Embed Size (px)
Citation preview

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000 373
PRACTICEprosthetics
Complete dentures: an introductionJ. F. McCord,1 and A. A. Grant,2
The purpose of this series is to reflect currentchanges in philosophy towards the pre-
scription of complete dentures. To achievethese aims, this series will deal with trends inedentulousness and changes in perceptions toedentulousness to the treatment modalities in complete denture provision.
This series is not intended to replace standardtextbooks of prosthodontics, but rather to serveas a chairside guide/aide-mémoire of clinicalprocedures for the general dental practitionerwith an interest in complete denture therapy.The balance of emphasis in this series has beendetermined by the experience gained in dealingwith difficulties acknowledged by practitionersand patient indictment of treatment they havereceived.
Over the past 30 years, surveys of adult dentalhealth indicate that the prevalence of people, indeveloping countries, becoming edentulous isdecreasing.1 The figures for England and Walescovering 1968 to 1988 are presented in Table 1.
In the United Kingdom as a whole, the over-all percentage of adults who were edentulousfell from 30% in 1978 to 21% in 1988.1 A par-allel study spanning 1985–1986 in the UnitedStates reported that 41% of adults over the ageof 65 were edentulous.2 According to Winklerin 1977,3 almost 50% of the 22.6 million eden-tulous Americans were 65 years of age or older.In parallel with this is the almost 50% drop inthe number of complete upper and completelower dentures (C/C) and relines providedunder General Dental Service (GDS) regula-tions between 1970 and 1990 (Table 2). Thistable also indicates the relative percentages ofthe total cost to the (dental) budget.4
Although these statements are factually cor-rect, they must be balanced, in the United King-dom at least, by two separate factors. First of all,
a significant number of general dental practi-tioners have become independent practition-ers, thus disengaging themselves from NationalHealth Service regulations, therefore manydentures provided will be unrecorded.
A second, and professionally important, factor is the finding that many (edentulous)patients when examined on routine dental visits, require replacement dentures (normativeneed) although they themselves did not feel thisneed (perceived view). This indicates thepotential for a possibly large reservoir of unmetneed in the population, in general, and in theedentulous elderly population in particular.
Clearly, although the (edentulous) percent-age of the adult population is estimated to con-tinue to decrease into the next century, theprovision of replacement complete dentures tothose currently edentulous will present a con-siderable task to the dental profession in theUnited Kingdom.5
Two factors adding to the relative complexityof this task are:
i) The reduction in teaching of prosthodontictechnology and in decreased minimumrequirements of completed cases duringundergraduate curricula. This means thatnew graduates are potentially less able toprovide a satisfactory prosthodontic service.
ii) Those patients who are edentulous arebecoming more clinically demanding eitherbecause of oral conditions present at thetime of total tooth loss or the deteriorationof anatomical, physiological and sometimespsychological well-being which often aresequelae of edentulousness.
For these reasons, a sound biologicalapproach to complete denture construction isnecessary and, although this will be emphasised
Age 1968 1978 1988
65–74 79% 74% 56%
75 and over 88% 87% 80%
All ages 37% 29% 20%
Table 1 Percentages of adult edentulous patients in England and Wales, 1968 –1988
1This introductoryarticle sets the scenefor a series of articleson complete dentureprosthodontics.
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital of Manchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 188: 373–374
In this part, we willdiscuss:• Changes in the levels of
edentulousness• Changes in the degree of
complexity of treatment ofedentulous patients
• Changes in how prostho-dontics is reported in professional journals.

PRACTICEprosthetics
374 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000
in the next three parts, the dental practitionermust be aware of the scientific basis of completedenture construction. This is of very real rele-vance in the United Kingdom, where the dentalpractitioner, at present, is the sole licensedagent to undertake clinical prosthodontic treat-ment for a patient. Practitioners should befamiliar with the technical aspects of completedenture construction in order that they maydirect the fabrication of the prostheses for which they are clinically and legallyresponsible. Failure to communicate clearlywith a dental technician cannot facilitate a har-monious prosthodontic team. The lattershould be built out of mutual respect betweenclinician, nurse, technician and patient.
Recent laboratory-based studies have indi-cated that there would appear to be an increas-ing trend towards the dental profession notfulfilling their responsibility to technical col-leagues who have received little or no trainingin relevant clinical sciences.6–8 Although two ofthese studies relate to removable partial den-tures, they nevertheless reflect a trend for clini-cians to abdicate their responsibilities in theprescription of a medical device.
While no apology should be made for anearly reference to the biological basis ofprosthodontics, due emphasis should be givento altering trends towards edentulousnessamong the population. Anecdotal and anam-nastic comments among those already edentu-lous reflect perceptions that there was aninevitability of edentulousness.9 These percep-tions were particularly prevalent among theworking classes, especially in the north ofBritain.
According to Todd and Lader,1 there wereinteresting variations in perceptions towardsedentulousness among dentate adults wearingpartial dentures and among dentate adults whodid not have a partial denture and these arelisted in Table 3.
