Embed Size (px)
Citation preview

Anticoagulant in Liver Cirrhosis
By
Mohamed Abdel Ghani SolimanDemonstrator of Tropical Medicine
Assiut University
The liver
& haemostasis
Coagulation factors
Anticoagulant proteins
Fibrinolyticsystem
Clearing coagulation
factors
Introduction
Ascites
Spontaneous bacterial
peritonitis
Variceal bleeding
Hepatic encephalopathy
Hepatorenalsyndrome
Hematologic abnormalities. Hematologic
abnormalities.
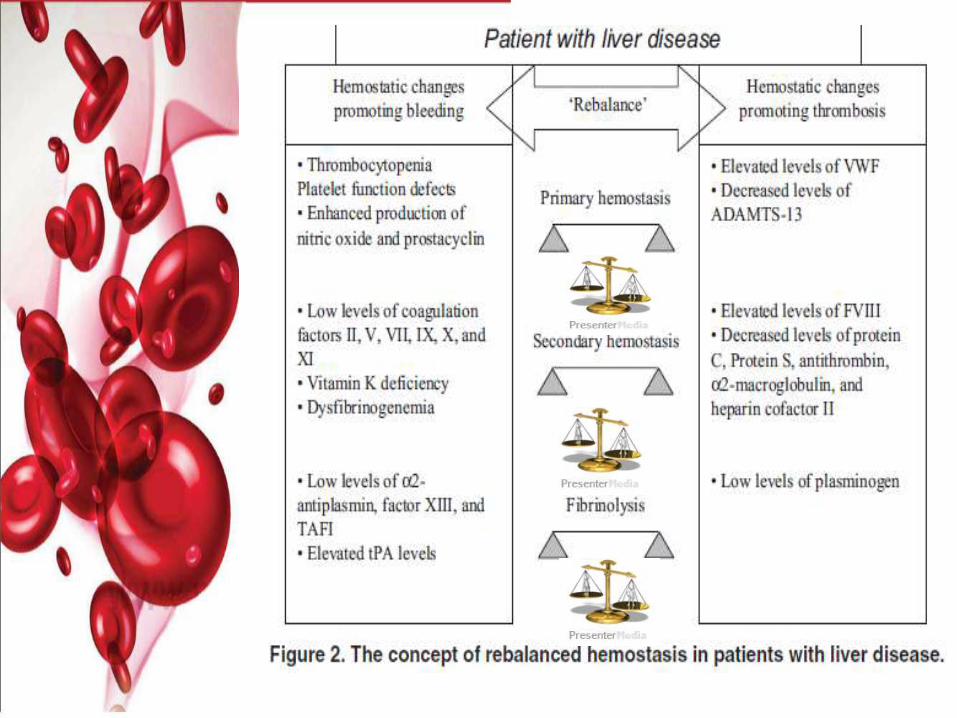
The aetiology of impairedhaemostasis in liver disease ismultifactorial and may include:
– Impaired coagulation factor synthesis.
– Synthesis of dysfunctional coagulationfactors.
– Increased consumption of coagulationfactors.
– Altered clearance of activatedcoagulation factors.
– Quantitative and qualitative plateletdisorders.
• Impaired prothrombin time in
cirrhotic patients has led to a
theory of "autoanticoagulation"
Should we give thromboprophylaxisto patients with liver cirrhosis and coagulopathy?
Our Topics:
• Physiology of haemostasis.
• The liver & the haemostatic system.
• Cirrhosis & haematological changes
– Bleeding VS Thrombosis.
• Anticoagulant in liver disease.
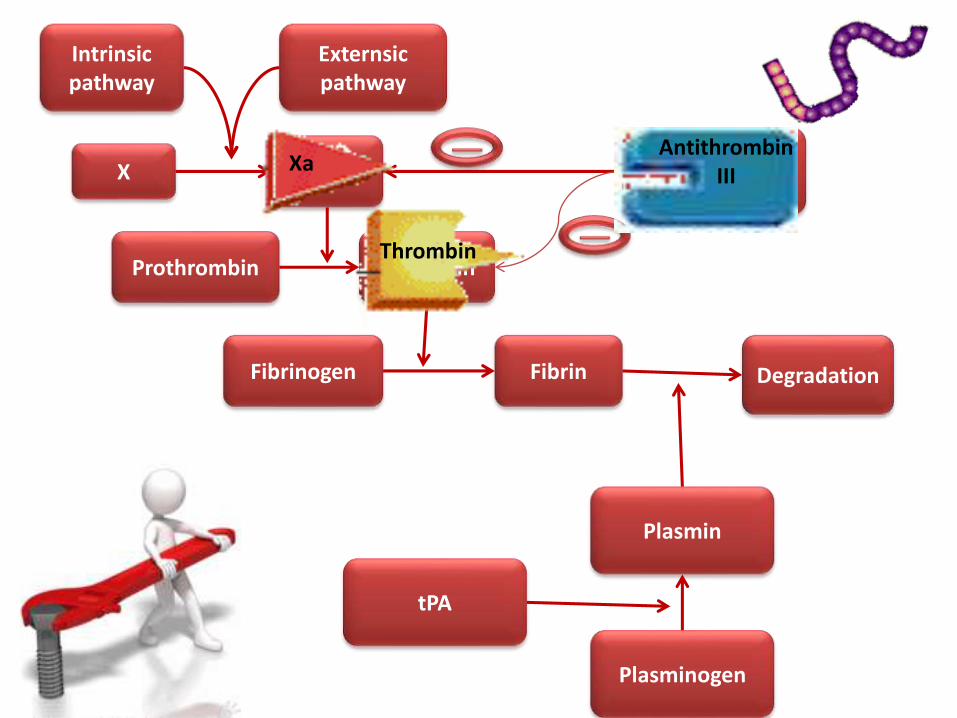
Physiology of haemostasis
Hemostasis is a cellular process withthe activated platelet as the primaryeffector and enabler of coagulation.
The structure of a clot is a plateletplug restrained by a fibrin meshformed by the conversion offibrinogen to fibrin by the enzymethrombin.
Tripodi, et al. Abnormalities of hemostasis and bleeding in chronic liver disease. Intern Emerg Med 2010.
