Embed Size (px)
Citation preview

ANTIMICROBIAL RESISTANCE A Threat to Public Health
PresenterDr. Gaurav RajawatJunior Resident
ModeratorDr. Meenakshi KalhanProfessor
PT. B.D.SHARMA, PGIMS, ROHTAK

CONTENTS Overview Global concern Antimicrobial Resistance: Mechanism Antimicrobial Resistance: Causes New Delhi Metallo-Beta-Lactamase-1(NDM-1)/Super bug
Initiatives taken by India: AMR Surveillance, National AMR policy


Antimicrobial resistance (AMR) is the ability of a microbe to resist the effects of medication previously used to treat them.
DEFINITION
This broader term also covers antibiotic resistance, which applies to bacteria and antibiotics.

CAN A PERSON BECOME RESISTANT TO ANTIBIOTICS ?NO
Antimicrobial resistance (AMR) is a property of the microbe, not of a person or other organisms infected by a microbe.

EVOLUTION OF ANTIBIOTIC RESISTANCE

There are definitepolicies/guidelines for appropriate use of antimicrobials at national level in specific national health programmes being run in the country e.g. RNTCP, National AIDS Control Programme, etc.
But for other diseases of public health importance like enteric fever, diarrhoeal disease, respiratory infections, etc individual hospitals are following their own antimicrobial policies and hospital infection control guidelines.
To monitor antimicrobial resistance it is necessary to have regulations for use and misuse of antibiotics in the country.

The Centers for Disease Control and Prevention (CDC) estimates more than two million people are infected with antibiotic-resistant organisms, resulting in approximately 23,000 deaths annually in the United States, costing $20-$35 billion annually.
In Europe, an estimated 25,000 deaths are attributable to antibiotic-resistant infections, costing €1.5 billion annually.
In India, it is estimated that 58,000 neonatal sepsis deaths are attributable to drug resistant Infections.
ANTIMICROBIAL RESISTANCE: GLOBAL CONCERN
Center for Disease Dynamics, Economics & Policy, 2015.

ANTIMICROBIAL RESISTANCE: GLOBAL CONCERNThree agents of greatest concern associated with both hospital- and community acquired infections. E-coli Klebsiella pneumoniae Staphylococcus aureus
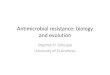
WHO 2014, reported E. coli resistance of more than 50 % fluoroquinolones and 3rd gen. cephalosporins.K.pneumoniae resistance rates to 3rd generation cephalosporins exceed 30-60%.MRSA resistance rates exceed 20-80%.
Percentage of Staphylococcus aureus isolates that are
methicillin resistant (MRSA), by country (2011-14)

ANTIMICROBIAL RESISTANCE: GLOBAL CONCERN
Between 2000 and 2010, total global antibiotic consumption grew by more than 30 percent, from approximately 50 billion to 70 billion standard units.
In most countries, about 20 percent of antibiotics are used in hospitals and other healthcare facilities, and 80 percent are used in the community, either prescribed by healthcare providers or purchased directly by consumers or caregivers without prescription.
Center for Disease Dynamics, Economics & Policy, 2015.

The countries consuming the most antibiotics overall in 2010 were India, 13 billion SU; China, 10 billion SU; and the United States, 7 billion SU.
However, in per capita terms among these countries, the United States led in 2010 with 22 SU per person, compared with 11 SU in India and 7 SU in China.
ANTIBIOTIC CONSUMPTION: WORLD

TOTAL ANTIBIOTIC CONSUMPTION IN SELECTED COUNTRIES, 2000 AND 2010WHO study, 2011 showed that 53% of Indians were
taking antibiotics without a prescription.
Center for Disease Dynamics, Economics & Policy, 2015.

