Embed Size (px)
Citation preview
Let’s All Go to the PROM
Stirling Bryan PhD, David Whitehurst PhDThursday March 8th, 2012
Quality Forum 2012: BC Patient Safety & Quality Council
The PROMs we’re not be talking about!
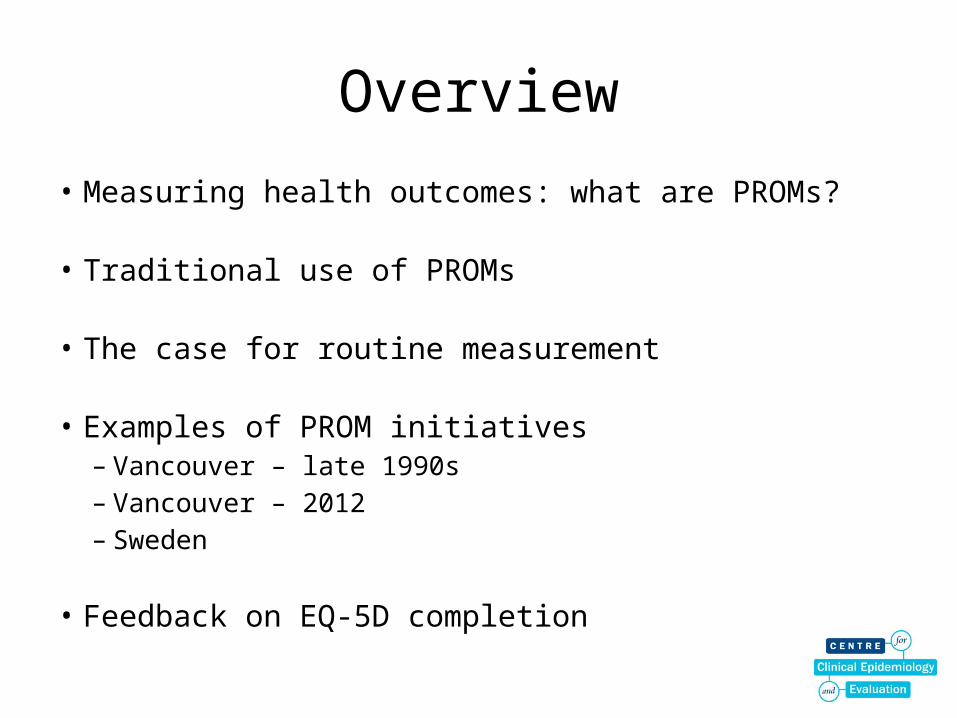
Overview
• Measuring health outcomes: what are PROMs?
• Traditional use of PROMs
• The case for routine measurement
• Examples of PROM initiatives– Vancouver – late 1990s– Vancouver – 2012– Sweden
• Feedback on EQ-5D completion
Measuring Health Outcomes
• Not a new concept: mortality & morbidity
• A wealth of information on outcomes – but with limits– Statistics Canada– Canadian Institute for Health Information (CIHI)– Poor outcomes / system failures
• What about the patient?– ‘Measurement of “success” in terms of improvements in
patients health status… is virtually non-existent in Canadian health care’ (McGrail et al, 2012)
Patient reported outcome measures (PROMs)
• Measures of health status or health-related quality of life completed by patients, commonly as a short questionnaire
• Used to assess a person’s health status at a particular point in time, or on a number of occasions
• Large number of PROMs developed over ‘recent’ years– Condition-specific measures (e.g. cataract removal, varicose
vein surgery, hip/knee replacement)– Generic measures, facilitating comparison between conditions
(e.g. EuroQol EQ-5D, Health Utilities Index, SF-36)
‘Traditional’ PROM uses
• Clinical research– E.g. Randomized controlled trials, cohort studies,
registries
• Economic evaluation research– Comparative analysis of two or more interventions
in terms of both costs and benefits
Terms you may come across
• Cost-benefit analysis• Cost-consequence analysis• Cost-minimisation analysis• Cost-effectiveness analysis• Cost-utility analysis
Increasingly, these two are the dominant
forms of evaluation
PROMs for Economic Evaluation
• Generic preference-based PROM measures– Index scores interpreted on a 0 to 1 scale– 0 = health state ‘equivalent to death’– 1 = full health
• Quality-Adjusted Life Years (QALYs)
• A number of alternatives exist
PROMs for Economic Evaluation (2)
• EQ-5D (www.euroqol.org): a widely-used measure – 5 dimensions, each with 3 levels– Defines 243 health states (35)– Scores range from -0.594 to 1.000
Example CUAs
• Statin therapy for secondary CHD prevention– Incremental cost per quality-adjusted life year (QALY) ranged
from $15,000 to $22,000– “Statin therapy is recommended for adults with clinical
evidence of CVD.”
