Embed Size (px)
Citation preview
Alternative therapy Alternative therapy for medically for medically
refractory angina refractory angina
BY- DR SARITA CHOUDHARYBY- DR SARITA CHOUDHARY

Refractory anginaRefractory angina
Angina pectoris is a condition characterized by chest discomfort due to myocardial ischaemia associated with coronary artery disease.
It is defined by presence of severe angina with objective evidence of ischemia as demonstrated by exercise treadmill testing, stress imaging studies or coronary physiologic studies and failure to relieve symptoms with conventional medical therapy and even with revascularization techniques.
Patients with refractory angina have either marked limitation of ordinary physical activity or are unable to perform any ordinary physical activity without discomfort (Canadian Cardiovascular Society [CCS] functional class III or IV).

Refractory angina pectoris is a chronic condition characterized by Refractory angina pectoris is a chronic condition characterized by the presence of angina caused by coronary insufficiency in the the presence of angina caused by coronary insufficiency in the presence of coronary artery disease which cannot be controlled presence of coronary artery disease which cannot be controlled by a combination of medical therapy, angioplasty and coronary by a combination of medical therapy, angioplasty and coronary bypass surgery. bypass surgery.
The presence of reversible myocardial ischemia should be The presence of reversible myocardial ischemia should be clinically established to be the cause of the symptoms.clinically established to be the cause of the symptoms.
Chronic is defined as a duration of more than 3 monthsChronic is defined as a duration of more than 3 months So it is the disabling chest pain that persists So it is the disabling chest pain that persists
Despite lifestyle adjustment and Despite lifestyle adjustment and Despite optimal medical therapy and Despite optimal medical therapy and Despite invasive coronary interventionsDespite invasive coronary interventions

ss
Algorithm to assess and treat refractory anginaAlgorithm to assess and treat refractory angina

Medical Therapy Commonly Prescribed forMedical Therapy Commonly Prescribed forAngina PectorisAngina Pectoris
Beta-blockers—decrease heart rate and contractilityBeta-blockers—decrease heart rate and contractility Calcium channel blockers—act as arterial vasodilator and decrease heart Calcium channel blockers—act as arterial vasodilator and decrease heart
rate and contractility.rate and contractility. Nitrates—act as venous and arterial vasodilatorNitrates—act as venous and arterial vasodilator Ranolazine- fRanolazine- fatty acid oxidation inhibition atty acid oxidation inhibition ,inhibition of the late Na+ flux.,inhibition of the late Na+ flux. Trimetazidine- metabolic modulationTrimetazidine- metabolic modulation Nicorandil- preconditioningNicorandil- preconditioning Fasudil- rhokinase inhibitionFasudil- rhokinase inhibition
Antiplatelet agents—for anti-inflammatory activityAntiplatelet agents—for anti-inflammatory activity
Angiotensin-converting enzyme inhibitors—improve endothelial function, and Angiotensin-converting enzyme inhibitors—improve endothelial function, and for anti-inflammatory activityfor anti-inflammatory activity
Statins—improve endothelial function, and for anti-inflammatory activityStatins—improve endothelial function, and for anti-inflammatory activity

Chronic ischemic heart disease: Treatment gapsChronic ischemic heart disease: Treatment gaps
Many patients have relative intolerances to maximum doses of traditional antianginal agents (-blockers, CCBs, and nitrates)
1 year after PCI or CABG 25% of patients still have anginaMany patients are deemed “inoperable”
Condition not suitable for PCI or CABGCo-morbidities make procedure too high risk
Patients continue to experience myocardial ischemia -blockers and many CCBs have similar depressive
hemodynamic and electrophysiologic effects

The most common reasons why further revascularization The most common reasons why further revascularization procedure is not possibleprocedure is not possible
Unsuitable anatomy, such as diffuse coronary sclerosisUnsuitable anatomy, such as diffuse coronary sclerosis One or several previous CABGs and/or PTCAs which exclude One or several previous CABGs and/or PTCAs which exclude
further benefit or possibility of further revascularization.further benefit or possibility of further revascularization. Lack of graft material.Lack of graft material. Impaired left ventricular function in patients with previous Impaired left ventricular function in patients with previous
CABG and/or PTCA.CABG and/or PTCA. Extracardiac diseases which increase perioperative/ Extracardiac diseases which increase perioperative/
postoperative morbidity or mortality, such as general postoperative morbidity or mortality, such as general arteriosclerotic disease, renal insufficiency, carotid stenosis and arteriosclerotic disease, renal insufficiency, carotid stenosis and pulmonary disease.pulmonary disease.
Age—often in combination with the above mentioned factors.Age—often in combination with the above mentioned factors.

Correlation - anxiety and ischaemic burdenCorrelation - anxiety and ischaemic burden
‘Angina is damaging my heart’
Restricted lifestyle Increasing anxiety, depressionReduced activity
DeconditioningWorseningsymptoms atlower thresholds
Cardicare
Angina Pectoris - Angina Pectoris - Understanding the options Understanding the options when Standard Therapy when Standard Therapy
FailsFails

CAD: Multiple treatment optionsCAD: Multiple treatment options
Reduce symptoms
Treat underlying
disease
PCI & CABG
Lifestyle intervention
Alternative TX
Medical
therapy

Current antianginal strategiesCurrent antianginal strategies
Current anti-anginal strategiesCurrent anti-anginal strategies
Non pharmacologic
Pharmacologic
TrimetazidineTrimetazidine
FasudilFasudil NicorandilNicorandil
IvabradineIvabradine
RanolazineRanolazine
EECPEECP
ChelationChelationtherapytherapy
SCSSCS
TMRTMR
Enhanced external Enhanced external counterpulsation (EECP)counterpulsation (EECP)
Transmyocardial Transmyocardial revascularizationrevascularization (surgical and (surgical and percutaneous)percutaneous)
Chelation therapyChelation therapy Spinal cord stimulation Spinal cord stimulation
(SCS)(SCS)
Therapeutic Options for Refractory Therapeutic Options for Refractory Angina PectorisAngina Pectoris
Coronary sinus reducerCoronary sinus reducer
Gene therapyGene therapy
Percutaneous in situ Percutaneous in situ coronary venous coronary venous arterializationarterialization
Heart transplantationHeart transplantation
Allen KB et al. N Engl J Med. 1999;341:1029-36. Bonetti PO et al. J Am Coll Cardiol. 2003;41:1918-
25. Murray S et al. Heart. 2000;83:217-20.

EECP - Enhanced External EECP - Enhanced External CounterPulsationCounterPulsation
It is a non invasive outpatient therapy consisting of ECG-gated It is a non invasive outpatient therapy consisting of ECG-gated sequential leg compression. sequential leg compression.
External, pneumatic compression of lower extremities in diastole.External, pneumatic compression of lower extremities in diastole.
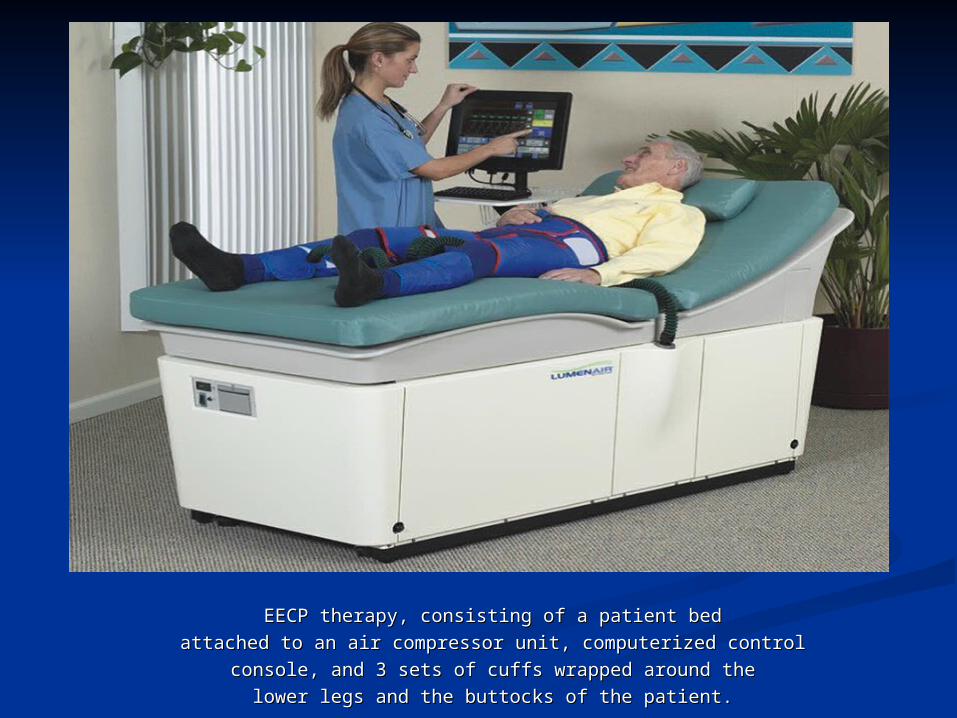
EECP therapy, consisting of a patient bedEECP therapy, consisting of a patient bed
attached to an air compressor unit, computerized controlattached to an air compressor unit, computerized control
console, and 3 sets of cuffs wrapped around theconsole, and 3 sets of cuffs wrapped around the
lower legs and the buttocks of the patient.lower legs and the buttocks of the patient.
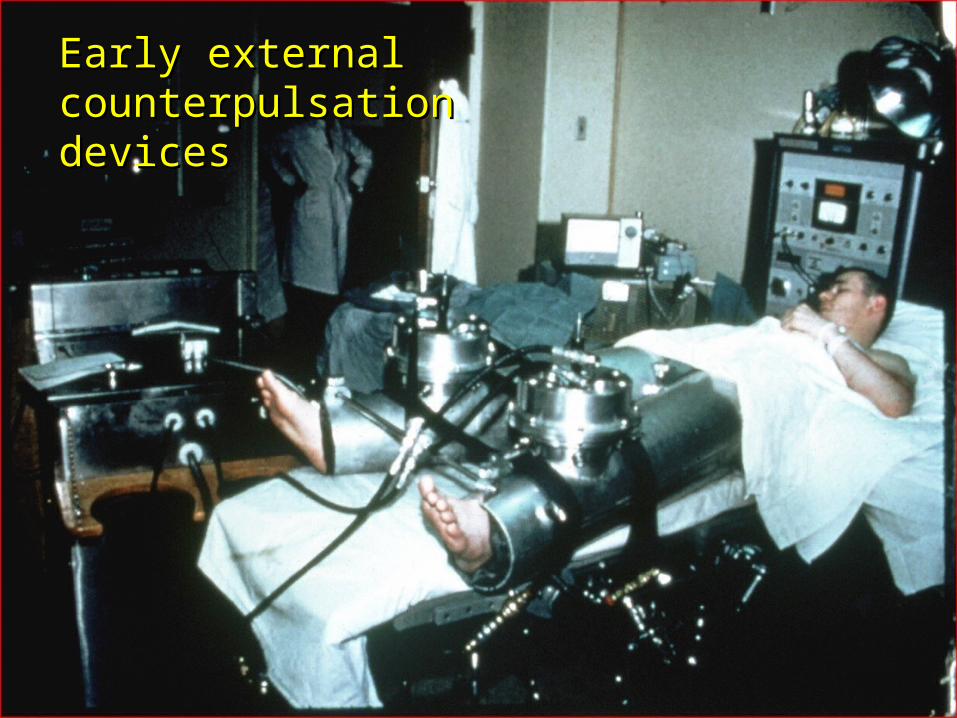
Early external Early external counterpulsation devicescounterpulsation devices

