Embed Size (px)
Citation preview
Holistic BallisticsHolistic BallisticsBullet Physics and Traumatic InjuriesBullet Physics and Traumatic Injuries
Matthew Esposito, MS IV
Dr. Dene W. Daugherty
Overview
• Introduction• Ballistic Physics (hang in there)• Physical Exam• GSW Workup and Management
– Head– Neck– Thorax– Abdomen– GU
– Extremities
Introduction
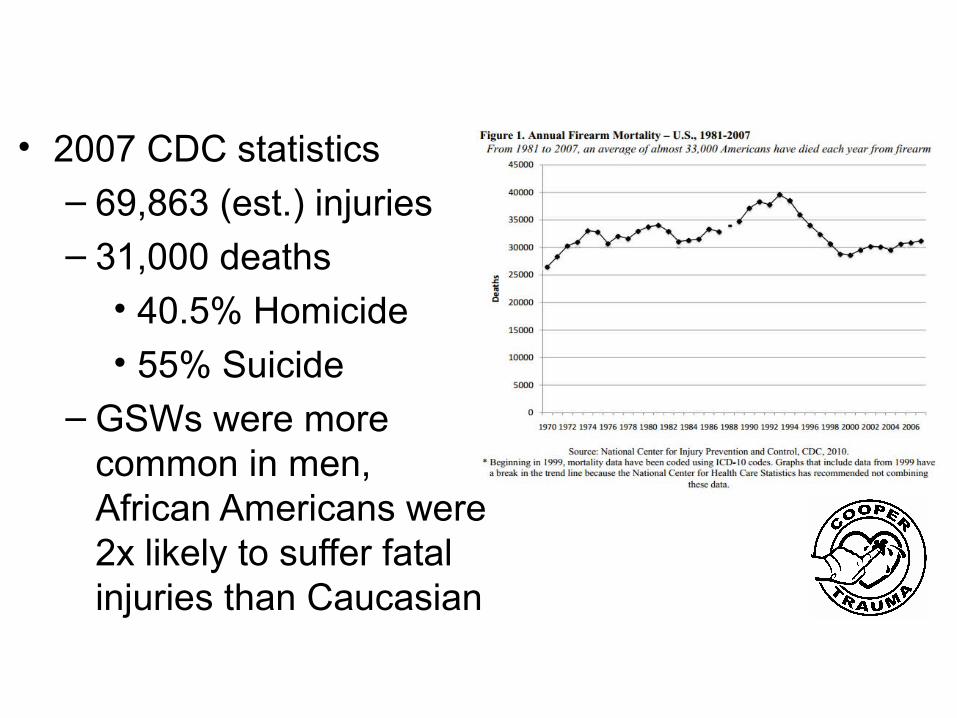
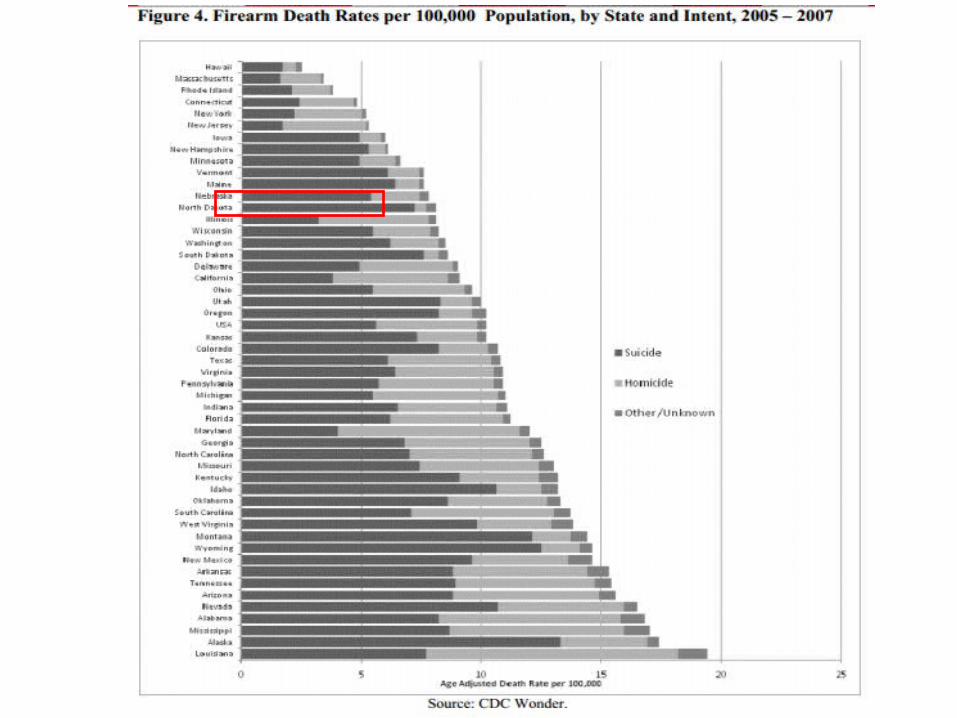
• 2007 CDC statistics– 69,863 (est.) injuries– 31,000 deaths
• 40.5% Homicide• 55% Suicide