Mechanism Antibiotic Resistance
Intrinsic (Natural) Acquired
Genetic Methods
Chromosomal Methods Mutations
Extra chromosomal Methods Plasmids

ANTIMICROBIAL RESISTANCE: MECHANISM
Bacteria resist the effects of antibiotics by using the following genetic strategies, with thousands of variations: Producing destructive enzymes to neutralize antibiotics.
Modifying antimicrobial targets, by mutation, so that drugs cannot recognize them.
Removing antimicrobial agents by pumping them out (efflux).
Preventing antibiotics from entering by creating a “biofilm” or otherwise reducing permeability.
Creating by passes that allow bacteria to function without the enzymes targeted by antibiotics.
Source: Penesyan et al. (2015)

CAN BACTERIA LOSE THEIR RESISTANCE CAPACITY?
Antibiotic resistance traits can be lost, but this reverse process occurs more slowly.
If the selective pressure that is applied by the presence of an antibiotic on the bacterial population is removed, they can potentially go back to a population of bacteria that responds to antibiotics
Yes
Mira PM, Crona K, Greene D, Meza JC, Sturmfels B, Barlow M (2015) Rational Design of Antibiotic Treatment Plans: A Treatment Strategy for Managing Evolution and Reversing Resistance. PLoSONE 10(5): e0122283. doi:10.1371/journal.pone.0122283

CAUSES OF ANTIMICROBIAL RESISTANCE1. Inappropriate use & misuse of
antibiotics
2. Indiscriminate use of antibiotics in agriculture and veterinary practice
3. Insufficient research and development

INAPPROPRIATE USE OF ANTIBIOTICS
Three main types of misuse as underlined by the European Centre for Disease Prevention and Control (ECDC) :
The unnecessary prescription of antibiotics for viral infections.
Frequent prescription of “broad-spectrum antibiotics”, instead of better targeted antibiotic.
Patient failure to adhere to regimens for prescribed antibiotics.

SELECTIVE PRESSURE

INAPPROPRIATE USE OF ANTIBIOTICS
Practical Guide to ANTIMICROBIAL STEWARDSHIP in hospitals.pdf 2015

INSTANCES OF IRRATIONAL DRUG USE
No drug needed e.g. unnecessary & ineffective antimicrobials or antidiarrhoeals given instead of Oral Rehydration Solution.
Unsafe drugs e.g. Analgin (Dipyrone) banned in most developed countries, but is used in many developing countries.
Under use of available effective drugs e.g. ORS not used effectively.

INSTANCES OF IRRATIONAL DRUG USE
Ineffective drugs & drugs with doubtful efficacy e.g. unnecessary excessive use of tonics & multivitamin preparations.
Incorrect use of drugs e.g. overuse of Injections
Many viral infection (sore throat, sinusitis, conjunctivitis etc ) does not need antibiotics for treatment.

INDISCRIMINATE USE OF ANTIBIOTICS IN AGRICULTURE AND VETERINARY PRACTICE
Antibiotic-resistance genes are used in genetically modified crops.
Antibiotics are also sprayed onto fruit trees to prevent and treat infection.
The use of antibiotics in feed supplements given to farm animals to promote animal growth and to prevent infections (rather than cure infections).An estimated 80 percent of all antibiotics consumed
in the United States are used in food animals (U. S. FDA 2010).

TRANSMISSION

INDISCRIMINATE USE OF ANTIBIOTICS IN AGRICULTURE AND VETERINARY PRACTICEThe use of the antibiotic avoparcin as a growth promoter in food animals in Europe resulted in the development and amplification of Vancomycin Resistant Enterococci (VRE) and subsequent colonization in human intestine.
Enerofloxacin was approved for use in food production animals in many countries. The use of this antibiotic in food animals has resulted in the development of ciprofloxacin-resistant strains of Salmonella spp. and Campylobacter spp.
The use of animal feed supplements with the antibiotic tylosin has led to the development of erythromycin-resistant streptococci and staphylococci.
European Union (EU) has banned the use of animal growth promoting antibiotics (tylosin, spiramycin, bacitracin and
virginiamycin)

INDISCRIMINATE USE OF ANTIBIOTICS IN AGRICULTURE AND VETERINARY PRACTICE
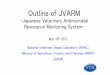
Global antibiotic consumption in livestock was conservatively estimated at 63,200 tons in 2010, accounting for nearly two-thirds of the estimated 100,000 tons of antibiotics produced annually worldwide.
By 2030, consumption is projected to rise by two-thirds, to 105,600 tons. Two-thirds of the increase is due to increase in the number of animals, and the remaining one third is due to the shift from extensive to intensive farming .
Center for Disease Dynamics, Economics & Policy, 2015.