The history...The history...
Research in external counterpulsation goes back nearly 50 years, to 1953 when Research in external counterpulsation goes back nearly 50 years, to 1953 when the the Kantrowitz brothers Kantrowitz brothers described the concept of increased coronary artery blood described the concept of increased coronary artery blood flow and perfusion at higher pressure when blood pressure is raised during flow and perfusion at higher pressure when blood pressure is raised during diastole – this is diastole – this is diastolic augmentationdiastolic augmentation. .
Sarnoff and colleagues Sarnoff and colleagues showed that left ventricular work and myocardial oxygen showed that left ventricular work and myocardial oxygen consumption are more related to the pressure at which the left ventricle must consumption are more related to the pressure at which the left ventricle must work, than the volume of blood it pumps. Mechanical left work, than the volume of blood it pumps. Mechanical left ventricular unloadingventricular unloading, , therefore, reduces the heart’s energy requirements. therefore, reduces the heart’s energy requirements.
Birtwell Birtwell combined the combined the two principles two principles in a system that increased coronary in a system that increased coronary perfusion pressure in diastole and decreased left ventricular tension during perfusion pressure in diastole and decreased left ventricular tension during systole. systole.
GorlinGorlin named this process “ named this process “counterpulsation”. counterpulsation”. By the early 1960’s By the early 1960’s Birtwell and Soroff, Dennis, and Osborn Birtwell and Soroff, Dennis, and Osborn all independently all independently
developed hydraulic external counterpulsation systems. To create developed hydraulic external counterpulsation systems. To create counterpulsation, all these devices pumped water in and out of a single chamber counterpulsation, all these devices pumped water in and out of a single chamber enclosing the legs. They were used in all early U.S. clinical studies of external enclosing the legs. They were used in all early U.S. clinical studies of external counterpulsation. counterpulsation.

The EECP ProcedureThe EECP Procedure
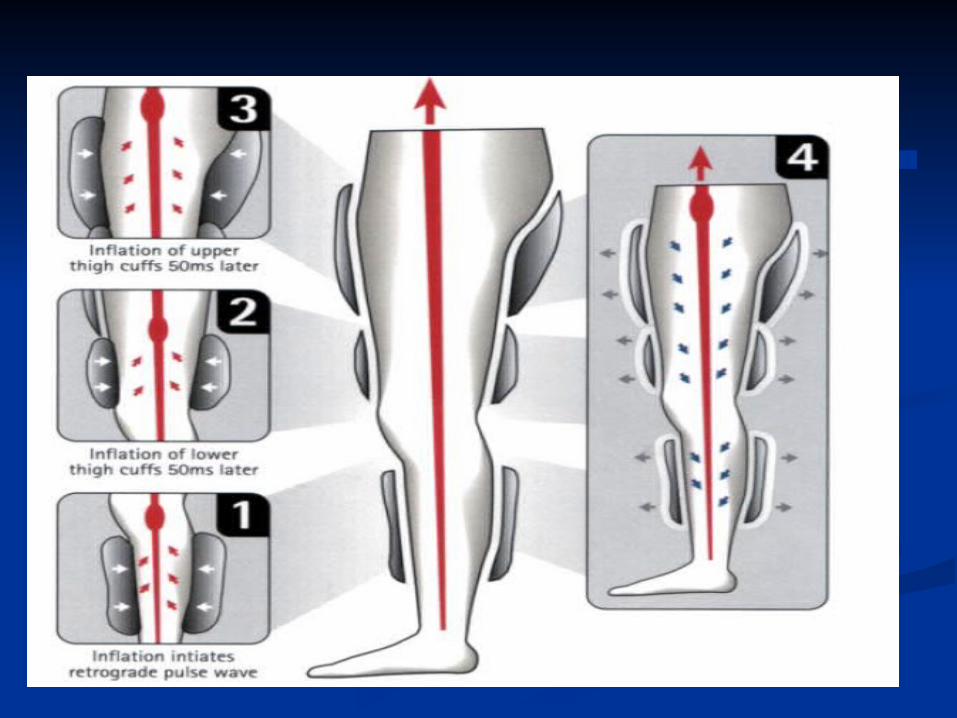
: • Series of 3 cuffs resembling oversized blood pressure cuffs wrapped around calves, lower thighs, upper thighs and buttocks
• The cuffs receive sequential distal-to-proximal pneumatic inflation upon onset of diastole.The compression of the lower extremity vascular bed increases diastolic pressure and flow and increases venous return.
• The pressure is then The pressure is then released at the onset of systole. released at the onset of systole. • Inflation and deflation are timed according to the R wave on Inflation and deflation are timed according to the R wave on
the patient’s cardiac monitor. the patient’s cardiac monitor. • The pressures applied and the inflation–deflation timing can The pressures applied and the inflation–deflation timing can
be altered by using the pressure waveforms and ECG on the be altered by using the pressure waveforms and ECG on the EECP therapy monitor.EECP therapy monitor.
• A finger plethysmogram is used throughout treatment to A finger plethysmogram is used throughout treatment to monitor diastolic and systolic pressure waveforms. monitor diastolic and systolic pressure waveforms.
• The current EECP device can generate external cuff The current EECP device can generate external cuff pressures as high as 220 to 300 mm Hg.pressures as high as 220 to 300 mm Hg.
Hemodynamic effects of EECP-:Hemodynamic effects of EECP-:
Increased Increased retrograde aortic blood flow; retrograde aortic blood flow; diastolic augmentation diastolic augmentation
to to increase coronary perfusion pressure increase coronary perfusion pressure and consequently, and consequently, coronary blood flow to ischemic regions.coronary blood flow to ischemic regions.
Increased Increased systolic unloading systolic unloading to decrease cardiac workload to decrease cardiac workload and myocardial oxygen demand.and myocardial oxygen demand.
Increased venous return Increased venous return to to raise cardiac outputraise cardiac output Improved left ventricular diastolic filling, peripheral flow-Improved left ventricular diastolic filling, peripheral flow-
mediated dilation, and endothelial function. mediated dilation, and endothelial function. Other putative mechanisms include recruitment of collaterals, Other putative mechanisms include recruitment of collaterals,
attenuation of oxidative stress and proinflammatory cytokines attenuation of oxidative stress and proinflammatory cytokines promotion of angiogenesis and vasculogenesis, and a promotion of angiogenesis and vasculogenesis, and a peripheral training effectperipheral training effect

Hemodynamic effects of EECP therapy. Right upper corner: showing the ECG tracing and finger Hemodynamic effects of EECP therapy. Right upper corner: showing the ECG tracing and finger pletysmogram. As soon as the device turned on (yellow line) diastolic augmentation starts. Right pletysmogram. As soon as the device turned on (yellow line) diastolic augmentation starts. Right
lower corner: showing the diastolic augmentation by echocardiography. a, aortic notch.lower corner: showing the diastolic augmentation by echocardiography. a, aortic notch.

Sequential Sequential inflation of inflation of
cuffscuffs Retrograde aortic Retrograde aortic
pressure wave pressure wave Increased Coronary Increased Coronary
perfusion pressureperfusion pressure Increased Venous Increased Venous
ReturnReturn Increased PreloadIncreased Preload Increased Cardiac Increased Cardiac
OutputOutput
Simultaneous Simultaneous deflation of deflation of cuffs in late cuffs in late
DiastoleDiastole Lowers Systemic Lowers Systemic
Vascular Resistance Vascular Resistance Reduced Preload Reduced Preload Decreased Cardiac Decreased Cardiac
workload workload Decreased Oxygen Decreased Oxygen
ConsumptionConsumption
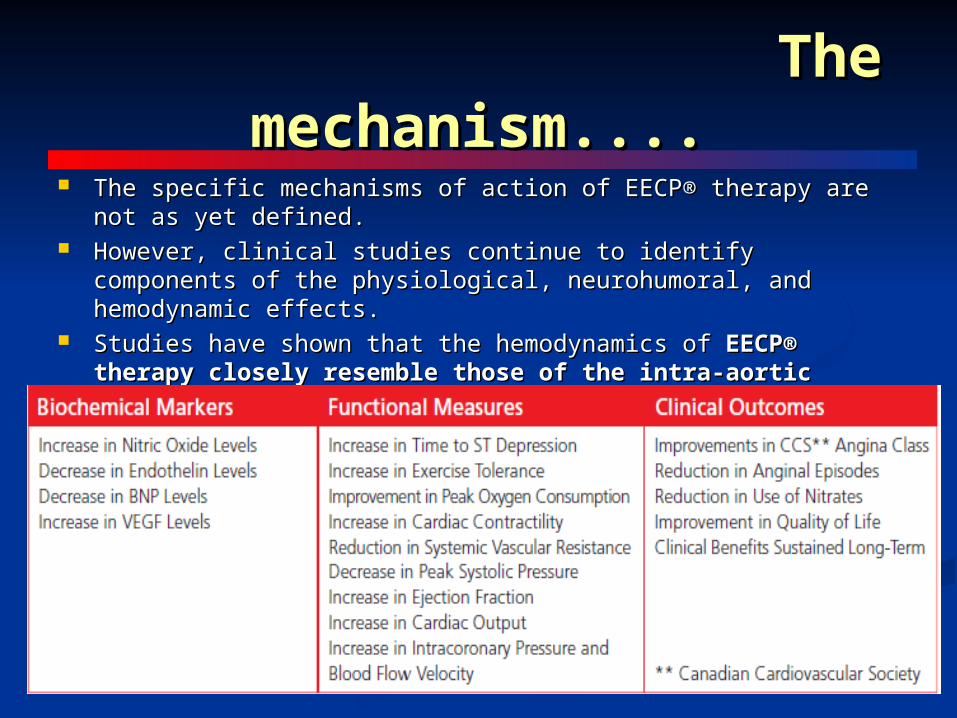
The mechanism....The mechanism.... The specific mechanisms of action of EECP® therapy are not as yet The specific mechanisms of action of EECP® therapy are not as yet
defined.defined. However, clinical studies continue to identify components of the However, clinical studies continue to identify components of the
physiological, neurohumoral, and hemodynamic effects.physiological, neurohumoral, and hemodynamic effects. Studies have shown that the hemodynamics of Studies have shown that the hemodynamics of EECP® therapy closely EECP® therapy closely
resemble those of the intra-aortic balloon pump (IABP).resemble those of the intra-aortic balloon pump (IABP).