– GSWs were more common in men, African Americans were 2x likely to suffer fatal injuries than Caucasian
Introduction
Introduction
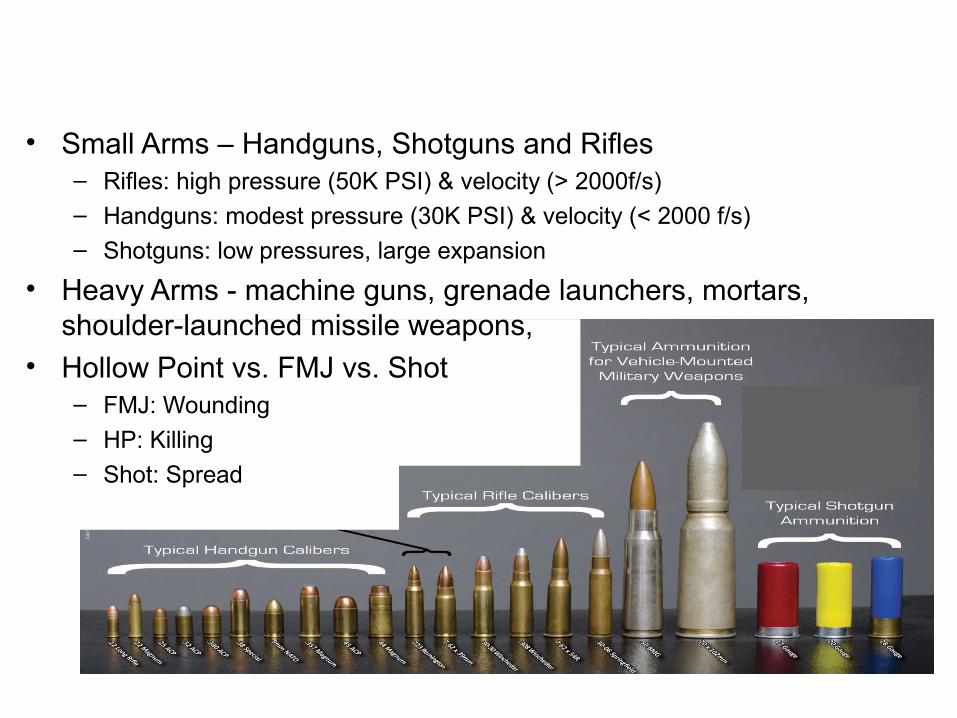
• Small Arms – Handguns, Shotguns and Rifles– Rifles: high pressure (50K PSI) & velocity (> 2000f/s)
– Handguns: modest pressure (30K PSI) & velocity (< 2000 f/s)– Shotguns: low pressures, large expansion
• Heavy Arms - machine guns, grenade launchers, mortars, shoulder-launched missile weapons,
• Hollow Point vs. FMJ vs. Shot– FMJ: Wounding
