Embed Size (px)
DESCRIPTION
Information on new anticoagulant drugs
Citation preview

Approach to the newer anticoagulants
Dr Melita KenealyConsultant Haematologist

Pradaxa (dabigatran)
• RE-LY trial – >18,000 pts non valv
AF + RF cf warfarin– Rate of stroke or sys
embolism (%/yr) • 1.54 (110mg),
1.11(150mg), 1.71(warfarin)
– similar major bleeding • less ICH, less life
threatening, more major GI bleed
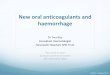
STROKE OR SYSTEMIC EMBOLISM (SSE)
Error bars = 95% CI; BID = twice daily.Dabigatran etexilate is not approved for clinical use in stroke prevention in atrial fibrillation outside the US and Canada.Connolly SJ, et al. N Engl J Med 2010;363:1875-1876.
0.50 0.75 1.00 1.25 1.50
SuperiorityP value
Non-inferiorityP value
Hazard ratio
Dabigatran110 mg BIDvs. warfarin
<0.001 0.30
Mar
gin
=1.
46
<0.001Dabigatran150 mg BIDvs. warfarin
<0.001
PFP stopped early due to bleeding concernsCriticisms – lack of stakeholder involvement

Xarelto (rivaroxaban)
• ROCKET-AF (stroke and systemic embolism)– N=14,264 v warfarin– Noninf efficacy HR 0.79 (0.66-0.96)– Bleeding similar
• EINSTEIN-DVT (acute sympto DVT)– N=3449 v clexane/warfarin 3-12mths– Noninferior efficacy HR 0.68 (0.44-1.04)– Similar major/sympt non-major bleeding rates 8%
PFP about to be rolled outHave they learnt from others’mistakes??


PRADAXA (DABIGATRAN) XARELTO (RIVAROXABAN)
ACTION Direct thrombin inhibitor Factor Xa inhibitor
PK Peak 0.5-2hT1/2 12-17h85% renal excrP-gp interactions35% protein bound
Peak 2-4hReduced bioavail fasting T1/2 11-13hHighly protein bound, predom renal excretion, some metabCYP3A4, P-gp interactions
INDICATION Approved VTE proph (PBS) and nonvalv AF+RF
Approved VTE proph (PBS), AF and treatment DVT/PE
DOSE AF 150bd oral but reduce dose to 110bd if any other RF (age>75, antiplt/NSAID CrCl 30-50) CI if CrCl<30VTE proph 150-200mg/d
AF 20mg/d (15mg CrCl30-50)DVT 15mgbd 3w then 20mg/dIf CrCl 15-29ml/min 10mg/dVTE proph 10mg/d
MONITORING Not required BUT difficult.APTT nonlinear, Rx x1.5-2.0TCT(sens,linear), Hemoclot
Not required but difficultAPTT, PT long but nonlinearChromogenic antiXa
PERIOP Mx CrCL>50 stop 2+ daysCrCl 30-50 stop 3-5d
*Withdraw 12-24hrs

Pradaxa peri-op

PRADAXA (DABIGATRAN) XARELTO (RIVAROXABAN)
REVERSAL None provenStop drug
Charcoal <2hDialysable
Can try:PlateletsAntifibrinolyticsFFPProthrombinexrFVIIa
None provenStop drug
Charcoal<8hNot dialysable
PTX reversed coag tests in healthy volunteers
Can try:PlateletsAntifibrinolyticsFFPProthrombinexrFVIIa

Management of bleeding

Summary
• New agents useful in subgroup of patients • No simple test to establish anticoagulant effect• Management of bleeding– Resuscitate, treat source, stop drug, call
haematologist!– No effective means of reversal, but short t1/2