• Anakinra for Rheumatoid Arthritis– Incremental cost per QALY in the region of $160,000– “Anakinra should not normally be used as a treatment for
rheumatoid arthritis. It should only be given to people who are taking part in a study on how well it works in the long term.”
Routine PROMs data…• The patient who has undergone surgery asks:
– Is my recovery post-surgery similar to that of other patients or should I be worried?
• The surgeon asks:– Which of my patients are experiencing on-going health problems and might
benefit from early clinical review?
• The health sector manager asks:– Which are the high performing surgical teams and what lessons can they
offer to other groups?
• The health service researcher asks:– How variable are surgical health outcomes across BC and what are the main
drivers of such variation?
Example 1: Vancouver, late 1990s
• RESIO (Wright et al, 2002)
• Participants– 138 surgeons and 5313 patients– cataract replacement, cholecystectomy, hysterectomy, lumbar
discectomy, prostactectomy, hip replacement
• Self-reported health-related QoL before and after– Generic measure: SF-36– Disease-specific instruments: e.g. VF-14 (visual function)
• Feedback of information to surgeons
Example 1: Results
• Cataracts:– 31% of patients booked for cataract surgery had a visual
function score of at least 91 (100 = no visual impairment)– Overall results positive (see figure) but 27% of patients
showed either no change or deterioration.
• Cost of the program: $12/patient
• 47% of surgeons said the exercise was of little value and did not wish to continue receiving such information
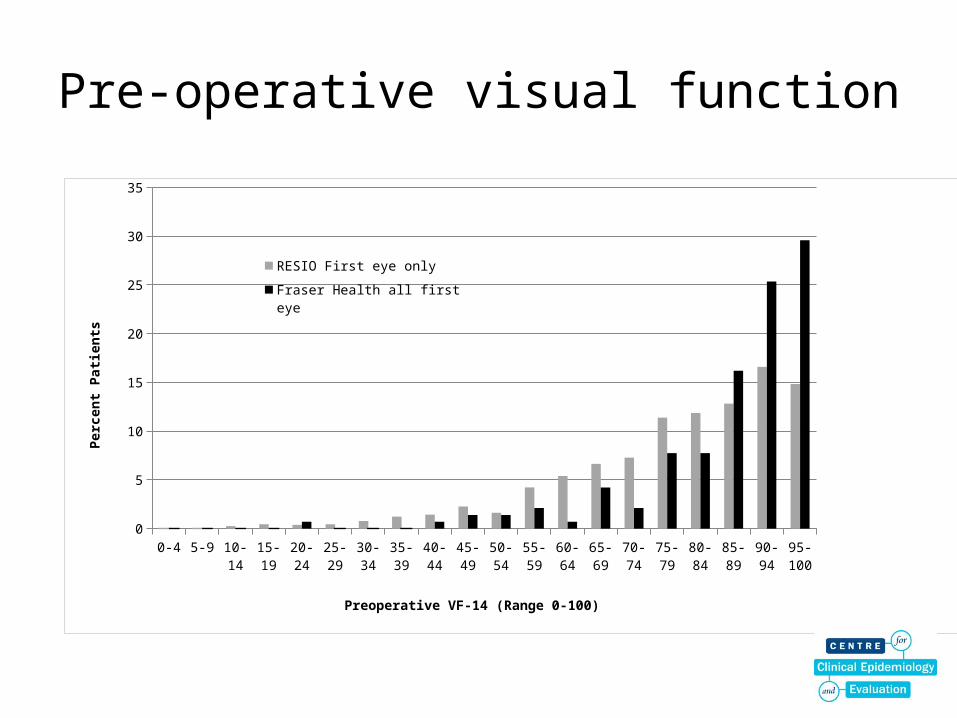
Pre-operative visual function
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90-94 95-100
0
5
10
15
20
25
30
35
RESIO First eye only
Fraser Health all first eye
Preoperative VF-14 (Range 0-100)
Perc
ent P
atien
ts
Example 2: VCH cataract outcomes
• The task:– “To implement a cataract surgery outcome
measurement strategy as a routine quality assessment tool within Vancouver Coastal Health (VCH).”
