Embed Size (px)
Citation preview
PHARMACOTHERAPEUTI
C RELEVANCE OF “ASIAN
INDIAN PHENOTYPE”P Guruprasad
DM, Clinical Pharmacology4/5/2015
1
Who are they ??
4/5/2015
2
Asian Indian Phenotype !!!
4/5/2015
3
Asian Indian Phenotype - introduction
The so called “Asian Indian Phenotype” refers to
certain unique clinical and biochemical
abnormalities in Indians which include increased
insulin resistance, greater abdominal adiposity i.e.,
higher waist circumference despite lower body
mass index, lower adiponectin and higher high
sensitivity C-reactive protein levels.
Epidemiology of type 2 diabetes: Indian scenario
V. Mohan, S. Sandeep, R. Deepa, B. Shah* & C. Varghese
Indian J Med Res 125, March 2007, pp 217-230
4/5/2015
4

Asian Indian Phenotype – fat
distribution
Total body fat –
An indian with BMI of 26 = European with BMI of 30 *
Fat distribution
More abdominal (subcutaneous) and visceral
IMPLICATION – increased cardiovascular risk due to lipotoxicity
Higher truncal skin fold and truncal to peripheral skin fold
ratio
Higher central to peripheral skin fold ratio
Even indian babies were relatively obese in comparison
with white american babies
Metabolically Obese Normal Weight (MONW) individual
4/5/2015
5
*Rush EC, Freitas I, Plank LD. Body size, body composition and fat distribution:
comparative analysis of European, Maori, Pacific Island and Asian Indian adults.
Br J Nutr. 2009 Aug;102(4):632–41.
Obesity measures – BMI and Waist
circumference
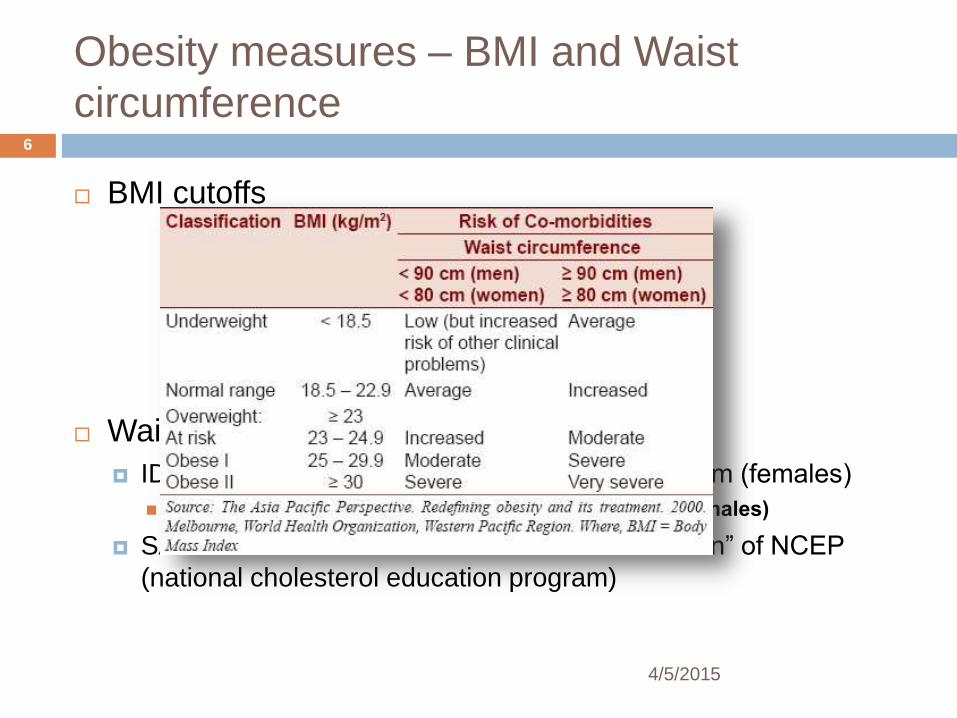
BMI cutoffs
Waist Circumference (WC)
IDF consensus cutoffs - ≥ 94 cm (males) / ≥ 80 cm (females)
South asians – cutoffs - ≥ 90 cm (males) / ≥ 80 cm (females)
SAM-NCEP cutoffs – a “South Asian modification” of NCEP
(national cholesterol education program)
4/5/2015
6
Asian Indian Phenotype – diabetes and
Blood pressure
Blood pressure
In comparison with white americans, Indians have significantly