– HP: Killing– Shot: Spread
Physics
Physics 101
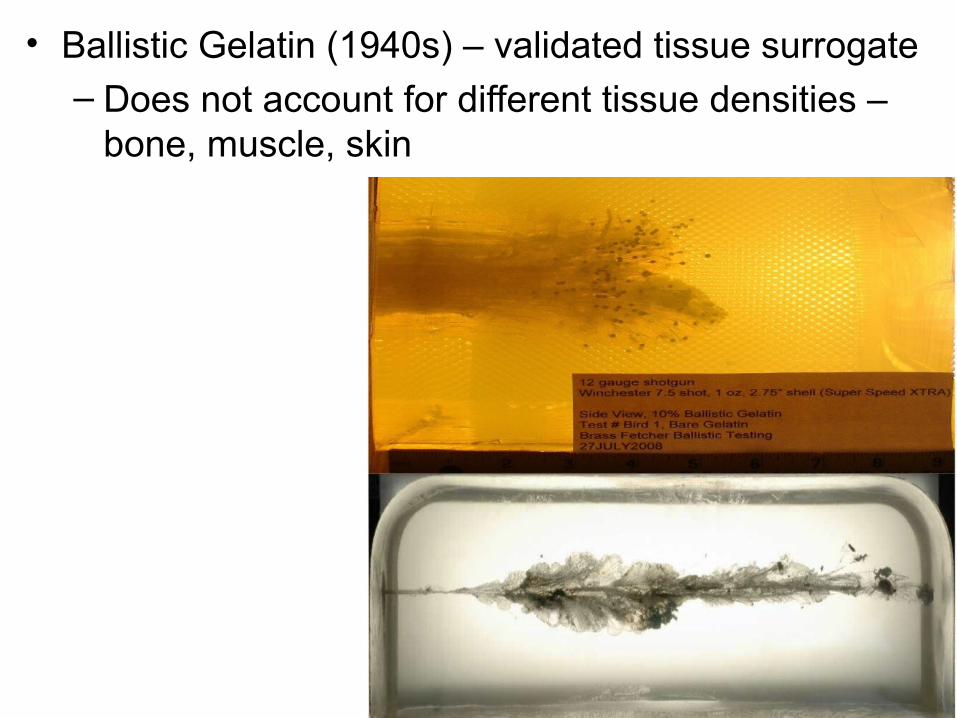
Physics• Ballistic Gelatin (1940s) – validated tissue surrogate– Does not account for different tissue densities –
bone, muscle, skin
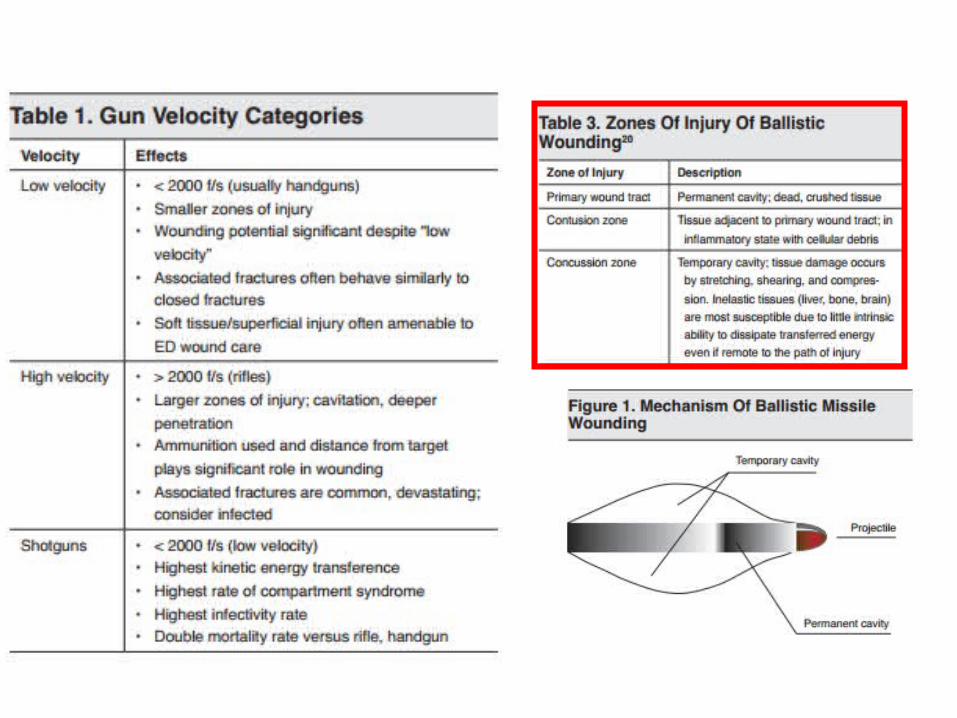
Physics• 3 Components
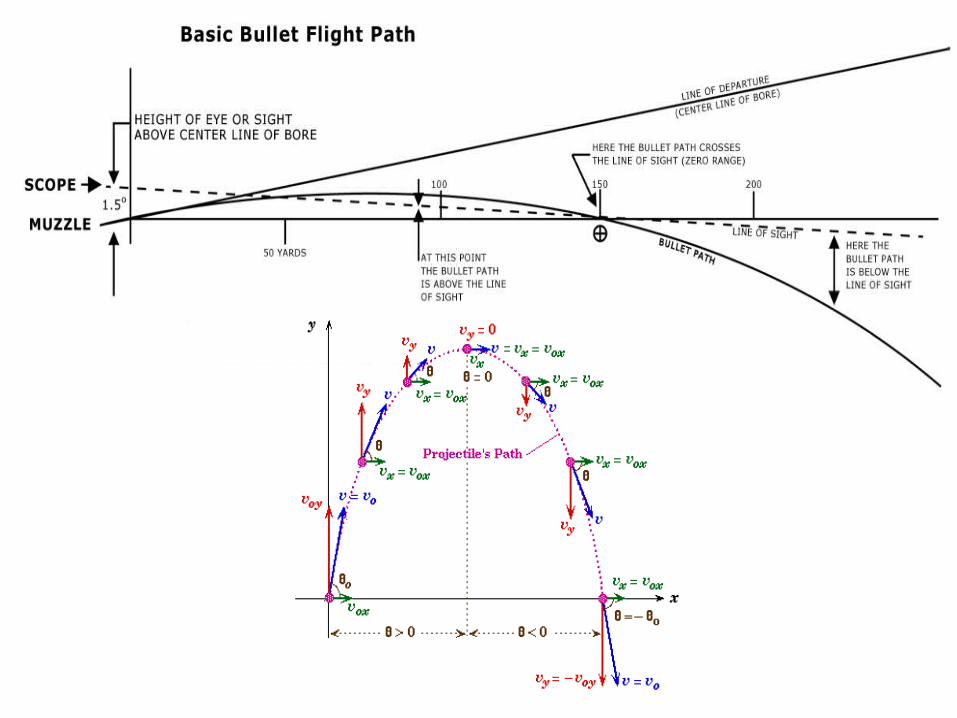
– Internal: Path of the projectile in the gun– External: Path from the muzzle to target
• gravity and air resistance– Terminal: Path inside target
• Permanent Cavity: Depends on caliber of ball• Temporary Cavity: Depends on velocity of ball,