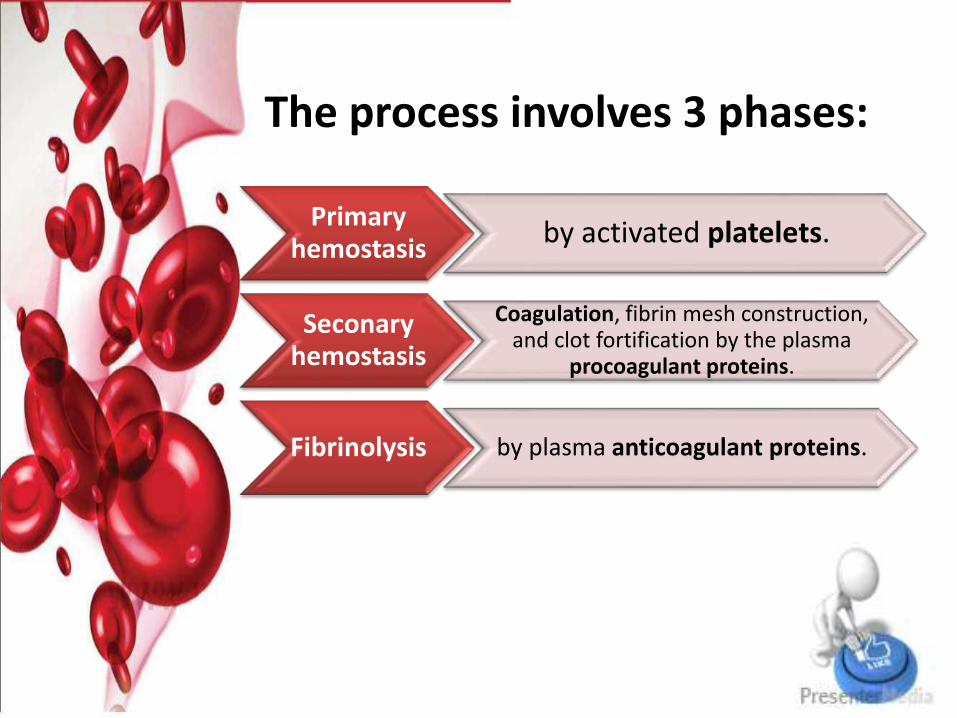
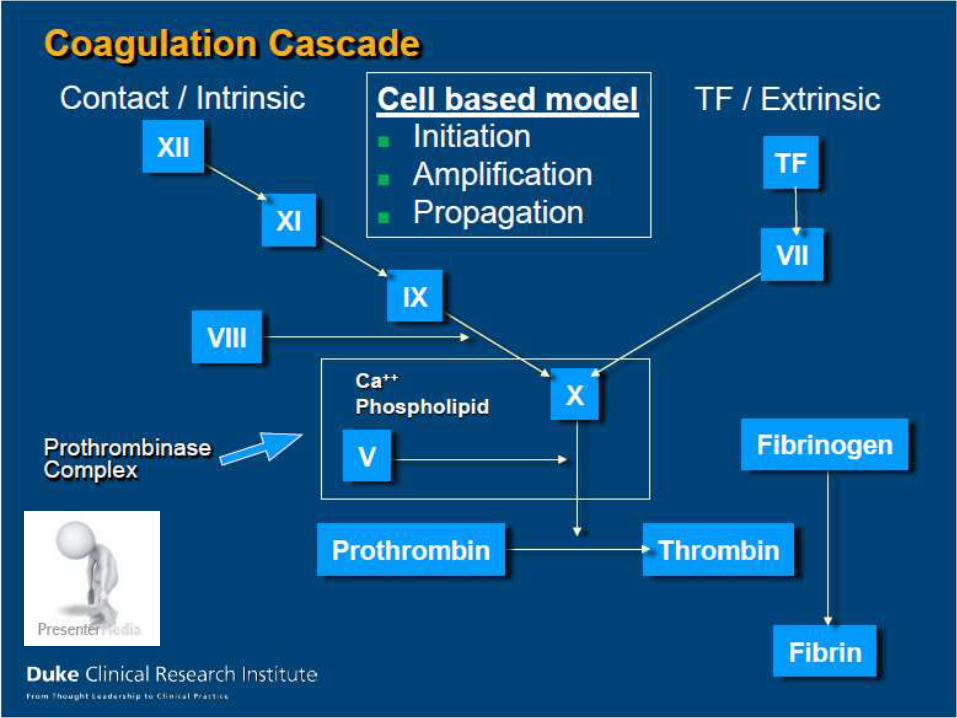
The process involves 3 phases:
Primary hemostasis
by activated platelets.
Seconaryhemostasis
Coagulation, fibrin mesh construction, and clot fortification by the plasma
procoagulant proteins.
Fibrinolysis by plasma anticoagulant proteins.
Virchow’s Triad
Platelet Activation and Factors for Clot Formationhttps://www.youtube.com/watch?v=R8JMfbYW2p4
Coagulation Cascade Animationhttps://www.youtube.com/watch?v=cy3a__OOa2M
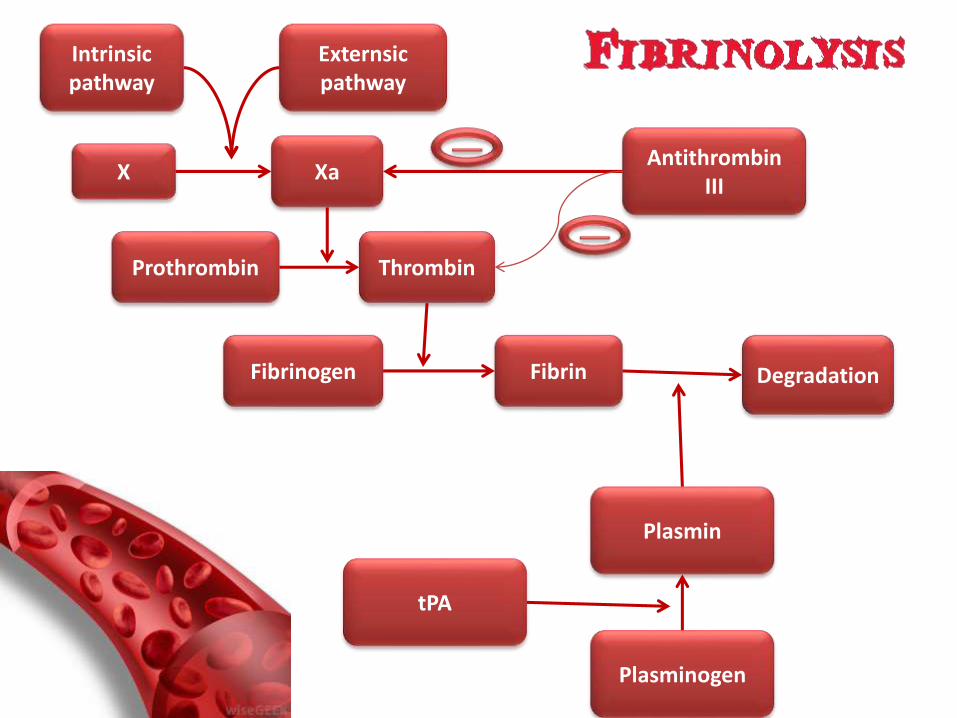
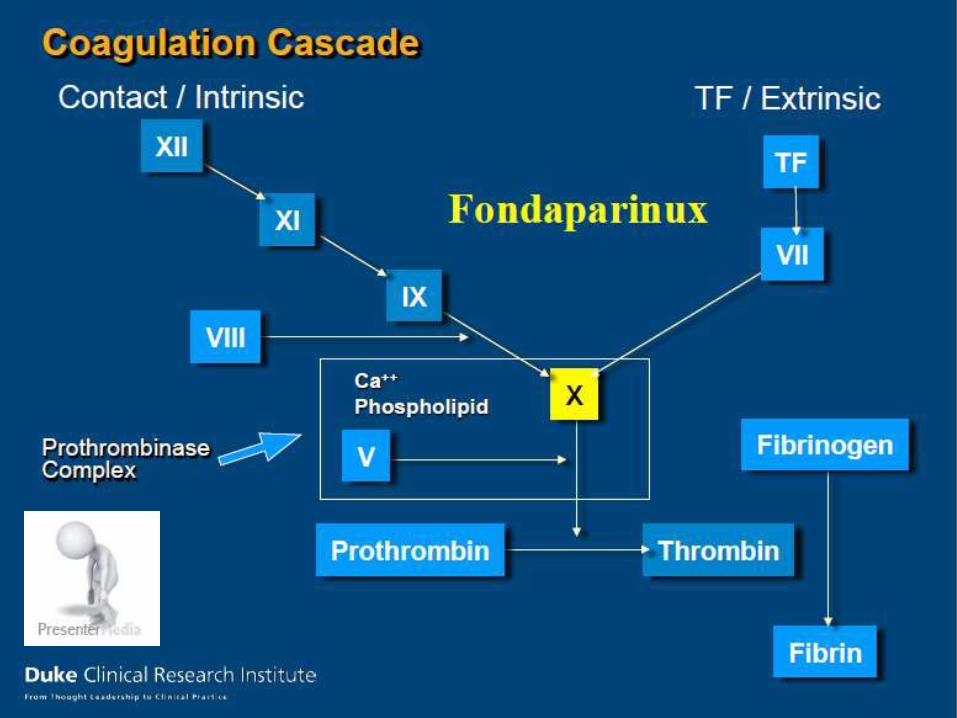
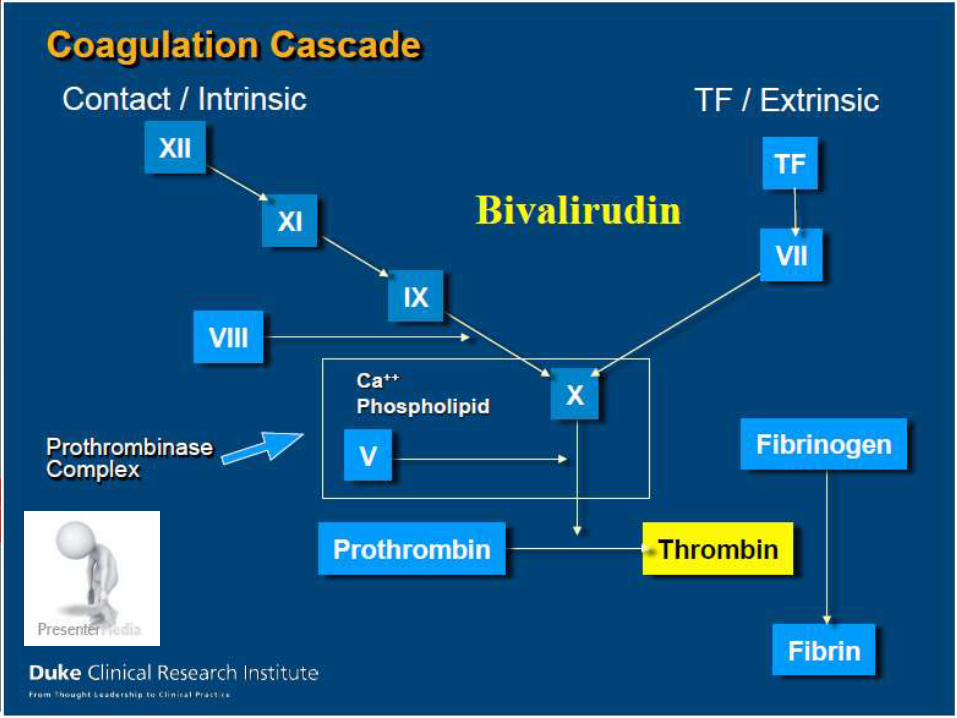
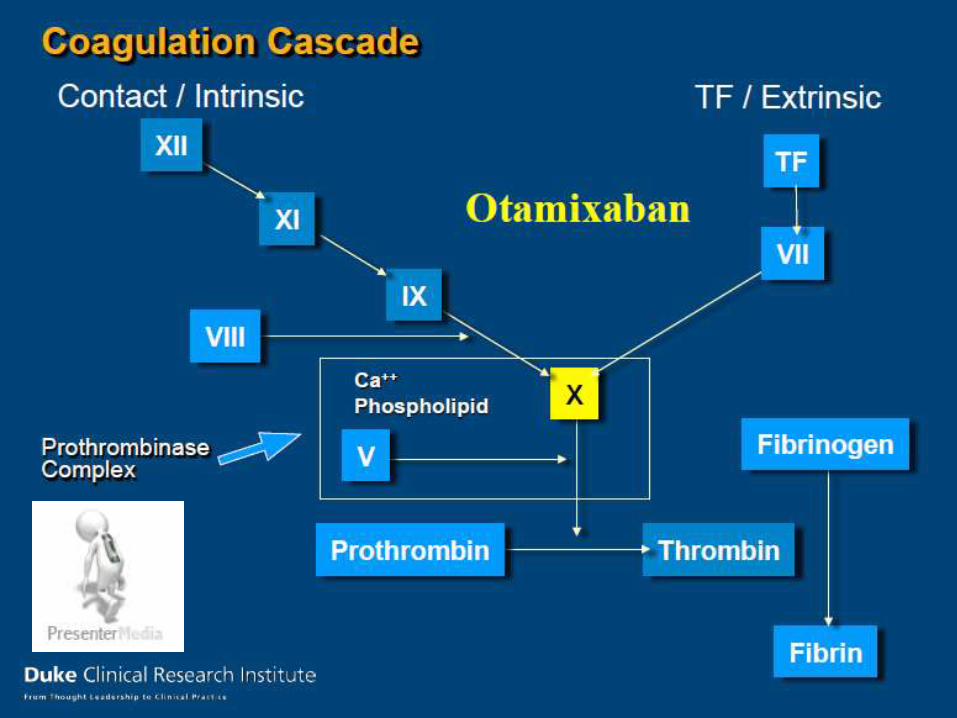
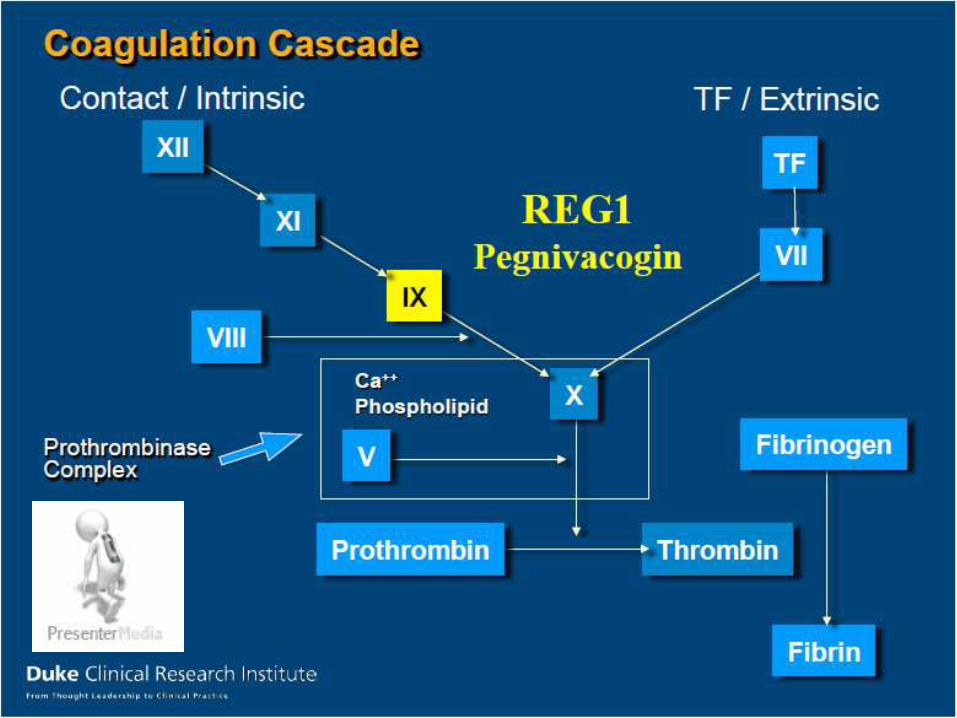
Intrinsic pathway
Externsicpathway
X Xa
Fibrinogen Fibrin
Prothrombin Thrombin
AntithrombinIII
Degradation
Plasmin
Plasminogen
tPA
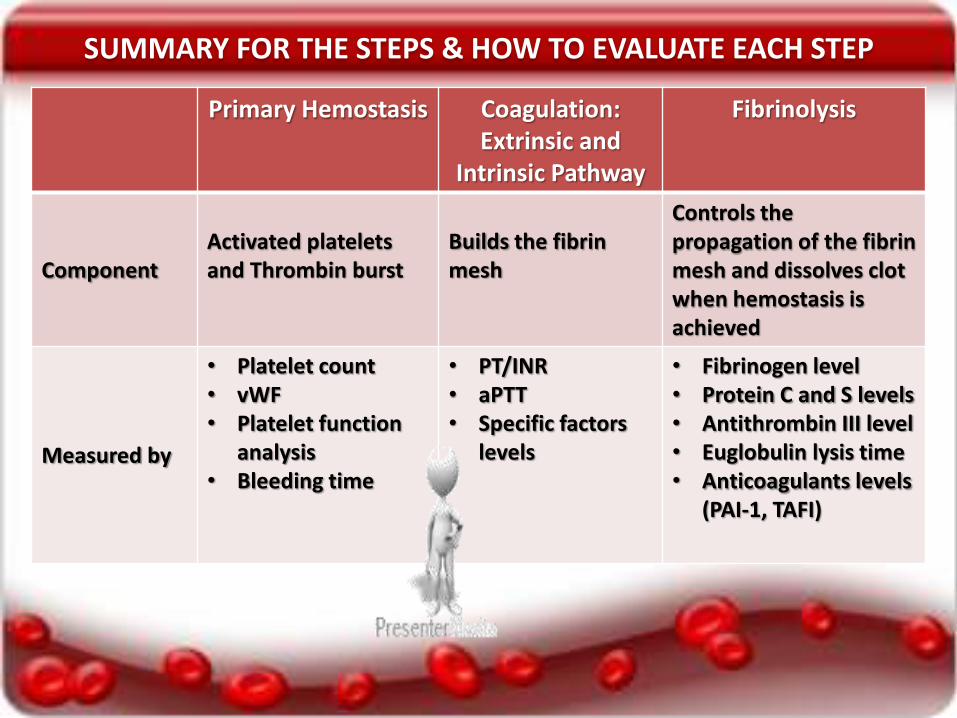
Primary Hemostasis Coagulation: Extrinsic and
