Embed Size (px)
Citation preview
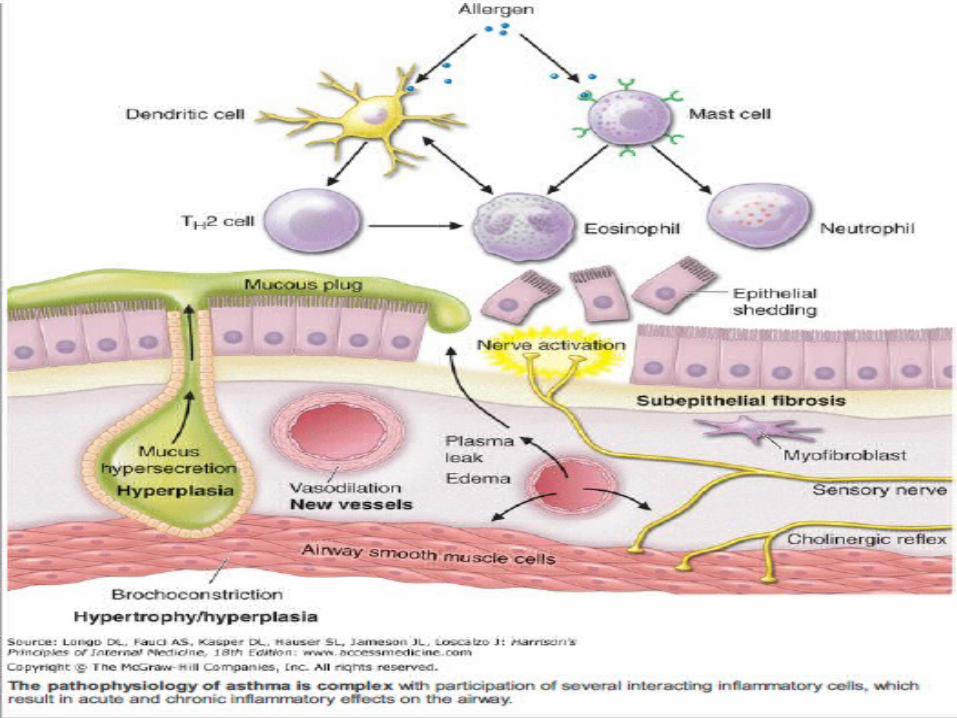
ASTHMA
DEFINITIONChronic inflammatory disorder of the airways
Widespread but variable airflow obstruction that is often reversible either spontaneously or with treatment
Bronchial hyperresponsiveness to a variety of stimuli
affects 300 million people world-widesocio-economic impact is enormous, poor control leads to days lost from school or work, unscheduled health-care visits and hospital admissions
Adult Asthma Facts14.5 million workdays lost due to asthma, a 2.3 fold increase from the early 80s to the mid 90sAdults accounted for over 1.3 million ED visits and 288,000 hospitalizations due to asthmaOne third of asthma related deaths occur in patients 35-44 years oldOver 50% of asthma related deaths occur in patients 65 years and older
Morb Mortal Wkly Rep. 2002 March 29; 51:1-13.
Atopymajor risk factor for asthmagenetically determined production of specific IgE antibodysuffer from other atopic diseases, particularly allergic rhinitis and atopic dermatitis (eczema)most common allergens are - house dust mites, cat and dog fur, cockroaches, grass and tree pollens
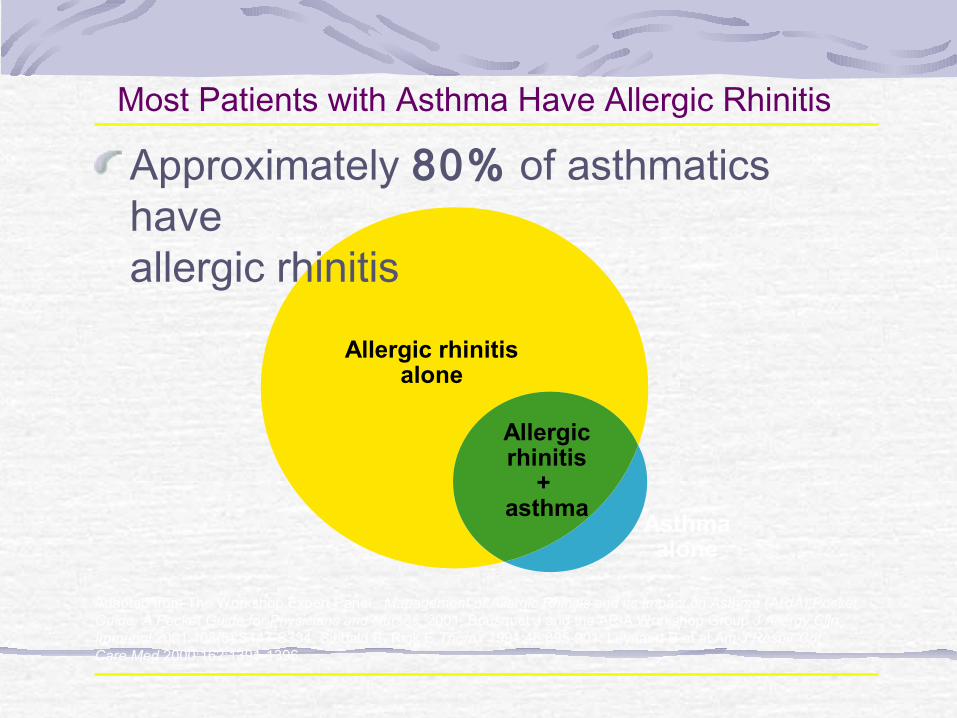
Most Patients with Asthma Have Allergic Rhinitis Approximately 80% of asthmatics have allergic rhinitis
Adapted from The Workshop Expert Panel. Management of Allergic Rhinitis and its Impact on Asthma (ARIA) Pocket Guide. A Pocket Guide for Physicians and Nurses. 2001; Bousquet J and the ARIA Workshop Group J Allergy Clin Immunol 2001;108(5):S147-S334; Sibbald B, Rink E Thorax 1991;46:895-901; Leynaert B et al Am J Respir Crit Care Med 2000;162:1391-1396.