can be 10-30x size of permanent cavity– Secondary Wounding: Newton’s 1st Law
Physical Exam• MARCHs vs. ABCDE
• Vital Signs & GCS
• Rapid Physical Assessment– DCAP BTLS– Location and Number of entry and exit wounds
• Hard vs. Soft Signs
• SAMPLE History
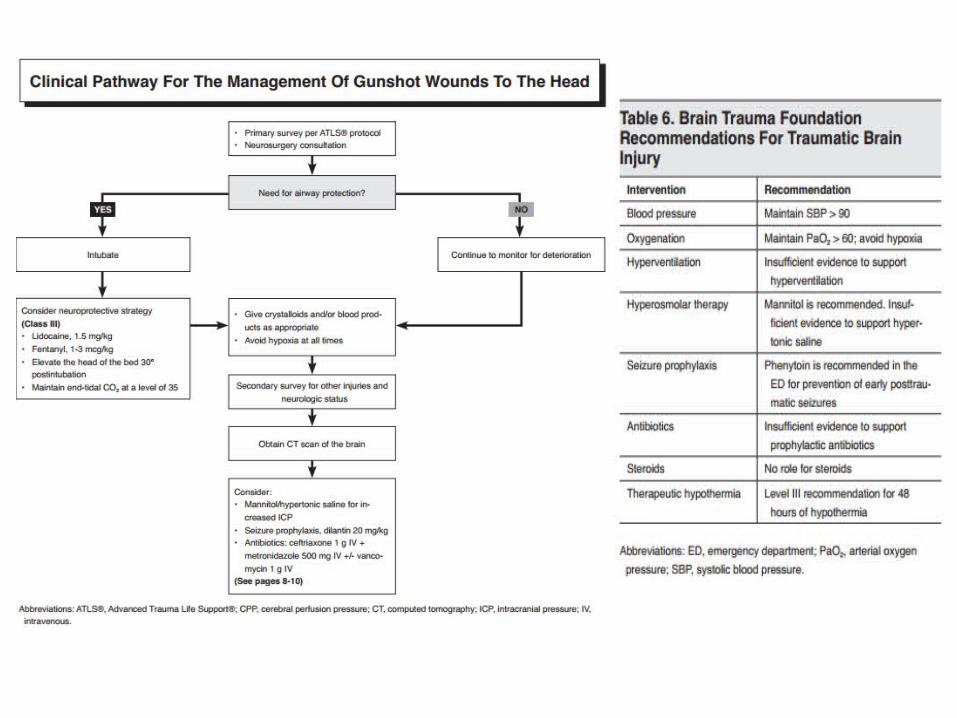
Head Injuries• Zafonte et al:
– 36% of patients dead on arrival to the ED or expired in the ED, 77% overall mortality in first 48hrs
• Eastern Association for the Surgery of Trauma– Introduced first set of guidelines for care of penetrating brain injury in 2001
• Fluid Resuscitation: Albumen vs. Synthetic Colloid vs. Hypertonic Saline• Imaging:
– Non-contrast CT
• Antibiotics: – Prophylaxis with Ceftriaxone +/- Metronidazole and Vancomycin
• Antiepleptics: – Phenytoin
• ICP Control: – Mannitol vs. Hypertonic Saline (3-23.4%)– Head of bed > 30°– No more Hyperventillation
Neck Injuries• ABCs, ATLS, Physical Examination of Wound
• Platysma violation is an indication for operative evaluation and observation for at least 24 hours.