BENEFITS....BENEFITS....
Significant benefits associated with EECP therapy include-Significant benefits associated with EECP therapy include- Angina reductionAngina reduction Improvement in quality of lifeImprovement in quality of life Prolongation of the time to exercise-induced ST-segment Prolongation of the time to exercise-induced ST-segment
depressiondepression Resolution of myocardial perfusion defectsResolution of myocardial perfusion defects Reduction of nitrate useReduction of nitrate use Reduction in hospitalizationReduction in hospitalization Low MACE rates at long-term follow-upLow MACE rates at long-term follow-up

35 hours total treatments35 hours total treatments 5 days per week x 7 weeks5 days per week x 7 weeks 1-2 hour per day1-2 hour per day 2 hours daily2 hours daily treatment sessions are separated by a treatment sessions are separated by a
30 minutes rest interval30 minutes rest interval Appears to reduce severity of Angina Appears to reduce severity of Angina Not shown to improve survivalNot shown to improve survival Indicated for CAD not amenable to Indicated for CAD not amenable to
revascularization revascularization Anatomy not amenable to proceduresAnatomy not amenable to procedures High risk co-morbidities with excessive riskHigh risk co-morbidities with excessive risk

Contraindications & PrecautionsContraindications & Precautions
Arrhythmias that interfere with machine triggeringArrhythmias that interfere with machine triggering Bleeding diathesisBleeding diathesis Active thrombophlebitis & severe lower extremity vaso-Active thrombophlebitis & severe lower extremity vaso-
occlusive diseaseocclusive disease Presence of significant AAAPresence of significant AAA(5 mm) or dissection(5 mm) or dissection PregnancyPregnancy Decompensated heart failureDecompensated heart failure Severe aortic regurgitationSevere aortic regurgitation Severe hypertension: greater than 180/ 110 mm HgSevere hypertension: greater than 180/ 110 mm Hg Severe chronic obstructive pulmonary diseaseSevere chronic obstructive pulmonary disease

Side effectsSide effects
ParesthesiasParesthesias Skin abrasion or ecchymosesSkin abrasion or ecchymoses BruisesBruises Worsening of heart failure in patients with Worsening of heart failure in patients with
arrhythmiasarrhythmias Leg or waist pain, Leg or waist pain, OedemaOedema

SUNY Stony Brook: The first publication - SUNY Stony Brook: The first publication - 19921992
Background:Background: Of 18 patients with chronic angina refractory to medical therapy: Of 18 patients with chronic angina refractory to medical therapy: - 8 had 19 prior revascularization attempts - 8 had 19 prior revascularization attempts - 7 had 14 prior mycardial infarcts- 7 had 14 prior mycardial infarcts
Methods:Methods: 36 one-hour treatment sessions36 one-hour treatment sessions
Pre- and post-treatment thallium treadmill stress tests to Pre- and post-treatment thallium treadmill stress tests to
identical exercise timesidentical exercise times
Separate post-treatment maximal routine treadmill stress testSeparate post-treatment maximal routine treadmill stress test
Results:Results: All patients reported improvement in anginal symptoms:All patients reported improvement in anginal symptoms:
- 16 patients (- 16 patients (89%89%) reported no angina during usual activities:) reported no angina during usual activities:
- 12 patients (- 12 patients (67%67%) with resolution of reversible perfusion defects) with resolution of reversible perfusion defects
- 2 patients (- 2 patients (11%11%) with improvement of reversible perfusion defects ) with improvement of reversible perfusion defects
- 4 patients ( - 4 patients (22%22%) with no change) with no change
Lawson WE, Hui JCK, Soroff HS, et al. Efficacy of enhanced external counterpulsation in the treatmentLawson WE, Hui JCK, Soroff HS, et al. Efficacy of enhanced external counterpulsation in the treatmentof angina pectoris. of angina pectoris. Am J Cardiol. Am J Cardiol. 1992;70:859-862.1992;70:859-862.

SUNY Stony Brook: 5-year Follow-upSUNY Stony Brook: 5-year Follow-up
Background:Background: A five-year follow-up was conducted on 33 angina A five-year follow-up was conducted on 33 angina patients treated between 1989 and 1992 with EECP, patients treated between 1989 and 1992 with EECP, to assess morbidity and mortality.to assess morbidity and mortality.
Methods:Methods: Review of patient records at 5 years post-EECP Review of patient records at 5 years post-EECP (range 4-7 years).(range 4-7 years).
Results:Results: 29 of 33 patients remained alive. Of these, 9 patients 29 of 33 patients remained alive. Of these, 9 patients were hospitalized (4 acute MI, 6 CABG/PTCA, were hospitalized (4 acute MI, 6 CABG/PTCA, 1 unstable angina and 1 other cardiac surgery).1 unstable angina and 1 other cardiac surgery).
Conclusions:Conclusions: Five-year survival without an interim event of 60% of patients treated with EECP Five-year survival without an interim event of 60% of patients treated with EECP
appears similar to that seen with comparable populations treated with appears similar to that seen with comparable populations treated with CABG/PTCA. CABG/PTCA.
Lawson WE, Hui JCK, Burger L, et al. Five-year follow-up of morbidity and mortality in 33 angina patient Lawson WE, Hui JCK, Burger L, et al. Five-year follow-up of morbidity and mortality in 33 angina patient treated with enhanced external counterpulsation. treated with enhanced external counterpulsation. J Invest Med. J Invest Med. 1997;45:212A.1997;45:212A.

The Multicenter Study of Enhanced External The Multicenter Study of Enhanced External Counterpulsation (MUST-EECP)Counterpulsation (MUST-EECP)
Design:Design: Multicenter, randomized, sham-controlled, double-blinded trialMulticenter, randomized, sham-controlled, double-blinded trial
Randomization:Randomization: Even assignment to EECP group or sham group in blocks of 10 Even assignment to EECP group or sham group in blocks of 10
allocated to each centerallocated to each center
Subjects:Subjects: 139 patients with chronic stable angina pectoris 139 patients with chronic stable angina pectoris
Duration: Duration: May 1995 - July 1997May 1995 - July 1997
Evaluate effect Evaluate effect of EECP on...of EECP on... Measured by…Measured by…
Exercise abilityExercise ability Exercise durationExercise durationTime to ST-Time to ST-
segment depressionsegment depression
Clinical statusClinical status Frequency of anginal episodesFrequency of anginal episodesIntake of nitroglycerinIntake of nitroglycerin

MUST-EECP:Exercise MUST-EECP:Exercise ResultsResults
37-4
4226
-10 0 10 20 30 40 50
Time to STDepression
ExerciseDuration
Active Sham
Seconds
Adjusted mean of change from baseline
p = ns
p = 0.01
}
}

Summary of Clinical ResultsSummary of Clinical Results
Compared to sham, EECP:Compared to sham, EECP: Increased time to exercise-induced ST segment depression (Increased time to exercise-induced ST segment depression (pp= 0.01)= 0.01) Decreased the frequency of angina episodes (Decreased the frequency of angina episodes (pp< 0.04)< 0.04)
Compared to baseline:Compared to baseline: Exercise duration increased significantly in both groupsExercise duration increased significantly in both groups
(Sham- p<0.03, Active- p< 0.001)(Sham- p<0.03, Active- p< 0.001) Time to ST segment depression increased significantly in Active Group Time to ST segment depression increased significantly in Active Group
only (p< 0.002)only (p< 0.002) EECP is a safe and effective treatment for angina pectoris refractory to medical therapyEECP is a safe and effective treatment for angina pectoris refractory to medical therapy
Benefits of EECP include an improvement of functional status in more than 70% of Benefits of EECP include an improvement of functional status in more than 70% of patientspatients
Benefits accrue both short-term and long-termBenefits accrue both short-term and long-term
In a meta-analysis of 13 observational studies that tracked 949 patients, CCS In a meta-analysis of 13 observational studies that tracked 949 patients, CCS anginal class was improved by ≥1 class in 86% of EECP-treated patients.anginal class was improved by ≥1 class in 86% of EECP-treated patients.**
The EECP The EECP Consortium reported results from 2289 consecutive patients Consortium reported results from 2289 consecutive patients undergoing EECP therapy treatment was associated with improved perfusion undergoing EECP therapy treatment was associated with improved perfusion images and increased exercise duration. **images and increased exercise duration. **
Similarly, the International EECP Registry reported improvement of ≥1 CCS Similarly, the International EECP Registry reported improvement of ≥1 CCS angina class in 81% of patients after EECP.***angina class in 81% of patients after EECP.***
Moreover, follow-up data indicate that the clinical benefit may be maintained Moreover, follow-up data indicate that the clinical benefit may be maintained for up to 5 years in patients with a favorable initial clinical responsefor up to 5 years in patients with a favorable initial clinical response
**Daemen J, Boersma E, Flather M, et al. Long-term safety and efficacy of percutaneous coronary intervention with stenting and coronary artery Daemen J, Boersma E, Flather M, et al. Long-term safety and efficacy of percutaneous coronary intervention with stenting and coronary artery bypass surgery for multivessel coronary artery disease: a meta-analysis with 5-year patient-level data from the ARTS, ERACI-II, MASS-II, bypass surgery for multivessel coronary artery disease: a meta-analysis with 5-year patient-level data from the ARTS, ERACI-II, MASS-II, and SoS trials. Circulation. 2008;118:1146-54.and SoS trials. Circulation. 2008;118:1146-54.
** Rodriguez A, Rodriguez AM, Baldi J, et al. Coronary stenting versus coronary bypass surgery in patients with multiple vessel disease and ** Rodriguez A, Rodriguez AM, Baldi J, et al. Coronary stenting versus coronary bypass surgery in patients with multiple vessel disease and significant proximal LAD stenosis: results from the ERACI II study. Heart. 2003;89:184-8.significant proximal LAD stenosis: results from the ERACI II study. Heart. 2003;89:184-8.
*** Mercado N, Maier W, Boersma E, et al. Clinical and angiographic outcome of patients with mild coronary lesions treated with balloon angioplasty *** Mercado N, Maier W, Boersma E, et al. Clinical and angiographic outcome of patients with mild coronary lesions treated with balloon angioplasty or coronary stenting. Implications for mechanical plaque sealing. Eur Heart J. 2003;24:541-51or coronary stenting. Implications for mechanical plaque sealing. Eur Heart J. 2003;24:541-51