While dental health education must be cred-ited with reduced levels of edentulousnessamong the population in general, the expan-sion of dental information in newspapers andmagazines has made the general public awareof the very real benefits of dental implants.Unfortunately, many patients do not satisfythe clinical criteria for the provision ofimplant-retained/supported prostheses. Thosepatients who are deemed unsuitable forimplants, for whatever reason, will doubtlessdevelop a negative stereotype towards conven-tional complete dentures and these negativestereotypes may make a successful outcome oftreatment doubtful.
A final aspect of perceptions towards com-plete dentures lies among the profession. Forthe purposes of this series, a survey of articleson complete denture prosthodontics in threejournals (British Dental Journal, Journal of theAmerican Dental Association and Journal ofProsthetic Dentistry) indicated that, in compar-ison to 30 years ago, the percentage of prostho-dontic articles had fallen from almost 30% toless than 10%.
Clearly this cannot be a facile comparison, asjournals should reflect alterations in trends oftreatment, and the developments during thepast 20 years of adhesive techniques have signif-icantly altered treatment trends. Concomitantwith the reduction in (complete denture)prosthodontic publications is the risk thatyounger practitioners may be deprived of theopportunity to become acquainted withprosthodontic techniques beyond conventionalundergraduate curricula.
Such a situation cannot be in the best inter-ests of those requiring prosthodontic treat-ment and the purpose of this series is to serveas a convenient chairside guide for practition-ers undertaking prosthodontic treatment. Asthis series is meant to supplement standardtextbooks of prosthodontics, references willbe used to enforce specific areas and to referreaders to key areas of general and prostho-dontic literature.
Year No of C/C No of relines % of total costC/C reline
1970 831,000 130,060 13.52 0.56
1980 509,180 99,770 6.02 0.32
1990 369,370 80,740 3.57 0.21
Figures from Dental Practice Board
Table 2 Details of the total numbers of complete dentures and relines provided under GDS regulations, 1970 –1990
1 Todd J, Lader D. Adult Dental Health,United Kingdom, 1988. London:OPCS, HMSO, 1991.
2 US Dept. of Health and SocialServices. Oral Health of United StatesAdults. National Findings. NIHPublication No. 87. 2868. 1987.
3 Winkler S. Symposium on CompleteDentures. Dent Clin N Am 1977; 21:197-198.
4 Dental Practice Board (Eastbourne ):Personal Communication.
5 McCord J F, Grant A A, Quayle A A.Treatment options for the edentulousmandible. Eur J Prosthodont RestDent 1992; 1: 19-23.
6 Basker R M, Harrison A, DavenportJ D, Marshall J L. Partial designs ingeneral dental practice — 10 yearson. Br Dent J 1988; 165: 245-249.
7 Walter J D. A study of partial denturedesign produced by an alumni groupof dentists in health service practice.Eur J Prosthodont Rest Dent 1995; 3:135-139.
8 Basker R M, Ogden A R, Ralph J P.Complete denture prescription — anaudit of performance. Br Dent J 1993;174: 278-284.
9 Fish E W. The Englishman’s teeth. BrDent J 1942; 72: 129-138.
Perception Dentate and no RPD Dentate and with RPD1978 1988 1978 1988
Very upsetting 53% 63% 34% 39%
Slightly upsetting 24% 24% 29% 28%
Not upsetting 23% 14% 27% 34%
Table 3 Perceptions of dentate adults to edentulousness

PRACTICEprosthetics
BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000 375
Clinical assessmentJ. F. McCord,1 and A. A. Grant,2
The clinician is responsible for the diagnosisand treatment of a variety of basic parame-
ters in respect of the provision of a completedenture service. These include the recognition ofa broad spectrum of the relevant and appliedanatomical, physiological and psychologicalconditions of each patient, with an understand-ing of the significance of each patient’s medicalstatus. The development of a treatment plan thatleads to the prescription of appropriate prosthe-ses follows and, finally, the clinician must ensurethat the technical requirements for each prosthe-sis are clearly communicated to the technician.Existing complete dentures which, ideally, havebeen considered to be satisfactory by the patient,should also be carefully assessed as an essentialaid to diagnosis and treatment planning.
This chapter will deal with the assessment ofthe edentulous patient and of his or her dentureas a means of determining why the patient isseeking treatment and what special problemsmight be considered. Two distinct but neverthe-less related assessments will be described,namely that of the patient and also of thepatient’s dentures.
Patient assessmentThe importance of establishing a rapport withthe patient cannot be overemphasised. Theprojection of an image as a caring and thought-ful clinician is the first step to achieving goodrapport. There are a number of simple methodsof developing good dentist–patient relations atthe outset of treatment.
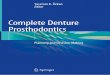
The first of these is practised by many experi-enced clinicians who take the opportunity toescort their patients from the waiting area to thesurgery. In addition to the value of the exercisegained, this philosophy affords the clinician theopportunity to assess the mien, gait and physicalappearance of each patient. Figure 1 indicates a60-year-old edentulous woman wearing com-plete upper and lower dentures that have beenworn for more than 20 years. In addition toobvious oro-facial ageing changes, there are tell-tale signs of ‘support’ problems on the bridge ofthe nose caused by spectacles. This, plus gener-alised loss of muscle bulk in the muscles of mas-tication, suggests that the patient’s biologicalage equals, or possibly exceeds, her chronologi-cal age. Early warning signs of support and ver-tical dimension problems concerning completedentures are thus clear (see Part 10).
