Embed Size (px)
Citation preview

1
AUTONOMIC NERVOUS SYSTEM
ARRANGEMENT, FUNCTION, PAIN,VISCERAL SENSIBILITY IN HEALTH AND DISEASE
PRESENTED BY:DR. ROBIN VICTOR1ST YEAR PGTDEPTT. OF PSYCHIATRYSMCH

2PLAN OF PRESENTATION HISTORY ANATOMY OF ANS FUNCTIONS OF ANS PAIN DISEASE CONCLUSION BIBLIOGRAPHY

3HISTORY
The scientific investigation of anatomy, physiology and pharmacology of autonomic nervous system began after the european renaissance.
However prior to this there were glimpses of some functions of the body, such as heart action, vomiting, purgation, and sweating which were not under voluntary control and subject to some special nerves, which were supposed to carry “ animal spirits” to all parts of the body for movement and glandular action

4Aristotle (384-322 B.C.) Had supposed that heart might
be the location of consciousness as a result of its marked fluctuations under emotional conditions
It was Aristotle who was probably first to distinguish five physical senses and he considered pain to be the “ passion of soul” that resulted from intensifation of the other sensory experience

5
Descartes (1596-1650) had shown in his study of human physiology, DE HOMINI (leyden, 1662), that there are reflex actions which do not involve the brain.

6THOMAS WILLIS
The first significant anatomical appreciation of the autonomic nervous system came with THOMAS WILLIS (1621-1675).
In his book PRACTICE OF PHYSICK (London, 1684) he showed the connections between intercostal and spinal nerves.

7
In his book CEREBRI ANATOME (Lon don, 1664), with illustrations by the great architect, SIR CHRISTOPHER WREN (1632--1723), he had clearly recognized the sympathetic nervous system.

8 CLAUDE BERNARD (1813-1878)
French physiologist, brilliantly demonstrated the physiologic significance of the autonomic ner vous system with his discovery of vasomotor responses to stimulation of sympathetic nerve trunks and slowing of the heart by stimulation of the vagus nerve.

9Contd. CLAUDE BENARD’S description of the
sympathetic control of pupillary, sudomotor, and pilomotor functions as well as vasomotor function was confirmed clinically by JOHANN F. HORNER (1831-1886).
Horner showed that "Horner's syndrome," is due to a lesion of the cervical sympathetic.

10
JOHN NEW PORT LANGLEY (1852--1925),
He defined THE AUTONOMIC NERVOUS SYSTEM as “an essentially efferent system, divided it into the orthosympathetic system on the one hand, and the parasympathetic system on the other demon strating their complementary and often antago nistic physiologic and pharmacologic reactions.”

11Contd.
Using nicotine to paralyze ganglionic synapses, he was able to locate the short postganglionic fibers in the parasympathetic system as well as the long postganglionic fibers characterizing the sympa thetic system.
It was his work which definitively established our understanding of the autonomic nervous system and its complementary division

12History
contd. HENRY HALLETT DALE, who is still with us at
92, identified acetylcholine for its inhibitory effect on the heart.(1915)
REID HUNT(1870-1948) discovered the remarkable blood-pressure-lowering effects of acetylcholine and also showed that tissues are more sensitive to acetylcholine after treatment with physostigmine.

13 Otto Loewi (1873-
1961) Demonstrated (arch. Ges.
Physiol. 189: 239, 1921) that vagal stimu lation releases acetylcholine in the heart, and he further established the existence of cholinesterase( the enzyme that splits ace tylcholine)
At the same time he showed that the action of physostigmine is to inhibit this enzyme.

14ANATOMY

15What is autonomic
nervous system?? The autonomic nervous system
represents the visceral component of the nervous system. It consists of neurones located within the PNS which are concerned with the control of the internal environment, through the innervation of secretory glands, cardiac and smooth muscle

16
Development of the Autonomic Nervous System Autonomic nerves, apart from the
preganglionic motor axons arising from the CNS, are formed by the neural crest by the 5th week.
The four major regions of neural crest cell distribution to the autonomic nervous system are
cranial vagal trunkal lumbosacral.