The Food & Drug Administration (FDA) has approved EECP® for The Food & Drug Administration (FDA) has approved EECP® for treatment of treatment of cardiovascular disease:cardiovascular disease:
In the In the 1970s, EECP® was first approved for cardiogenic shock1970s, EECP® was first approved for cardiogenic shock and and acute myocardial infarction .acute myocardial infarction .
EECP was approved by the US Food and Drug Administration in 1995 for EECP was approved by the US Food and Drug Administration in 1995 for the treatment of patients with CAD and refractory angina pectoris who fail to the treatment of patients with CAD and refractory angina pectoris who fail to respond to standard revascularization procedures and aggressive respond to standard revascularization procedures and aggressive pharmacotherapy.pharmacotherapy.
In June In June 2002, EECP® was approved for congestive heart 2002, EECP® was approved for congestive heart failure failure

TMLR - Transmyocardial Laser TMLR - Transmyocardial Laser RevascularizationRevascularization
High power CO2 YAG and excimer laser High power CO2 YAG and excimer laser
conduits in myocardial to create new channels conduits in myocardial to create new channels
for blood flowfor blood flow
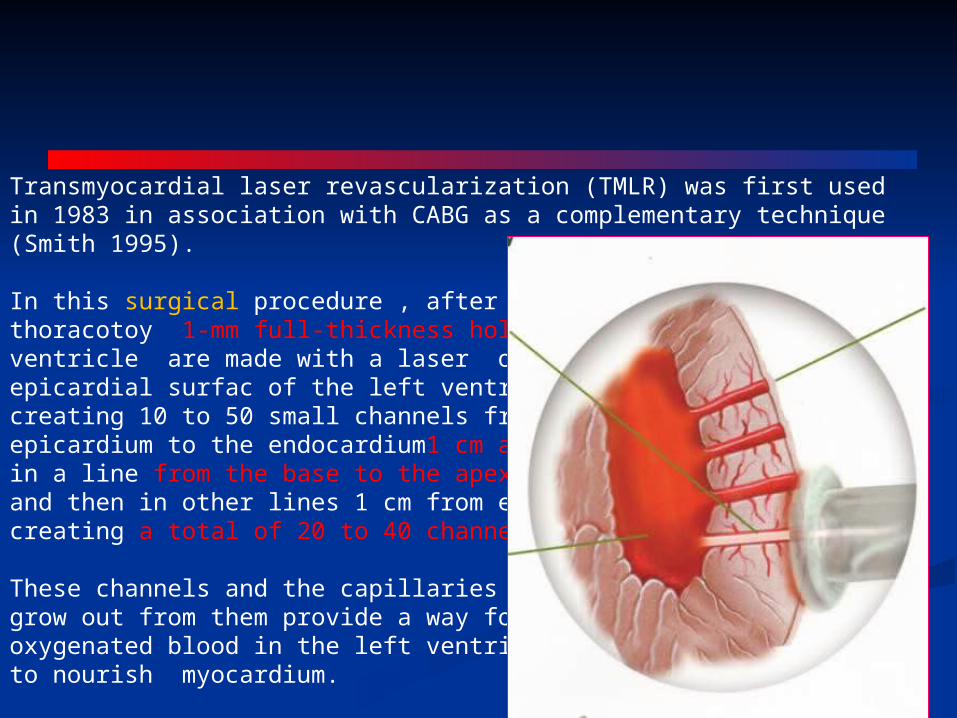
Transmyocardial laser revascularization (TMLR) was first usedin 1983 in association with CABG as a complementary technique(Smith 1995).
In this surgical procedure , after left lateralthoracotoy 1-mm full-thickness holes through the left ventricle are made with a laser on the epicardial surfac of the left ventricle, creating 10 to 50 small channels from theepicardium to the endocardium1 cm apart in a line from the base to the apex, and then in other lines 1 cm from each other, creating a total of 20 to 40 channels.
These channels and the capillaries that grow out from them provide a way for oxygenated blood in the left ventricle to nourish myocardium.
The epicardial channel opening usually closes spontaneously The epicardial channel opening usually closes spontaneously and mimic the sinusoids in a reptile’s heart, which has no and mimic the sinusoids in a reptile’s heart, which has no coronary arteries.coronary arteries.
20 percent of these remain patent; and new capillaries 20 percent of these remain patent; and new capillaries 0.1 to .3 mm in diameter, lined with 0.1 to .3 mm in diameter, lined with endothelium, extend out into the myocardium from endothelium, extend out into the myocardium from the channels. the channels.
The laser is triggered to fire on the R wave of the The laser is triggered to fire on the R wave of the electrocardiogram when the ventricle is in diastole, maximally electrocardiogram when the ventricle is in diastole, maximally distended and electrically quiescent. Synchronization of the distended and electrically quiescent. Synchronization of the very brief laser pulse to the R wave of the electrocardiogram very brief laser pulse to the R wave of the electrocardiogram reduces the risk of arrhythmia. reduces the risk of arrhythmia.

Biologic Plausibility of TMRBiologic Plausibility of TMR• MyocardialMyocardial DenervationDenervation
– Mylenated fiberMylenated fiber– Sympathetic fibersSympathetic fibers
• Endocardial channelsEndocardial channels– 20 % stay remain patent20 % stay remain patent
• Neoangiogenesis from channelsNeoangiogenesis from channels– New capillaries 0.1-0.3 diameter New capillaries 0.1-0.3 diameter
with endothelium with endothelium
formation of new capillaries from pre-existing formation of new capillaries from pre-existing ones (angiogenesis) or by the enlargement and ones (angiogenesis) or by the enlargement and functional recruitment of pre-existing collateral functional recruitment of pre-existing collateral
vessels (arteriogenesis)vessels (arteriogenesis)
COCO2 2 Laser Laser
Full-thickness 1 mm Full-thickness 1 mm channel created with a 20 channel created with a 20 joules single pulse. joules single pulse.

Relief of angina does not simply result from denervation because the Relief of angina does not simply result from denervation because the benefits of TMR extend out to 5 years, beyond the time when the nerves benefits of TMR extend out to 5 years, beyond the time when the nerves would have grown back. would have grown back.
Its beneficial effect is a consequence of neoangiogenesis, resulting in Its beneficial effect is a consequence of neoangiogenesis, resulting in improved myocardial blood flow.improved myocardial blood flow.
Patients with poor left ventricular ejection fraction are not good Patients with poor left ventricular ejection fraction are not good candidates for laser therapy.candidates for laser therapy.

Possible perioperative and postoperative complications encompass Possible perioperative and postoperative complications encompass ––
mortality rates range from 5–20% and the perioperative morbidity mortality rates range from 5–20% and the perioperative morbidity has been between 32 and 68% in different studieshas been between 32 and 68% in different studies
myocardial infarctionmyocardial infarction low output syndromelow output syndrome ventricular arrhythmias, atrial fibrillationventricular arrhythmias, atrial fibrillation sudden development of mitral regurgitation as a result of laser sudden development of mitral regurgitation as a result of laser
injury to the chordae tendineaeinjury to the chordae tendineae bleedingbleeding postoperative complications, such as wound infection or postoperative complications, such as wound infection or
pneumonia.pneumonia.

A single randomized multicenter comparison of TMR A single randomized multicenter comparison of TMR (with a holmium:YAG laser) plus CABG versus CABG (with a holmium:YAG laser) plus CABG versus CABG alone in patients in whom some myocardial segments alone in patients in whom some myocardial segments were perfused by arteries considered not amenable to were perfused by arteries considered not amenable to grafting showed a significant reduction in perioperative grafting showed a significant reduction in perioperative mortality (1.5% vs 7.6%, respectively), with the survival mortality (1.5% vs 7.6%, respectively), with the survival benefit of the TMR–CABG combination present after 1 benefit of the TMR–CABG combination present after 1 year of follow-up.*year of follow-up.*
* Allen KB, Dowling RD, DelRossi AJ, et al. Transmyocardial laser revascularization combined with coronary artery bypass grafting: a * Allen KB, Dowling RD, DelRossi AJ, et al. Transmyocardial laser revascularization combined with coronary artery bypass grafting: a multicenter, blinded, prospective, randomized, controlled trial. J Thorac Cardiovasc Surg 2000;119:540–9multicenter, blinded, prospective, randomized, controlled trial. J Thorac Cardiovasc Surg 2000;119:540–9..

PERCUTANEOUS PERCUTANEOUS TRANSMYOCARDIAL LASERTRANSMYOCARDIAL LASERREVASCULARIZATIONREVASCULARIZATION
TMR has also been performed percutaneously, using a TMR has also been performed percutaneously, using a less-invasive catheter-based approach that is referred to as less-invasive catheter-based approach that is referred to as PTMLR. PTMLR.
A catheter laser fiberoptic system is introduced through the A catheter laser fiberoptic system is introduced through the femoral artery and through the aortic valve into the left femoral artery and through the aortic valve into the left ventricle. The laser-made channels in the myocardium are ventricle. The laser-made channels in the myocardium are created from the endocardium towards the epicardium created from the endocardium towards the epicardium guided by fluoroscopy and simultaneous transoesophageal guided by fluoroscopy and simultaneous transoesophageal echocardiographic monitoring. echocardiographic monitoring.
Injury to the epicardial coronary artery, chordae tendineae, Injury to the epicardial coronary artery, chordae tendineae, bleeding into the pericardial sac and neurological bleeding into the pericardial sac and neurological complications are possible.complications are possible.

The mortality rate is estimated to 1%.The mortality rate is estimated to 1%. Further scientific data are needed before the role of Further scientific data are needed before the role of
percutaneous laser revascularization in the therapeutic arsenal percutaneous laser revascularization in the therapeutic arsenal can be determined.can be determined.
The Potential Angina Class Improvement From Intramyocardial The Potential Angina Class Improvement From Intramyocardial Channels (PACIFIC) trial was a multicenter, randomized study Channels (PACIFIC) trial was a multicenter, randomized study comparing PTMLR in addition to medical therapy with medical comparing PTMLR in addition to medical therapy with medical therapy alone in patients with CCS class III or IV RAP. At 12 therapy alone in patients with CCS class III or IV RAP. At 12 months, exercise tolerance significantly increased in the PTMLR months, exercise tolerance significantly increased in the PTMLR group, as did anginal class scores and quality-of-life group, as did anginal class scores and quality-of-life measurements. There was no significant difference, however, in measurements. There was no significant difference, however, in overall mortalityoverall mortality
Oesterle SN, Sanborn TA, Ali N, et al. Percutaneous transmyocardial laser revascularisation for severe angina: the PACIFIC randomised trial. Potential class Oesterle SN, Sanborn TA, Ali N, et al. Percutaneous transmyocardial laser revascularisation for severe angina: the PACIFIC randomised trial. Potential class improvement from Intramyocardial channels. Lancet 2000;356:1705–10.improvement from Intramyocardial channels. Lancet 2000;356:1705–10.

