Embed Size (px)
Citation preview

ARRHYTHMIAS Dr. Rashad Siddiqi FCPS (Anaesthesiology), FCPS (Cardiothoracic Anaesthesia)
Associate Prof of Anaesthesiology CMH Lahore Medical College
Consultant Cardiac Anaesthetist Army Cardiac Center Lahore

Learning Objectives
Etiology and recognition of common peri-operative arrhythmias
Review management of cardiac arrhythmias, with a focus on the relevant recent literature

Implies normal sequence of conduction, originating in the sinus node and proceeding to the ventricles via the AV node and His-Purkinje system.
ECG Characteristics: Regular narrow-complex rhythm
Rate 60-100 bpm
Each QRS complex is proceeded by a P wave
P wave is upright in lead II & downgoing in lead aVR
Normal Sinus Rhythm

Mechanisms of Arrhythmia
Arrhythmias
Altered Automaticity
Ectopic Foci
Reentry / Conduction
Block

Bradyarrhythmias

Sinus Bradycardia
Decreased Automaticity

Normal Sinus Bradycardia
Occurs in normal children and adults (as low as 30/min during sleep)
May also be seen in the absence of heart disease: At rest, in 25 - 35% of asymptomatic individuals < 25 yrs
age In well-conditioned athletes In some elderly patients As a manifestation of a rare familial syndrome (mutation
in HCN4, one of a family of pacemaker ion channel genes)

Hypoxia, Hypothermia, Hypothyroidism Intrinsic disease of the SA node (e.g. sick sinus syndrome) Drugs:
Digoxin Beta-blockers Quinidine Adenosine Calcium channel blockers
Seizure (post-ictal) Infection like Diphtheria, acute rheumatic fever, viral
myocarditis Increased intracranial pressure (cushing’s reflex) Electrolyte imbalance e.g., hyperkalemia
Sinus Bradycardia - Causes

Maintain airway; supplemental O2 (if hypoxic) IV access 12 lead ECG (if available)
Trea
tmen
t of B
rady
card
ia
Assess appropriateness for clinical condition HR typically less than 50 bpm
Hypotension? Acutely altered mental status? Signs of Shock? Ischemic chest discomfort? Acute Heart failure?
Atropine 0.5mg IV; or TransCutaneous Pacing; or Dopamine / Adrenaline infusion
Monitor & Observe
NO
YES

Bradycardia during Anaesthesia
• Drugs - inhalational agents - suxamethonium - induction agents - neostigmine
• Airway - hypoventilation - hypoxia
• Vagal reflexes • Regional anaesthesia
• Surgical factors - IVC compression - pneumoperitoneum
• Undetected blood loss • Cardiac Event
- tension pneumothorax - haemothorax - tamponade - myocardial depression

Rhythms due to Conduction Block

1st Degree AV Block
ECG Characteristics: Prolongation of the PR interval, which is constant
All P waves are conducted
Usually benign but such patients are at higher risk of developing AF or CCF
Treatment not warranted except in rare cases of “Pacemaker Syndrome”
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/
Cheng S, et al. JAMA 2009 Magna. Circ Arrhythm Electrophysiol 2013
Crisel RK, et al Eur Heart J 2011

2nd Degree AV Block
Mobitz 1
(Wenckebach)
ECG Characteristics: Progressive prolongation of the PR interval until a P wave is not conducted.
As the PR interval prolongs, the RR interval actually shortens
Usually benign unless associated with underlying pathology, i.e. MI
Treatment: remove “reversible” causes
No treatment for asymptomatic patients
atropine / pacemaker for symptomatic

ECG Characteristics: Constant PR interval with intermittent failure to conduct
• Rhythm is dangerous as the block is lower in the conduction system
• May cause syncope or may deteriorate into complete heart block
• Causes: drugs, anterioseptal MI
• Treatment: permanent pacemaker
Mobitz 2
2nd Degree AV Block