17
Contd.
The cranial neural crest gives rise to the cranial parasympathetic ganglia, whereas the vagal neural crest gives rise to the thoracic parasympathetic ganglia.
The trunkal neural crest gives rise to the sympathetic ganglia, mainly the paravertebral ganglia, and suprarenomedullary cells.

18
The enteric nervous system is different from the other components of the ANS because it can mediate reflex activity independently of control by the brain and spinal cord
The enteric nervous system is derived from the neural crest
Premigratory neural crest cell once within the gut wall there is a regionally specific pattern of enteric ganglia formation which may be controlled by the local splanchnopleuric mesenchyme. Cranial neural crest from somite levels 1–7 contributes to the enteric nervous system

19
DIFFERENCES BETWEEN THE SOMATIC AND AUTONOMIC NERVOUS SYSTEM
SOMATIC AUTONOMIC
ORGAN SUPPLIED
SKELETAL MUSCLE CARDIAC MUSCLE ,SMOOTH MUSCLE, GLANDULAR CELL
DISTAL MOST SYNAPSE
WITHIN THE CNS OUTSIDE THE CNS
NERVE FIBRES MYELINATED PREGANG.-MYELINATEDPOSTGANG.-NON-MYELINATED
PERIPHERAL PLEXUS FORMATION
ABSENT PRESENT
EFFECTOR TRANSMITTER
ACh ACh, NORADRENALINE

20
AUTONOMIC MOTOR GANGLION Axons of the 1st (preganglionic) neuron leaves
the CNS to synapse with the 2nd (postganglionic neuron)
Axons of the 2nd (postganglionic) neuron extend to the organ it serves

21
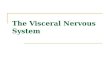
The autonomic nervous system is divided into three major parts:
sympathetic Parasympathetic enteric. These differ in organization and structure but
are functionally integrated. Most, but not all, structures innervated by the autonomic nervous system receive both sympathetic and parasympathetic fibres, whereas the enteric nervous system is a network of neurones intrinsic to the wall of the gastrointestinal tract.

22
Sympathetic nervous system Also called the thoraco-lumbar system: all
its neuron are in the lateral horn of the gray matter from T1-L2 Or L3
Has a wide distribution with the ganglia away from the organs. It innervates all sweat glands, the erector pili muscles, the muscular walls of many blood vessels, the heart, lungs and respiratory tree, the abdomino-pelvic viscera, the oesophagus, the muscles of the iris, and the non-striated muscle of the urogenital tract, eyelids and elsewhere.

23
Contd. Postganglionic fibres are long
Pre: postganglionic fibre ratio – 1:20 to 1:100
Principle transmitters / neuroeffector :---noradrenaline ---adrenalineStability of transmitter-NA is stable, hence diffuses out for wider actions

24
Parasympathetic nervous system
Also called as the craniosacral system : all its ganglionic neurons are in the brainstem or sacral level of the spinal cord
Cranial nerves 3,7,9,10. In lateral horn of gray matter from S2-S4
Distributuion is limited to head , neck and trunk with ganglia usually on or close to the organ
Postganglionic fibres are short

25
Contd. Pre : postganglionic fibre ratio – 1 : 1 or 1 : 2
Principle transmitters / neuroeffector :--acetylcholine
Stability of transmitter-ACh is rapidly destroyed hence acts locally

26

27
NEUROTRANSMITTERS NORADRENALINE: Synthesis :
TOH DDC tyrosine dopa dopamine DBH noradrenaline STORAGE: Stored in the synaptic vesicles or the granules
within the adrenergic nerve terminal. Stored as a complex with ATP which is adsorbed onto protien chromagranin.

28 RELEASE:
The nerve impulse coupled release of NA takes place by exocytosis. The release is modulated by presynaptic receptors,of which α2 inhibitory control is predominant.
UPTAKE : THREE types – 1. Axonal uptake- By active amine pump (NET)
at neuronal membrane which transports the NA by sodium coupled mechanism.
It is the most important mech.