DIRET TRIALDIRET TRIALStone GW, Teirstein PS, Rubenstein R, et al. A prospective, multicenter, randomized trial ofStone GW, Teirstein PS, Rubenstein R, et al. A prospective, multicenter, randomized trial of
percutaneous transmyocardial laser revascularization in patients with nonrecanalizable chronic total occlusions. J Am Coll Cardiol percutaneous transmyocardial laser revascularization in patients with nonrecanalizable chronic total occlusions. J Am Coll Cardiol
2002;39:1581–72002;39:1581–7. . Leon M. DIRECT trial: Late breaking trials. Presentedat: Transcatheter Therapeutics. Washington,DC, October 20, Leon M. DIRECT trial: Late breaking trials. Presentedat: Transcatheter Therapeutics. Washington,DC, October 20,
2000. 2000.
The results of the direct myocardial revascularization in the The results of the direct myocardial revascularization in the Regeneration of Endomyocardial Channels Trial (DIRECT) Regeneration of Endomyocardial Channels Trial (DIRECT) tempered the initial enthusiasm surrounding PTMLR. tempered the initial enthusiasm surrounding PTMLR.
This randomized, placebo-controlled, prospective trial enrolled 298 This randomized, placebo-controlled, prospective trial enrolled 298 patients into 3 treatment arms: placebo PTMLR procedure, low-patients into 3 treatment arms: placebo PTMLR procedure, low-dose PTMLR (10–15 channels created), or high-dose PTMLR (20–dose PTMLR (10–15 channels created), or high-dose PTMLR (20–25 channels created). 25 channels created).
The results were similar for treatment arms, representing a large The results were similar for treatment arms, representing a large placebo effect.placebo effect.
It demonstrated no therapeutic benefitIt demonstrated no therapeutic benefit on patient survival angina on patient survival angina class, Quality of life ,exercise durationclass, Quality of life ,exercise duration and this therapy was thus and this therapy was thus promptly abandoned.promptly abandoned.
TMR and PTMLR have been recently evaluated by TMR and PTMLR have been recently evaluated by Schofield and McNab.Although there was an Schofield and McNab.Although there was an improvement in the more subjective outcome measures improvement in the more subjective outcome measures (including exercise tolerance testing, angina score, and (including exercise tolerance testing, angina score, and quality of life), this was counterbalanced by a higher risk quality of life), this was counterbalanced by a higher risk of postoperative mortality(5%) and morbidity (including of postoperative mortality(5%) and morbidity (including MI, heart failure, thromboembolic events, pericarditis, MI, heart failure, thromboembolic events, pericarditis, acute mitral insufficiency, and neurologic events).*acute mitral insufficiency, and neurologic events).*
Mainly used as adjunct therapy during CABG to treat Mainly used as adjunct therapy during CABG to treat myocardial that cannot be bypassed.myocardial that cannot be bypassed.
Class llb indication in ACC/AHA 2012 CAD guidelinesClass llb indication in ACC/AHA 2012 CAD guidelines
* Schofield PM, McNab D. NICE evaluation of transmyocardial laser revascularization and percutaneous laser revascularisation for refractory * Schofield PM, McNab D. NICE evaluation of transmyocardial laser revascularization and percutaneous laser revascularisation for refractory angina. Heart 2010;96:312–3.angina. Heart 2010;96:312–3.

CHELATION THERAPYCHELATION THERAPY
It was first proposed as a potential treatment for It was first proposed as a potential treatment for atherosclerosis in the 1950s, after it was noted that atherosclerosis in the 1950s, after it was noted that patients treated for lead poisoning felt relief of their patients treated for lead poisoning felt relief of their anginal symptoms after undergoing ethylenediamine-anginal symptoms after undergoing ethylenediamine-tetraacetic acid (EDTA) therapy.tetraacetic acid (EDTA) therapy.
Since then, various small, uncontrolled studies have been Since then, various small, uncontrolled studies have been published, with conflicting results.published, with conflicting results.
It consists of a series of intravenous infusions of EDTA in It consists of a series of intravenous infusions of EDTA in combination with other substances, has been touted as a combination with other substances, has been touted as a putative noninvasive means of improving blood flow in putative noninvasive means of improving blood flow in atherosclerotic vessels, treating angina, and preventing atherosclerotic vessels, treating angina, and preventing cardiac events.cardiac events.
The hypothesis for atherosclerosis regression involves the The hypothesis for atherosclerosis regression involves the ability of EDTA to extract calcium from the atherosclerotic ability of EDTA to extract calcium from the atherosclerotic plaque. This hypothesis has never been scientifically plaque. This hypothesis has never been scientifically validated and, in fact, is no longer applicable.validated and, in fact, is no longer applicable.
Probable mechanism include EDTA reduces oxidative stress Probable mechanism include EDTA reduces oxidative stress in the vascular wall, in the vascular wall, lowers LDL, VLDL, and Iron stores, lowers LDL, VLDL, and Iron stores, inhibits platelet aggregation and relaxes vasomotor tone.inhibits platelet aggregation and relaxes vasomotor tone.
Consist of 30 treatments over about 3 monthsConsist of 30 treatments over about 3 months Program to assess Alternative Treatment strategies to achieve Cardiac Program to assess Alternative Treatment strategies to achieve Cardiac
Health (PATCH) trial showed the ineffectiveness of chelation therapy . Health (PATCH) trial showed the ineffectiveness of chelation therapy .
Knudson ML, Wyse DG, Gailbraith PD, et al. Chelation therapy for ischemic heart disease: a randomized controlled trial. JAMA 2002; 287:481–6Knudson ML, Wyse DG, Gailbraith PD, et al. Chelation therapy for ischemic heart disease: a randomized controlled trial. JAMA 2002; 287:481–6

TACT (Trial to Assess Chelation Therapy) TACT (Trial to Assess Chelation Therapy) Lamas GA, Goertz C, Boineau R, et al. Effect of disodium EDTA chelationLamas GA, Goertz C, Boineau R, et al. Effect of disodium EDTA chelation
regimen on cardiovascular events in patients with previous myocardial infarction: the TACT randomized trial. JAMA. 2013;309:1241–regimen on cardiovascular events in patients with previous myocardial infarction: the TACT randomized trial. JAMA. 2013;309:1241–
5050.. RCT comparing chelation with placebo in patients who had RCT comparing chelation with placebo in patients who had
experienced MI. experienced MI. The primary composite endpoint of total mortality, recurrent The primary composite endpoint of total mortality, recurrent
MI, stroke, coronary revascularization, or hospitalization for MI, stroke, coronary revascularization, or hospitalization for angina occurred in 222 (26%) patients in the chelation group angina occurred in 222 (26%) patients in the chelation group and 261 (30%) patients in the placebo group (hazard ratio: and 261 (30%) patients in the placebo group (hazard ratio: 0.82; 95% CI: 0.69 to 0.99; 0.82; 95% CI: 0.69 to 0.99; P=0.035P=0.035
Disodium EDTA, particularly when infused too rapidly, may Disodium EDTA, particularly when infused too rapidly, may cause hypocalcemia, renal failure, and death.cause hypocalcemia, renal failure, and death.

Despite these positive findings, the TACT investigators Despite these positive findings, the TACT investigators did not recommend the routine use of chelation therapy did not recommend the routine use of chelation therapy to reduce symptoms or cardiovascular complications for to reduce symptoms or cardiovascular complications for all patients with SIHD, given the modest overall benefit, all patients with SIHD, given the modest overall benefit, high proportion of patient withdrawals (18% lost to high proportion of patient withdrawals (18% lost to follow-up), absence of adequate scientific basis for the follow-up), absence of adequate scientific basis for the therapy.therapy.
Changed from class lll to class llb in 2014 SIHD focused Changed from class lll to class llb in 2014 SIHD focused update.update.

NeurostimulationNeurostimulation It is for the palliation of angina by interruption or modification of the afferent It is for the palliation of angina by interruption or modification of the afferent
neural signals through which pain is perceived. neural signals through which pain is perceived. Different surgical techniques have been used to interrupt the innervation of Different surgical techniques have been used to interrupt the innervation of
the heart, including autotransplantation, sympathectomy and plexectomy.the heart, including autotransplantation, sympathectomy and plexectomy. More recent studies using transcutaneous electrical nerve stimulation More recent studies using transcutaneous electrical nerve stimulation
(TENS) and spinal cord stimulation (SCS) have produced the most (TENS) and spinal cord stimulation (SCS) have produced the most promising results.promising results.
Mannheimer first described the beneficial effects of TENS in early 1980s.Mannheimer first described the beneficial effects of TENS in early 1980s. In TENS, two electrodes are applied to the chest—one in the dermatome In TENS, two electrodes are applied to the chest—one in the dermatome
with the highest intensity of projected pain and the other in the contralateral with the highest intensity of projected pain and the other in the contralateral dermatome. The stimulus intensity is adjusted to just below the individual’s dermatome. The stimulus intensity is adjusted to just below the individual’s pain threshold.pain threshold.
They act by reducing the activation of central pain receptors. In addition, They act by reducing the activation of central pain receptors. In addition, there is a reduction in sympathetic discharge, leading to a decrease in there is a reduction in sympathetic discharge, leading to a decrease in cardiac work load and myocardial oxygen demand.cardiac work load and myocardial oxygen demand.

SPINAL CORD STIMULATIONSPINAL CORD STIMULATION
power source conducting wires electrodes atstimulation site
Stimulation typicallyadministered for 1-2 hrs tid
Therapeutic mechanism appears to be alteration of anginal pain perception

Spinal cord stimulation appears to be the most promising Spinal cord stimulation appears to be the most promising neurostimulatory technique for refractory angina. neurostimulatory technique for refractory angina.
It is performed under local anaesthesia. In SCS, the epidural It is performed under local anaesthesia. In SCS, the epidural space is punctured at the level of the fourth or sixth thoracic space is punctured at the level of the fourth or sixth thoracic vertebra, and Tuohy-type needle was advanced in the midline vertebra, and Tuohy-type needle was advanced in the midline through the intervertebral spaces into the epidural space an through the intervertebral spaces into the epidural space an electrode is introduced to the level of the first or second electrode is introduced to the level of the first or second thoracic vertebra. thoracic vertebra.
An electrode stimulator is then placed subcutaneously in the An electrode stimulator is then placed subcutaneously in the upper left abdomen. upper left abdomen.
The device has an epidural lead, extension wire, and pulse The device has an epidural lead, extension wire, and pulse generator. generator.

An extension lead is tunneled subcutaneously to the An extension lead is tunneled subcutaneously to the midline incision and connected to the electrode.midline incision and connected to the electrode.
The pulse generator is telemetrically programmed .The pulse generator is telemetrically programmed . The pulse generator is turned on or off when the patient The pulse generator is turned on or off when the patient
quickly touches the skin over the pulse generator with an quickly touches the skin over the pulse generator with an external magnet. external magnet.
It is used for at least 2 hours four times daily.It is used for at least 2 hours four times daily. The patient can also use the magnet to switch between The patient can also use the magnet to switch between
the two preset stimulation strengths.the two preset stimulation strengths.