Asthmaalone
Allergic rhinitisalone
Allergicrhinitis
+ asthma
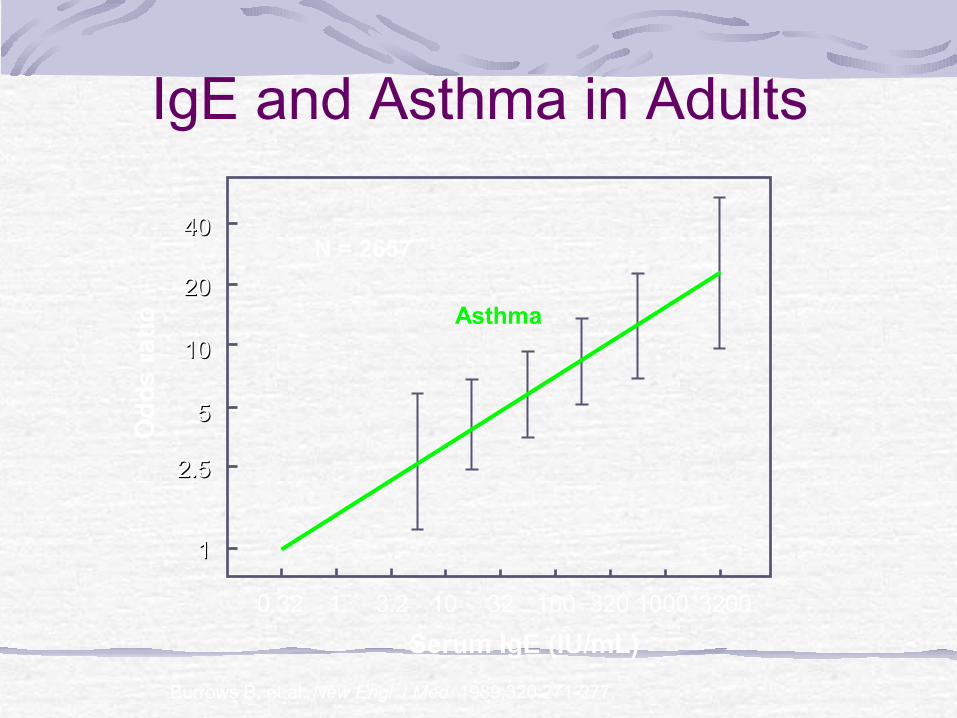
IgE and Asthma in Adults
Asthma
Serum IgE (IU/mL)
Od
ds
ra
tio
N = 2657
0.32 1 3.2 10 32 100 320 1000 3200
11
2.52.5
55
1010
2020
4040
Burrows B, et al. New Engl J Med. 1989;320:271-277.
Intrinsic Asthmanegative skin tests to common inhalant allergens and normal serum concentrations of IgElater onset of disease (adult-onset asthma), commonly have concomitant nasal polyps, and may be aspirin-sensitive
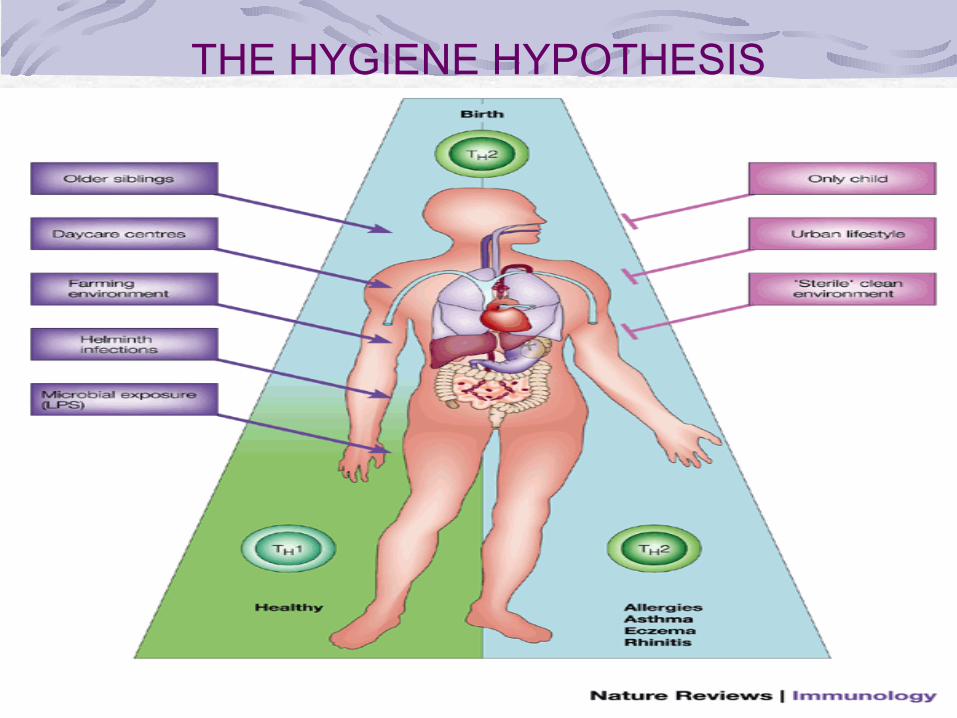
THE HYGIENE HYPOTHESIS
AIR POLLUTIONsulfur dioxide, ozone, and diesel particulates, may trigger asthma symptomsIndoor air pollution may be more important with exposure to nitrogen oxides from cooking stoves and exposure to passive cigarette smoke
OCCUPATIONAL EXPOSURE
relatively common and may affect up to 10% of young adultsChemicals such as toluene diisocyanate and trimellitic anhydride, fungal amylase in wheat flour in bakerssuspected when symptoms improve during weekends and holidays