• Background:– Key issue: need full engagement of the ophthalmology
community in VCH– Culture amongst most physicians is not one of routine
and standardized measurement of indications and outcomes
Example 2: The proposal
• Development of a registry of all patients having cataract surgery done within VCH
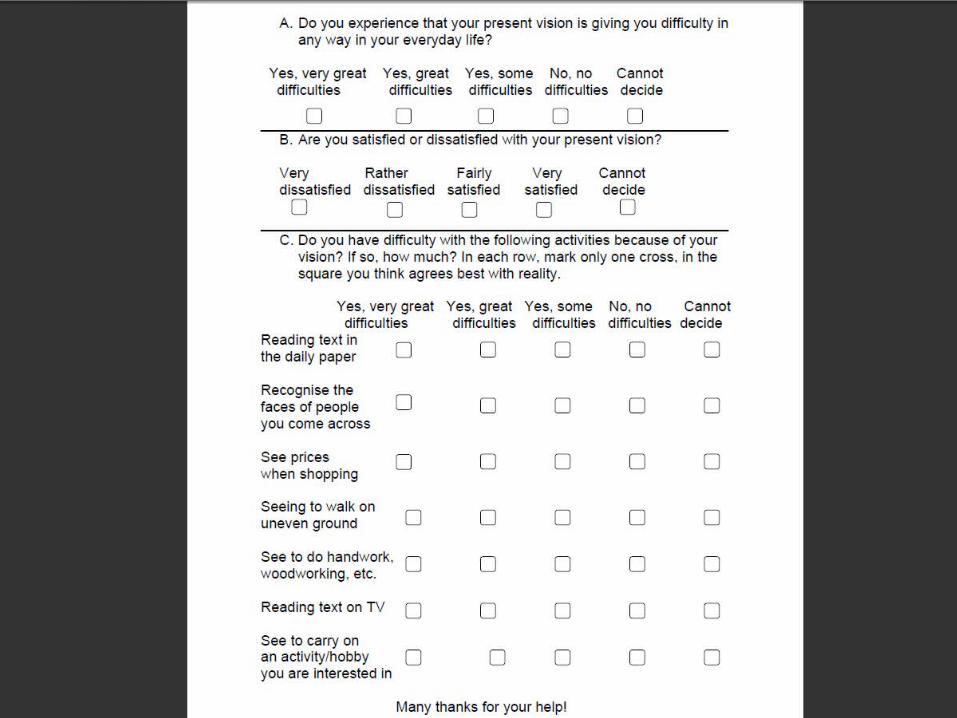
• Data will be collected on:– patient characteristics– indications for surgery– visual function before and after surgery (CATQUEST)– clinical information
• Mechanisms for data collection include:– surgery booking form (to be expanded)– Postal/online survey of patients before and after surgery
17
Example 3: Learning from Sweden?
• http://p2icare.se/en/filmer/
How’s your health?
• Your data...





![2012-13 Prom Dress Code[2] › userfiles › 127 › 2012-13 Prom Dress Code(1).pdfForest Park High School Prom 2013 Prom Dress Code To: Prom participants From: Jeff Jessee, Principal](https://img.pdfslide.net/doc/110x75/5f284715184c880cdb06d74d/2012-13-prom-dress-code2-a-userfiles-a-127-a-2012-13-prom-dress-code1pdf.jpg)