Intrinsic Pathway
Fibrinolysis
ComponentActivated platelets and Thrombin burst
Builds the fibrin mesh
Controls the propagation of the fibrin mesh and dissolves clot when hemostasis is achieved
Measured by
• Platelet count• vWF• Platelet function
analysis• Bleeding time
• PT/INR• aPTT• Specific factors
levels
• Fibrinogen level • Protein C and S levels• Antithrombin III level• Euglobulin lysis time• Anticoagulants levels
(PAI-1, TAFI)
SUMMARY FOR THE STEPS & HOW TO EVALUATE EACH STEP
HEMOSTASIS IN
CHRONIC LIVER DISEASE
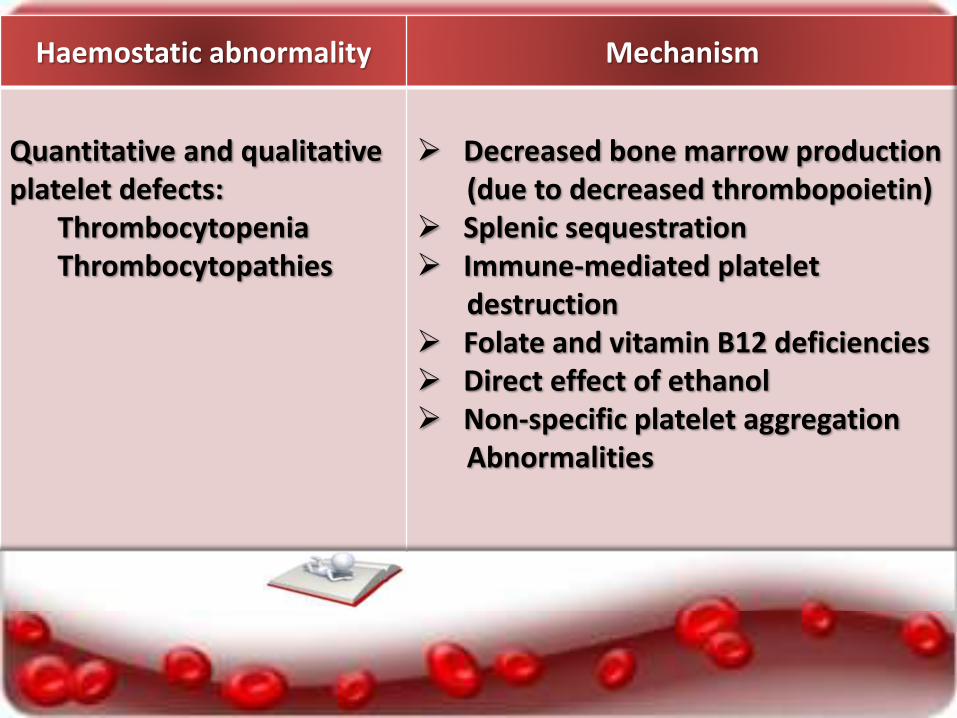
Haemostatic abnormality Mechanism
Quantitative and qualitative platelet defects:
ThrombocytopeniaThrombocytopathies
Decreased bone marrow production (due to decreased thrombopoietin)
Splenic sequestration Immune-mediated platelet
destruction Folate and vitamin B12 deficiencies Direct effect of ethanol Non-specific platelet aggregation