Mobitz Type I vs Type II
Mobitz type I & II can’t be differentiated in 2:1 blocks
every other beat is non-conducted so no opportunity to observe PR prolongation a long rhythm strip or a previous ECG examined
PR > 300ms or narrow QRS means block at AV node (type I)
response to atropine confirms type I block
worsening by carotid sinus massage means type I block

3rd Degree (Complete) Block
ECG Characteristics: No relationship between P waves and QRS complexes
Constant PR intervals and RR intervals Block at AV node: 2/3rd narrow QRS Block at bundle of His: narrow QRS Trifascicular block: wide QRS complex
• May be caused by inferior MI and its presence worsens the prognosis
• May cause syncopal symptoms, angina, or CHF
• Treatment: removing “reversible causes” / permanent pacemaker

Tachyarrhythmias

Increased/Abnormal Automaticity
Sinus tachycardia
Junctional tachycardia
Ectopic atrial tachycardia
www.uptodate.com
Ectopic Foci & Beats

Causes of Ectopic Foci & Generation of Arrhythmias
Hypoxia: Lung disease
Ischemia: CAD, Angina (local hypoxia)
Sympathetic Stimulation: Anxiety, Exercise, CHF, hyperthyroidism
Bradycardia: “Escape” rhythms…
Electrolyte Disturbances: K+, Ca++, Mg++
Drugs: Caffeine, stimulants, antiarrhyhtmic
Stretch: CHF, hypertrophy, valve disease

normal ("sinus") beats
sinus node doesn't fire leading to a period of asystole (sick sinus syndrome)
p-wave has different shape indicating it did not originate in the sinus node, but somewhere in the atria.
QRS is slightly different but still narrow, indicating that conduction through the ventricle is relatively normal
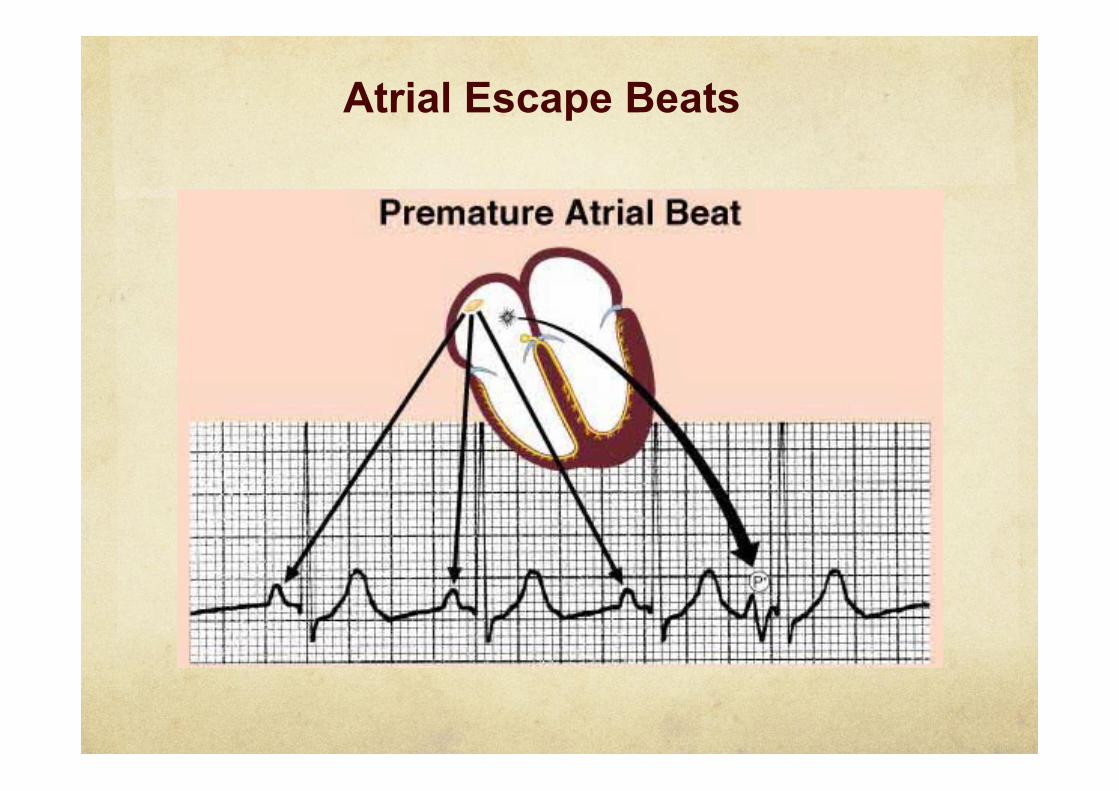
Atrial Escape Beats