29
Contd. 2 .Vesicular uptake—By another pump
VMAT2( vesicular monoamine transporter2) at the membrane of the intracellular vescicle,transports NA in exchange with the H+ ions
3. Extraneuronal uptake– occurs by organic cation transporters OCT1 and OCT2 into the cells of other tissues
METABOLISM: occurs mainly by the two catabolic enzymes :MAO( A & B) – located in the mitochondria in presynaptic neurons

30 COMT-Located largely out of the presynaptic
nerve terminals in the liver & other tissues the major metabolites formed are – VMA, 3-
methoxy-4-hydroxyl phenylethylene glycol, metanephrine , normetanephrine & 3,4 diOH mandelic acid.

31
Receptors : membrane bound G-protein coupled receptors ALQUIST classified them into two types α and β receptorsa receptors include-α1, a2A, α2B, α2C Β receptors include- β1, β2, β3

32Contd.
All can be postsynaptic receptors but only the a2 receptors
act presynaptically. The post synaptic receptors cause physiological function and ultimately cause signal transduction and gene expression in the postsynaptic neuron.
Presynaptic a2 receptors act as autoreceptors regulating the NA release. they act as brake for the NA neuron.

33
Adrenaline/Epinephrine Adrenaline is synthesized in the medulla of the
adrenal gland in an enzymatic pathway that converts the amino acid tyrosine into a series of intermediates and, ultimately, adrenaline.
Tyrosine is first oxidized to L-DOPA, which is subsequently decarboxylated to give dopamine. Oxidation gives norepinephrine.
The final step in adrenaline biosynthesis is the methylation of the primary amine of noradrenaline. This reaction is catalyzed by the enzyme phenylethanolamine N-methyltransferase (PNMT) which utilizes S-adenosylmethionine (SAMe) as the methyl donor

34
Differences between a1 and a2 receptors
a1 a2Location Postjuntional on the
effector organsPrejunctional on the nerve endings, postjunctional in brain. Pancreatic β cells and extajunctional in certain blood vessels
Functions observed
GU smooth muscles-contractionVasoconstrictionGland-secretionGut-relaxationLiver-glycogenolysis
Inhibitor of transmitter release.VasoconstrictionDecreased sympathetic flow.Decreased insulin release.Platelet aggregation.
Effector pathway
IP3/DAG cAMPCa2+K+ channelIP3/DAG

35
Differences between β1, β2, β3 receptors
β1 β2 β3
Location Heart,JG cells in kidney
Bronchi, blood vessel, uterus,liver
Adipose tissue
Potency of NA as agonist
Moderate Weak Strong
Selective agonist
Dobutamine
Salbutamol, terbutaline
BRL37344
Selective antagonist
Metaprolol, atenolol
a methyl propanalol
CGP20712A

36
Acetylcholine Synthesis : ATP + ACETATE + CoEn-A ACETYL CoEn-A choline acetyl transferase + Choline acetylcholine +CoEn-AStorage :Stored in the ionic solution within small synaptic vesicles but some free ACh also present in the cytoplasm of cholinergic terminals.Release:Occurs from the nerve terminals by exocytosis in response to a nerve Action Potential.

37Metabolism:
Ach is metabolized by two enzymes present in the body.These include:Specific/true- acetylcholinestaraseNon specific-butyrylcholinestarase. acetylcholine cholinesterase choline +acetate.

38
Cholinoreceptors Two classes of receptors for Ach have been
recognized: The muscarinic and the nicotinic receptors
MUSCARANIC RECEPTORS: these are selectively stimulated by muscarine and
inhibited by atropine They are G-Protien coupled receptor Location- blood vessel, eye, smooth muscle, and
glands of the gastrointestinal, Respiratory and urinary tracts, sweat glands, etc.
Five subtypes :- M1, M2, M3, M4, M5.