• Airway Management: RSI and ETT with surgical backup
• Evaluation: Unstable Patient OR, Stable Patient Imaging– Zones 1, 3: Require additional imaging in a stable patient– Zone 2: Selective operative management
• Imaging: Angiography, CTA, duplex ultrasonography, direct visualization or esophagogram
• CT with angiography should be obtained to evaluate for vascular or aerodigsestive track injuries in stable patients
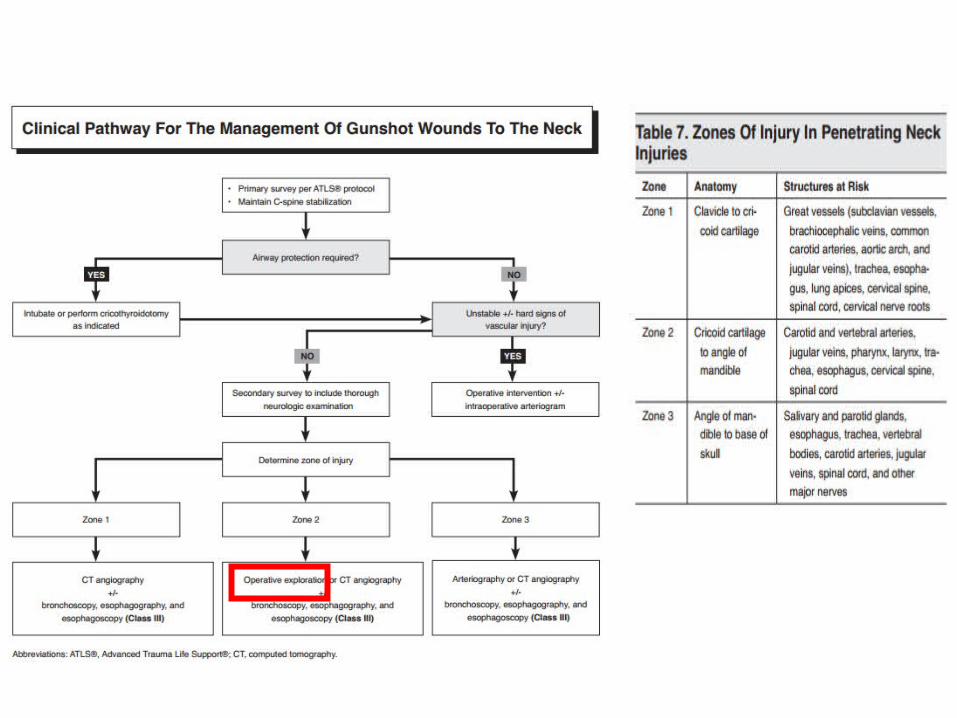
Neck Injuries
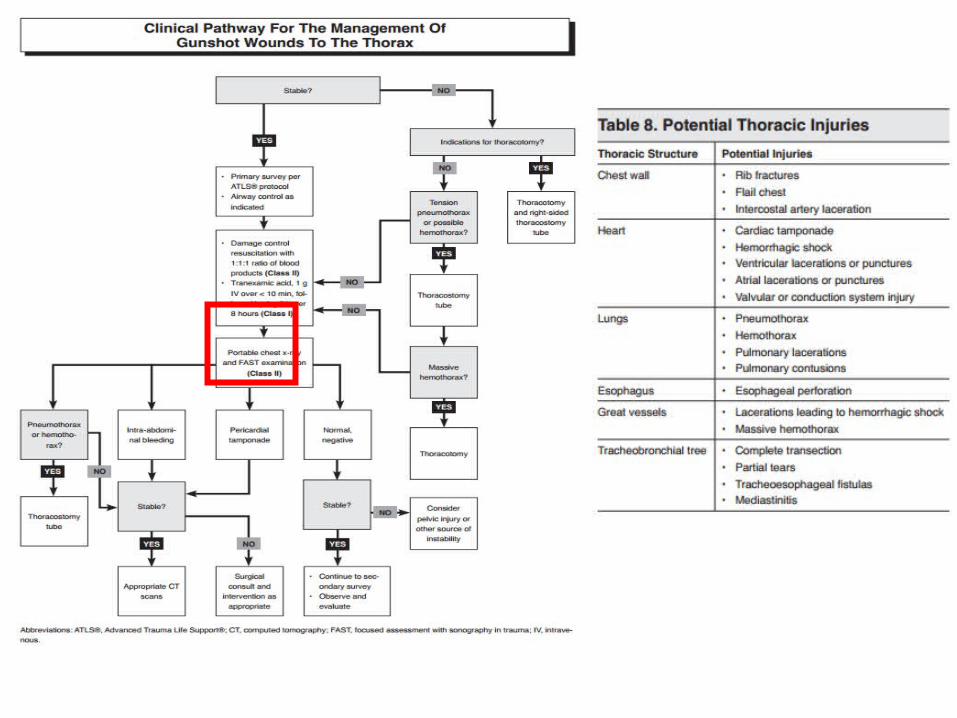
Thoracic Injuries• Major vascular injuries occur in 4% of penetrating chest trauma, if
tracheobronchial injuries are present, the proportion of patients with major vascular injuries increases to 30%. Many don’t survive to the ED
• Imaging:– E-FAST: Look for pericardial effusion, hemoperitoneum, pneumothorax, and
hemothorax– CXR: Required in all thoracic GSW
– CT: Hemodynamically stable patients, find occult injuries