Angina pectoris often results from ischemic episodes that excite chemosensitive Angina pectoris often results from ischemic episodes that excite chemosensitive and mechanoreceptive receptors in the heart.and mechanoreceptive receptors in the heart.
Ischemic episodes release a collage of chemicals, including adenosine and Ischemic episodes release a collage of chemicals, including adenosine and bradykinin, that excites the receptors of the sympathetic and vagal afferent bradykinin, that excites the receptors of the sympathetic and vagal afferent pathways. pathways.
Sympathetic afferent fibers from the heart enter the upper thoracic spinal cord Sympathetic afferent fibers from the heart enter the upper thoracic spinal cord and synapse on cells of origin of ascending pathways. Excitation of and synapse on cells of origin of ascending pathways. Excitation of spinothalamic tract cells in the upper thoracic and lower cervical segments, spinothalamic tract cells in the upper thoracic and lower cervical segments, contributes to the anginal pain experienced in the chest and arm.contributes to the anginal pain experienced in the chest and arm.
Cardiac vagal afferent fibers synapse in the nucleus tractus solitarius of the Cardiac vagal afferent fibers synapse in the nucleus tractus solitarius of the medulla and then descend to excite upper cervical spinothalamic tract cells. This medulla and then descend to excite upper cervical spinothalamic tract cells. This innervation contributes to the anginal pain experienced in the neck and jaw. innervation contributes to the anginal pain experienced in the neck and jaw.
The spinothalamic tract projects to the medial and lateral thalamus and, activates The spinothalamic tract projects to the medial and lateral thalamus and, activates several cortical areas, including the anterior cingulate gyrus, lateral basal frontal several cortical areas, including the anterior cingulate gyrus, lateral basal frontal cortex, and the mesiofrontal cortex.cortex, and the mesiofrontal cortex.
Mechanism of action -both an Mechanism of action -both an antalgic effectantalgic effect, mainly due to , mainly due to modulation of pain signal in the spinal cord and change in modulation of pain signal in the spinal cord and change in metabolism of beta-endorphine .metabolism of beta-endorphine .
antiischemic effect antiischemic effect expressed by decrease in the serum expressed by decrease in the serum catecholamine level, exerted by reducing sympathetic tone catecholamine level, exerted by reducing sympathetic tone leading to decrease in myocardial oxygen consumption at a leading to decrease in myocardial oxygen consumption at a comparable level of cardiac work. Redistribution of blood from comparable level of cardiac work. Redistribution of blood from non-ischaemic to ischaemic areas is also proposed.non-ischaemic to ischaemic areas is also proposed.
The effect of transcutaneous electrical nerve stimulation (TENS) The effect of transcutaneous electrical nerve stimulation (TENS) on coronary flow was not accomplished in patients with a heart on coronary flow was not accomplished in patients with a heart transplant which suggests that neurostimulation employs its effect transplant which suggests that neurostimulation employs its effect through neural mechanisms employed at the microcirculatory through neural mechanisms employed at the microcirculatory level.level.
Contraindications to this therapy include,Contraindications to this therapy include, Unstable anginaUnstable angina Unfavorable physical conditionUnfavorable physical condition Cardiac pacemaker or ICDCardiac pacemaker or ICD Lack of patient complianceLack of patient compliance Obvious infection, allergic or immune response Obvious infection, allergic or immune response
to implanted materialsto implanted materials Anticoagulation that might increase bleeding at Anticoagulation that might increase bleeding at
the implantation site.the implantation site.


Randomized Trial of SCS vs. CABG For Patients with Randomized Trial of SCS vs. CABG For Patients with Refractory AnginaRefractory Angina
14.6 15.216.2
13.7
4.4 4.15.2
3.1
02468
1012141618
Anginal attacks NTGconsumption
Anginal attacks NTGconsumption
Mean number
perweek
Baseline
6 months
Spinal cord stimulation (n=53) CABG (n=51)
*P < 0.0001
****
(Mannheimer, et al. Circulation 1998;97:1157)
104 Patients with refractory angina, not suitable for PCI and high risk for re-op (3.2% of patients accepted for CABG)
No difference in symptom relief between SCS and CABG
It is frequently complicated by persistent skin irritation, It is frequently complicated by persistent skin irritation, which makes adequate continuation of therapy difficult. which makes adequate continuation of therapy difficult.
Meanwhile, SCS has a rather high incidence of Meanwhile, SCS has a rather high incidence of catheter catheter dislodgementdislodgement requiring repositioning, requiring repositioning, painpain at the device at the device site and site and device migrationdevice migration may occur in a large proportion may occur in a large proportion of patients; furthermore, of patients; furthermore, infectioninfection of the device system of the device system may also occur.may also occur.

Safety and Efficacy of the Safety and Efficacy of the
Coronary Sinus Reducer Coronary Sinus Reducer
in Patients with Refractoryin Patients with Refractory
Angina: the COSIRA Trial Angina: the COSIRA Trial
((Coronary Sinus ReducerCoronary Sinus Reducer
for Treatment of Refractoryfor Treatment of Refractory
Angina)Angina)
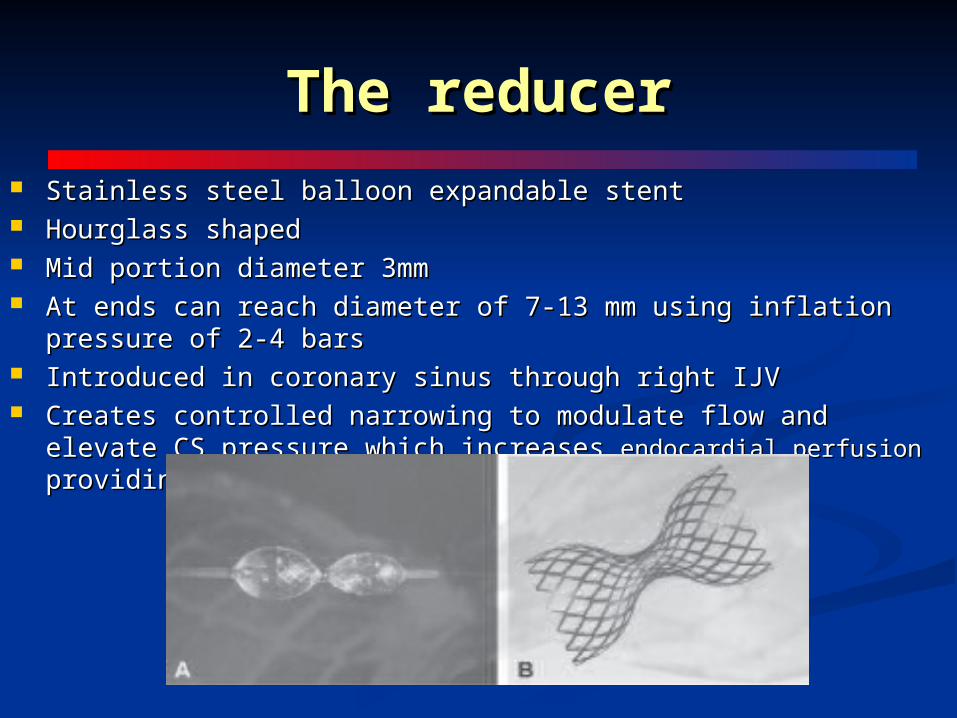
The reducerThe reducer
Stainless steel balloon expandable stentStainless steel balloon expandable stent Hourglass shapedHourglass shaped Mid portion diameter 3mm Mid portion diameter 3mm At ends can reach diameter of 7-13 mm using inflation pressure of 2-4 barsAt ends can reach diameter of 7-13 mm using inflation pressure of 2-4 bars Introduced in coronary sinus through right IJVIntroduced in coronary sinus through right IJV Creates controlled narrowing to modulate flow and elevate CS pressure Creates controlled narrowing to modulate flow and elevate CS pressure
which increases which increases endocardial perfusion endocardial perfusion providing relief of ischemia and anginaproviding relief of ischemia and angina

Implantation of the reducer stent in coronary sinusImplantation of the reducer stent in coronary sinus

mechanism of action...mechanism of action...
The Reducer creates a slight increase in CS pressure which The Reducer creates a slight increase in CS pressure which results in dilatation of the capillaries and arterioles and results in dilatation of the capillaries and arterioles and improves perfusion of ischemic sub-endocardial myocardiumimproves perfusion of ischemic sub-endocardial myocardium
In the setting of obstructive CAD –increased CS pressure can In the setting of obstructive CAD –increased CS pressure can lead to:lead to:
Redistribution of collateral blood flow from non-ischemic into Redistribution of collateral blood flow from non-ischemic into ischemic territories of the myocardiumischemic territories of the myocardium
Redistribution of arterial blood from sub-epicardial to sub-Redistribution of arterial blood from sub-epicardial to sub-endocardial vessels, with normalization of the endocardial/ endocardial vessels, with normalization of the endocardial/ epicardialblood flow ratio epicardialblood flow ratio
Redistribution of arterial blood significantly reducing Redistribution of arterial blood significantly reducing myocardial ischemiamyocardial ischemia
Study Study AIM-To examine whether implantation of the Reducer could AIM-To examine whether implantation of the Reducer could
effectively and safely improve angina symptoms in patients with effectively and safely improve angina symptoms in patients with obstructive CAD, CCS class 3 or 4, having concomitant evidence of obstructive CAD, CCS class 3 or 4, having concomitant evidence of reversible myocardial ischemia and unsuitable for revascularizationreversible myocardial ischemia and unsuitable for revascularization
STUDY-Prospective, phase-II, randomized, double-blind, sham-STUDY-Prospective, phase-II, randomized, double-blind, sham-controlled, multi-center clinical trial to test the safety and efficacy of controlled, multi-center clinical trial to test the safety and efficacy of the Reducer in 104 patientsthe Reducer in 104 patients
RESULTS- RESULTS- Primary endpoint: CCS ≥ 2 class Improvement Primary endpoint: CCS ≥ 2 class Improvement 35% (18/52) of the patients in the Reducer group vs.15% (8/52) of 35% (18/52) of the patients in the Reducer group vs.15% (8/52) of patients in the sham-control group improved by ≥2 CCS classes patients in the sham-control group improved by ≥2 CCS classes (p =0.024)(p =0.024)

The resultsThe results

summarysummary The COSIRA trial evaluated the CS Reducer as a new therapy for The COSIRA trial evaluated the CS Reducer as a new therapy for
patients with refractory anginapatients with refractory angina Reducer implantation was significantly better than a sham intervention Reducer implantation was significantly better than a sham intervention
to improve angina symptoms in patients with advanced coronary to improve angina symptoms in patients with advanced coronary artery disease unsuitable for revascularization and treated with optimal artery disease unsuitable for revascularization and treated with optimal medical therapymedical therapy
The improvement of ≥2 angina CCS classes (the primary end point) The improvement of ≥2 angina CCS classes (the primary end point) occurred 2.3 times more frequently in the Reducer group, occurred 2.3 times more frequently in the Reducer group, demonstratinga clinically meaningful difference (P =0.024)demonstratinga clinically meaningful difference (P =0.024)
Based on these findings, percutaneous transvenous implantation of Based on these findings, percutaneous transvenous implantation of the CS Reducer is a safe and effective treatment for patients with the CS Reducer is a safe and effective treatment for patients with refractory angina who are not suitable for coronary revascularization refractory angina who are not suitable for coronary revascularization despite maximally tolerated therapydespite maximally tolerated therapy