Causes Mitral valve prolapse / MS
Coronary heart disease
exercise testing in IHD patients
Toxins or chemicals — Smoking, alcohol, and coffee
Miscellaneous - acute and chronic pulmonary disease
Atrial Escape Beats
Atrial Escape Beats

• A single ectopic focus fires near the AV node, which then conducts normally to the ventricles (usually initiated by a PAC)
• The rhythm is always REGULAR
• Prolonged runs of PSVT may result in atrial fibrillation or atrial flutter
• May be terminated by carotid massage
• Treatment: carotid massage, adenosine, Ca++ channel blockers, ablation
• Adenosine preferred in hypotension,
Rhythm usually begins with PAC
Note REGULAR rhythm in the tachycardia
Paroxysmal SVT

Paroxysmal SVT
• Treatment – vagal maneuvers – adenosine – if not effective
• Ca++ channel blockers, beta blockers, digoxin • cardioversion
– Ca++ channel blockers, beta blockers, and primary antiarrhythmic agents should not be serially administered because of potential additive negative hypotensive, bradycardic, and proarrhythmic effects.
– Class IIa antiarrhythmic drugs • amiodarone, procainamide, sotalol, felcanide
– in LV dysfunction • digoxin, amiodarone, diltiazem

• “wandering pacemaker”
• Multiple ectopic foci fire in the atria, all of which are conducted normally to the ventricles
• The rhythm is always IRREGULAR
• P-waves of different morphologies (shapes) ± variable PR interval
• HR >100 (in COPD patients >90)
Note IRREGULAR rhythm in the tachycardia
Multifocal Atrial Tachycardia
(McCord et al, Chest 1998)

Causes Pulmonary disease (60%)
COPD, Ac Resp Failure, Pneumonia, embolism
Drugs for Resp Diseases (theophylline, salbutamol)
Cardiac disease coronary, valvular, hypertensive and other
when associated with heart failure
Other conditions: Hypokalemia
Hypomagnesemia
Chronic renal failure (15%) – cause unclear
Sepsis
Multifocal Atrial Tachycardia

Treatment correction of electrolytes
treatment of underlying disease
removal of cause
disappointing results with anti-arrhythmics
Ca++ channel blocker (verapamil)
beta blockers
Multifocal Atrial Tachycardia

Multifocal Atrial Tachycardia

there is no p wave, indicating that it did not originate anywhere in the atria, but since the QRS complex is still thin and normal looking, we can conclude that the beat originated somewhere near the AV junction.
QRS is slightly different but still narrow, indicating that conduction through the ventricle is relatively normal
Junctional Escape Beats
Causes hypokalemia digitalis toxicity chronic lung disease acute myocardial infarction
Treatment No therapy in asymptomatic discontinue or control exposure to offending agents persistent, limiting symptoms:
beta blockers
Ca++ channel blockers
class IA, IC, or III antiarrhythmic
Junctional Escape Beats

• a "retrograde” p-wave may sometimes be seen on the right hand side of beats that originate in the ventricles, indicating that depolarization has spread back up through the atria from the ventricles
QRS is wide and much different looking than the normal beats. This indicates that the beat originated somewhere in the ventricles.
• no p wave, indicating that the beat did not originate anywhere in the atria
Ventricular Escape Beats