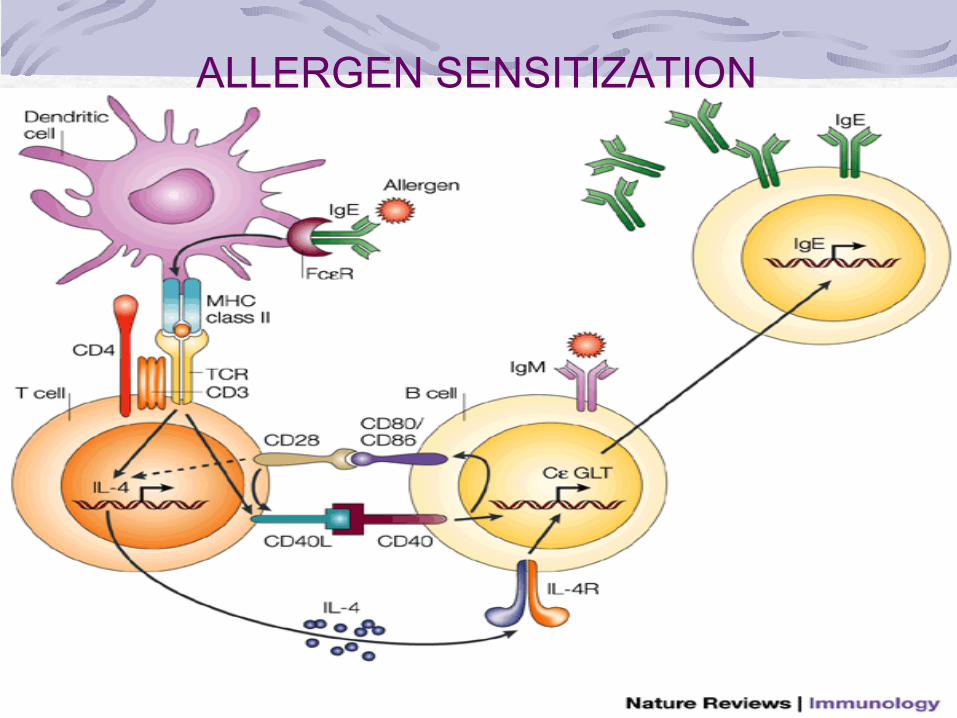
ALLERGEN SENSITIZATION
DENDRITIC CELL WITH AN ALLERGEN
DENDRITIC CELL CAPTURES THE ALLERGEN AND RUNS WITH IT TO THE LYMPH NODE
DENDRITIC CELL RELEASES THE
ALLERGEN
T CELL CAPTURES THE ALLERGEN
CELL RECRUITMENT
MUSCLE CELL HYPERTROPHY
TISSUEDAMAG
E
MORE TISSUE DAMAGE
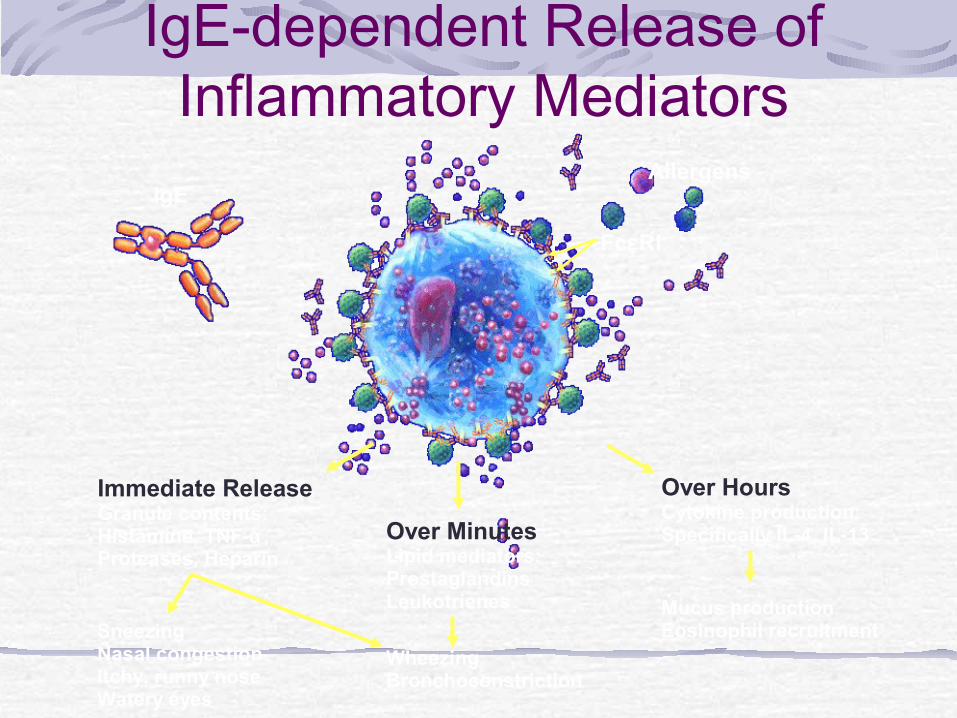
IgE-dependent Release of Inflammatory Mediators
IgEAllergens
FcεRI
Over MinutesLipid mediators: ProstaglandinsLeukotrienes
WheezingBronchoconstriction
Over HoursCytokine production:Specifically IL-4, IL-13
Mucus productionEosinophil recruitment
Immediate ReleaseGranule contents:Histamine, TNF-α, Proteases, Heparin
Sneezing Nasal congestionItchy, runny noseWatery eyes
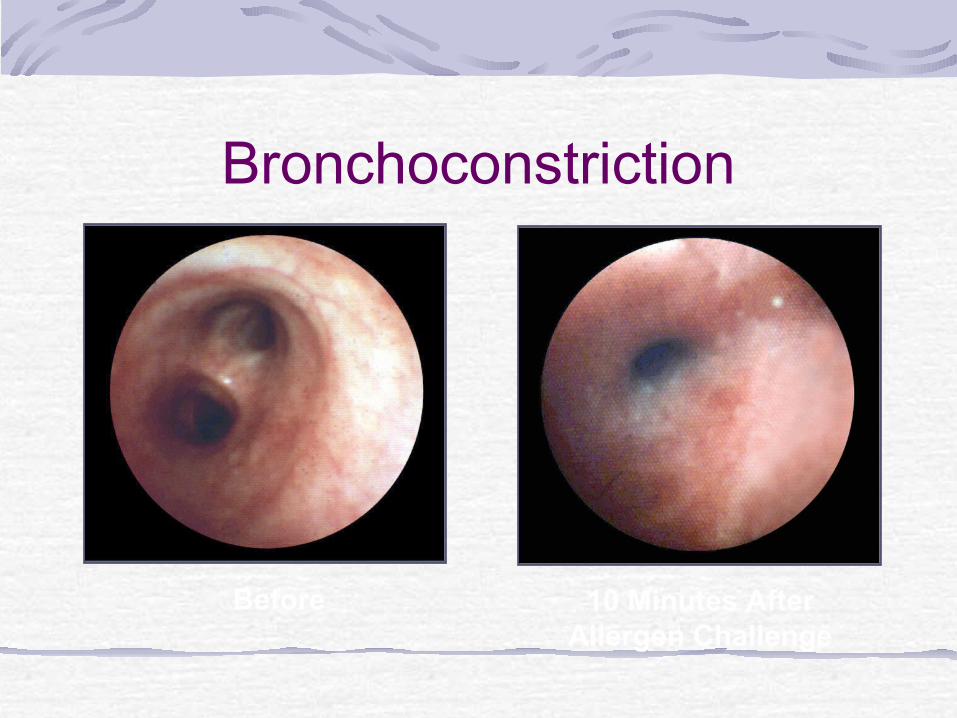
Before 10 Minutes After Allergen Challenge
Bronchoconstriction
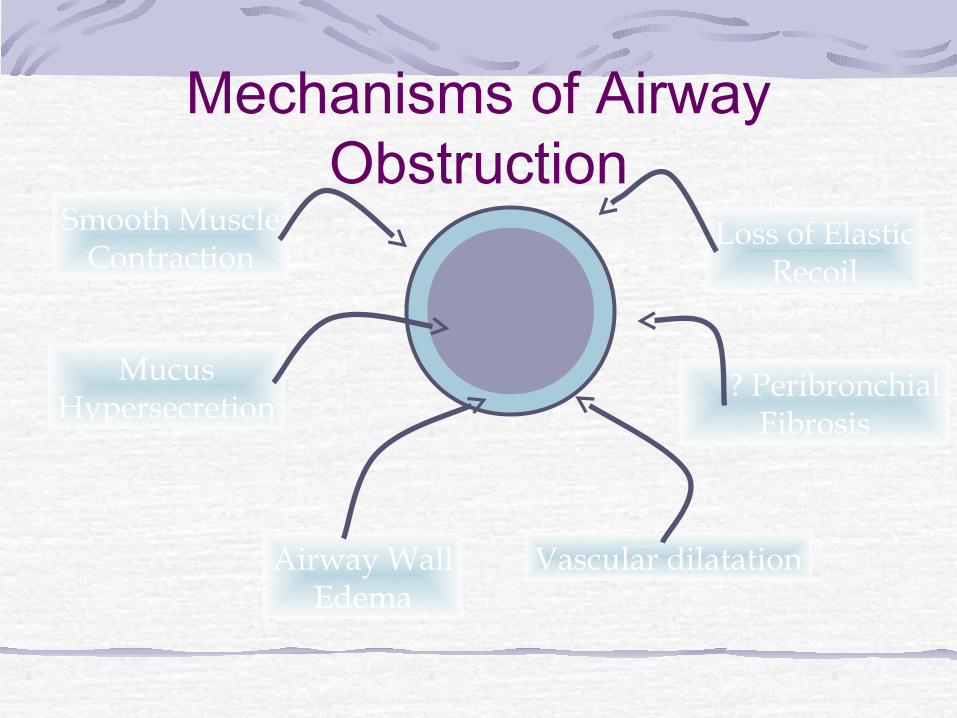
Mechanisms of Airway Obstruction
Smooth MuscleContraction
MucusHypersecretion
Loss of ElasticRecoil
? PeribronchialFibrosis
Airway WallEdema
Vascular dilatation