39 NICOTINIC RECEPTORS :
They are selectively activated by nicotine and blocked by tubocurarine or hexamethonium.
They are ligand gated cation channel : their opening causes opening of the channels and rapid flow of the cations resulting in depolarization and action potential.
Location-neuromuscular junction, adrenal medulla, autonomic ganglia.
Two subtypes:- NM and NN.

40
Differences among muscarinic receptors.
M1 M2 M3Location Autonomic
ganglia ,gastric glands, cortex, hippocampus and corpus striatum
SA node, AV node, atrium, ventricle, cholinergic nerve endings, visceral smooth muscle
Visceral smooth muscle, iris, ciliary muscle, exocrine gland, vascular endothelium
Functions Histamine release, acid secretion, learning, memory, motor function
Hyperpolarization of the SA node, dec. rate of impulse generation, dec .velocity of conduction,dec. contractility of ventricles,dec Ach release, tremors,analgesia, visceral smooth muscle contraction
visceral smooth muscle contraction, contraction of pupil, ciliary muscle contraction ,release of NO causing vasodilation

41
Contd.M1 M2 M3
Transducer mechanism
IP3/DAG3-inc. In cytosolic ca2+,PLA2 inc.—PG synthesis
K+ channel opening, dec. CAMP,
IP3/DAG3-inc. In cytosolic ca2+,PLA2 inc.—PG synthesis
Agonist Mcn-343,Oxotremorine
Methacholine Bethanechol
Antagonist Pirenzipine, telenzepine
Tripitramine Darifenacine

42
CHARACTERISTIC FEATURES OF NICOTINIC RECEPTORS
NM NN
Location and function
Neuromuscular junction: depolarization of muscle end plate-contraction of muscle
Autonomic ganglia: depolarization—postganglionic impulseAdrenal medulla-catecholamine releaseCns: site specific action
Nature Has intrinsic ion channel,pentamer of a2 β ε or γ and δ subunits
Has intrinsic ion channel,pentamer of a2 β ε or γ and δ subunits
Transducer mechanism
Opening of Na+, K+ channels
opening of Na+, K+, Ca2+ channels
Agonist PTMA , nicotine DMPP,nicotineAntagonist Tubocurarine, Hexamethonium,
trimethaphan

43
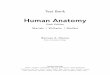
Norepinephrine projections inbrain
Norepinephrine has both ascending and descending projections.
Ascending noradrenergic projections originatemainly in the locus coeruleus of the brainstem and regulatemood, arousal, cognition, and other functions.

44Contd.
Descending noradrenergic projections extend down the spinal cord and regulate pain pathways.

45
acetylcholine projections
Two sets of acetylcholine projections are there:
Arising from the brainstem neurotransmitter centre.
Arising from the basal forebrain.

46Contd.
Acetylcholine projections originating in the brainstem extend to many brain regions, including the prefrontal cortex, basal forebrain, thalamus, hypothalamus, amygdala, and hippocampus.
These projections may regulate arousal, cognition, and other functions

47Contd.
Cholinergic neurons originating in the basal forebrain project to the prefrontalcortex, hippocampus, and amygdala; they are believed to be involved in memory

48
FUNCTIONS OF THE AUTONOMIC NERVOUS SYSTEM
The autonomic system is vital to the maintenance of internal homeostasis
The ANS is directly involved in tonic, reflex, and adaptive control of autonomic function, and integrates autonomic with hormonal, immunomodulatory, and pain controlling responses to internal and external environmental challenges

49Sympathetic nervous
system: Deals with“Fight or Flight”
known as the E division ie. exercise, emergency and embarrassment

50
Sympathetic responses are mainly mediated by the NA
Main actions include : BLOOD VESSELS-constriction of arterioles and
veins causing rise in B.P. HEART- cardiac stimulation. Increases the rate,
force and conduction velocity. BRONCHIOLES- bronchodilation EYE- contraction of the radial muscle of iris
causing mydriasis. GUT – intestinal relaxation, inhibits peristalsis and
secretion, contraction of the sphincters

51Contd.
SPLENIC CAPSULE- contraction BLADDER- Bladder trigone contraction
while Detrusor muscle relaxation resulting in retention of urine.
UTERUS- relaxation of the uterine muscle.
METABOLIC- causes glycogenolysis resulting in hyperglycemia, hyperlacticacidemia. Also causes lipolysis

52
Parasympathetic nervous system Deals with “rest and digest” Known as the D division ie. Digestion, defecation and diuresis.