Abnormalities
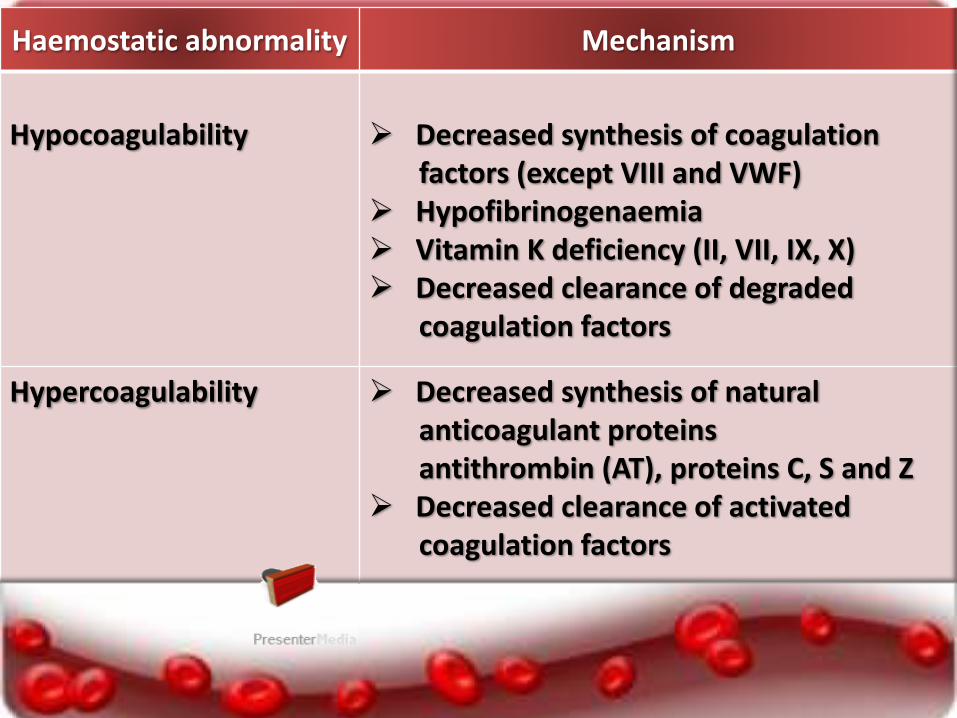
Haemostatic abnormality Mechanism
Hypocoagulability Decreased synthesis of coagulation factors (except VIII and VWF)
Hypofibrinogenaemia Vitamin K deficiency (II, VII, IX, X) Decreased clearance of degraded
coagulation factors
Hypercoagulability Decreased synthesis of naturalanticoagulant proteinsantithrombin (AT), proteins C, S and Z
Decreased clearance of activatedcoagulation factors
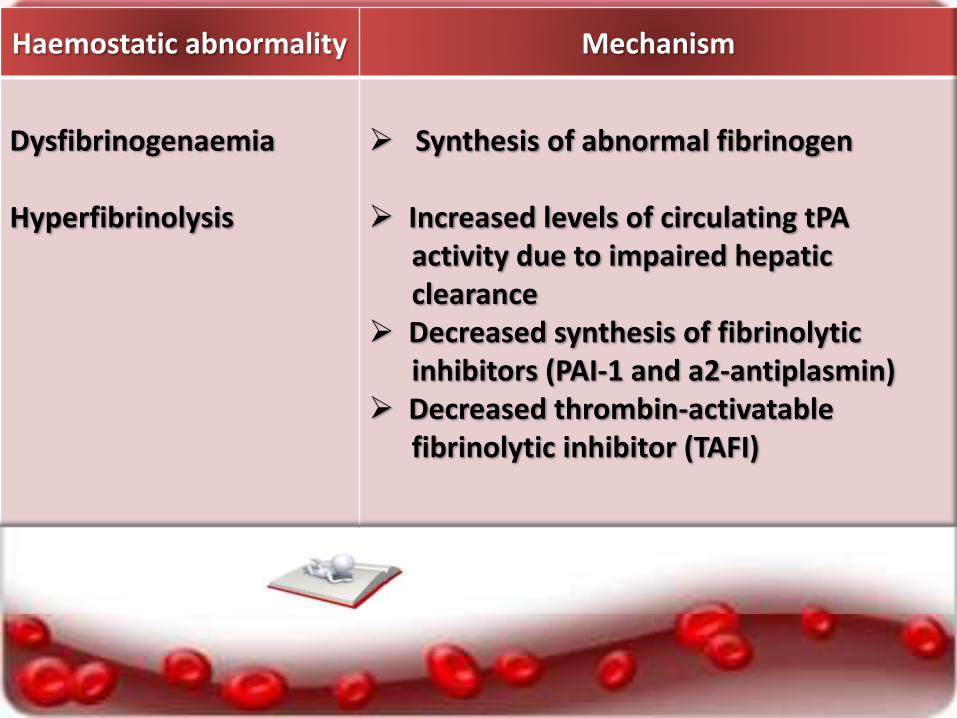
Haemostatic abnormality Mechanism
Dysfibrinogenaemia
Hyperfibrinolysis
Synthesis of abnormal fibrinogen
Increased levels of circulating tPAactivity due to impaired hepatic clearance
Decreased synthesis of fibrinolyticinhibitors (PAI-1 and a2-antiplasmin)
Decreased thrombin-activatablefibrinolytic inhibitor (TAFI)

Portal Vein Thrombosis
Prevalence of portal vein thrombosis:
• Lower than 1% in compensated cirrhosis.