• Treatment: Surgery is often the final common pathway– Thoracotomy, Needle Decompression & Tube Thoracostomy– Fluid Resuscitation (crystalloid, PRBC + FFP 1:1, TXA) – Antibiotic PPX
Thoracic Injuries
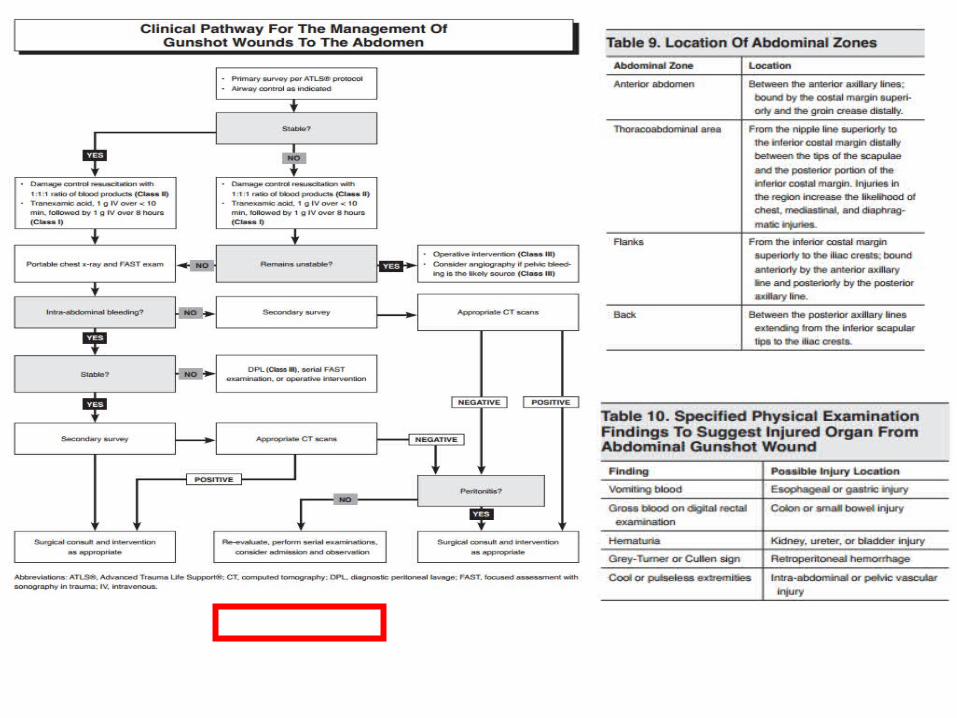
Abdominal Injuries• Hollow-organ injuries are the most common (small bowel)• CT and Ultrasound have relegated DPL to an infrequent procedure
– Still useful in an unstable patient who cant be transported to CT
• Treatment:– Fluid Resuscitation
– Unstable: Hemorrhage Control and Exploratory Laparotomy– Stable: Serial Abdominal Exams, Laboratory Values, Imaging– Interventional Radiology – Diagnostic Laparoscopy
Abdominal Injuries
GU Injuries• Only 10% of trauma patients have GU injuries and only 15% of that
subset have penetrating trauma• Few life threatening injuries except for kidney or major lacerations to
renal vasculature• Majority of injuries are to the external genitalia
• Examination:– Look for blood at meatus and gross hematuria– Retrograde urethrogram or CT cystogram
