of hair• flap surgery• Scalp extension and expansion

Androgenic Alopecia in WomenAndrogenic Alopecia in Women(Female pattern hair loss)(Female pattern hair loss)
• Women with androgenetic alopecia do not have higher levels of circulating androgens.
• Normal menses• Normal fertility• Diffuse central thinning• There is not usually any recession of
the frontal hairline.

• Associated findings: Signs or symptoms of hyperandrogenism should be looked for, ie, hirsutism,moderate to severe or treatment-refractory acne,irregular menses, infertility, and/or galactorrhea.Acanthosis nigricans is a marker for insulin resistance which is commonly associated with hyperandrogenism

• If a woman has irregular menses, abrupt hair loss, hirsutism, or acne recurrence, an endocrine evaluation is appropriate.
• In this situation, total testosterone, free testosterone, dehydroepiandrosterone sulfate,and prolactin levels should be obtained.

• Check TSH and serum ferritin• Hypothyroidism• iron deficiency (serum ferritin or serum iron
and TIBC)
• telogen effluvium








• Minoxidil• Finasteride?• Spironolactone (Aldactone)• Cyproterone Acetate with
Ethinyloestradiol (Diane )
TREATMENT:

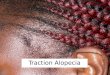
Traction alopeciaTraction alopecia• This condition is caused by localized
trauma to the hair follicles from tight hairstyles that pull at hair over time.
• If the condition is detected early enough, the hair will regrow.
• Braiding, cornrows, tight ponytails, and extensions are the most common styling causes.





![Symmetric alopecia in the dog [Read-Only]alaskanmalamute.org/.../uploads/2015/11/Symmetric-alopecia-in-the … · of alopecia in the dog Pathogenesis Clinical appearance of alopecia](https://img.pdfslide.net/doc/110x75/5ebdda54a09b4c70d34c1b77/symmetric-alopecia-in-the-dog-read-only-of-alopecia-in-the-dog-pathogenesis.jpg)