• (10%–25%) of candidate for liver transplant.
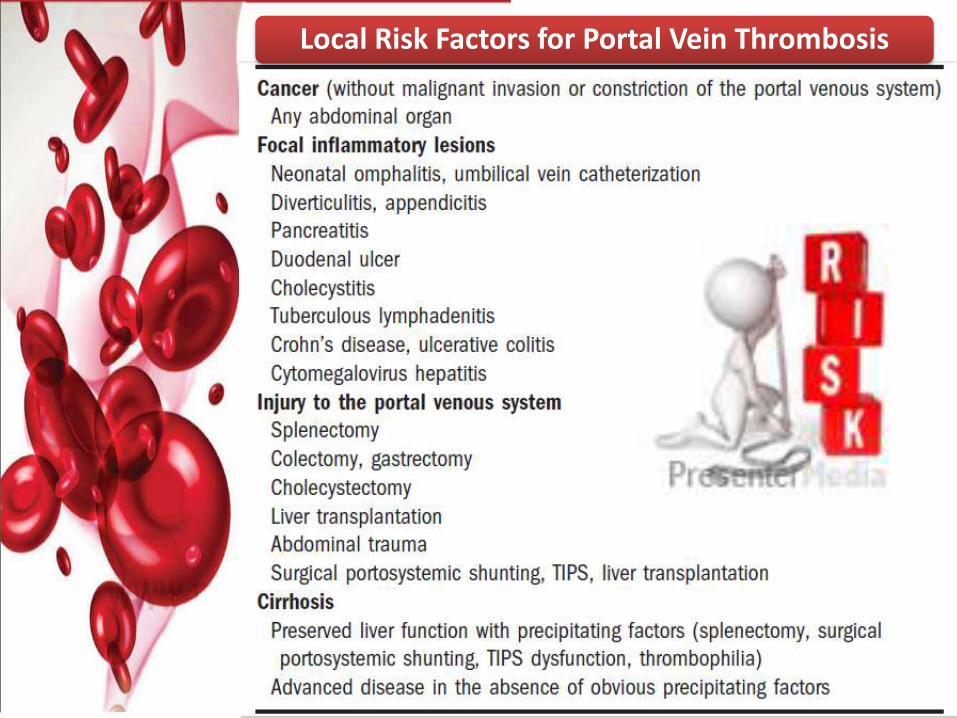
Local Risk Factors for Portal Vein Thrombosis
Risk factors for the development of PVT:
Decreased portal flow velocity.
Genetic prothrombotic factors
(i.e. MTHFR677-TT polymorphism)
leading to ↑ thrombin generation.
High FVIII combined with low
Protein C .
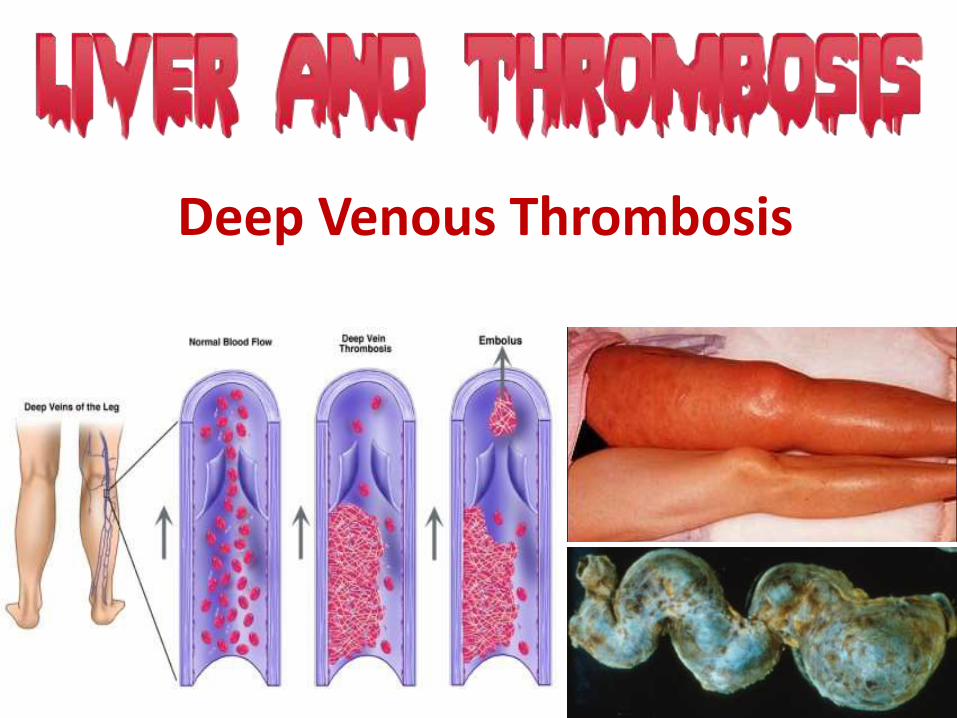
Deep Venous Thrombosis
Deep Venous Thrombosis
The incidence of DVT/PE ranges from 0.5% to 1.9%,
similar to patients without comorbidities.
Risk factors:
serum albumin level was independently
associated with the occurrence of thrombosis.
Gulley, et al. Deep vein thrombosis and pulmonary embolism in cirrhosis patients (2008).
Deep Venous Thrombosis
Gulley, et al. Deep vein thrombosis and pulmonary embolism in cirrhosis patients (2008).
Risk factors:
liver resection can unbalance the haemostatic equilibrium.
share the same risk factors as general population
such as venous stasis, infection, congestive heart failure,
acute respiratory disease, surgery (orthopaedic) and
immobilization.
Arterial Thrombosis
Hepatic artery thrombosis following liver
transplantation which worsen the prognosis.
It seems to be related to a hypercoagulable
state in the postoperative period.
Arterial Thrombosis
Patients with chronic liver disease could
develop atherothrombosis.
It is not clear if there is an increased risk of
coronary heart disease or stroke in these cases.