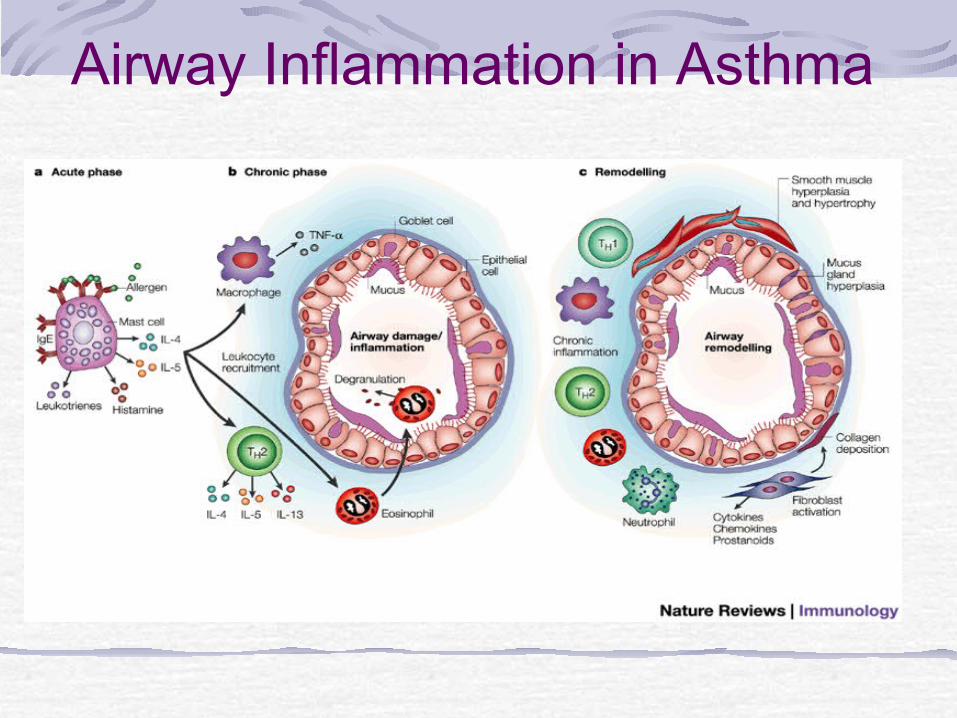
Airway Inflammation in Asthma
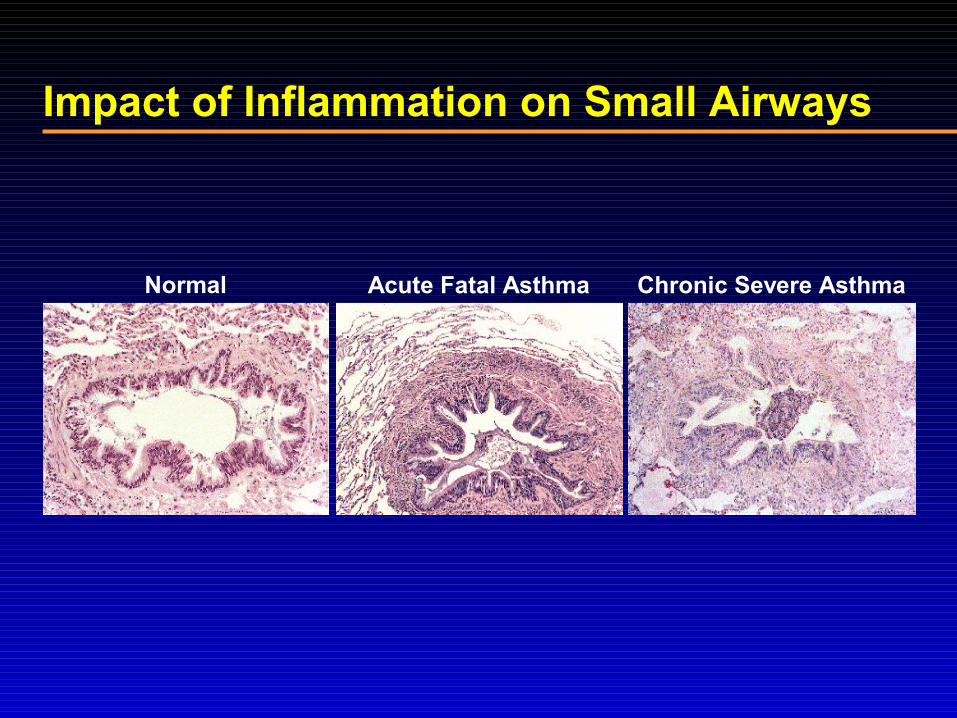
Acute Fatal Asthma
Impact of Inflammation on Small AirwaysImpact of Inflammation on Small Airways
Normal Chronic Severe Asthma
CLINICAL FEATURES AND
DIAGNOSIS
SYMPTOMSRecurrent episodes of:
Shortness of breathWheezingChest tightnessCough, particularly at night and early in the morning
PATTERN OF SYMPTOMSPerennial, seasonal or both
Continual, episodic or both
Diurnal variations, especially nocturnal and on awakening early in the morning
PRECIPITATING AND/OR AGGRAVATING FACTORS
Viral respiratory infectionsEnvironmental allergensExerciseOccupational chemicals or allergensIrritantsChanges in weatherEndocrine factorsGERDSinusitis
PHYSICAL EXAMNormal physical exam - asthma is under controlExpiratory wheezing with normal or decreased air movementAccessory respiratory muscle useOminous sign- no wheezing with decreased air movement
Cough may be the dominant symptom in some patients, and the lack of wheeze or breathlessness may lead to a delay in reaching the diagnosis of so-called ‘cough-variant asthma
