Embed Size (px)
Citation preview

ANN
NULAR PA
NCREAS: AN UNUSU
UAL PRESSENTATIONN

Case Report
CASE REPORT
A forty three years male presented with a moderateintensity pain in the epigastric region, radiating to back forone week. He also complained of non bilious vomitingcontaining undigested food particles. He had lost about 7 kgweight in last 5 months. He had an episode of paindiagnosed as acute pancreatitis 6 months back on the basisof raised serum amylase and lipase levels. He was treatedconservatively that time. He was neither an alcoholic nor asmoker. On examination patient was afebrile, anicteric witha pulse rate of 74 per min and blood pressure of 110/70 mmHg. Abdominal examination revealed non tender, epigastricfullness, with succusion splash in the epigastrium. Routineblood investigations showed Hb - 13.1 gm/dL, TLC -11,600/cu mm and platelet count - 1,97,000/cu mm. Hisliver function showed raised serum alkaline phosphatase -310 IU (n <117 IU) and serum gamma glutamide transpeptidase (GGTP) - 104 (n <50 IU). Serum amylase was371 (30-110IU/L) and Serum lipase was 810 (23-300 U/L).His CA 19.9 was marginally raised to 77 U/mL (0-35U/mL).
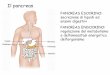
Contrast enhanced computerised tomography (CECT)whole abdomen showed abnormally placed subhepaticgallbladder with enlarged pancreatic head (4 × 3 cm) anddilated main pancreatic duct (4 mm). No pancreaticcalcification was seen (Fig 1). CT also showed evidence ofbiliary and duodenal obstruction with gastric distension.Duodenal obstruction was also confirmed by uppergastrointestinal endoscopy showing grossly distendedstomach with food residue. The scope could not benegotiated beyond second part of duodenum.
On the basis of above findings and investigations wemade a working diagnosis of a pancreatic mass (? chronicpancreatitis,?? carcinoma pancreas) with gastric outletobstruction, biliary obstruction and pancreatic ductobstruction. Patient was planned for a resection procedureand accordingly preoperative preparation and counseling ofthe patient was done. He was operated on 2nd Dec’ 2009. At
307 Apollo Medicine, Vol. 7, No. 4, December 2010
ANNULAR PANCREAS: AN UNUSUAL PRESENTATION
Nitish Anchal*, Prithpal Singh**, Saket Goel***, Sanjay Sikka@, Deep Shikha Arora@@
and Deepak Govil****Junior Consultant, Department of Surgery,**Fellow, Department of Surgical Gastroenterology, ***Senior Consultant,Department of Surgical Gastroenterology, @Senior Consultant, Department of Gastroenterology, Senior Consultant,
Department of Histopathology, Indraprastha Apollo Hospitals, Sarita Vihar, New Delhi 110 076.Correspondence to: Dr. Deepak Govil, Senior Consultant, Department of Histopathology, Indraprastha Apollo Hospitals,
Sarita Vihar, New Delhi 110 076.
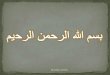
operation we found that the gall bladder fundus wasadherent to the posterior peritoneal fold (Fig 2). There wasa hard pancreatic head mass measuring about 4×5cm,along with a grossly distended and dilated CBD. Liverappeared normal. We performed a Whipple’s pancreato-duodenec-tomy with a feeding jejunostomy. Thepancreatic duct was also dilated (5 mm) and we did a ductto mucosa pancreato- jejunostomy. Postoperativelyfeeding was started through jejunostomy tube on secondpostoperative day and on 5th postoperative day oral feedswere started. Patient had a smooth postoperative recoveryand was discharged on ninth postoperative day.Histopathology of surgical specimen showed second partof duodenum was narrow and surrounded by pancreatictissue all around. Histopathological diagnosis was annularpancreas with chronic pancreatitis with chroniccholecystitis and reactive peripancreatic lymphnodes.
We retrospectively reviewed the preoperative CECT ofthe patient, it was done from a local hospital and still didnot show evidence of annular pancreas.
REVIEW OF LITERATURE
Annular pancreas is an uncommon condition in adults.The ring formation generally originates from the failure ofnormal clockwise rotation of ventral pancreas. Firstdescribed by Tiedmann in 1818 [1], its incidence is1:20,000 population. It has bimodal presentation i.e is seeneither in Infants or in 4th & 5th decade of life [2].
Embryonic development of pancreas andbiliary tree
The ventral pancreatic bud and biliary system arisefrom the hepatic diverticulum, and the dorsal pancreaticbud arises from the dorsal mesogastrium. After clockwiserotation of the ventral bud around the caudal part of theforegut, there is fusion of the dorsal pancreas (locatedanterior) and ventral pancreas (located posterior). Finally,
Apollo Medicine, Vol. 7, No. 4, December 2010 308
Case Report
Fig 1 CECT whole abdomen
Fig 2 Intraoperative findings of the case.
the ventral and dorsal pancreatic ducts fuse, and thepancreas is predominantly drained through the ventralduct, which joins the common bile duct (CBD) at the levelof the major papilla. The dorsal duct empties at the level ofthe minor papilla.
There are two theory postulated for development ofannular pancreas. Lecco [3] postulated that adhesion of the
distal tip of the ventral primordium to the duodenal wall,before its migration, is responsible for the pancreaticobstructing ring. Baldwin [4] stated that persistence andfurther development of the left ventral bud is responsiblefor the formation of the annular pancreatic tissue aroundthe duodenum. Abdominal pain was the most frequentsymptom, followed by vomiting and jaundice. Thesymptoms of the disease in adults are often associated with