Center for Disease Dynamics, Economics & Policy, 2015.
Antibiotic Consumption In Livestock, Top Ten Countries 2010–2030 (projected for 2030)

INDISCRIMINATE USE OF ANTIBIOTICS IN ANIMAL HUSBANDRY: INDIAN SCENARIO
Non-therapeutic uses of antibiotics common in poultry production. However, currently there is no regulatory provision regarding the use of antibiotics in livestock.
The prescribed tolerance limit (mg/Kg) of antibiotics use shall not exceed for sea foods including shrimps, prawns or any other variety of fish and fishery products (The Prevention of Food Adulteration Rules, 1995-part XVIII)
a) Tetracycline (0.1) mg/Kg b) Oxytetracycline (0.1) mg/Kgc) Trimethoprim (0.05) mg/Kgd) Oxolinic acid (0.3) mg/Kg

LEGISLATION ON ANTIBIOTICS AS GROWTH PROMOTERS
Center for Disease Dynamics, Economics & Policy, 2015.

WATER POLLUTION Industry uses larges volumes of
detergents and disinfectants - including quaternary ammonium compounds (QACs) - known together as biocides
Nearly all domestic cleaning products and shampoos also contain QACs.
They wash out in large volumes with the waste water from factories and homes.
QAC resistance genes are significant because they are often located with antibiotic resistance genes on the same piece of DNA, so exposure to one will co-select for the other.

INSUFFICIENT RESEARCH AND DEVELOPMENT
Pharmaceutical industries do not consider antibiotic development as an economically wise investment as antibiotics are used for relatively short duration.
Antibiotics are not as profitable as drugs that treat chronic conditions, such as diabetes, asthma, psychiatric disorders.
Fast development of resistant strains also making antibiotic ineffective soon

INSUFFICIENT RESEARCH AND DEVELOPMENT

INSUFFICIENT RESEARCH AND DEVELOPMENT
4. Regulatory approvals–
Red tapism, no clear rules and regulations
Differences in clinical trial requirements among countries
Changes in regulatory and licensing rules.

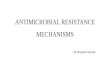
NO. OF ANTIBACTERIAL DRUGS APPROVED VS YEAR OF INTERVALS

NEW DELHI METALLO-BETA-LACTAMASE-1(NDM-1)(SUPERBUG)
New Delhi Metallo-beta-lactamase 1 (NDM-1) is a genetic element with multiple resistance genes that can be harbored by and transmitted between Gram-negative bacteria.
NDM-1 was first described by Yong et al in 2009.
http://aac.asm.org/content/53/12/5046.full?view=long&pmid=19770275

NAMING NEW DELHI METALLO BETA -LACTAMASE
It was first identified in a Swedish patient returning from New Delhi, India, in 2008.
The infection was unsuccessfully treated in a New Delhi hospital and after the patient's repatriation to Sweden, a carbapenem-resistant Klebsiella pneumoniae strain bearing the novel gene was identified.
The authors concluded that the new resistance mechanism "clearly arose in India, but there are few data arising from India to suggest how widespread it is

WHY (NDM-1) WAS IN NEWS?
In Aug,2010 a study by a multi-national team was published in a journal ’The Lancet Infectious Diseases’ which reported many NDM-1 resistance cases in India.
The authors concluded that India should be avoided for elective and cosmetic surgeries because of NDM-1 bacterial strain