higher blood pressures
Indian children in the age group 8-14 years had significantly
higher blood pressure when compared with their american
counterparts* (after adjusting for BMI)
Diabetes
Diabetes is 3-6 time more common among asian indians than
whites (when adjusted for age and BMI)
Diabetes occurs 10 years (on an average) earlier among Indians
Many indians develop diabetes mellitus at BMI less than 25 kg/m2
South asian diabetics have 2-4 times the mortality seen among
white and Chinese diabetics*Jafar TH, Islam M, Poulter N, Hatcher J, Schmid CH, Levey AS, et al. Children in South Asia have higher body mass-
adjusted blood pressure levels than white children in the United States: a comparative study. Circulation. 2005 Mar
15;111(10):1291–7.
4/5/2015
7
Asian Indian Phenotype- Metabolic
Syndrome (MS)
Metabolic syndrome – increases risk of cardiovascular
disease by 2 fold
Most south asians (Indians) – MONW (Metabolically
obese, normal weight) individuals
Prevalence of MS among Indians – (≥ 30% )*
Prevalence among females higher than in males (by 50%)
More than europeans, similar to american whites
Cardiovascular disease risk due to MS
Hazards ratio of 2.1 among south asians which is higher than
that seen among europeans (HR of 1.6)
4/5/2015
8
*Chow CK, Naidu S, Raju K, Raju R, Joshi R, Sullivan D, et al.
Significant lipid, adiposity and metabolic abnormalities amongst 4535
Indians from a developing region of rural Andhra Pradesh.
Atherosclerosis. 2008 Feb;196(2):943–52.
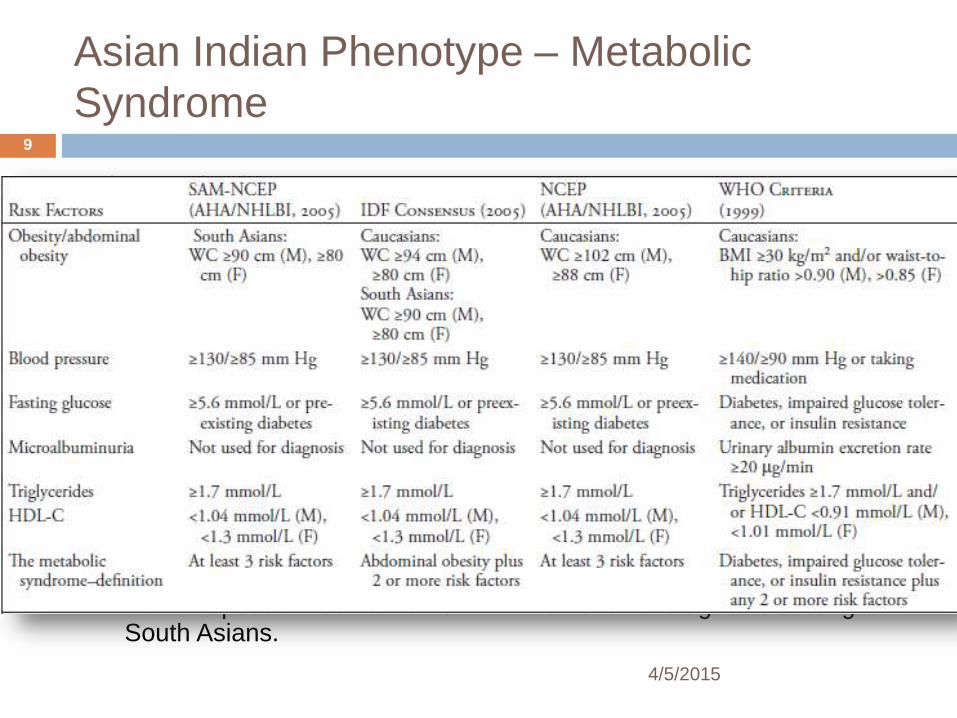
Asian Indian Phenotype – Metabolic
Syndrome
Three criteria
IDF (International Diabetes Federation)
NCEP ( National Cholesterol Education Programme)
WHO
Since the cut-offs for BMI and WC were not appropriate for Asian Indians – underestimation of MS (Metabolic Syndrome)
Only IDF has South Asian Specific Cut-offs for WC .