GENE THERAPYGENE THERAPY Clinical experience with protein growth factors and genes encoding for Clinical experience with protein growth factors and genes encoding for
those growth factors to enhance myocardial angiogenesis primarily those growth factors to enhance myocardial angiogenesis primarily involves vascular endothelial growth factor (VEGF)and fibroblast growth involves vascular endothelial growth factor (VEGF)and fibroblast growth factor(FGF)factor(FGF)
Multiple delivery methods (protein alone, plasmid, and adenoviral Multiple delivery methods (protein alone, plasmid, and adenoviral vectors) and routes (intravenous, intracoronary, intramyocardial) have vectors) and routes (intravenous, intracoronary, intramyocardial) have been used in clinical trials.been used in clinical trials.
Although the promise of angiogenesis is great, randomized placebo-Although the promise of angiogenesis is great, randomized placebo-controlled trials demonstrate excellent safety but only modest efficacy controlled trials demonstrate excellent safety but only modest efficacy based on secondary angina and quality-of-life .based on secondary angina and quality-of-life .
Plasids (small, circular DNA pieces) represent a relatively inefficient Plasids (small, circular DNA pieces) represent a relatively inefficient means of delivering a gene protein. They are taken up inefficiently by means of delivering a gene protein. They are taken up inefficiently by most cells and are unprotected against cellular defense mechanisms. most cells and are unprotected against cellular defense mechanisms.

Losordo et al. * published the first randomized, phase-1 clinical Losordo et al. * published the first randomized, phase-1 clinical trial testing the safety of intramyocardial delivery of VEGF plasmid trial testing the safety of intramyocardial delivery of VEGF plasmid in humans with myocardial ischemia. in humans with myocardial ischemia.
Using a left anterior thoracotomy, the plasmid VEGF DNA was Using a left anterior thoracotomy, the plasmid VEGF DNA was directly injected into the myocardium at risk in five patients with directly injected into the myocardium at risk in five patients with symptomatic angina in whom conventional therapy had failed.symptomatic angina in whom conventional therapy had failed.
Dobutamine SPECT showed evidence of reduced ischemia in all Dobutamine SPECT showed evidence of reduced ischemia in all five patients after 30 and 60 days. Rentrop collateral flow was five patients after 30 and 60 days. Rentrop collateral flow was increased in all five patients after 60 days.increased in all five patients after 60 days.
* * Losordo DW, Vale PR, Symes JF, et al. Gene therapy for myocardial angiogenesis: initial clinical results with direct myocardial injection of ph VEGF 165 as sole Losordo DW, Vale PR, Symes JF, et al. Gene therapy for myocardial angiogenesis: initial clinical results with direct myocardial injection of ph VEGF 165 as sole
therapy for myocardial ischemia. Circulation 1998;98:2800–4therapy for myocardial ischemia. Circulation 1998;98:2800–4..

Adenovirus GENe Therapy (AGENT) trialAdenovirus GENe Therapy (AGENT) trial
First randomized, double-blinded, placebo-controlled trial of gene therapy First randomized, double-blinded, placebo-controlled trial of gene therapy enrolling 79 patients with documented CAD by angiography, objective enrolling 79 patients with documented CAD by angiography, objective evidence of ischemia . Sixty patients received direct injection of recombinant evidence of ischemia . Sixty patients received direct injection of recombinant adenovirus 5 FGF-4 and 19 patients received placebo. adenovirus 5 FGF-4 and 19 patients received placebo.
Follow-up treadmill tests were performed at 4 and 12 weeks, and the active Follow-up treadmill tests were performed at 4 and 12 weeks, and the active treatment group had a greater improvement in exercise duration and a 30% treatment group had a greater improvement in exercise duration and a 30% increase in exercise tolerance time, as compared with the placebo group.increase in exercise tolerance time, as compared with the placebo group.
It should be noted that the placebo group showed marked improvement It should be noted that the placebo group showed marked improvement from baseline, demonstrating the importance of double-blinded, placebo-from baseline, demonstrating the importance of double-blinded, placebo-controlled trials in this population.controlled trials in this population.
Grines C. Late breaking trial results: the AGENT trial. Presented at: American College of Cardiology, 50th Annual Scientific Sessions, March 2001, Orlando, FLGrines C. Late breaking trial results: the AGENT trial. Presented at: American College of Cardiology, 50th Annual Scientific Sessions, March 2001, Orlando, FL..
ESMR (Extracorporeal Shockwave Myocardial ESMR (Extracorporeal Shockwave Myocardial Revascularization)Revascularization)
It is a breakthrough in management of refractory angina It is a breakthrough in management of refractory angina pectorispectoris
The treatment is performed using a special generator that The treatment is performed using a special generator that produces low intensity shockwaves, a kind of sound waves produces low intensity shockwaves, a kind of sound waves similar to, but of lower strength than Extracorporeal Shock similar to, but of lower strength than Extracorporeal Shock Wave Lithotripsy (ESWL) that is used in the treatment of Wave Lithotripsy (ESWL) that is used in the treatment of kidney stones .kidney stones .
These waves stimulate the formation of new blood vessels in These waves stimulate the formation of new blood vessels in the heart.the heart.
The shock wave schedule consists of three 20-minute The shock wave schedule consists of three 20-minute sessions per week over nine weeks.sessions per week over nine weeks.

The patient must first undergo cardiac SPECT (single photon The patient must first undergo cardiac SPECT (single photon emission computed tomography) testing to identify the location of emission computed tomography) testing to identify the location of the ischemic areas.the ischemic areas.
Afterwards a handheld device called a transducer is placed over Afterwards a handheld device called a transducer is placed over the skin and shockwaves will then be delivered directly to the the skin and shockwaves will then be delivered directly to the ischemic region under echocardiographic guidance. ischemic region under echocardiographic guidance.
ESMR is an alternative therapy for patients who have angina, ESMR is an alternative therapy for patients who have angina, even though they take medicine, and are not suitable candidates even though they take medicine, and are not suitable candidates for coronary angioplasty or bypass surgeryfor coronary angioplasty or bypass surgery
Nishida T,Shimokawa H et al. Extracorporeal cardiac shock wave therapy markedly ameliorates ischemia-induced myocardial dysfunction in pigs in vivo. Circulation 2004;110: Nishida T,Shimokawa H et al. Extracorporeal cardiac shock wave therapy markedly ameliorates ischemia-induced myocardial dysfunction in pigs in vivo. Circulation 2004;110: 3055-3061.3055-3061.
[ Faber L, Lindner O, Prinz C, Fricke E, Hering D, Burchert W, Horstkotte D. Echo guided extracorporeal shockwave therapy for refractory angina improves regional [ Faber L, Lindner O, Prinz C, Fricke E, Hering D, Burchert W, Horstkotte D. Echo guided extracorporeal shockwave therapy for refractory angina improves regional myocardial blood flow as assessed by PET imaging. J. Am. Coll. Cardiol. 2010;55:A120.E1125myocardial blood flow as assessed by PET imaging. J. Am. Coll. Cardiol. 2010;55:A120.E1125
Caspari GH, Erbel R. Revascularization with extracorporeal shock wave therapy: first clinical results. Circulation 1999;100(Suppl 18):84-89.Caspari GH, Erbel R. Revascularization with extracorporeal shock wave therapy: first clinical results. Circulation 1999;100(Suppl 18):84-89.

PERCUTANEOUS IN SITUPERCUTANEOUS IN SITUCORONARY VENOUS ARTERIALIZATIONCORONARY VENOUS ARTERIALIZATION
Percutaneous in situ coronary venous arterialization (PICVA) is Percutaneous in situ coronary venous arterialization (PICVA) is a percutaneous approach to CABG that redirects arterial blood a percutaneous approach to CABG that redirects arterial blood flow from the occluded, offending artery into an adjacent flow from the occluded, offending artery into an adjacent coronary vein, thereby arterializing the vein and providing coronary vein, thereby arterializing the vein and providing retroperfusion to ischemic myocardium.retroperfusion to ischemic myocardium.
Even in the most severe cases of CAD, the venous system is Even in the most severe cases of CAD, the venous system is generally free of atherosclerosis, and the individual veins are generally free of atherosclerosis, and the individual veins are dispensable, owing to a redundant venous system.dispensable, owing to a redundant venous system.
Percutaneous in situ coronary artery bypass (PICAB) is an Percutaneous in situ coronary artery bypass (PICAB) is an advancing technology for this group of patients with refractory advancing technology for this group of patients with refractory angina.angina.

The procedure requires that the occluded artery and corresponding The procedure requires that the occluded artery and corresponding great vein be imaged. A needle is advanced proximal to the great vein be imaged. A needle is advanced proximal to the occlusion in the artery and into the adjacent vein under ultrasound occlusion in the artery and into the adjacent vein under ultrasound guidance. A connector is then placed in between the structures, and guidance. A connector is then placed in between the structures, and a plug is placed proximal to the coronary sinus so that venous a plug is placed proximal to the coronary sinus so that venous retroperfusion may occur.retroperfusion may occur.
Arterial blood flow is redirected from a diseased artery to an adjacent Arterial blood flow is redirected from a diseased artery to an adjacent coronary vein, and then rerouted back to the artery after the lesion .coronary vein, and then rerouted back to the artery after the lesion .
Thus, the coronary vein acts as an in situ coronary bypass conduit Thus, the coronary vein acts as an in situ coronary bypass conduit
rather than as a means of retroperfusion. rather than as a means of retroperfusion. It requires two arteriovenous fistulae to be created—one on either side It requires two arteriovenous fistulae to be created—one on either side
of the artery blockage—and that the vein be blocked both distally and of the artery blockage—and that the vein be blocked both distally and proximally.proximally.
Oesterle et al. * reported the first successful case of PICVA in a 53-Oesterle et al. * reported the first successful case of PICVA in a 53-year-old diabetic German man diagnosed with CCS class IV angina year-old diabetic German man diagnosed with CCS class IV angina refractory to medical therapy and not a good candidate for CABG or refractory to medical therapy and not a good candidate for CABG or PCI PCI
Currently it must be considered experimental only.Currently it must be considered experimental only.
**Oesterle SN, Reifart N, Hauptmann E, et al. Percutaneous in situ coronary venous arterialization: report of the first human catheterbased coronary Oesterle SN, Reifart N, Hauptmann E, et al. Percutaneous in situ coronary venous arterialization: report of the first human catheterbased coronary artery bypass. Circulation 2001;103:2539–43.artery bypass. Circulation 2001;103:2539–43.