This reported 37 cases isolates with NDM-1 in the United Kingdom, 44 in Chennai, 26 in Haryana, and 73 in various other
sites in Pakistan and India.
An environmental point prevalence study conducted between 26 September and 10 October 2010 found bacteria with the NDM-1
gene in drinking water and seepage samples in New Delhi. (Johnson and Woodford 2013)

NDM-1: THE LANCET NAMING APOLOGY
On 12 January 2011, the editor of The Lancet, Richard Horton, apologized and acknowledged that naming a superbug after New Delhi was an "error".“
Following this, Ajai R. Singh, editor of Mens Sana Monographs, demanded that such 'geographic names giving' be abandoned and replaced by 'scientific name giving'.
He proposed changing NDM-1 to PCM (plasmid-encoding carbapenem-resistant metallo-beta-lactamase)
Furthermore name is not changed yet and follows the naming of most genes of this type.
• VIM: Veronna imipenemase in Italy• GIM: Germany imipenemase• DIM: Dutch imipenemase

WHY IS NDM-1 DANGEROUS? The World Health Organisation (WHO) –“NDM-1 could be ushering in the dooms day scenario of a world without antibiotics.“
The NDM-1 gene causes bacteria to produce an enzyme called a carbapenemase.
Carbapenemase makes nearly every antibiotic ineffective including Carbapenems.

CAN NDM-1 BE TREATED ? At the moment, the only way to combat the spread of NDM-1 is through quickly identifying, isolating infected patients, disinfecting hospital equipment, following hand-hygiene procedures and surveillance in hospitals.
Patients with NDM-1-related infections have been treated with a combination of medications, but there is no effective treatments are available for many of the infections caused by NDM-1.

COMBATING ANTIBIOTIC RESISTANCE
Better hygiene -preventing infections from happening in the first place.
To have access to safe water. Infection control in health-care facilities. Vaccination- to reduce the need for antibiotics. To have national action plans on AMR. Greater innovation and investment are required in research and development of new antimicrobial medicines, vaccines, and diagnostic tools.

1. 12th Five Year Plan- Containment of AMR 2. The National Policy for Containment of Antimicrobial
Resistance3. National Anti-Microbial Resistance Research and
Surveillance Network (AMRRSN)4. Jaipur declaration (a WHO initiative)5. Chennai declaration6. The Drugs and Cosmetic Rule, 1945 were amended
in 2013 to include a new Schedule H1.7. National Treatment Guidelines for Antimicrobial Use
in Infectious Diseases
.
INITIATIVES TAKEN BY INDIA WITH RESPECT TO AMR

INITIATIVES TAKEN BY INDIA WITH RESPECT TO AMR8. 2016 February, the Union Health Minister
launched a multimedia campaign called “Medicines with the Red Line” to create awareness on the rational use of medicines which carry a red line on their strip
AUG. 2016

MEDICINES WITH THE RED LINE: A AWARENESS CAMPAIGN 2016

12TH FIVE YEAR PLAN: CONTAINMENT OF AMR A National Programme for containment of AMR has been initiated with the following objectives:- To generate awareness among healthcare providers and in the people regarding rational use of antibiotics.
To establish a laboratory based surveillance system.
To strengthen infection control guidelines and practices and
To promote rational use of antibiotics

Released in 2011 & yet to be implemented Key points-a) Proposed Actions to monitor Sale of
Antibioticsb) Set up an Antibiotic Management Team
(AMT)c) Establishment of inter-sectoral
coordination committeed) Reducing antibiotic selection pressures
by appropriate control measurese) Promotion of discovery of newer and
effective antimicrobials based on current knowledge of resistance mechanisms
THE NATIONAL POLICY FOR CONTAINMENT OF ANTIMICROBIAL RESISTANCE

INITIATIVES TAKEN BY INDIA WITH RESPECT TO AMR
a) Proposed Actions to monitor Sale of Antibiotics
Schedule H of the drug and cosmetics act contains a list of drugs which are required to be dispensed on the prescriptions of a registered medical practitioner.
A separate schedule as Schedule H1 may be introduced under the Drugs and Cosmetics Rules to regulate sale of antibiotics exclusively.
A provision could be incorporated for spot suspensions /cancellation of the sale license for contravention of the provision of Schedule H1