Extremity Injuries• Considerations:– Vascular and Nerve Injuries– APIs– Compartment Syndrome– Fractures– Nerve Impairment
– Joint Injuries
• Evaluation:– CTA vs. Angiography vs. Duplex Ultrasonography– Serial Compartment Checks
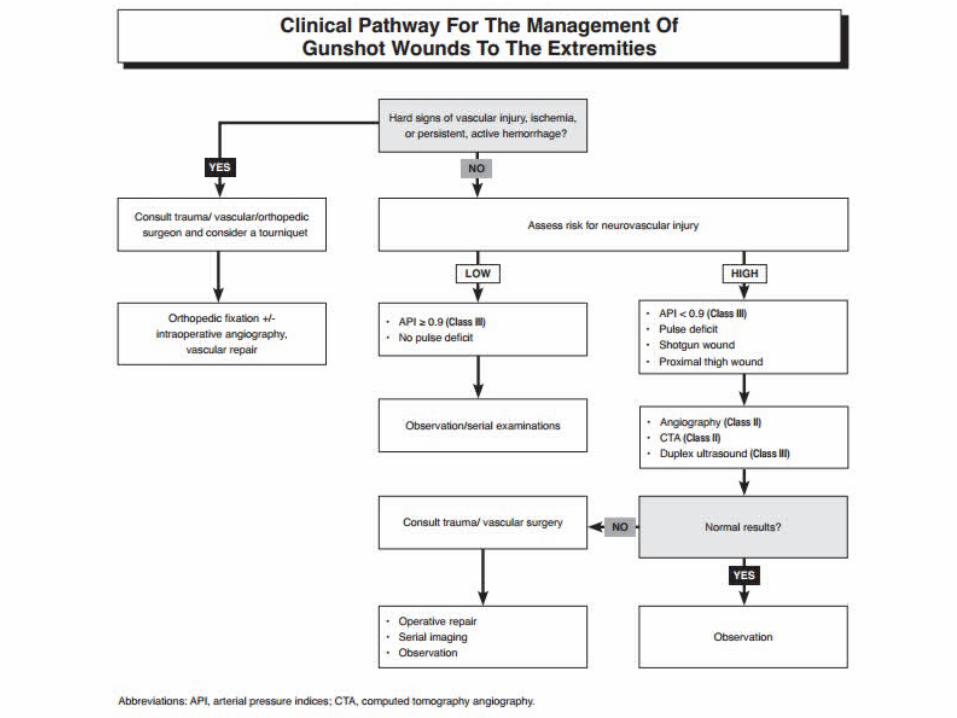
Extremity Injuries
Review
• Count the number of holes• Pan-Scan• Bullets are not sterile• Blood + FFP (1:1)
ReferencesFirearm Injury Center at Penn “Firearm Injury in the US”
Bruner D., Gustafson C., Visintainer C., “Ballistic Injuries in the Emergency Department” Emergency Medicine Practice December 2011 Volume 13 Number 12
Hollerman JJ, Fackler ML. Wound Ballistics. In: Tintinalli's Emergency Medicine: A Comprehensive Study Guide. New York, NY: McGraw-Hill; 2011.
Ong RC, Mulvaney SW. Military Medicine. In: Tintinalli's Emergency Medicine: A Comprehensive Study Guide. New York, NY: McGraw-Hill; 2011.
Fackler ML. Wound Ballistics: A Review of Common Misconceptions. JAMA. 1988;259(18):2730-2736. doi:10.1001/jama.1988.03720180056033.