HEART TRANSPLANTHEART TRANSPLANT
For patients who have disabling angina and in whom all For patients who have disabling angina and in whom all conventional and alternative treatment modalities have conventional and alternative treatment modalities have failed, heart transplantation should be considered. failed, heart transplantation should be considered.
Heart transplants are severely limited in number, with Heart transplants are severely limited in number, with only 3,000 transplantations being performed worldwide.only 3,000 transplantations being performed worldwide.
Heart transplantation remains a final option for these Heart transplantation remains a final option for these patients.patients.

Alternative Therapies for Relief of Symptoms inAlternative Therapies for Relief of Symptoms inPatients With Refractory Angina: RecommendationPatients With Refractory Angina: Recommendation


CONCLUSIONCONCLUSION
End-stage angina pectoris refractory to conventional End-stage angina pectoris refractory to conventional medical therapy and not amenable to either CABG or PCI medical therapy and not amenable to either CABG or PCI represents a truly desperate and frustrating condition for represents a truly desperate and frustrating condition for both the patient and physician. both the patient and physician.
There is no suggestion that any of the alternative There is no suggestion that any of the alternative treatments for refractory angina may improve prognosis.treatments for refractory angina may improve prognosis.
The choice of treatment should be mainly based on a The choice of treatment should be mainly based on a careful assessment of the balance between the benefits for careful assessment of the balance between the benefits for the disabling symptoms of patients and the risk associated the disabling symptoms of patients and the risk associated with the different treatment options.with the different treatment options.

THANK YOUTHANK YOU..........

Current pharmacologic Current pharmacologic antianginal strategiesantianginal strategies
New mechanistic approaches to anginaNew mechanistic approaches to angina Rho kinase inhibition (Rho kinase inhibition (fasudilfasudil)) Metabolic modulation (Metabolic modulation (trimetazidinetrimetazidine)) Preconditioning (Preconditioning (nicorandilnicorandil)) Sinus node inhibition (Sinus node inhibition (ivabradineivabradine)) Late Na+ current inhibition (Late Na+ current inhibition (ranolazineranolazine))

Rho kinase inhibition: FasudilRho kinase inhibition: Fasudil Rho kinase triggers vasoconstriction through Rho kinase triggers vasoconstriction through
accumulation of phosphorylated myosinaccumulation of phosphorylated myosin
Adapted from Seasholtz TM. Am J Physiol Cell Physiol. 2003;284:C596-8.
Ca2+ Ca2+
PLC
SR Ca2+
Receptor
Agonist
Myosin
Myosin-P
Myosin phosphatase
PIP2
IP3
MLCK
VOC ROC
Ca2+
Calmodulin
Rho
Rho kinase
Fasudil

Metabolic modulation (pFOX): Metabolic modulation (pFOX): TrimetazidineTrimetazidine
O2 requirement of O2 requirement of glucose pathway is glucose pathway is lower than FFA lower than FFA pathwaypathway
During ischemia, During ischemia, oxidized FFA levels oxidized FFA levels rise, blunting the rise, blunting the glucose pathwayglucose pathway
FFA Glucose
Acyl-CoA
Acetyl-CoA
Pyruvate
Energy for contraction
Myocytes
β-oxidation
Trimetazidine
MacInnes A et al. Circ Res. 2003;93:e26-32.Lopaschuk GD et al. Circ Res. 2003;93:e33-7.
Stanley WC. J Cardiovasc Pharmacol Ther. 2004;9(suppl 1):S31-45.
pFOX = partial fatty acid oxidationFFA = free fatty acid

Preconditioning: NicorandilPreconditioning: Nicorandil
Nitrate-associated effects• Vasodilation of coronary epicardial arteries
Activation of ATP-sensitive K+ channels• Ischemic preconditioning• Dilation of coronary resistance arterioles
IONA Study Group. Lancet. 2002;359:1269-75.Rahman N et al. AAPS J. 2004;6:e34.
N O
O NO2
HN
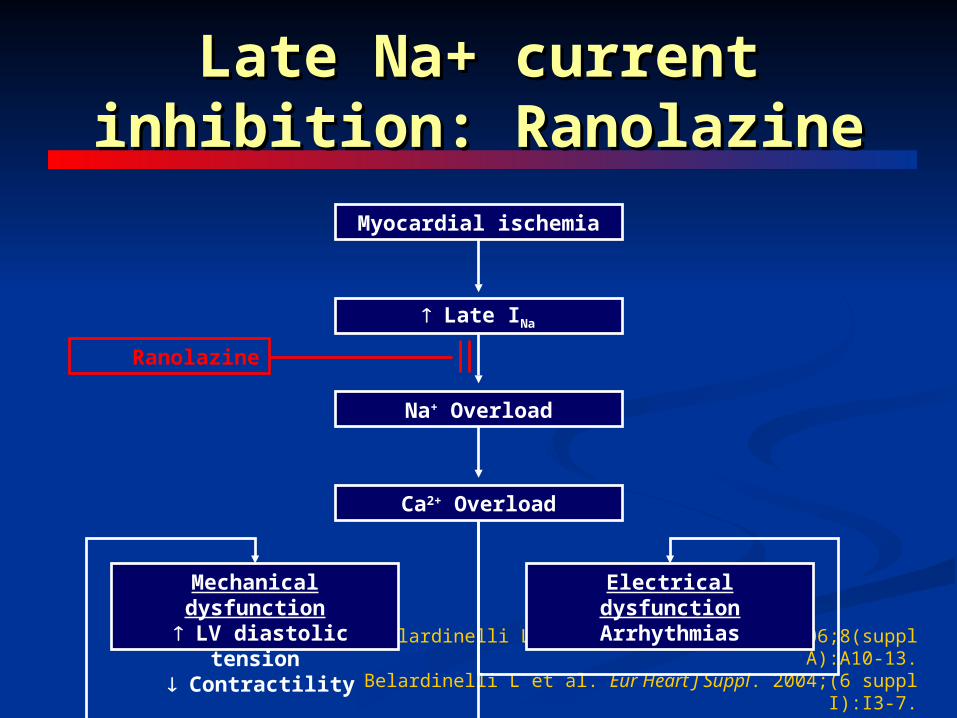
Late Na+ current inhibition: Late Na+ current inhibition: RanolazineRanolazine
Belardinelli L et al. Eur Heart J Suppl. 2006;8(suppl A):A10-13.Belardinelli L et al. Eur Heart J Suppl. 2004;(6 suppl I):I3-7.
Myocardial ischemia
Late INa
Na+ Overload
Ca2+ Overload
Mechanical dysfunction LV diastolic tension
Contractility
Electrical dysfunctionArrhythmias
Ranolazine

Understanding Angina at the Understanding Angina at the Cellular LevelCellular Level
Ischemia impairs cardiomyocyte Ischemia impairs cardiomyocyte sodium channel functionsodium channel function
Impaired sodium channel function Impaired sodium channel function leads to:leads to: Pathologic increased late sodium Pathologic increased late sodium
currentcurrent Sodium overloadSodium overload Sodium-induced calcium overloadSodium-induced calcium overload
Calcium overload causes diastolic Calcium overload causes diastolic relaxation failure, which:relaxation failure, which: Increases myocardial oxygen Increases myocardial oxygen
consumptionconsumption Reduces myocardial blood flow Reduces myocardial blood flow
and oxygen supplyand oxygen supply Worsens ischemia and anginaWorsens ischemia and angina
Ranolazine
Ischemia
↑ Late INa
Na+ Overload
Diastolic relaxation failureExtravascular compression
Ca++ Overload
Chaitman BR. Circulation. 2006;113:2462-2472

Na+/Ca2+ overload and Na+/Ca2+ overload and ischemiaischemia
Adapted from Belardinelli L et al. Eur Heart J Suppl. 2006;8(suppl A):A10-13.
Late Na+ current
Diastolic wall tension (stiffness)
Intramural small vessel compression( O2 supply)
O2 demand
Na+ overload
Ca2+ overload
Myocardial ischemia

Ischaemia( oxygen supply/ Demand)
late Na+ current
Na+/Ca++ exchange pump activation
[Ca2+] overload
Diastolic wall tension (stiffness)
Vascular compression
[Na+]i
RanolazineRanolazine

Metabolic modulation (pFOX) Metabolic modulation (pFOX) and ranolazineand ranolazine
Clinical trials showed ranolazine SR 500–Clinical trials showed ranolazine SR 500–1000 mg bid (~2–6 µmol/L) reduced angina1000 mg bid (~2–6 µmol/L) reduced angina
Experimental studies demonstrated that Experimental studies demonstrated that ranolazine 100 µmol/L achieved only 12% ranolazine 100 µmol/L achieved only 12% pFOX inhibitionpFOX inhibition Ranolazine does not inhibit pFOX substantially at Ranolazine does not inhibit pFOX substantially at
clinically relevant doses clinically relevant doses Fatty acid oxidation Inhibition is not a major Fatty acid oxidation Inhibition is not a major
antianginal mechanism for ranolazineantianginal mechanism for ranolazineMacInnes A et al. Circ Res. 2003;93:e26-32.
Antzelevitch C et al. J Cardiovasc Pharmacol Therapeut. 2004;9(suppl 1):S65-83.
Antzelevitch C et al. Circulation. 2004;110:904-10.
pFOX = partial fatty acid oxidation
Ranolazine: Key conceptsRanolazine: Key concepts
Ischemia is associated with ↑ Na+ entry into Ischemia is associated with ↑ Na+ entry into cardiac cells cardiac cells Na+ efflux by Na+/Ca2+ exchange results in ↑ Na+ efflux by Na+/Ca2+ exchange results in ↑
cellular [Ca2+]i and eventual Ca2+ overload cellular [Ca2+]i and eventual Ca2+ overload Ca2+ overload may cause electrical and Ca2+ overload may cause electrical and
mechanical mechanical dysfunctiondysfunction ↑ ↑ Late INa is an important contributor to the Late INa is an important contributor to the
[Na+]i - dependent Ca2+ overload[Na+]i - dependent Ca2+ overload Ranolazine reduces late INa Ranolazine reduces late INa
Belardinelli L et al. Eur Heart J Suppl. 2006;8(suppl A):A10-13.Belardinelli L et al. Eur Heart J Suppl. 2004;(6 suppl I):I3-7.

Medication Medication ClassClass
Impact Impact on HRon HR
Impact Impact on BPon BP
Physiologic Physiologic MechanismMechanism
Beta Beta BlockersBlockers
Decrease pump Decrease pump functionfunction
Calc Calc Channel Channel BlockersBlockers
Decrease Pump Decrease Pump function + Vaso-function + Vaso-dilitationdilitation
NitratesNitrates Vaso-dilitationVaso-dilitation
RanolazineRanolazine OO OO Reduced Cardiac Reduced Cardiac StiffnessStiffness
Pharmacologic Classes for Treatment of Angina