INITIATIVES TAKEN BY INDIA WITH RESPECT TO AMR
b) Set up an Antibiotic Management Team (AMT) – This is a Multi disciplinary team with experts in Infectious diseases, Internal medicine, Clinical microbiology etc
The functions of the AMT is to develop the hospital antimicrobial policy.
c) Establishment of inter-sectoral coordination. Central Council for Scientific and Industrial Research Ministry of Health and Family Welfare, Indian Council for Agricultural Research Department of Animal Husbandry .

ANTIMICROBIAL SURVEILLANCE SYSTEM: INDIA The Indian Council of Medical Research began setting up the Anti-Microbial Resistance Surveillance Network in 2011.
When complete, its focus will be on: 1. Diarrhea (e.g.,Shigella, Vibrio cholerae)2. Enteric fever (e.g., Salmonella Typhi , S. Paratyphi)3. Sepsis caused by Enterobacteriacea (e.g., E-coli,
Klebsiella pneumoniae)4. Gram-negative organisms (e.g., Pseudomonas
aeruginosa, Acinetobacter baumannii)5. Gram-positive bacteria (e.g.,MRSA and VRE)6. Fungal infections (e.g., Candida spp.), and7. Respiratory pathogens (e.g., Streptococcus
pneumoniae).

DESIGN FOR AMR SURVEILLANCE 1. Identification of the pathogens / diseases of
public health importance for surveillance- Extended Spectrum- lactamases [ESBLs] and Metallo -lactamases [MBLs], NDM-1, MRSA & VRE
2. Creating a network of AST laboratories- In the first phase, the following three central Govt. Hospital in Delhi will be included for AMR surveillance.
a) Sucheta Kriplani Hospital (SKH) & Lady Hardinge Medical College (LHMC), New Delhi
b) Dr Ram Manohar Lohia (RML) Hospital, New Delhic) Vardhman Mahavir Medical College (VMMC) and Safdarjung
Hospital, New Delhi

3. Standardize methodology for microbial identification and AST- Laboratories should be having expertise to do MRSA, ESBL and Carbapenemase (Modified Hodge test / Imipenem + EDTA E test) testing.
4. AST Data analysis - WHONET 5 for AST data reporting and analysis
5. Dissemination of AMR data- The AMR data generated by the respective network laboratories should be sent to the coordinating center, regularly on a quarterly basis.
6. Development of National Repository of Bacterial strains / cultures - Institute of Microbial technology (IMTECH), Chandigarh has the requisite infrastructure and expertise to do the same.
DESIGN FOR AMR SURVEILLANCE

THE ACTION PLAN FOR AMR SURVEILLANCE:
A one day sensitization workshop for the senior microbiologists of the network laboratories.
2-3 days training workshop for junior microbiologist/ data reporting personnel on various aspects of AST specially quality control and data analysis/ transmission.
Followed by regular monitoring and review meetings once in 6/12 months

RESEARCH IN AMR SURVEILLANCE New and simple surveillance tools with the capability to detect AMR at the lowest capable health centre should be developed and its ability to track the infection should be established.
All surveillance activities should be linked with epidemiological studies particularly surveillance around relevant vaccination programs.
A National Health Policy Unit should be entrusted with analysis of the surveillance data and provide advisory for framing of policies for use of antibiotics according to region, nation or hotspots.

THE DRUGS AND COSMETIC RULE, 1945 WERE AMENDED IN 2013 TO INCLUDE A NEW SCHEDULE H1.
The drug testing laboratories in the country should be strengthened in terms of infrastructure, number and also training of drug inspectors.
The supply of a drug mentioned in Schedule H1 shall be recorded in a separate register at the time of the supply.
It contains the name and address of the prescriber, the name of the patient, the name of the drug and the quantity supplied and such records shall be maintained for three years and be open for inspection.