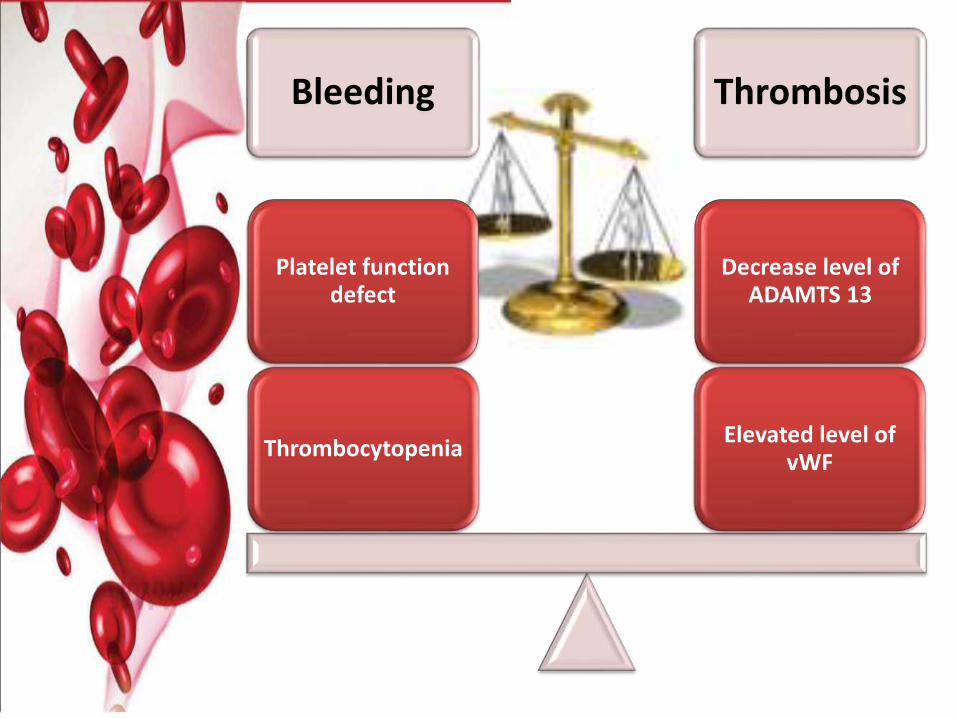
Bleeding Thrombosis
Decrease level of ADAMTS 13
Elevated level of vWF
Platelet function defect
Thrombocytopenia
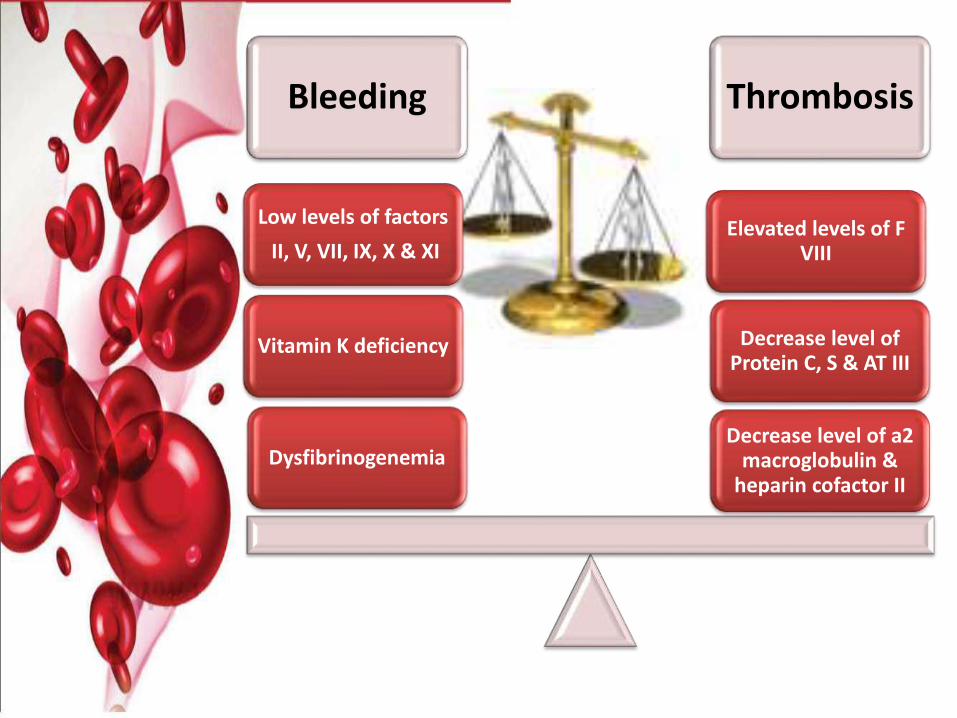
Bleeding Thrombosis
Decrease level of a2 macroglobulin &
heparin cofactor II
Decrease level of Protein C, S & AT III
Elevated levels of F VIII
Vitamin K deficiency
Low levels of factors
II, V, VII, IX, X & XI
Dysfibrinogenemia
Should we give thromboprophylaxisto patients with liver cirrhosis and coagulopathy?
Intrinsic pathway
Externsicpathway
X Xa
Fibrinogen Fibrin
Prothrombin Thrombin
AntithrombinIII
Degradation
Plasmin
Plasminogen
tPA
AntithrombinIII
Xa
Thrombin
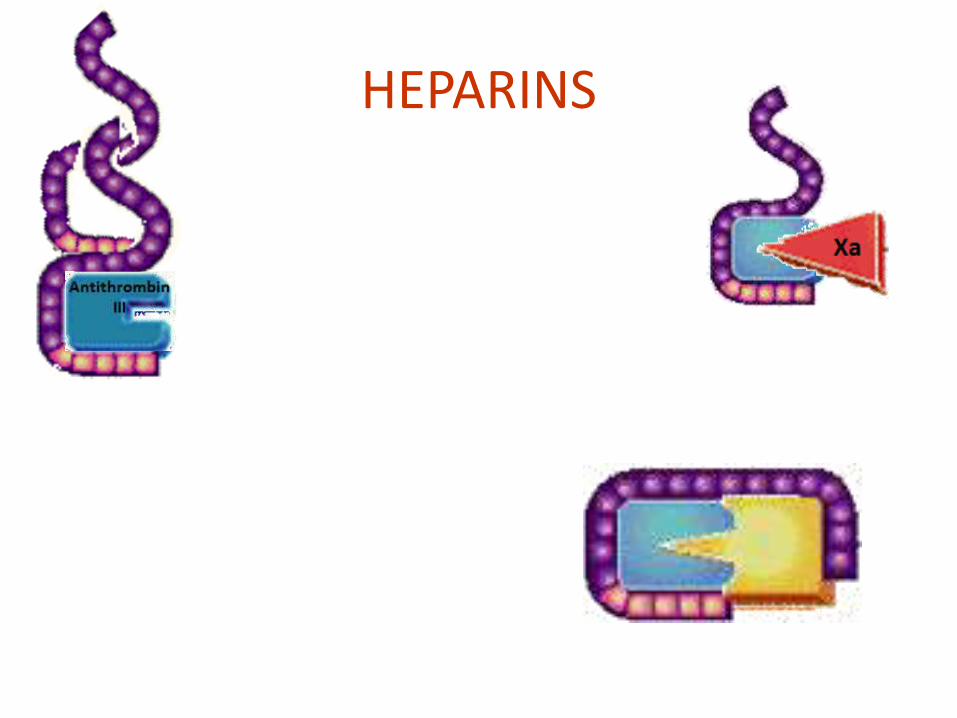
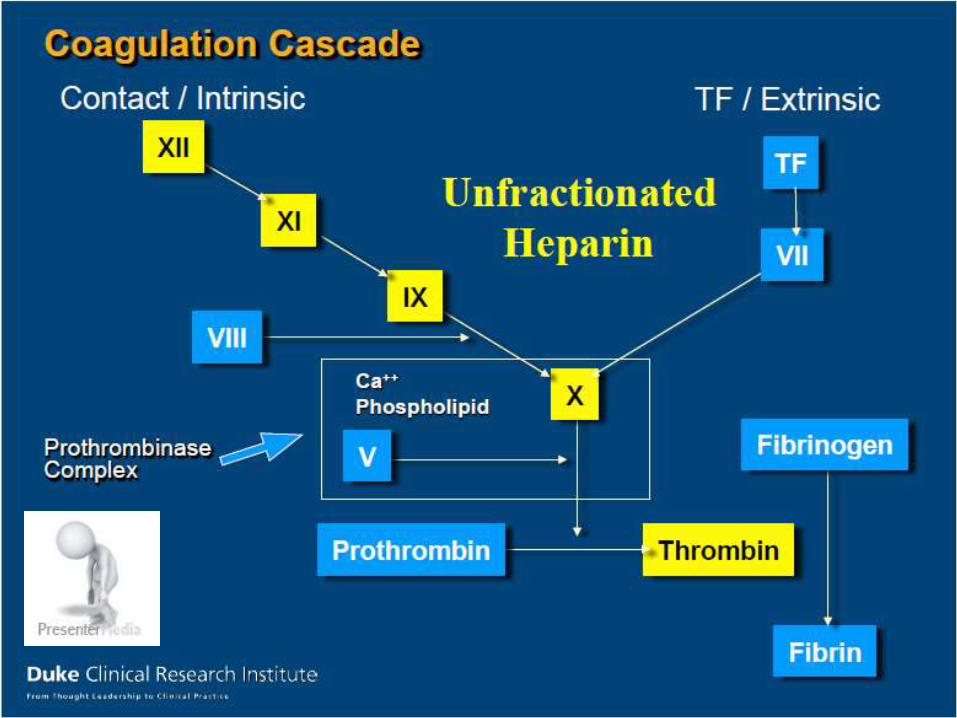
HEPARINS
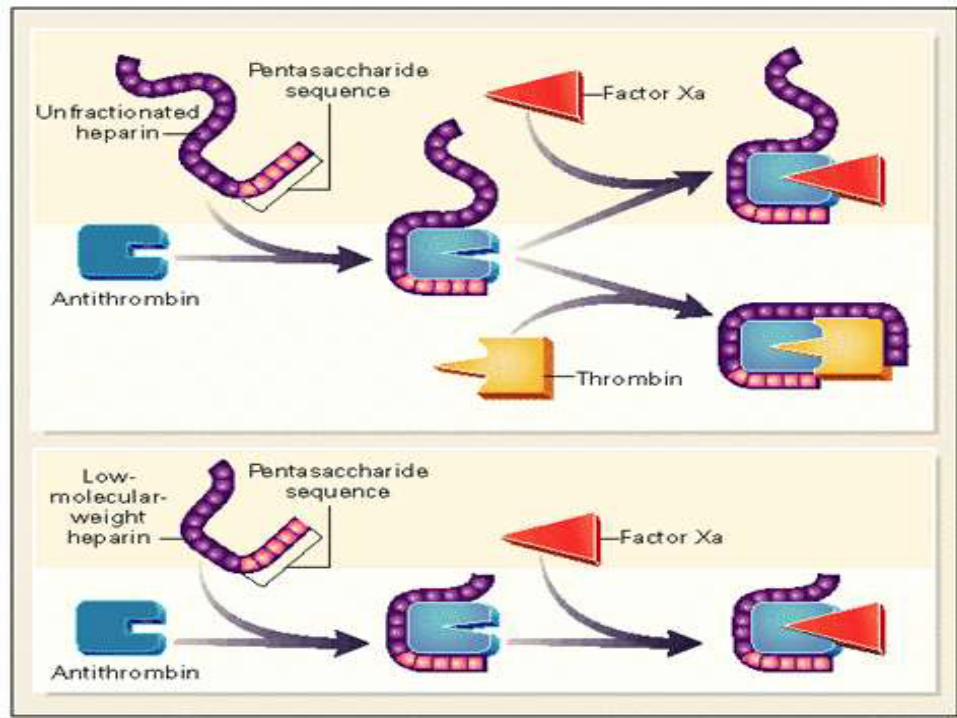
Unfractionated heparin
Inhibits thrombin by accelerating the activity of antithrombin.
Dose of heparinTreatment: 80 units/kg IV bolus (if desired)