Case Report
309 Apollo Medicine, Vol. 7, No. 4, December 2010
pancreatic or gastric outlet obstruction. Division orresection of the pancreatic annulus have high morbidityand mortality rate [6]. Bypass surgery of the annulus in theform of gastrojejunostomy, duodenojejunostomy orpancreatico-duodenectomy. Annular Pancreas was foundconcomitantly with ampullary carcinoma (5 cases) andpancreatic adenocarcinoma (3 cases). The differentialdiagnosis between focal inflammatory lesions in the head ofthe pancreas due to chronic pancreatitis and pancreaticcancer remains a challenging task for radiologists,pathologists and surgeons. The association of annularpancreas and periampullary malignancy in adults must notbe overlooked, and their coexistence must be considereduntil its absence is proved. Annular pancreas can be a rarecause of gastric, biliary and pancreatic duct obstruction. Itmay be associated with recurrent pancreatitis. Resection isadvisable if there is suspicion of malignancy.
REFERENCES
1. Tiedmann Fuber die verschiedenheiten desausfuhrangsganges der bauchspeicheldruse beidenmenschen und saugetieren. Dtsch Arch Physiol1818; 4: 403.
2. Kiernan PD, ReMine SG, Kiernan PC, ReMine WH.Annular pancreas - Mayo Clinic experience from 1957to1976 with a review of the literature. Arch Surg 1980; 115:46-50.
3. Lecco TM. Zur Morphologie des pankreasannulare.Sitzungb Akad Wissensch 1910; 119: 391-406.
4. Baldwin WM. A specimen of annular pancreas. Anat Sec1910; 4: 299-304.
5. Dharmsathaphorn K, Burrell M, Dobbins J. Diagnosis ofannular pancreas with endoscopic retrogradecholangiopancreatography. Gastroenterology 1979;77:1109-1114.
6. Michael C Beachley, Charles A Lankau. Symptomaticadult annular pancreas. Digestive Diseases andSciences. 1973; 18(6), 513-516.
complications of peptic ulcer, pancreatitis, duodenalobstruction and biliary tract obstruction. Although annularpancreas may encircle the duodenum completely in adults,the food usually can pass through the duodenum withoutproblem. But, annular pancreas may compress and obstructthe duodenum secondary to chronic pancreatitis.
In our cases, patient presented with gastric outletobstruction and pancreatitis with raised serum amylase andlipase levels. His CA 19.9 was marginally raised. Onendoscopy scope couldn’t be negotiated beyond secondpart of duodenum.
The preoperative diagnosis of annular pancreas is oftendifficult. Imaging is of paramount importance to establish acorrect diagnosis and to minimize surgical intervention.Upper GI series have been considered the study of choice.CT scan illustrate the pancreatic tissue, completely orpartly encircling the duodenum. Crocodile jawconfiguration of pancreatic tissue is typical for annularpancreas. Presence of pancreatic tissue posterolateral to2nd part duodenum has sensitivity 92% and specificity100%. Endoscopic ultrasonography and MRCP are usefultools for diagnosis of Annular Pancreas.
ERCP is invasive, and its indication is limited in patientswith acute pancreatitis because it may aggravate thesituation or induce iatrogenic pancreatitis in normalpatients. Once duodenal obstruction is present, ERCP maybe technically difficult or impossible [5]. MRCP is a non-invasive method for visualizing the biliary tree andpancreatic duct without injection of contrast medium.When the aberrant pancreatic duct encircling andextending to the right side of the duodenum is identified byMRCP, the diagnosis of annular pancreas is established.But, sometimes the pancreatic duct without dilation isinvisible on MRCP.
Surgery is still necessary to confirm the diagnosis. Themain goal of surgical treatment is relief of duodenal,

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/