The next, and arguably the most important,stage in both developing a rapport and effectiveassessment of the patient is to elicit the appro-priate complaints/symptoms (ie pain, loose-ness, eating, speech problems, appearance etc.)and particularly the patient’s expectations.Care should be taken to ensure that the patient’sviews are listened to and not misinterpreted bythe clinician, as this may lead to subsequentproblems. The importance of paying attentionto what the patient says is critical and the clini-cian must establish that they are in no doubtwhat the patient means. Anecdotally, manyexperienced clinicians report that patients con-fide to them that ‘you are the first dentist whohas really listened to me’. It must be stated that itis during this phase of treatment that essentialbackground information is gleaned.
The patient’s psychological needs may be metby effective communication, including theinfluence of body image on acceptance of treat-ment. Similarly, the dentist must guard againstthe development of frustrations which mayarise from communicating with an apparently‘difficult’ and demanding patient.
The medical background of the patient is alsoeasier to obtain from a patient who has had anopportunity to relax during a preliminary con-versation designed to reduce patient apprehen-sion. Dental patients may harbour fears overproblems encompassing appearance, speech orserious illness and expression of these fearsoften requires careful questioning. Many condi-tions do not present overt signs but may causeextreme discomfort to the denture patient. Forexample, a replacement denture providedbefore the detection of low-grade deficiencystates may call into question the value of theclinical service provided.1 Practitioners mayfind it useful to use a simple questionnaire toassess the medical background, and a variety ofsuch questionnaires are available.
For simplicity, the assessment of the patientwill be sub-divided into soft tissue and hardtissue assessment.
Soft tissue assessmentThe tone of the lips and cheeks may be assessedby asking fundamental questions (eg address,family details etc.) which tend to promoteunguarded replies and provide an opportunityfor useful observations. This form of question-ing will also tend to indicate the functional rela-
2In this article, helpfulguidelines are given tothe assessment ofpatients and theirdentures. A simpleassessment sheet issuggested to serve asa record of the initialassessment visit.
In this part, we willdiscuss:• General assessment of
the patient• Assessment of (oral and
facial) soft tissues• Assessment of (oral) hard
tissues• Assessment of current
dentures• Possible treatment
options.
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 188: 375–380

PRACTICEprosthetics
376 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000
tionship of the lips and tongue to the denturesin speech (Fig. 2). For example, it is generallyaccepted that the tips of the maxillary incisorteeth touch the vermilion border of the lowerlip during fricative (‘f ’ and ‘v’) sounds. This canbe assessed easily as can the assessment of sibi-lant sounds which reflect the closest speakingspace as well as the appropriate positioning ofthe upper incisor teeth. In addition, the pres-ence of facial asymmetry, atrophy or hypertro-phy should be noted.
The oral mucosa should be checked rou-tinely for the presence of ulcers, stomatitis, orfrank pathology. The clinician should alsonote the presence of adverse soft tissue attach-ments to the edentulous ridges or any otherabnormalities.
The presence of displaceable tissue, eg fibroustuberosities, hyperplasia and fibrous ridges,should be noted and this may merit considera-tion/remedial action prior to complete dentureconstruction. Similarly, the presence of mini-mally-displasive tissues should be recorded asthese may require appropriate relief to be incor-porated into the denture. A simple clinical test isto palpate the ridges firmly with a gloved finger;signs of pain or discomfort will indicate that themucosa overlying the ridge is unable to toleratemuch pressure (Fig. 3).
Hard tissue assessmentThe edentulous ridges should be assessed forform, presence of retained roots, tori anddegree of inter-ridge space. The classification of
ridge form by Atwood,2 which has been modi-fied by Cawood and Howell3 is a useful meansof describing ridge shape, although it does notnecessarily describe ridge consistency. It does,however, provide a useful aide-mémoire forinclusion in the patient’s notes. The nature ofridges eg the presence of undercuts, knife-edgeridges should also be recorded, as they requiresubtle modifications to the master casts (ierelief) prior to processing.
In addition to the above, the clinician shouldassess the quality and quantity of the patient’ssaliva. This may affect decisions regardingselection of the impression technique and, further, relate to denture-retention potential.Diminished salivary levels may also sound awarning regarding possible frictional effects onthe peri-denture tissues and may also con-tribute to altered taste perception.
When these factors have been assessed, thepresence of anatomical, physiological orpathological factors may indicate that pre-definitive/transitional treatment is required(see Part 3).
A thorough assessment of the biological envi-ronment into which a prosthesis is planned is asine qua non if the expectations and perceptionsof the patient are to be realistically gauged. Theclinician has to determine if the patient’s expec-tations are realistic and, further to establishwhether he/she feels confident that a successfuloutcome is achievable. If the patient’s expecta-tions are unrealistic and if the clinician hasdoubts that a successful outcome is outside theirpotential, then there are realistically only twooptions to consider:
• No treatment is commenced and or• Refer the patient to a clinician who spe-
cialises in prosthodontics.