EVALUATION
CLINICAL HISTORYSPIROMETRYMETHACHOLLINE CHALLENGE TESTALLERGY SKIN TESTS
Spirometry: A Simple, Basic Measurement
Essential to initial evaluationHelps assess severity of airflow obstructionAids in differential diagnosis
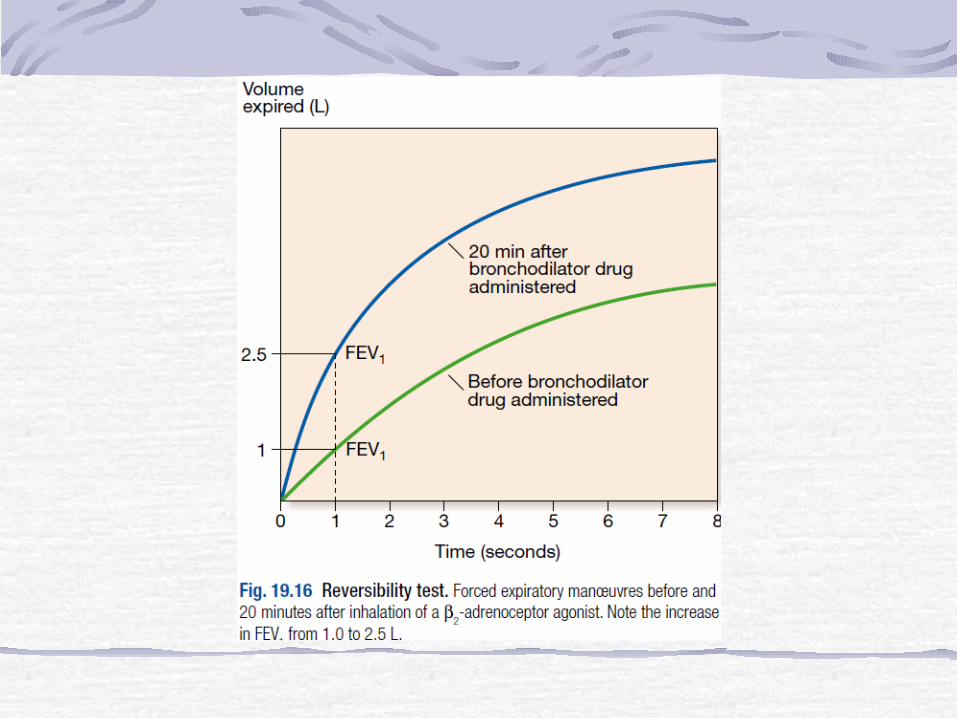
Obstructive versus restrictive airway diseaseReversibility of airflow obstruction
Confirms periodic home PEFR measurements in selected patients
Spirometry in asthma
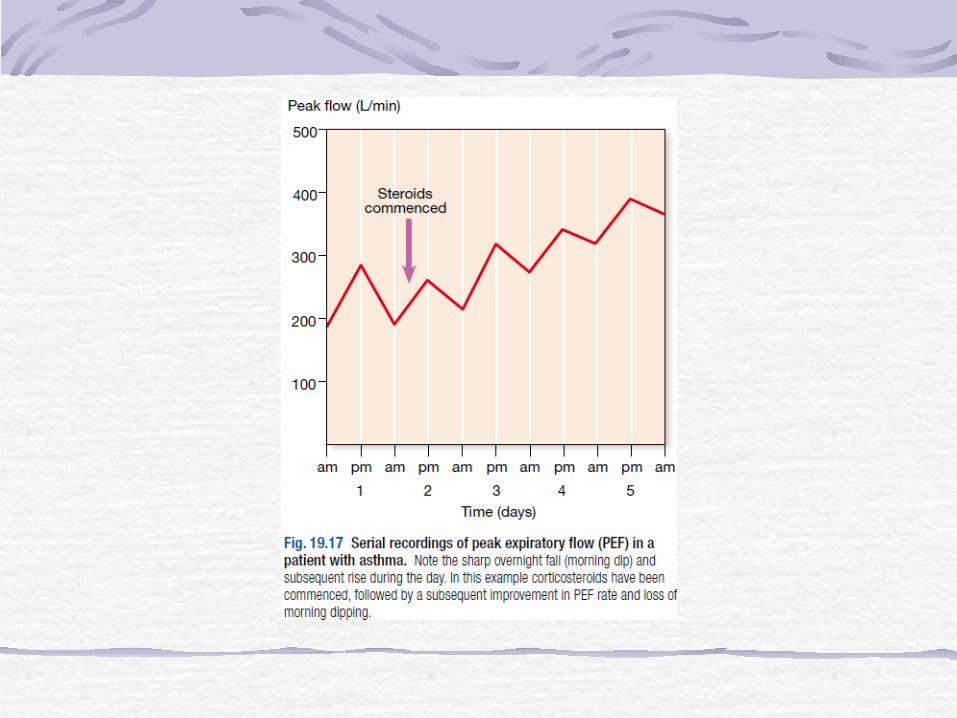
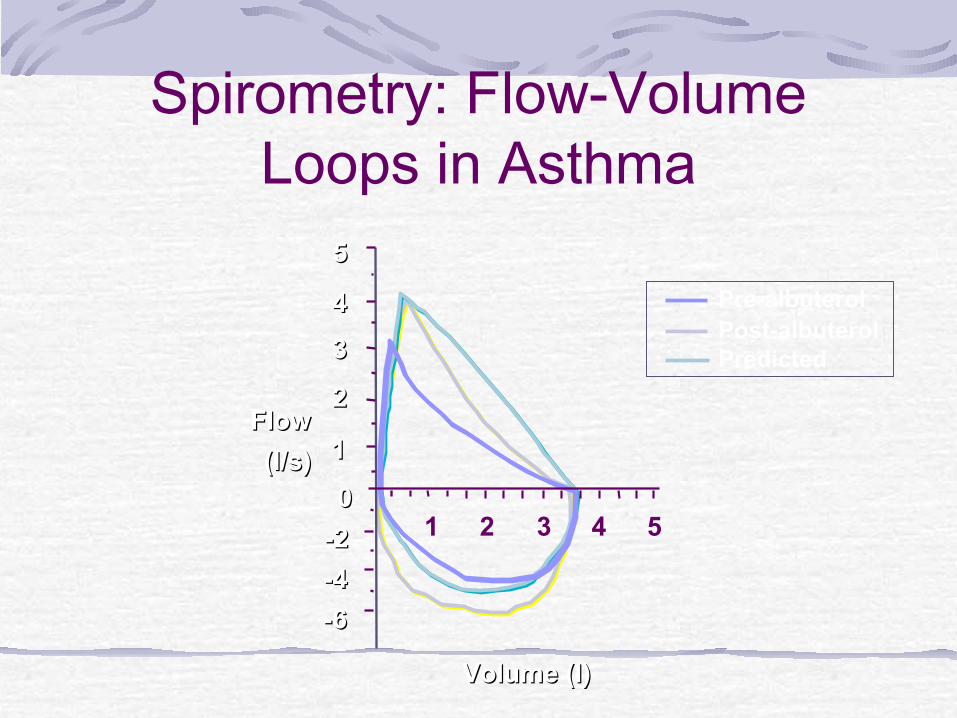
reduced FEV1, FEV1/FVC ratio, and PEFImprovement in FEV1>12% with bronchodilator therapy Measurements of PEF twice daily may confirm the diurnal variations in airflow obstruction – more than 20% is considered diagnostic

FlowFlow
(l/s)(l/s)
Volume (l)Volume (l)
-2-2
00
-4-4
11
33
22
44
55
21 3 4 5
-6-6
Pre-albuterolPost-albuterolPredicted
Spirometry: Flow-Volume Loops in Asthma
Bronchoprovocation Challenges