TREATMENT REQUIRED IN • frequent (> 30% of complexes) or are increasing in frequency • come close to or on top of a preceding T-wave (R on T) • 3 or more PVC's in a row (run of V-tach) • Any PVC in the setting of an acute MI • PVC's come from different foci ("multifocal" or "multiformed”) These may result in ventricular tachycardia or fibrillation.
sinus beats Unconverted V-tach to V-fib V-tach
“R on T phenomenon”
time

Re-entrant Rhythms

The Re-entry Mechanism
Fast Conduction Path Slow Recovery
Slow Conduction Path Fast Recovery
Electrical Impulse
Cardiac Conduction Tissue
Repolarizing Tissue (long refractory period)
Premature Beat Impulse

Fast Conduction Path Slow Recovery
Slow Conduction Path Fast Recovery
Electrical Impulse
Cardiac Conduction Tissue
Tissues with these type of circuits may exist:
• in the SA node, AV node, or any type of heart tissue • in a “macroscopic” structure such as an accessory pathway in WPW
The Re-entry Mechanism

Premature Beat Impulse
1. An arrhythmia is triggered by a premature beat
2. The beat cannot gain entry into the fast conducting pathway because of its long refractory period and therefore travels down the slow conducting pathway only
Fast Conduction Path Slow Recovery
Slow Conduction Path Fast Recovery
Cardiac Conduction Tissue
Repolarizing Tissue (long refractory period)
The Re-entry Mechanism

3. The wave of excitation from the premature beat arrives at the distal end of the fast conducting pathway, which has now recovered and therefore travels retrograde (backwards) up the fast pathway
Fast Conduction Path Slow Recovery
Slow Conduction Path Fast Recovery
Cardiac Conduction Tissue
The Re-entry Mechanism

4. On arriving at the top of the fast pathway it finds the slow pathway has recovered and therefore the wave of excitation ‘re-enters’ the pathway and continues in a ‘circular’ movement. This creates the re-entry circuit
Cardiac Conduction Tissue
Fast Conduction Path Slow Recovery
Slow Conduction Path Fast Recovery
The Re-entry Mechanism
AV nodal reentrant tachycardia (AVNRT)
Supraventricular tachycardia
AV reentrant tachycardia (AVRT)
Wolf – Parkinson – White syndrome
Atrial flutter
Ventricular tachycardia
Atrial fibrillation
Ventricular fibrillation
The Re-entrant Rhythm