This can only be answered fully if, following theabove, an examination of the patient’s denturesis made.
Denture assessmentWhile there is universal acceptance of a peri-odontal index of treatment needs4 and an indexof need for orthodontic treatment,5 prostho-dontists have been singularly unsuccessful inestablishing an index of denture quality.6,7
For that reason, a simple yet easy-to-followscheme for the assessment of dentures isdescribed. Practitioners are recommended touse a denture assessment template similar tothat in Table 1 to ensure that an accurate recordof findings is kept.
In essence, the denture assessment and den-ture-wearing history is structured as follows.(These procedures may seem tedious to the inex-perienced clinician, but it is remarkable howsimple it is to incorporate into a replacementdenture features that may be the essential causefor patients seeking replacement dentures.)
Fig. 2 Stability oflower dentures plusphonetic aspects offunction depend onthere beingappropriatefunctionalrelationship of thedentures to the lips,cheeks and tongue
Fig. 3 Mild blanchingof atrophic mucosa isevident over themandibular ridge.Palpation with agloved finger willindicate the ability ofthe soft tissue overthe ridge towithstand firm,digital pressure
Fig. 1 Lateral view of 60-year-old edentulous patient withlack of lip support and'support' problems on thebridge of her nose fromspectacle-wearing

PRACTICEprosthetics
BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000 377
General factors:Denture-wearing historyRecord the age of the present dentures, the fre-quency with which previous dentures havebeen replaced and the patient's experienceswith these dentures. Note the denture basematerials used and the condition of the den-tures, including signs and sites of obvious wearand usage. It is also a useful idea to record thedietary habits of the patient to determine therange and consistency of foods eaten by thepatient. At this stage, there is much merit inproviding the patient with a biscuit and observ-ing if and how it is eaten, the time taken to eatthe biscuit and any signs of denture instability(see Part 5).
The above, in addition to helping diagnose ifthe patient functions with the denture, must bemeasured with how the patient perceives thedenture. If function is perceived by the patientto be acceptable, and looseness and occlusalwear are the only complaints, then the clinicianshould consider the provision of dentures usinga copy or replica technique.
Specific factors:Extension of the complete upper denture • Check the peripheral extension, including
presence, fit and placement of the post dam.This may be done using a ball-ended bur-nisher to help determine the displaceabilityof tissues (Fig. 4).
• Appropriate utilisation of the functionalwidth and depth of the sulcus should be pre-sent as these relate to function (Fig. 5).
Extension of the complete lower denture• Check the extension of the denture base in
relation to the optimal available denture-bearing area, ie half-way up the retromolarpads and functional extension onto buccalshelves and lingual sulci .
• NB Appropriate extension relates to stability;instability tends to result in patients beingaware of (denture) movement in function.
Assessment of retention • Retention of the maxillary denture may be
assessed by placing the thumb on the palatalaspect of the maxillary canine and the fore-finger on the labial aspect and via a rotationof the wrist, pulling the thumb labially. Thisis an assessment of the adequacy of theperipheral seal.
• A number of factors relate to retention8,namely peripheral seal, tissue fit and sec-ondary factors such as support (displace-able tissue) and stability (muscle/occlusalimbalance). Neuromuscular control, par-ticularly in the case of dentures worn regu-larly over many years, is an importantsecondary factor.
• Testing the retentive quality of the lower den-
tures is problematic as it tends to be inti-mately associated with stability (muscle con-trol).
• A rough guide to retentive qualities of acomplete lower denture may be gauged byassessing the resistance to vertical displace-ment. This may be evaluated by asking thepatient to relax with his/her tongue at rest.Place a probe between the lower incisor teethand assess the resistance to upward pressureof the probe and denture. Although a com-ponent of stability should be present, thepresence of a peripheral seal should resistupward movement of the denture (Fig. 6).
Assessment of stability• Stability of a denture may, generally speak-
ing, be assessed via alternate pressing on theright and left occlusal surfaces of the premo-lar teeth to detect the presence of rocking orrotational movements. This may suggest thepresence of fitting inaccuracies, underutili-
Denture details: time worn Maxillary Mandible
Patient's perceptions:Acceptable (A), not acceptable (N)
Dentist's perceptions:Condition of dentures: A/N
Retention:Tissue adaptation: A/N
Peripheral seal: A/N
Border/peripheral extension:Labial to ridge: A/NBuccal to ridge: A/NLingual to ridge: A/NPosterior extension: A/N
C/C relationships:RCP: A/NOVD: A/NArticulation: A/N
Teeth: Plastic? Porcelain?
Appearance:Lip supportIncisal levelIncisal planePosterior planesAppearance
Ridges - Atwood order:I, II, III, IV, V, VI
Denture bearing tissues:HealthyAcutely inflamedChronically inflamedHyperplasticFlabbyHard tissue undercutOther
Table 1 Complete denture assessment

PRACTICEprosthetics
378 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000
sation of denture-bearing areas or supportproblems (ie flabby ridges) — this applies toboth dentures.
• Assessment of the upper denture is generallyperformed with the operator standingbehind the patient.