However, IDF criteria uses waist circumference as a compulsory component for diagnosis of MS. This also leads to underestimation of MS among South Asians.
Only 30% of indians who have MS satisfy all 3 criteria
SAM-NCEP (South Asian Modified- NCEP)
New Proposed modification of NCEP criteria for diagnosis among South Asians.
4/5/2015
9
Asian indian phenotype – dyslipidemia and
procoagulant tendency
Higher prevalence of dyslipidemia among indians (when
compared with white americans)
“South Asian Dyslipidemia” *
High levels of Apo B, triglycerides, and Lp(a)
Borderline high levels of LDL cholesterol
Low levels of Apo A1, and HDL cholesterol
Also HDL is small and dysfunctional
Indians are associated with higher levels of PAI-
1(Plasminogen Activator Inhibitor-1) and fibrinogen
4/5/2015
10
*Joshi P, Islam S, Pais P, Reddy S, Dorairaj P, Kazmi K, et al. Risk factors
for early myocardial infarction in South Asians compared with individuals in
other countries. JAMA J Am Med Assoc. 2007 Jan 17;297(3):286–94.
Asian Indian Phenotype – Coronary artery
disease (CAD)
Risk of coronary artery disease related mortality – higher
among indians (about 2 times)
Not completely explained by known risk factors*
Highest incidence of premature CAD in the world
CAD occurs 5-10 years earlier among south asians
Case fatality rates from CAD – highest among indians
(15%) when compared with many countries (low, middle
income and developed countries)
4/5/2015
11
*Forouhi NG, Sattar N, Tillin T, McKeigue PM, Chaturvedi N. Do
known risk factors explain the higher coronary heart disease
mortality in South Asian compared with European men?
Prospective follow-up of the Southall and Brent studies, UK.
Diabetologia. 2006 Nov;49(11):2580–8.
Asian indian phenotype
No study has yet linked the Asian indian phenotpye to
any gene
Known risk factors do not completely explain the
increased susceptibility of south asians to
cardiovascular disease
New biomarkers required
Eg.- female, buffalo hump, double chin and age > 35 years *
4/5/2015
12
*Misra A, Jaiswal A, Shakti D, Wasir J, Vikram NK, Pandey RM,
et al. Novel phenotypic markers and screening score for the
metabolic syndrome in adult Asian Indians. Diabetes Res Clin
Pract. 2008 Feb;79(2):e1–5.
Asian Indian Phenotype – economic
impact
4/5/2015
13
India lost 9.2 million potentially productive years of
life in 2000 *
India lost USD 9 billion of its national income in 2005
due to premature deaths from cardiovascular disease,
stroke and diabetes (WHO)
And may lose USD 237 billion in 2015 if proper
measures to prevent these premature deaths are not
taken (WHO)
*Reddy KS. India Wakes Up to the Threat of
Cardiovascular Diseases. J Am Coll Cardiol. 2007 Oct
2;50(14):1370–2.