methacholine or histamine challenge calculation of the provocative concentration that reduces FEV1 by 20% (PC20)Measures the increased AHRexercise testing is done to demonstrate the postexercise bronchoconstriction if there is anpredominant history of EIA
Reasons for Performing Bronchoprovocation Challenges in
Clinical Practice
To quantify the severity of the airway hyperresponsiveness(AHR)Clarify a clinical diagnosis of asthma when a reasonable degree of doubt existsTo determine the presence of bronchial hyperresponsiveness in patients with chronic cough

ALLERGIC TRIGGERS
INHALANT ALLERGENS
Animal allergensHouse-dust mites Cockroach allergensIndoor fungi (molds)Outdoor allergens
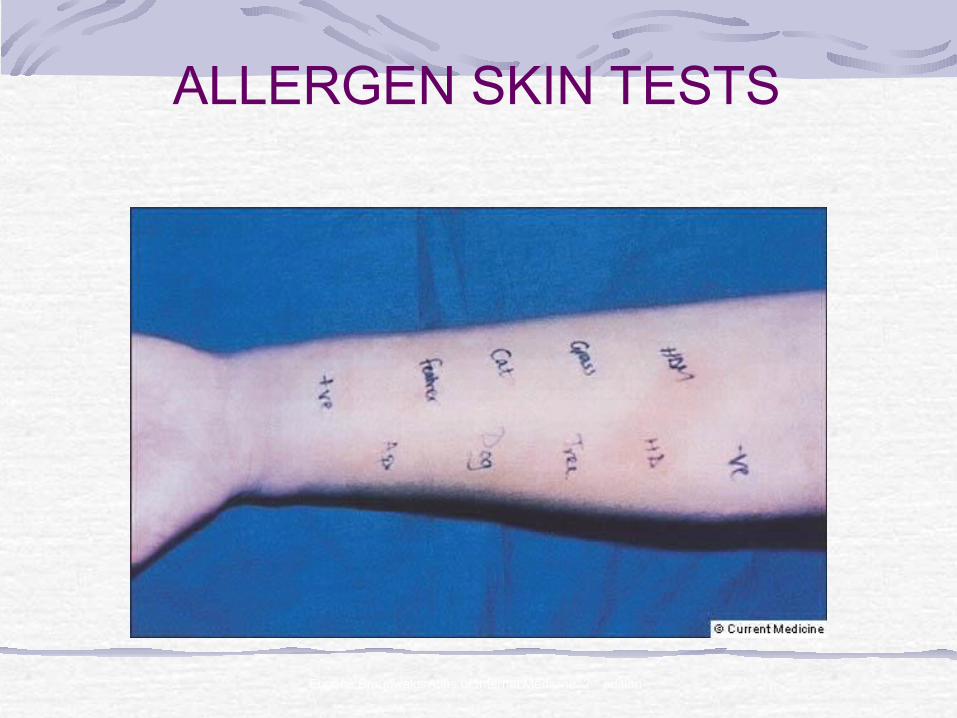
ALLERGEN SKIN TESTS
Eugene Braunwald, Atlas of Internal Medicine, 2nd edition
EVALUATIONCBC with differential ( eosinophilia often seen in asthma, ABPA and CS vasculitis)Total igEspecific IgE to inhaled allergens [radioallergosorbent test(RAST)]CXRCT of the chestABG in status asthmaticus