• The presence of inappropriate and adverseocclusal planes may result in stability problemsas may some occlusal errors. For example, ifthe upper posterior planes dip posteriorly(Fig. 7) then the effect on closure of the den-tures will be for the lower denture to slide ante-riorly, often resulting in an ulcer lingual to thelower ridge.
Assessment of dentures as functional unitsUpper tooth position• This is usually directly related to the registra-
tion visit. A variety of subtly interconnectedfactors require to be established when den-tures are assessed.
• Contribution to lip support: has the dentureprovided appropriate lip support? Upperanterior teeth placed on the ridge may affectspeech, resulting in problems of instabilitywith the lower denture and do not restore the vermilion border of the upper lip.
• Position of the mid-incisal point. This is afunction of appropriate lip support and ifthe correct position is not achieved or if themaxillary denture teeth are set on the ridge,
the mid-incisal point may be placed inap-propriately (Fig. 8). The exception is apatient who has been recently renderededentulous or has a large, undercut anteriorridge; in these cases, a full labial flange maynot be appropriate.
• Angulation of the incisal plane. A usefulguideline is that this should be parallel to theinterpupillary line.
• Angulation of the posterior occlusal planes.Conventional wisdom suggests that these bemade parallel to the ipsilateral alar-traguslines. Reference has already been made toinappropriate occlusal planes and theireffect on lower dentures.
Lower tooth position • It is generally accepted that, in the interests
of (lower) denture stability, the central fos-sae of the lower posterior teeth and the necksof the lower anterior teeth should lie over theresidual mandibular crest.
• Relation of lingual cusps to resting tongueheight. By convention, the tongue, at rest,should lie at the level of the lingual cusps ofthe lower denture.
• The presence of lingual undercuts should beavoided as these may lead to denture insta-bility (Fig. 9). This factor may be extended inthe case of patients with an atrophicmandible. In these cases, it is consideredprudent to position the mandibular teeth ina position of minimal muscular conflict(neutral zone — see Part 4).8
• The presence of molar teeth over the ascend-ing portion of the mandibular ramus tendsto encourage displacing movements of thelower denture and this practice should beavoided (Fig. 9).
Occlusal relations in retruded contactposition (RCP)The minimal requirements for any completedentures should be that they exhibit balancedocclusion in retruded contact position.9,10 In
Fig. 4 The tissuesinvolved in the postdam area are notuniformlydisplaceable. Prior todefining the form ofthe post dam on themaster cast, theclinician shoulddetermine, using a ball-endedburnisher, therelativedisplaceability fromthe midline throughthe pterygo-hamularnotch bilaterally
Fig. 5 As the attachment ofbuccinator remains essentiallyin the pre-extraction positionand as the maxilla resorbs ina palatal direction, theclinician should use thefunctional width and depth ofthe sulcus to create a moreideal peripheral seal
Fig. 6 The patient in this photograph has developedexcellent denture control via a muscular balance oftongue, cheeks and lips
Fig. 7 The inappropriate form of the posterior occlusalplanes of this upper denture will, in addition to producinga poor aesthetic result, result in unstable lower dentures

Fig. 9 The lower molars posetwo problems: 1. Their excessive bucco-lingual width presents lingualundercuts to the tongue,thereby inducing dentureinstability.2. The second molars are sitedon the ascending portion of themandible, encouraging anincline-plane effect on thelower denture
BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000 379
essence, this means that there should be simul-taneous and even bilateral contacts in RCP. Thisshould be established with the operator's fore-finger placed on the buccal periphery of lowerdentures to assist stability. The operator shoulddetect any slide, be it protrusive or lateral, asthese will tend to de-stabilise the lower denture.N.B. For protrusive and lateral movements totake place, appropriate anterior and buccaloverjets must be present and the presence ofincisal and/or cuspal locking detected andeliminated where required.
Assessment of appropriate freewayspaceThis is measured indirectly by subtracting theocclusal vertical dimension from the restingfacial height (RFH-OVD). Clinicians shoulddetermine the biological capacity of the patientto withstand occlusal loading and prescribe theOVD appropriately.
Is balanced occlusion or balanced articulationrequired?As has been mentioned earlier, the clinician isadvised to determine the masticatory needs ofthe patient at an early stage in the diagnosis/treatment planning stage. Examination of theocclusal surfaces of the dentures may assist inthe determination of whether balanced occlu-sion or balanced articulation is prescribed.Alternatively, the biscuit test or other suchfunctional test may be used. If balanced artic-ulation is selected, then continuous anddynamic occlusal contacts should be presentin border movements of the mandible, inaddition to RCP — this is demanding of theskills of the prosthodontist and of the techni-cian! The importance of assessing this occlusalrequirement should not be overlooked at thisstage. Technicians as a rule do not see patientsand thus are not able to advise on the occlusalscheme appropriate for the patient. We advo-cate that this assessment be made at the timeof the initial visit as it is part of the diagnosticprocess — most registration techniques onlyrecord RCP and do not consider occlusalrequirements of a patient.
Does the patient experience pain when denturesocclude?If this is the case, the clinician must determinewhether the cause is systemically-related,occlusally-related or related to a support prob-lem (see Part 10).
