Embed Size (px)
Citation preview

Alterative Donor HSCT
Now Everyone Has a Donor
Richard Champlin, M.D.

Donor Priority
• HLA matched sibling • HLA matched unrelated donor • Alternative Donor
– One antigen mismatched related or unrelated donor
– Cord Blood – Haploidentical Donor

Best Available Donor

Busulfan-Fludarabine AlloSCT for AML

Survival of patients with early, intermediate, and advanced disease depending on degree of HLA matching (8/8, 7/8, and 6/8) for HLA-A, -B, -C, and -DRB1.
Lee S J et al. Blood 2007;110:4576-4583

Pros and Cons • Matched unrelated donor-
– Pros: • Results ~= matched sib (GVHD higher) • Large system of registries, can find high res 8 of 8 match for >
50% • Can go back to donor for DLI, second transplant, cell therapy
– Cons: • Time search to transplant 2-4 months, too long for urgent patients • 8 of 8 match in only about half, lower if minority race/ethnic origin • Donor unavailability (at least 35%) • Need to carefully coordinate collection and transplant, locked in to
dates, • Uncertain donor availability for second transplants, DLI • Hard to coordinate with chemo for patients with relapsed disease

Pros and Cons • One Antigen Mismatched Unrelated Donor-
– Pros: • Available donor for >90%
– Cons: • All the limitations of matched unrelated donors • Higher risk of rejection, GVHD, infections, TRM • Higher cost/resource requirements- corresponds to
complications • Survival about 10% less than matched transplant

Pros and Cons • Cord Blood
– Pros: • Immunologically immature- less prone to produce GVHD • Less risk of transmitting infection • Immunologically naïve- no preexisting immunity • Can successfully transplant across HLA mismatch • Can identify 5 of 6 or 4 of 6 match for most patients • Has potent GVL effect, ?better than BM • Cells already collected, shorter time search to transplant • Results improving,
– in recent reports = matched unrelated

Pros and Cons • Cord Blood
– Cons: • Low cell dose, slow recovery hematopoiesis and
immunity, • Survival depends on cell dose- double cord required for
most adults • GVHD major problem (with 4 of 6 or 5 of 6 matched Tx) • Relatively high TRM • Can’t go back to the donor for more cells or DLI (?CLI) • Resource intensive
– $$$ for cord(s) – $$$$ for transplant care – Staff/facility requirements – $$$$$ Need system of banks, cost for collection, QA, storage

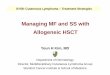
Cum
ulat
ive
Inci
denc
e
SIB
P < 0.01
MMUD
MUD
DUCB 0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5 Years post-transplantation
Minnesota-Fred Hutchinson Experience-Relapse by Donor Type
Brunstein et al 2010

N=3038 Bone marrow Peripheral blood Transplants Year 1980 - 2003
N=280 Cord blood transplants Year 1996 - 2010
59%
25%
M. D. Anderson BMT Department Minority Allo-transplants by Stem Cell Source

Pros and Cons • Haploidentical related
– Pros: • Almost everyone has a haplo match (parent,
child, half of siblings) • Improved results with post transplant
cyclophosphamide, recent results = MUD • Donor immediately available to transplant
center, allows close coordination with chemotherapy
• Don’t need a registry/ banks • Costs similar to matched sibling transplant

Pros and Cons • Haploidentical related
– Cons • Ultimate challenge- most alloreactive transplant • Historically, high rate rejection/GVHD/TRM • T-cell depletion- slow immune recovery,
variable results, poorer results in adults • Studies with post transplant cyclophosphamide-
improved results, but short follow up • Concerns that measures to reduce GVHD will
also reduce GVL and increase risk of relapse

Post Transplant Cyclophosphamide for Haploidentical Transplantation
Luznik,L. Fuchs E.J. et al


Ciurea BBMT 2012

Figure 2
Ciurea 2012

Cumulative incidence of graft-versus-host disease (GVHD) by donor type: (A) grades 2 to 4 acute GVHD, (B) grades 3 to 4 acute GVHD, (C) clinically extensive chronic GVHD, and (D)
severe chronic GVHD by National Institutes of Health consensus criteria.
Bashey A et al. JCO 2013;31:1310-1316

Cumulative incidence of nonrelapse mortality (NRM) and relapse of malignancy by donor type: (A) NRM and (B) relapse; both were analyzed as competing risks.
Bashey A et al. JCO 2013;31:1310-1316
©2013 by American Society of Clinical Oncology

Adjusted estimated probabilities of (A) overall and (B) disease-free survival by donor type.
Bashey A et al. JCO 2013;31:1310-1316
©2013 by American Society of Clinical Oncology






Conclusions • HLA matched sibling- still donor of choice • Many centers question whether MUD is next
priority, can move more quickly to cord blood or haplo transplant
• Improving results with Cord Blood and Haploidentical transplants rivaling matched sib and MUD
• Do cord blood transplants mediate greater GVL effect?
• Are haplo transplants with post Tx Cy associated with more relapse?
• Almost every patient in need has a donor for HSCT