Exhaled NO is now being used as a noninvasive test to measure eosinophilic airway inflammationThe typically elevated levels in asthma are reduced by ICS, so this may be a test of compliance with therapy
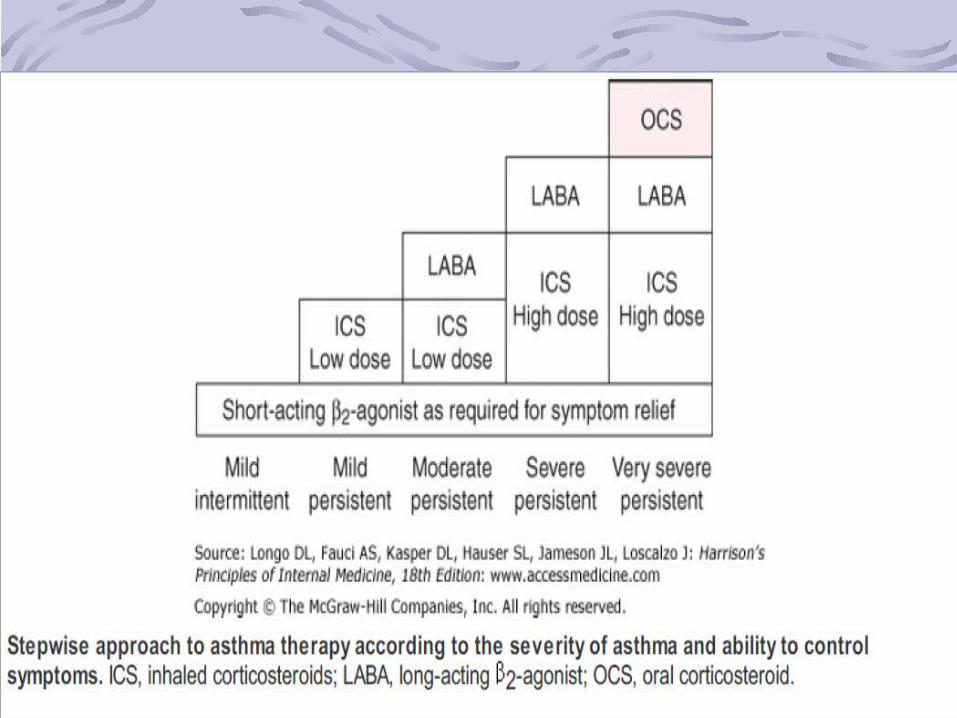
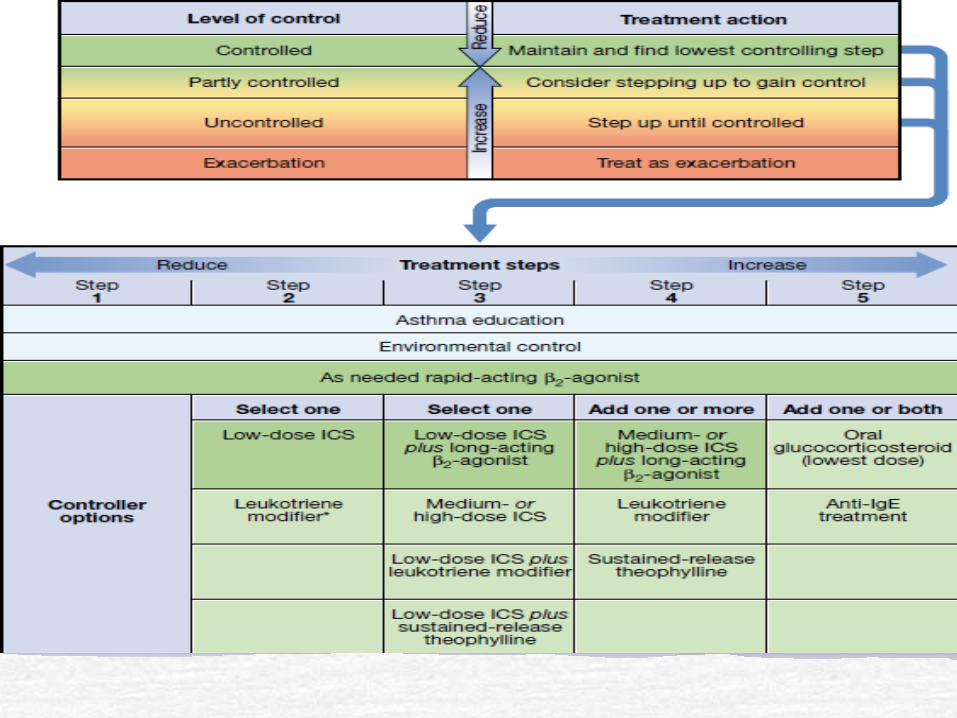
ASTHMA CLASSIFICATION AND THERAPY
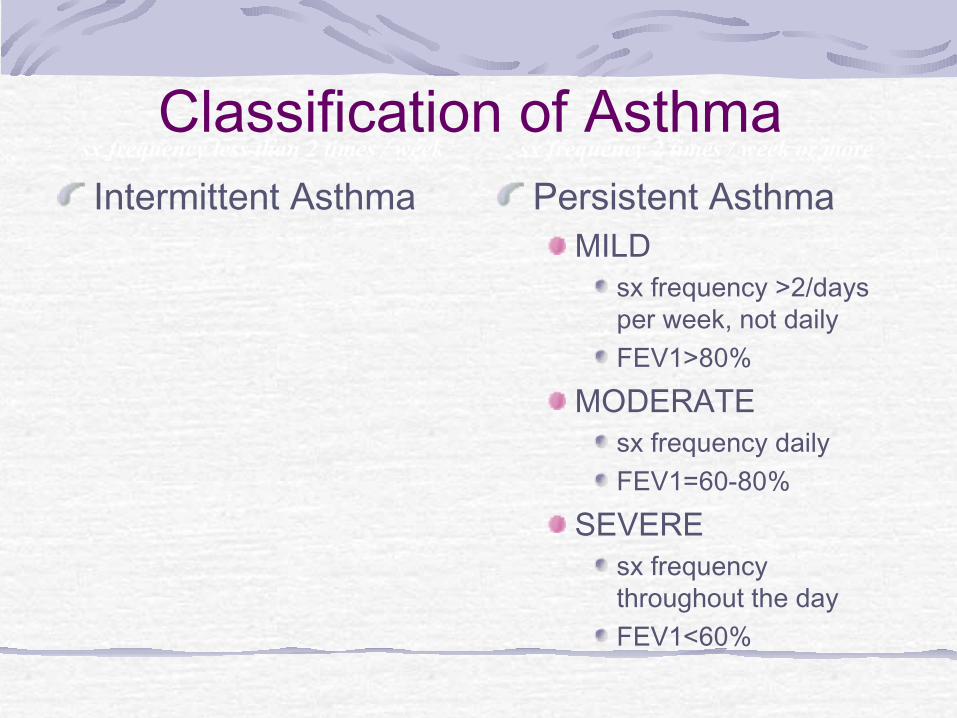
Classification of Asthma Intermittent Asthma Persistent Asthma
MILDsx frequency >2/days per week, not dailyFEV1>80%
MODERATEsx frequency dailyFEV1=60-80%
SEVEREsx frequency throughout the dayFEV1<60%
sx frequency less than 2 times / week sx frequency 2 times / week or more
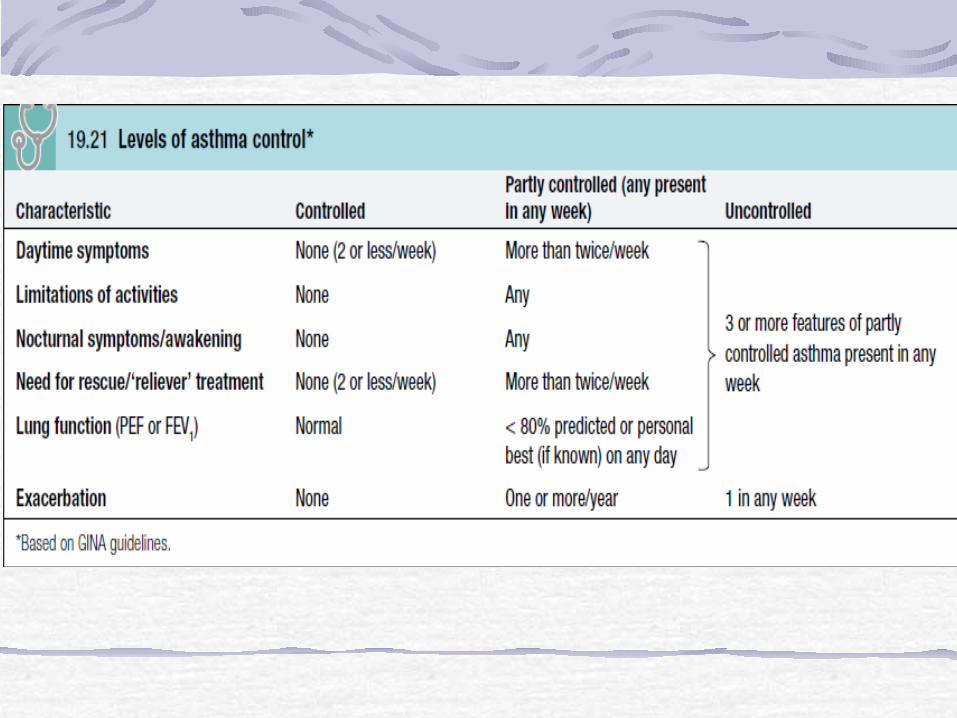
Goals of Therapy: Asthma Control
■ Minimal or no chronic symptoms day or night■ Minimal or no exacerbations■ No limitations on activities; no school/work
missed■ Maintain (near) normal pulmonary function■ Minimal use of short-acting inhaled beta2-
agonist■ Minimal or no adverse effects from
medications
Avoidance of aggravating factors
particularly important occupational asthmarelevant to atopic patients where removing or reducing exposure to relevant antigens, e.g. a pet animal, may effect improvement