Atrio-Ventricular Nodal Re-entry • supraventricular tachycardia
Atrial Re-entry • atrial tachycardia • atrial fibrillation • atrial flutter
Atrio-Ventricular Re-entry • Wolf Parkinson White Ventricular Re-entry
• ventricular tachycardia • ventricular fibrillation
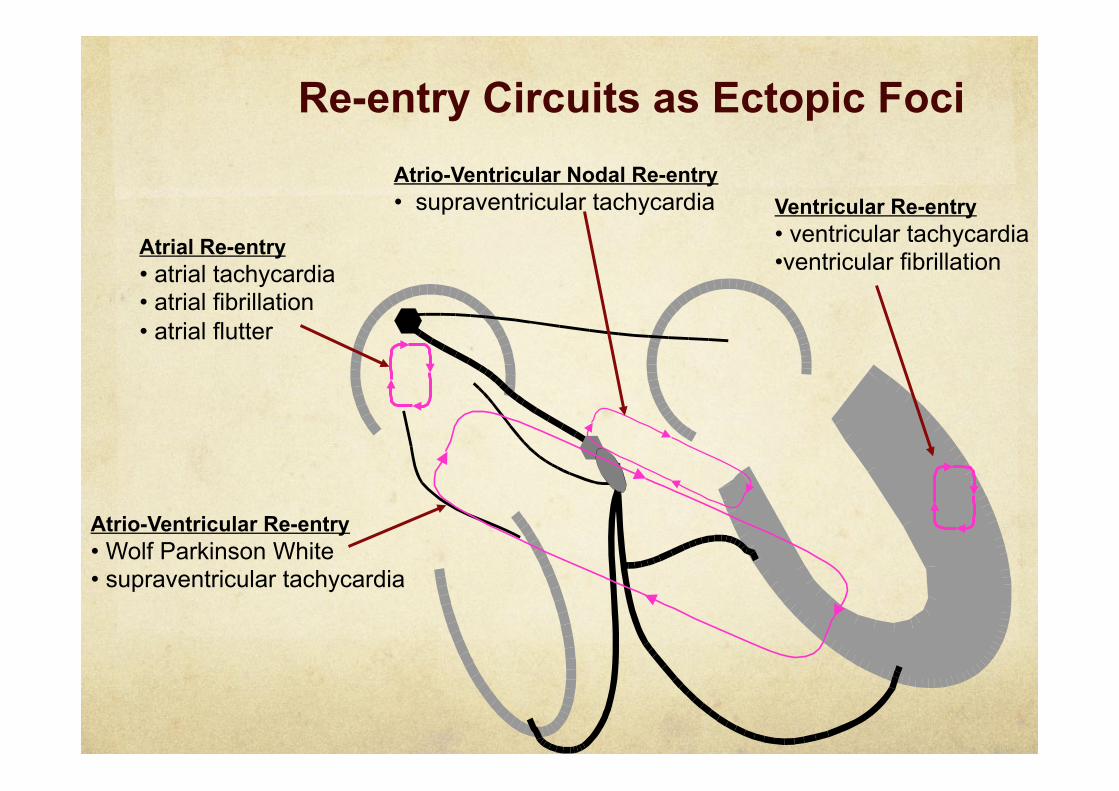
Ventricular Re-entry • ventricular tachycardia • ventricular fibrillation
Atrio-Ventricular Nodal Re-entry • supraventricular tachycardia
Atrial Re-entry • atrial tachycardia • atrial fibrillation • atrial flutter
Atrio-Ventricular Re-entry • Wolf Parkinson White • supraventricular tachycardia
Re-entry Circuits as Ectopic Foci

Rate 100-270 Normal QRS Aberrancy possible
Acute Rx: • Vagal maneuvers • Adenosine 6-12 mg IV push • Ca++ channel blockers
AV Nodal Re-entrant Tachycardia

Atrial flutter is caused by a reentrant circuit in the wall of the atrium
ECG Characteristics: Typical: “sawtooth” flutter waves at a rate of ~ 300 bpm
Flutter waves have constant amplitude, duration, and morphology through the cardiac cycle
There is usually either a 2:1 or 4:1 block at the AV node, resulting in ventricular rates of either 150 or 75 bpm
www.uptodate.com
Atrial Flutter

Unmasking of flutter waves with adenosine.
Acute Rx: • ventricular rate control can be difficult • AV nodal blockers prevent 1:1 conduction • Ibutilide 1-2mg rapid IV infusion – have paddles ready • Rapid pacing or low voltage DC cardioversion is effective • Anticoagulation as per atrial fibrillation
Atrial Flutter

Atrial fibrillation is caused by numerous waves of depolarization spreading throughout the atria, leading to an absence of coordinated atrial contraction Classifification • Recurrent: when AF occurs on 2 or more occasions • Paroxysmal: episodes that generally last 7 days or less (most last less than
24 hours) • Persistent: AF that lasts more than 7 days • Permanent: paroxysmal or persistent AF with failure to cardiovert or not
attempted
www.uptodate.com
Atrial Fibrillation


Atrial Fibrillation Causes

Treatment of Atrial Fib Haemodnamically Stable Patient:
Rate control therapy: β blockers – esmolol, metoprolol, propranolol
Ca++ channel blockers – verapamil, diltiazem
Amiodarone Digoxin - for AF with CHF, or LV dysfunction (not to be
given in patients with paroxysmal AF)
Conversion of rhythm: Class I recommendation: flecainide, propafenone, ibutilide
Class II a recommendations: amiodarone
Class IIb: administration of quinidine/procainamide.
Anticoagulation therapy:

Treatment of Atrial Fib Haemodynamically Unstable Patient:
life-threatening - emergency electrical cardioversion (irrespective of the duration of AF)
non-life-threatening haemodynamic instability where there is a delay in organising electrical cardioversion,
intravenous amiodarone should be used
known permanent AF (caused mainly by a poorly controlled ventricular rate) beta-blockers (esmolol, metoprolol, propranolol) calcium channel blockers (verapamil, diltiazem)
amiodarone (where beta-blockers or calcium antagonists are contraindicated or ineffective)

Treatment of Atrial Fib
Haemodynamically Unstable Patient:
Antithrombotic therapy for acute-onset AF emergency intervention should be performed ASAP
initiation of anticoagulation should not delay any emergency intervention
Heparin:
heparin should be started at initial presentation
continue heparin until full assessment made and appropriate antithrombotic therapy started

Treatment of Atrial Fib
Haemodynamically Unstable Patient:
Antithrombotic therapy for acute-onset AF Oral Anticoagulation
Needed in acute onset AF is uncertain
Not needed in confirmed acute onset AF (<48 hours) if converted to sinus rhythm successfully
Needed in confirmed acute onset AF if:
stable sinus rhythm not successfully restored
high risk of recurrence
high risk of stroke

Treatment
• Unstable – DC cardioversion • Stable monomorphic – Adenosine, Amiodarone • Stable polymorphic - treat underlying etiology
Rate 100-200 Wide QRS Monomorphic vs Polymorphic
Ventricular Tachycardia

Monomorphic common in previous Q wave MI
not caused by acute ischemia
Polymorphic (May have long QT interval)
Medication
Electrolyte imbalance
Congenital predisposition
Myocardial ischemia
Ventricular Tachycardia

www.uptodate.com
Ventricular fibrillation is caused by numerous waves of depolarization spreading throughout the ventricles simultaneously, leading to disorganized ventricular contraction and immediate loss of cardiac function.
ECG Characteristics: Absent P waves
Disorganized electrical activity
Deflections continuously change in shape, magnitude and direction
Ventricular Fibrillation

Questions

Question 1
A 25-year-old patient presenting with palpitations is noted to have a wide complex, irregular tachycardia at a rate of 260. The upstroke of the QRS is slurred. The blood pressure is normal, and the patient appears well. Most likely diagnosis is:
A. Atrial fibrillation with WPW syndrome
B. Unstable Ventricular Tachycardia
C. Supraventricular Tachycardia
D. Atrial Flutter
E. Ventricular Fibrillation
Answer “A”

Question 2
A 50 years old gentleman is undergoing emergency exploratory laparatomy under GA. On ECG monitors, you notice wide-complexed ectopic beats occurring 3 to 4 times a minute. His heart rate remains 74 bpm and BP is 130/84mmHg. This arrhythmia is considered benign when the ectopic beats:
A. come on top of a preceding T-wave
B. occur three or more in a row
C. happen in an acute MI setting
D. are coming from same focus
E. are more than 30% of complexes
Answer “D”

Question 3
A 60-year-old man with a history of prior anterior myocardial infarction develops a monomorphic wide complex tachycardia after non-cardiac surgery. The differential diagnosis includes:
A. Ventricular Fibrillation B. Supraventricular Tachycardia C. Torse De Pointes D. Atrial Fibrillation E. SVT with aberrant conduction Answer “E”

Question 4
First line drug for rate control in atrial fibrillation is
A. amiodarone
B. digoxin
C. esmolol
D. verapamil
E. quinidine
Answer “C”
Question 5
A 60 years old patient has arrived in emergency department with 6 days history of atrial fibrillation. This type of AF is classified as:
A. Chronic
B. Recurrent
C. Persistent
D. Paroxysmal
E. Permanent
Answer “D”

Thank you





