Do speech problems occur when dentures areworn?Although this will also be dealt with in Part10, the clinician should ensure that thesespeech problems are not present when nodentures are worn or with other, unassociateddentures.
Does retching occur and if so, when?This not uncommon and functional condition isbest recognised and treated prior to definitivetreatment and usually involves a period of desen-sitising and/or provision of a training plate.11,12
Assessment of appearanceAlthough strictly speaking not a functionalcomponent, this important aspect of dentureassessment does relate to the functions of mas-tication and speech. Important factors to assesshere are:
1. Appearance of anterior teeth — is thereappropriate:
• Upper lip support*• Restoration of philtrum*• Tooth shade, mould and arrangement*• Buccal corridors*• Harmony of gingival matrices of anterior
and posterior teeth*• Lower lip support**see Part 5
2. Posterior aesthetics — are these appropriate:• Occlusal planes• Anatomical and natural flow from anteriors
to posteriors• Gingival contours.
Other aspects of denture assessmentRemove both dentures and assess the following:
PRACTICEprosthetics
Fig. 8 In addition tonot being in the mid-line of the face, themid-incisal point ispoorly sited antero-posteriorly andvertically withsubsequentfunctional problems

PRACTICEprosthetics
• Impression surface of each denture. Ensureno surface irregularities are present — thesemay well induce support problems.
• Polished surfaces of each denture. Theseshould be free of undercuts and should con-form to the structures surrounding the den-ture space.
• Occlusal and incisal surfaces of each den-ture. Ensure that the relationship of teeth tothe indentation of the ridge on the impres-sion surface is as described above. In the caseof the upper anteriors, a device such as theAlma gauge may help relate these teeth to theincisal papilla (see Part 5). In the case of thelower posterior teeth, a wax knife may beused to relate the lower posteriors to theridge (see Part 8).
When the assessment of the patient and thepatient’s dentures have been made, a realisticdiagnosis of any real or potential problems,may be made. Figure 10 is an algorithm ofhow patient and denture assessments mayrelate.
Reference has been made previously to theimportance of taking into account the viewsof the patient. If the patient does not co-operate, then a successful outcome cannotbe predicted.
As with all other branches of medicine/
dentistry, the maxim ‘no diagnosis, no treat-ment’ is worth bearing in mind. Only when anaccurate diagnosis is made may a realistic treat-ment plan be formed.
Decision-making factors will be discussed inPart 3.
380 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 7, APRIL 8 2000
One may influence the other
Function - Speech - Denture space - Displacement
Reasonable?Unreasonable
Ridge from undercuts
Assessment of patient
Saliva - quality and function
Biological versuschronological age
Soft tissueassessment
Hard tissueassessment
Patient's perceptionsof dentures
Assessmentof denture
Patient's denture-wearing historyPatient's denture-wearing habitsPatient's views and expectations
of dentures
Normative assessment of denture extension, retention
and stability
Function - Anterior tooth position - Posterior tooth position - Occlusal relationship
Clinical assessment
Fig. 10 Algorithm of clinicalassessment for replacementcomplete dentures
1 Grant A A, Heath J R, McCord J F.Complete prosthodontics: problemsdiagnosis and management. P25,London: Wolfe, 1994.
2 Atwood D A. The reduction ofresidual ridges: a major oral diseaseentity. J Prosthet Dent 1971; 26: 266-270.
3 Cawood J I, Howell R A. Aclassification of the edentulous jaws.Int J Oral Maxillfac Surg 1988; 17:232-236.
4 Ainamo J, Barnes D, Beagrie G.Cutress T, Martin J, Sardo-Infirri J.Development of the World HealthOrganisation (WHO) CommunityPeriodontal Index of Treatment Need(CPITN). Int Dent J 1982; 32: 281-291.
5 Shaw W C, Richmond S, O'Brien KD, Brook P, Stephens C D. Qualitycontrol in orthodontics: Indices oftreatment need and treatmentstandards. Br Dent J 1991; 170: 107-112.
6 Pinsent R H, Laird W R E. Thedevelopment of criteria for theassessment of complete dentures.Comm Dent Health 1989; 6: 329-336.
7 Vervoorn J M, Duinkerke A S H,Luteijn F, Bouman T K, van de Poul,A C M. Reproducibility of anassessment scale of denture quality.Comm Dent Oral Epidemiol 1987; 15:209-210.
8 Jacobson T E, Krol A J Acontemporary review of the factorsinvolved in complete dentureretention, stability and support. JProsthet Dent 1983; 49: 5-15; 165-172; 306-313.
9 Basker R M, Davenport J, Tomlin HR. Prosthetic treatment of theedentulous patient. 3rd ed. P92-110,London: Macmillan, 1992.
10 Watt D M, MacGregor A R. Designingcomplete dentures 2nd ed.pp89-92 Bristol: Wright, 1986.
11 Barsby M J. The use of hypnosis inthe management of ‘gagging’ andintolerance to dentures. Br Dent J1994; 176: 97-102.
12 Barsby M J. The control ofhyperventilation in the managementof ‘gagging’. Br Dent J 1997; 182:109-111.
Helpful Hints1 Assess the denture environment.2 Assess the patient's expectations.3 If 1 is perceived to be generally
satisfactory and 2 is supportive,consider a replica denture technique.