Asian Indian Phenotype - theories
4/5/2015
14
Adipose tissue overflow hypothesis*
Primary adipose tissue – subcutaneous tissue compartment
Small for south asians
During excess energy intake, the subcutaneous tissue is
saturated early leading to expansion of other adipose tissue
compartments
Thrifty gene hypothesis
*Sniderman AD, Bhopal R, Prabhakaran D, Sarrafzadegan
N, Tchernof A. Why might South Asians be so susceptible
to central obesity and its atherogenic consequences? The
adipose tissue overflow hypothesis. Int J Epidemiol. 2007
Feb;36(1):220–5.
Asian indian phenotype – what do current
international treatment guidelines say ?
ADA (American Diabetic Association) Diabetic Care guidelines, 2013
Overweight + Ethnicity (asian american) is an indication for testing for hyperglycemia among asymptomatic adults and children
NCEP-ATP III guidelines
Remark – type 2 DM associated with a very high risk for coronary heart disease among south asians
Advice for treatment of south asians Special attention for identification of risk factors
Emphasis on lifestyle changes
Cholesterol management guidelines are the same
2013 ACC/AHA Blood Cholesterol Guideline
Under safety recommendation for statins – higher dose of statins may be used for patients of asian ancestry 4/5/2015
15
Asian Indian Phenotype – what do current
international treatment guidelines say ?contd.
2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk
10 yr risk for ASCVD (atherosclerotic cardiovascular disease) for asian Americans is lower than for non-hispanic whites
Ethnic group specific algorithms for this 10yr risk is not available; but needed to be developed
Guidelines with no reference to South Asians
2014 evidence based guideline for the management of high blood pressure in adults (report from the panel members appointed to the Eight joint national committee)
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
2013 ESC guidelines on the management of stable coronary artery disease
4/5/2015
16
Asian Indian Phenotype – what do current
international treatment guidelines say ?contd.
• 2013 AHA/ACC/TOS Guideline for the Management
of Overweight and Obesity in Adult
One of the questions the guideline sought to address was
– “Are differences across population subgroups in the
relationships of BMI and waist circumference cutpoints
with CVD, its risk factors, and overall mortality sufficiently
large to warrant different cutpoints? If so, what should
they be?”
The groups that were considered included “asian”
The data on the question were mostly poor in quality
Not enough quality data to address cutoffs for BMI and
WC for CVD risk
4/5/2015
17
Recommendations of the Second Indo-US summit on
prevention of cardiovascular diseases among South
Asians (2009)
Framingham risk scores (estimates for 10 year risk for
CAD)
Risk estimated must be multiplied by a factor of 2 for south
asians
Threshold lowering of all risk factors
Universal screening from the age of 18 years
Lifestyle modification
Aggressive pharmacotherapy for control of dyslipidemia
4/5/2015
18
Indian studies and programs
Some important epidemiological studies
Jaipur heart watch study (JHWS)
Chennai Urban Rural Epidemiology Study (CURES)
Cohort studies – Bombay Cohort Study; New Delhi Birth Study
National Program on Diabetes, Cardiovascular diseases
and stroke
Launched in 10 states
3 components
Health promotion
Targeting high risk subjects to prevent disease
Surveillance and research
4/5/2015
19
Asian Indian Phenotype – more questions
than answers !!
4/5/2015
20
Whether the cutoffs of CAD risk factors need to be
reconsidered for the Indian scenario ?
Can be answered only by well planned randomized clinical
trials
Whether any genes have a role to play in increasing the
risk for CAD among south asians ?
Are current treatment regimens and treatment goals
sufficient for decreasing morbidity and mortality due to
cardiovascular diseases ?
Again the only solution is RCTs
Premature CAD and related mortality.
Sleeping or not ??
4/5/2015
21
All the following parameters are used to estimate the 10
year risk for Coronary Heart disease according to the
Framingham Point Scores EXCEPT
Age
LDL cholesterol
Smoking status
Blood pressure
- Correct answer
questions
4/5/2015
22