then 18 units/kg/hr IV infusion. Check aPTT6 hours after bolus and adjust infusion to maintain aPTT within the therapeutic range established by the local laboratory. It is recommended to use an algorithm-based
dosing protocol
Prophylaxis: 5000 units sc q12hr (or q8hr if obese i.e. weight >120 kg).
Low Molecular Weight Heparin
Enoxaparin (Lovenox®)
Dalteparin (Fragmin®)
Tinzaparin (Innohep®)
Directly inhibits factor Xa activity
Dose of enoxaparin
Treatment: 1.5 mg/kg sc qday
or 1 mg/kg sc BID.
Prophylaxis: 40 mg sc qday
Low Molecular Weight Heparin Dose of dalteparin
Treatment: 200 units/kg sc qday Prophylaxis: 5000 units sc qday
Dose of tinzaparin Treatment: 175 units/kg sc qday Prophylaxis: 3500 units/kg sc qday
Monitoring Routine monitoring is not required for LMWHs Anti Xa levels in the following situations
Renal failureExtreme weightsPregnancyRecurrent thromboses on therapeutic doses
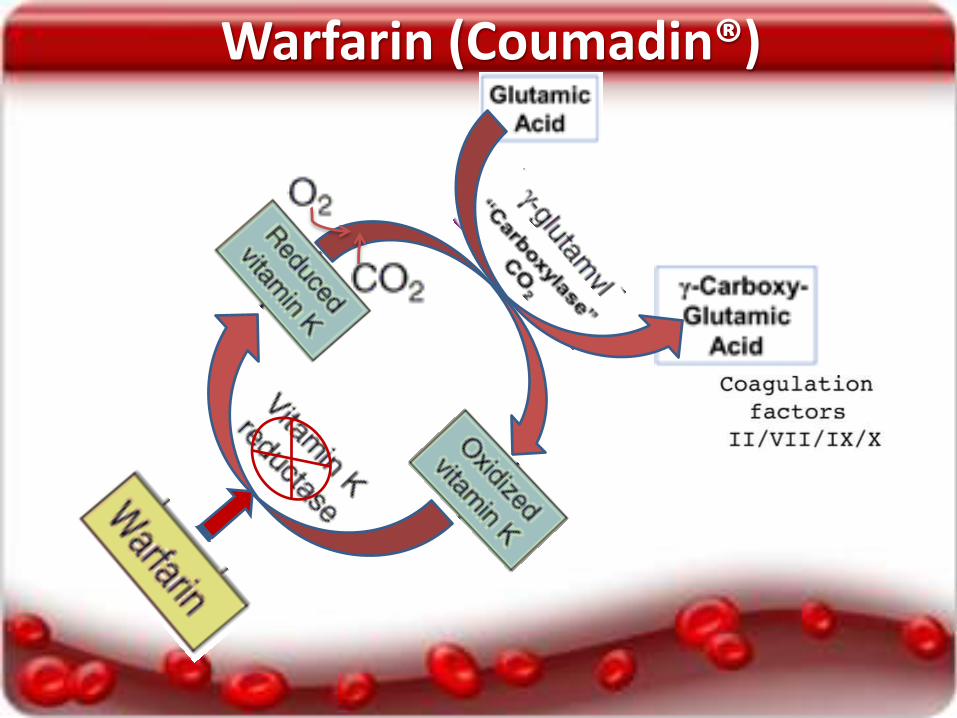
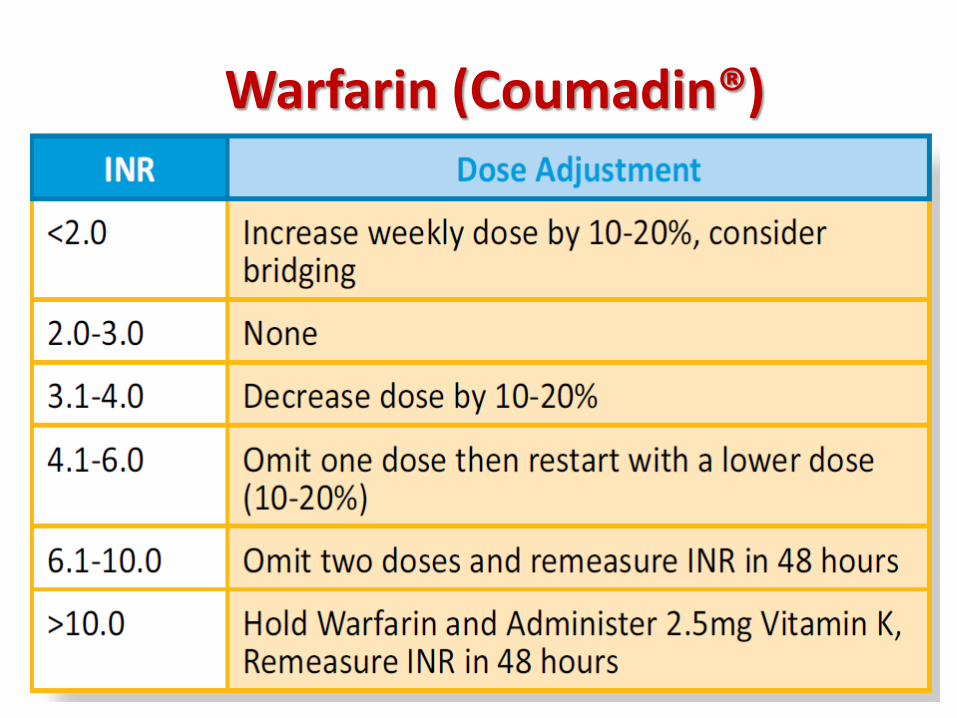
Warfarin (Coumadin®)
Warfarin (Coumadin®) Inhibits the proper synthesis of the vitamin K-
dependent clotting factors. Initiate warfarin at 5-10 mg po qday.