53
Parasympathetic actions are mainly mediated via Ach.
Main actions include: Heart--hyperpolarization of the SA node and
decreased rate of diastolic depolarization resulting in bradycardia. Increase in the refractory period at the AV node resulting in conduction delay. Also reduction of the force of atrial contraction
Blood vessels –dilatation, fall in B.P. and flushing.vasodilation mediated by EDRF and NO
BRONCHIOLES- constricts the bronchioles and increases the secretions.

54Contd.
EYE- constriction of the circular muscle of the iris causing miosis.contraction of the ciliary muscle causing spasm of accommodation, increased outflow facility and reduction in the IOP.
GUT- Tone and peristalsis in the git is increased and the sphincters relax causing abdominal cramps and evacuation of stool
BLADDER-detrusor muscle contracts while bladder trigone and sphincter relaxation causing voiding of bladder.

55Contd.
Glands- secretion from all the glands are increased via M2 and M3 Receptors.There occurs sweating, salivation, lacrimation tracheobronchial and gastric secretion. secretion of milk is not affected.

56

57PAIN
Definition:
The International Association for the Study of Pain
Pain is "an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage"
• Monheim : “An unpleasant emotional experience usually initiated by noxious stimulus and transmitted over a specialized neural network to the CNS where it is interpreted as such.”

58
History• Derived from Latin -“Poena” meaning
punishment from God.• Homer thought pain was due to arrows shot by
God. • Plato contented, pain and pleasure arose from
within the body, an idea that perhaps gave birth to the concept that pain is an emotional experience more than a localized body disturbance.
• The Bible makes reference to pain not only in relationship to injury and illness but also an anguish of the soul.

59
Nociceptors are special receptors that respond only to noxious/damaging stimuli and generate nerve impulses which the brain interprets as “pain.”
This process is called nociception or the perception of pain
Types of nociceptors : Aδ Mechanical NociceptorsC Polymodal NociceptorsC fibre mechanical nociceptorsHigh threshold cold nociceptors
Nociceptors

60
Pain receptorsAδ – Transmit fast/sharp pain, sensitive to mechanical noxious stimuli. small, myelinated. High conductance speed: 5-15m/sec
C – Transmit slow/dull pain, sensitive to many noxious stimuli (chemical, etc.) small, unmyelinated. Slow conductance speed: 0.2-5m/sec

61
Deep tissue nociceptors
Unlike cutaneous pain, deep pain is diffuse and difficult to localize, with no discernable fast (first pain) and slow (second pain) components. In many cases deep tissue pain is associated with autonomic reflexes (e.g. sweating, hypertension and tachypnea).
Units that do not respond to mechanical stimuli have been termed silent nociceptors.Silent nociceptors are also present within the viscera. Silent visceral afferents fail to respond to noxious stimuli, but become responsive under inflammatory conditions.
mostly polymodal C- and A-fibres.

62The nociceptive mechanism
Consists of a multitude of events as follows:
Transduction: This is the conversion of one form of energy to another.
It occurs at a variety of stages along the nociceptive pathway from:
– Stimulus events to chemical tissue events.– Chemical tissue and synaptic cleft events to electrical
events in neurones. – Electrical events in neurones to chemical events at
synapses.

63
Transmission: Electrical events are transmitted along neuronal
pathways, while molecules in the synaptic cleft transmit information from one cell surface to another.
Modulation: The adjustment of events, by up- or down
regulation. This can occur at all levels of the nociceptive pathway, from tissue, through primary (1°) afferent neurone and dorsal horn, to higher brain centres.