4 If 1 is perceived to be less thandesirable by dentist and patient and2 is supportive of dentures in general,a replacement denture should beconsidered.
5 If 1 is (normatively) perceived to beacceptable and 2 is unfavourable theneither the assessment of the denture isnot thorough enough or the patient'sexpectations are perhapsunattainable. It would be sensible toenlist the opinion of a specialist — ordo not treat!
CorrectionBecause of a font problem on page 263 of issue 5 of the BDJ on 11 March 2000 in the article by P. Hollows et al. on “Delays in the referral and treatment of oral squamous cell carcinoma”, some ofthe symbols were incorrectly indicated: all c2’s on this page should read χ2. We apologise for anyinconvenience caused

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 8, APRIL 22 2000 419
3PRACTICE
prosthetics
Pre-definitive treatment:rehabilitation prosthesesJ. F. McCord,1 and A. A. Grant,2
In formulating a treatment plan for theedentulous patient, early decisions must be
made regarding essential oral tissue rehabili-tation and other necessary pre-prostheticmeasures. It is essential that the mouth is inan optimal state of health prior to commenc-ing prosthetic treatment, and failure toachieve this may well produce an unsatisfac-tory treatment result. The latter is therapeuti-cally unacceptable as well as being ethicallyquestionable.
While some patients may present for theirfirst denture with underlying conditions, it ismore common to find that those seekingreplacement appliances are in need of pre-pros-thetic treatment. This may be because of thelong-term consequences of denture wearing,and may also relate to the greater likelihood ofsystemic conditions having oral consequencesin the age group concerned.
In essence, problems that may benefit frompreliminary treatment might involve both softand/or hard tissues.
It should be appreciated that the followinglists are not exhaustive as only the more com-monly encountered conditions will be dealtwith. Rare and more complex problems shouldbe the subject of referral for treatment by a spe-cialist. The lists are included for the sake of sim-plicity, as many conditions cannot becompartmentalised and may occur simultane-ously, and be complicated by oral manifesta-tions of a general disease state.
Some treatment measures may require whatmight be termed ‘rehabilitation devices’. Theseare considered separately later in this chaptertogether with comments on their usefulness.Depending on a variety of situations, the den-
tist may find it necessary to modify the patient'sexisting dentures or, occasionally, to construct aspecial appliance, as the old denture may beirreversibly altered.
Common soft tissue conditions are:
• Tissue distortion• Denture-related stomatitis• Angular cheilitis• Fibrous degeneration of the residual ridge(s)• Border faults• Hyperplasia of the border tissues.
Common hard tissue conditions are:
• Unerrupted teeth and retained roots• Sharp bony ridges• Enlarged tuberosities• Tori and other bony prominences• Sharp mylohyoid ridges.
Common soft tissue conditionsTissue distortionA soft tissue-supported denture may become illfitting because of continuing resorption ortooth wear. Both may result in uneven forcesbeing directed to the underlying mucosa andthese tend to cause distortion of the surfacecontours of the residual ridges. This resultsfrom the unbound tissue fluid being drivenfrom its normal resting position.
An impression of the tissues in their distortedstate, when poured in gypsum, will reproducethe distorted form of the residual ridges (Fig.1). A denture made using such a cast will onlyfit the patient as well as the denture it replaces.
Distortion is most evident where thickenedmucoperiosteum is present and while somesigns of inflammation may be seen, there maybe little or no obvious signs of deformation.
Fig. 1 Thedisplacement of thisfibrous tuberosity isobvious.Displacement ordistortion of thinner,more displaceablefibrous mandibularridges will posesupport problemsfor lower dentures
This article deals withthe treatment ofcommon conditionsaffecting the denturesupporting tissues.Several preliminary(non-definitive)treatment options arepresented along witha brief account of theirrationale.
In this part, we willdiscuss:• Common soft tissue
conditions• Common hard tissue
conditions• Rehabilitation devices.
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 188: 419–424

420 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 8, APRIL 22 2000
The tissues will recover their stable form ifthe cause of the distorting force is removed andthis recovery in such cases, in theory, is a time-dependent phenomenon. At least 90 minutesafter removal of the old denture should beallowed prior to obtaining working impres-sions. Where distortion is obvious and severe,tissue recovery will take much longer and it maybe necessary for the old dentures to be removedfor several hours.
There can be no denying that the optimaldenture-related tissue option is to leave thedentures out for several hours before attendingsurgery. For most patients this is an unaccept-able option and would lead to social embarrass-ment, an occurrence that should always beavoided. Moreover, it is also not a feasibleoption to keep a patient in a surgery chair whilethe tissues resolve. The clinician, however, mayimprove matters by relieving denture under-cuts and carrying out a chairside reline using athin resilient lining material such as Visco-gel™(Dentsply Limited, Surrey) over a 24-hourperiod. Patients should be encouraged, how-ever, to remove their dentures whenever it issocially convenient to do so (ie when they are inthe house alone).