Consider lower doses in the elderly, patients with impaired nutrition, liver failure, congestive heart failure, or with a high risk of bleeding.
An initial INR should be done on Day 3. In the absence of any bleeding, the warfarin
dose should be adjusted based on the table below.
An INR should then be done every 3-4 days, until the INR is therapeutic and stable.
Warfarin (Coumadin®)

Management of Some Common Clinical Issues Related to
Coagulation in Liver Disease
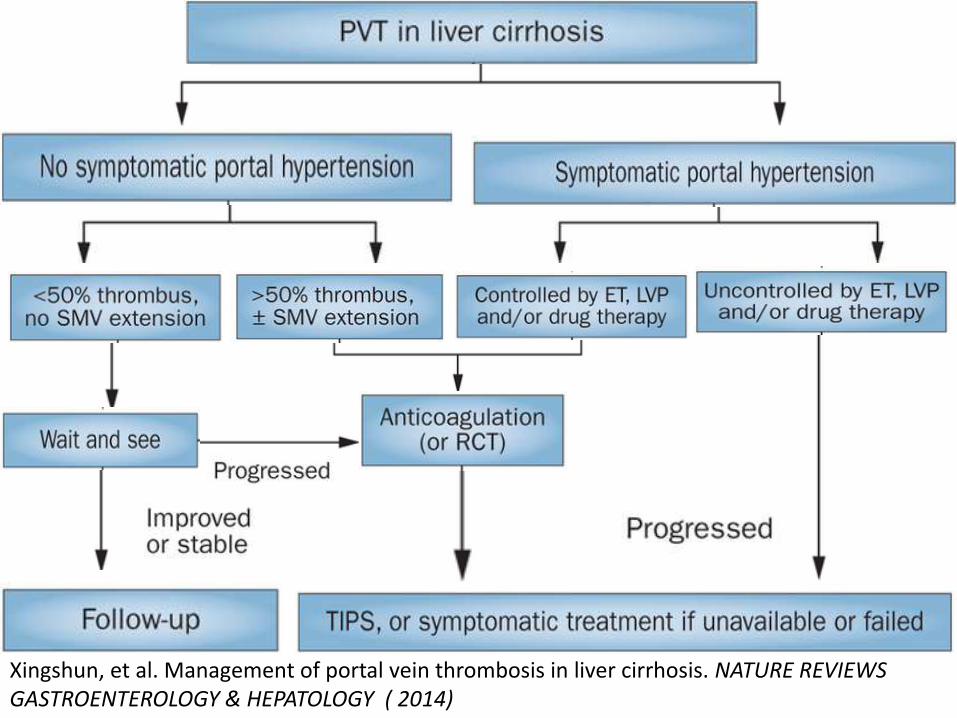
Xingshun, et al. Management of portal vein thrombosis in liver cirrhosis. NATURE REVIEWS GASTROENTEROLOGY & HEPATOLOGY ( 2014)
PVT
Acute or subacute PVT can betreated with therapeuticanticoagulation (LMWH) and mayprolong survival in these patients.
Esophageal varices should betreated aggressively endoscopicallybefore anticoagulation.
PATRICK , et al. Coagulation in Liver Disease: A Guide for the Clinician. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY (2013).
Currently available VKAs have a verynarrow therapeutic window incirrhosis patients and are problematicin patients with baseline elevated INR.
Patients with chronic PVT andcavernous transformation are less likelyto benefit from anticoagulation.
Premature discontinuation ofanticoagulation (before transplant) islikely to result in thrombus recurrence.
PATRICK , et al. Coagulation in Liver Disease: A Guide for the Clinician. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY (2013).
Deep vein thrombosis orpulmonary embolus
Consider medical prophylaxis in allhospitalized cirrhosis patients aswith any medical inpatient.
Medical therapy for acute VTEshould be with LMWH in therapeuticdoses similar to PVT treatmentunless contraindicated.
PATRICK , et al. Coagulation in Liver Disease: A Guide for the Clinician. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY (2013).
Do not assume the hospitalizedcirrhosis patient is “auto-anticoagulated” because the INR iselevated.
Presence of nonbleeding esophagealvarices should not preclude VTEprophylaxis.
PATRICK , et al. Coagulation in Liver Disease: A Guide for the Clinician. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY (2013).
Performance of invasiveprocedures
If high-risk procedure, transfuse
prophylactic platelets to a target of
at least 50–60 X 109/L or closer to
100 X 109/L for very high risk.
If postprocedural bleeding occurs
in mucosal sites or from puncture
wounds, consider hyperfibrinolysis.
PATRICK , et al. Coagulation in Liver Disease: A Guide for the Clinician. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY (2013).
Treat underlying disordersaggressively before electiveprocedures (infection, renal failure,etc).
Intranasal Desmopressin Acetate(DDAVP®) may be an effective andeconomical alternative prophylacticmeasure in procedures such as dentalextractions.
PATRICK , et al. Coagulation in Liver Disease: A Guide for the Clinician. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY (2013).
Do not use a moderately elevatedINR (3) as a measure of proceduralbleeding risk.
Avoid using FFP for prophylaxis, butif used, consider adequate dosing toreplace factors is 20–40 mL/kg .
PATRICK , et al. Coagulation in Liver Disease: A Guide for the Clinician. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY (2013).
• Do not use prophylactic transfusion of FFP or platelets in ALF without clinically evident bleeding.
CONCLUSION
• The liver plays major role inhemostasis.
• Liver disease affect all phases ofhaemostasis.
• Auto-anticoagulated.
• Rebalancing
• INR as single test doesn’tdetermine the true state ofcoagulation
CONCLUSION
• Consider the use ofthromboprophylaxis in cirrhoticpatients if there is a risk forthrombosis.
• There is a need to revise theguidelines regarding anticoagulationin this special population.
CONCLUSION
We suffers from a lack of accurate,reliable, and clinically availabletesting methods to properly assessthe true state of hemostasis.
Because some patients with chronicliver disease are predisposed forbleeding, some for hypercoagulation,and some in a stable balance.