House dust mite exposure may be minimised by replacing carpets with floorboards and using mite impermeable beddingMeasures to reduce fungal exposure and eliminate cockroachesMedications known to precipitate or aggravate asthma should be avoided
Smoking cessation
BRONCHODILATOR THERAPIES
beta2-adrenergic agonists, anticholinergics, and theophyllineShort-acting beta2-agonists (SABAs) such as albuterol and terbutaline – doa 3-6 hrs Long-acting 2-agonists (LABAs) include salmeterol and formoterola doa >12 hours
CONTROLLER THERAPIES
Inhaled Corticosteroids - most effective controllers for asthmaSystemic CorticosteroidsAntileukotrienes - montelukast and zafirlukastCromones - Cromolyn sodium and nedocromil sodiumAnti-IgE -Omalizumab
MANAGEMENT OF CHRONIC ASTHMA
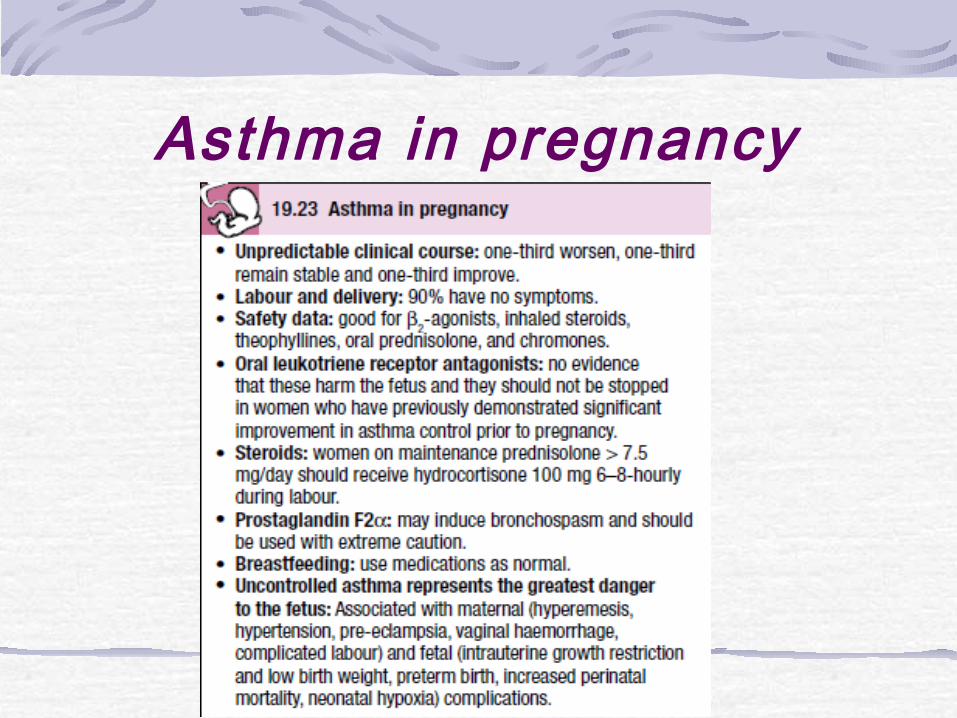
Asthma in pregnancy

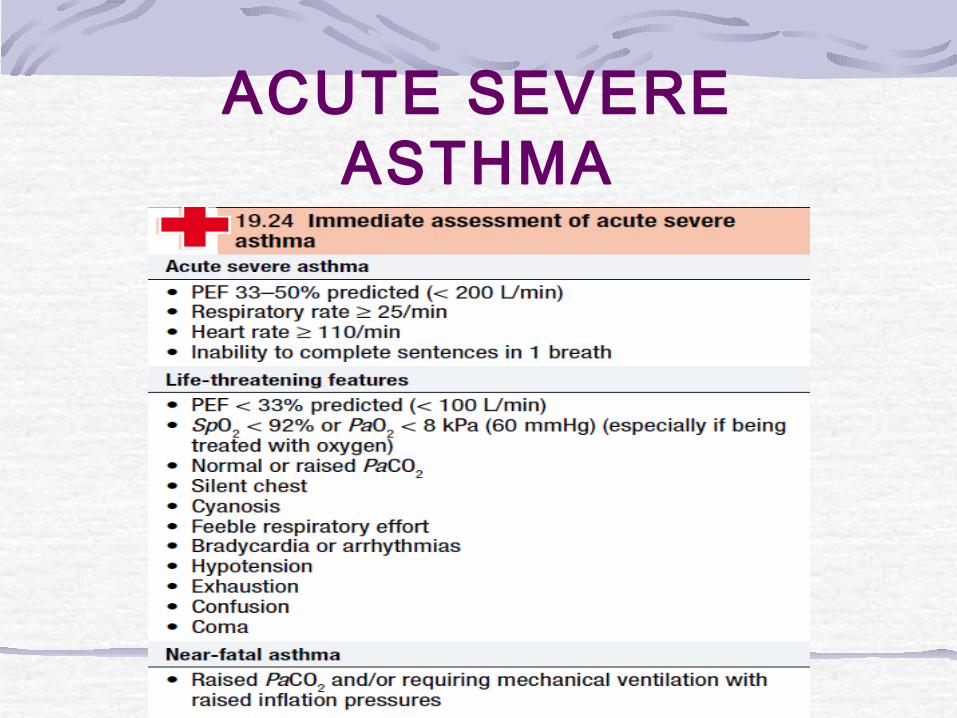
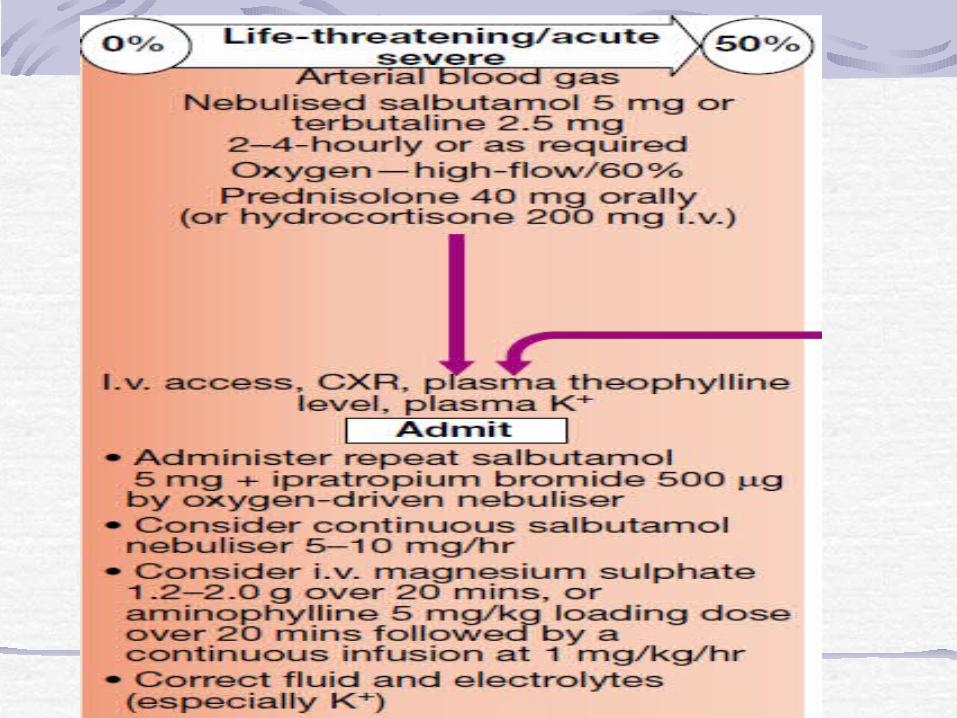
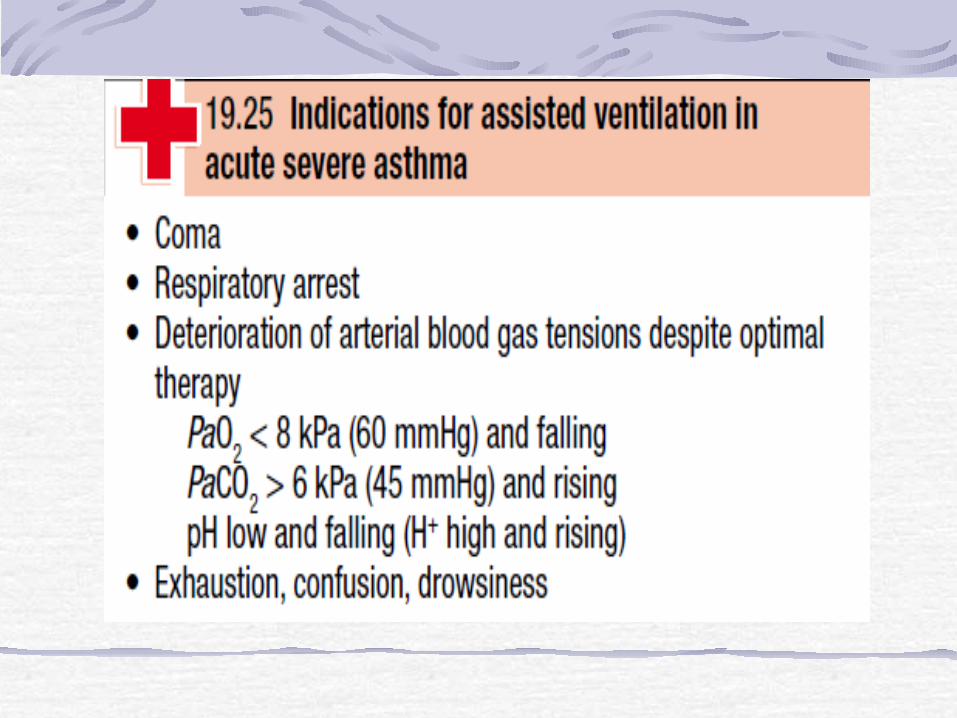
ACUTE SEVERE ASTHMA