64
• Glutamate - Central• Substance P - Central• Bradykinin - Peripheral• Prostaglandins - Peripheral
Pain Initiator
s
• Serotonin• Endorphins• Enkephalins• Dynorphin
Pain Inhibito
rs
The Neurochemicals of Pain

65
Pain Pathways From the site of pain
generation, i.e. from the periphery, the pain senses are carried by Aδ & C fibres.
Their cell bodies are situated in the dorsal root ganglion.
The central processes of the neuron, lying in the ‘sensory root’ of the spinal nerve enter the dorsal horn to terminate in the SGR ( Substantia gelatinosa Rolandi), situated in the tip of dorsal horn.

66
From the SGR, next order ( i.e. 2nd order) neuron arises, crosses to the opposite side, then moves up through the white matter of spinal cord to reach the brain.
Most of these 2nd order neurons travel up as spinothalamic tract (STT), then ultimately terminate in the proper area of thalamus, from these specific nuclei of thalamus, next order neurons arise to terminate on the cerebral cortex, at areas SI & SII as well as cingulate gyrus (which is the key area for production of some emotions).

67
At SGR, there is a synapse between 1st order & 2nd order neuron. Also there is synapse of 2nd & 3rd order neuron at thalamus.
The NT (neurotransmitter ) at the synapse between Aδ fiber & 2nd order neuron at SGR is glutamate while the NT between C fiber & 2nd order neuron (slow pain) at SGR is substance P.

68 Other 2nd order neurons, from SGR also
are known, & they also cross to the opposite side to reach different areas of brain.
The tip of dorsal horn, particularly the SGR plays a key role in modification of pain perception. It is called a gate. As a gate can be shut/ partially opened/ fully opened to control incoming traffic, so also behaves the SGR controlling the incoming traffic of pain.

69
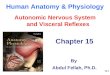
Neospinothalamic Tract for Fast Pain
The fast type A(δ) pain fibers transmit mainly mechanical and acute thermal pain.
They begin mainly in lamina I at the dorsal horn.
End in the ventroposterior part of the thalamus from where they are transmitted to the somatosensory cortex via third order neurons.

70Paleospinothalamic tract for Slow Pain
This pathway transmits pain mainly from peripheral slow chronic Type C pain fibers.
In this pathway, the peripheral fibers begin almost entirely in lamina II and III of dorsal horns of spinal cord.
End in the intralaminar part of thalamus from where they are transmitted to the frontal cortex or somatosensory cortex.

71

72
CORTICAL PAIN PROCESSING Sensory aspects of pain seem to be processed in the
Somatosensory cortex. Emotional distress associated with pain seems to be
processed in the Anterior Cingulate Cortex (ACC).
Subjects with lesions in ACC could still accurately judge the intensity of pain. But they were not in the least bothered by it.
On the other hand, subjects empathy for the pain of others only elicits activity in ACC, not Somatosensory cortex.

73
Somatosensory cortex
Anteriorcingulatecortex

74
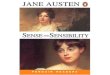
The gate control theory of pain Ronald Melzack, a Canadian researcher
proposed the gate control theory with Patrick David Wall in 1965
It asserts that non-painful input closes the "gates" to painful input, which prevents pain sensation from traveling to the central nervous system. Therefore, stimulation by non-noxious input is able to suppress pain.

75The firing of the
projection neuron determines pain. The inhibitory interneuron decreases the chances that the projection neuron will fire. Firing of C fibers inhibits the inhibitory interneuron (indirectly), increasing the chances that the projection neuron will fire.

76Contd.
Firing of the Aβ fibers activates the inhibitory interneuron, reducing the chances that the projection neuron will fire, even in the presence of a firing nociceptive fiber,

77DISEASE ASSOCIATED
WITH ANS SUBSTANCE ABUSE DISORDER -ALCOHOL RELATED DISORDER Alcohol ion channel activities associated with nicotinic Ach receptors are enhanced via alcohol.In withdrawal phase symptoms of autonomic hyperactivity are seen :Anxiety facial flushingArousal mydriasisSweating tachycardia and raised B.P.