THE DRUGS AND COSMETIC RULE, 1945 WERE AMENDED IN 2013 TO INCLUDE A NEW SCHEDULE H1.
The drug specified in Schedule H1 shall be labeled with the symbol Rx which shall be in red and clearly displayed on the left top corner of the label, and shall also be labeled with drug warning.
Drug Inspectors may conduct surprise raids at the chemist shops to ensure that the provision of the Drugs and Cosmetics Rules especially in respect of Schedule H1 are strictly complied by the licensees.

THE DRUGS AND COSMETIC RULE, 1945 WERE AMENDED IN 2013 TO INCLUDE A NEW SCHEDULE H1.
Incentives should be given to pharmacies for not selling antibiotics without prescription and appropriate regulation for the same should be formulated.
Appropriate steps will be taken to curtail the availability of fixed dose combination of antibiotics in the market, by and large combinations should be discouraged except for naturally interactive ones like Cotrimoxazole, Amoxyclave, etc.

NATIONAL CAMPAIGNS: BEST PRACTICES Two of the best known national campaigns took place in France and Belgium.
In France, which once had the highest rate of antibiotic consumption in Europe, the government launched an awareness campaign called “Antibiotics are not automatic” in 2001, as a part of a program to preserve antibiotic effectiveness.
This campaign achieved a reduction in antibiotic prescribing of 27 percent over five years in all regions of the country, with the greatest decline, 36 percent, in children 6 to 15 years of age.
Belgium, the Belgian Antibiotic Policy Coordination Committee established a national media campaign in 2000 that succeeded in reducing antibiotic prescribing by 36 percent over seven years.

DRUG DIVISION: HARYANA Drug division of Haryana has worked for promotion of rational use of Medicines during the 2012-2013
Activities-a. Prescription auditsb. Trainings and workshops on rational drug usec. Publication of material on rational drug use 3. Audit of drug stores 4. Setting up Centralized Medicine Testing Unit.

DRUG DIVISION HARYANA: FINDINGS Incomplete format of Prescriptions- In 58% prescriptions, all drugs were written in generic names. In 27% of prescriptions a mix of generic and brand naming of drugs were used.
Polypharmacy- It was found that the number of drugs prescribed per encounter in hospital was 3.4 and higher than the WHO recommended values of 1.6-1.8
Treatment was incomplete in respect of dosage form, strength, frequency and duration of the treatment.

DRUG DIVISION HARYANA: FINDINGS No mention of drug strength - In 71% prescriptions, none of the drugs that were prescribed mentioned the strength.
Overuse of analgesics and antibiotics- 54 % prescriptions were having antibiotics as compared to the WHO standard of 15-25%. While, 57% of the prescriptions were having analgesics.

• Using antibiotics, prescribed by a doctor• Completing the full antibiotic course, even if they feel
better• Not sharing antibiotics with others or using leftover
prescriptions.• Public health education and awareness • Stopping the use of antibiotics as growth-promoters in
farm animals.
People
• Enhancing infection prevention and control• Prescribing and dispensing antibiotics only when they
are truly needed, after antibiotic sensitivity testing, when possible.
• Prescribing and dispensing the right antibiotics to treat the illness.
• Ban on over- the counter sale of antibiotics• Compliance with rules and regulations
Health workers and pharmacists
How to tackle resistance- Contribution from all stakeholders

• Having national plans and guidelines on antimicrobial resistance
• Strengthening resistance tracking and laboratory capacity;
• Regulating and promoting appropriate use of medicines.
• Increase spending on innovation and infrastructure
Policymakers
• Promoting innovation and research and development of new tools
• Promoting Cooperation and Information Sharing Among all Stakeholders.
Industry
Cont..


SUGGESTED READING National policy for containment of antimicrobial
resistance India 2011.Pdf Global action plan on antimicrobial resistance 2015.pdf Center for Disease Dynamics, Economics & Policy,
2015.pdf HSHRC Annual Report 2012-13.pdf