78
AMPHETAMINE ABUSE DISORDERAmphetamine causes release of the catecholamines mainly Dopamine and Norepinephrine.Intoxication is associated with tachycardia, pupillary dilatation, elevated blood pressure ,psychomotor agitation all due to the involvement of ANS.

79
CAFFEINE RELATED DISORDERSActivation of the NA neurons has been hypothesized to be involved in mediation of symptoms of caffeine-Withdrawal and caffeine-induced-anxietydisorder. Patients are perceived as “wired” , over-talkative and irritable.

80
COCAINE ABUSE DISORDERCocaine blocks the reuptake of NA ,DA and Serotonin.Intoxication symptoms due to involvement of ANS include HTN, mydriasis and tachycardia
NICOTINE ABUSE DISORDERNicotine cause increase in the conc. Of NA which causes stimulatory effects likeimproved attention, learning, reaction time and problem solving.

81
OPIOID ABUSE DISORDERS Short term activity decreases the NA activity in the locus coeruleus Long term activity causes compensatory rebound hyperactivity.This also explains the use of CLONIDINE α2 adrenergic receptor agonist which decreases the release of NE in the treatment of the withdrawal symptoms.

82
Schizophrenia NE SYSTEM: There is neuronal degeneration withinthe neuronal reward system resulting in anhedonia
ACh AND THE NICOTINIC SYSTEM:Post mortem studies show decrease in the muscarinic and the nicotinic receptors in the caudate , putamen, hippocampus and the prefrontal cortex. They all affect cognition which is impaired in schizophrenia.

83
BIPOLAR AFFECTIVE DISORDER“ Monoamine hypothesis of depression “Depression is caused due to the Deficiency of monoamine neurotransmitters like NA, DA and 5HT.Certain drugs that deplete them cause depression and all the antidepressants act by increasing them.

84
Monoamine interaction: NE controls the 5-HT releaseNE regulates the 5HT neurons by α1 and α2 Receptors.
NE neurons from the locuscoeruleus travel to midbrain raphe and release NE on the α1 postsynaptic receptors on the 5HT neuronal bodies.it stimulates the 5-HT neurons and increases the 5HT.

85
NE neurons also innervate the axon terminals of the 5-HT neurons. Here NE released onto the α2 postsynaptic receptors inhibit the 5-HT neurons thus inhibiting the 5HT release
Role of ACh :Cholinergic agonist cause anergia, lethargy behaviour and psychomotor retardation.They can exacerbate depression.

86
Anxiety disorders Patients with all types of anxiety
disorders exhibit symptoms consistent with an exaggerated noradrenergic system
Symptoms including : Cvs: tachycardia Muscular: headache Git :diarrhea Respiratory system : tachypnea

87
PTSD There is ample evidence showing dysfunction
of NE in PTSD. The hypothesis that the noradrenergic system is hyper reactive, or sensitized, after trauma exposure is supported by findings of increased autonomic and sympathetic activity in patients with PTSD.
There have also been studies reporting increased plasma and cerebrospinal fluid (CSF) levels of NE in women with PTSD compared to healthy controls and increased levels of catecholamine metabolites in sexually abused girls when compared to non-abused girls.

88
Drugs that act to attenuate this effect by decreasing the firing of NE neurons, including substances such as:
alcohol opioids benzodiazepines, are commonly used, and abused, by patients with anxiety disorders as a form of self-medication. In structured interviews patients with PTSD reported
that these drugs reduce hyperarousal symptoms

89Da costa syndrome
In 1871 JACOB DA COSTA published a paper “ON IRRITABLE HEART “in which heDescribed the soldiers with the autonomic cardiac symptoms.Symptoms include:Fatigue on exertion Shortness of breathPalpitations Sweating Fainting headacheWHO classifies this as somatoform autonomic dysfunction.ICD--- 45.3

90
OCD Less evidence exist for
the dysregulation of the NA system in OCD.
Antecodal reports show improvement of the symptoms with the use of oral CLONIDINE.

91
ADHD Locus coeruleus plays a major rolein attention.It constitutes mainly central sympathetic system.
The peripheral NA system is more important in ADHD as there is peripheral accumulation of epinephrine which resets the locus coeruleus at a lower level.
Cardinal symptoms include: Inattention HyperactivityImpulsivity

92
One review of plasma and urinary epinephrine concentration in children with ADHD compared to non-ADHD children suggested an imbalance in the ratio of epinephrine to norepinephrine, with epinephrine being much lower than normal.
Tricyclic antidepressants (TCAs) and atomoxetine are potent norepinephrine reuptake inhibitors (NRIs), perhaps restoring a more normal ratio of epinephrine and norepinephrine.Clonidine also helps in the treatment of ADHD.
Treatment of ADHD mainly consist of central nervous system stimulants.

93PAIN DIORDERS
HYPERALGESIA Hyperalgesia is an increased sensitivity to
pain, which may be caused by damage to nociceptors or peripheral nerves.
Is divided into two subtypes: Primary hyperalgesia: describes pain sensitivity
that occurs directly in the damaged tissues. Secondary hyperalgesia: describes pain
sensitivity that occurs in surrounding undamaged tissues,

94
ALLODYNIA Allodynia is a pain due to a stimulus which does not
normally provoke pain. There are different kinds or types of allodynia: Mechanical allodynia (also known as tactile
allodynia) Static mechanical allodynia – pain in response to
light touch/pressure Dynamic mechanical allodynia – pain in response
to stroking lightly Thermal (hot or cold) allodynia – pain from normally
mild skin temperatures in the affected area Movement allodynia - pain triggered by normal
movement of joints or muscles

95
Complex regional pain syndrome (CRPS)
It is a chronic systemic disease characterized by severe pain, swelling, and changes in the skin.
It often initially affects an arm or a leg and often spreads throughout the body ( 92% of patients have reported experiencing its spread, and 35% of patients report symptoms throughout their whole body.)

96 Type I, formerly known as reflex
sympathetic dystrophy (RSD), Sudeck's atrophy, reflex neurovascular dystrophy (RND), or algo neurodystrophy, does not exhibit demonstrable nerve lesions. As the vast majority of patients diagnosed with CRPS have this type, it is most commonly referred to in as Type I.
Type II, formerly known as causalgia, has evidence of obvious nerve damage. Type II CRPS tends to feature the more painful and difficult-to-control symptoms of CRPS.

97
Phantom limb pain Is a complex phenomenon that includes a wide
variety of symptoms ranging from tingling and itching to burning and aching in the amputated limb.
Most important causes include: 1) maladaptive changes in the primary sensory
cortex after amputation (maladaptive plasticity) 2) a conflict between the signals received from the
amputated limb (proprioception) and the information provided by vision that serves to send motor commands to the missing limb
3) vivid limb position memories that emerge after amputation.

98Conclusion
The Autonomic Nervous System is vital in maintainence of the internal environment of the body in the balanced state.
Its main components that is the sympathetic and the parasympathetic system work in both complementary and antagonistic manner to achieve this.
Effect is brought about by various neurotransmitters which act on different receptors situated in many organs of the body.
Dysfunction of ANS gives rise to widespread disorders as discussed.

99BIBLIOGRAPHY
--GRAY’S ANATOMY FOR STUDENTS, 2nd EDITION. --ESSENTIAL MEDICAL PHARMACOLOGY-
K.D.TRIPATHI --KAPLAN & SADOCK’S COMPREHENSIVE
TEXTBOOK OF PSYCHIATRY, 9TH EDITION-BENJAMIN J SADOCK & VIRGINIA A SADOCK.
--SYNOPSIS OF PSYCHIATRY, 10TH EDITION-BENJAMIN J SADOCK & VIRGINIA A SADOCK.
--STAHL’S ESSENTIAL PSYCHOPHARMACOLOGY, 3RD EDITION-STEPHEN M. STAHL
INTERNET SOURCES.

100