Denture-related stomatitisWhere chronic irritation of the mucosa con-tacted by a denture base has occurred, aninflammatory condition may be observed. It ismost commonly associated with the upper den-ture and may be seen as a vivid inflammation ofthe whole area covered by the denture. In theearly stages, discrete areas of pinpoint inflam-mation can be seen in the region of the palatalmucous glands. A further form is described aspapillary hyperplasia in which a nodular hyper-plasia of the central palatal area is seen.
The condition is usually symptomless andthe patient may be unaware of its presence.
A large number of causative factors have beenimplicated, the most common of which is den-ture-related trauma. The trauma may arisefrom occlusal faults (static or dynamic), poordenture hygiene, poor fit of the denture base, orroughness of the denture base. These are all fac-
tors that may be present in dentures which havebeen used over a prolonged period. The condi-tion may be associated with the presence ofCandida albicans, invasion of which appears tobe stimulated by trauma to the affected tissues,and particularly when the dentures are worncontinuously.
Other factors implicated in denture-relatedstomatitis include endocrine disorders, defi-ciency states, opportunistic infection associ-ated with antibiotic therapy and associatedwith xerostomia.
Denture-induced trauma is resolved mosteffectively when the patient is not wearing thedentures. If this is not practicable — as resolu-tion may take up to 6 weeks to effect — alterna-tive measures are required. Where the traumaarises from ill-fitting bases, stabilisation of thedenture by means of tissue conditioners may becarried out. This may have to be repeated per-haps several times until the condition isresolved, as tissue conditioners in use over sev-eral weeks can themselves be a source oftrauma.
Where occlusal or articulation faults are pre-sent, the dentures will require more radicalmodification to remove the effects of traumaand this is considered in the section on rehabili-tation devices (see previous page).
Angular cheilitisThis painful and unsightly inflammation of thecorners of the mouth results from constantwetting of the angles of the mouth by saliva. Itmay be caused by lack of lip support followingtooth extraction, poorly designed dentureflanges not providing adequate lip support orloss of occlusal vertical dimension.
Other causes include vitamin deficiencyand iron deficiency. Secondary infection bystaphylococcal organisms may occur, but itmay be associated with an intraoral candidalinfection. Where denture-related stomatitisand angular cheilitis occur together, Candidaalbicans is almost certainly implicated, inwhich case antifungal agents eg Miconazolewill be required as part of the treatment. Bearin mind that the denture in such a case is asource of infection and it must be placed in a suitable antifungicide — such as dilutehypochlorite — overnight.
Fibrous degeneration of the residual ridgeOne result of prolonged denture wearing maybe the development of a hypermobile, readilydisplaceable ridge form. This can be disadvan-tageous to the production of a stable denture.Such a readily displaceable form is also subjectto the greatest tissue distortion (Fig. 2). Thus aprolonged period of recovery is required beforecommencing the impression stage of treatmentand special impression procedures are required(vide infra).
PRACTICEprosthetics
Fig. 2 This slideillustrates a casewhere the maxillaryanterior ridge isobviously readilydisplaceable;inappropriateimpressiontechniques are likelyto result in denturesof inappropriatesurface form andtissue contact

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 8, APRIL 22 2000 421
Surgical procedures may be consideredwhere fibrous degeneration has occurred, butthese should be approached with caution andconsidered as a last resort.
Border faultsWhere a denture has been worn for a prolongedperiod of time the presence of border faultsmight be anticipated. The most common ofthese is over-extension, but where the borderswere inaccurate at insertion, then there may beregions of overextension and others of under-extension.
Where over-extension is present, the resul-tant trauma will produce tenderness, swellingand possibly ulceration (Fig. 3).
Overextended regions must be relieved andthe patient instructed to return for furtherexamination in 1 week. If, at that stage,recovery is not complete, the procedure isrepeated until complete healing has takenplace. Treatment may then proceed to theimpression stage.
Occasionally, a frenum or muscle attach-ment is so prominent that it prevents the cre-ation of an adequate peripheral seal. In suchcases, it may be necessary to consider surgicalrepositioning of a muscle attachment, orremoval of frenal tissue. The surgical treatmentmust be supplemented with the production ofa stent, or modified prosthesis, during thehealing phase in order that the operated condi-tion might be maintained. Stents will be con-sidered further in the section on rehabilitationdevices below.
Hyperplasia of the border tissuesA result of chronic irritation produced by anoverextended border may be hyperplasia of thetissue. This can be painless and the patient isoften unaware of its presence. Sometimes, how-ever, where the mass of hyperplastic tissue islarge, patients may show concern — oftenabout the possibility that such a ‘growth’ ismalignant.
The source of irritation must be removed.This requires reduction of the over-extendedflanges, or possibly removal of the entire den-ture flange. Where the areas concerned areextensive, the preferred treatment is for thedenture not to be worn. The patient shouldbe encouraged to massage the hyperplastictissue with the ball of the finger. Reduction ofthe denture flange and resolution of the tis-sue mass will have the effect of the denturefeeling loose, and the patient should bewarned of this.
Over a period of some 4–6 weeks much, if notall, of the tissue mass will resolve. Surgery maybe indicated if resolution is incomplete, but thisshould be only after the conservative approachdescribed above has been completed, and as alast resort.
Common hard tissue conditionsUnerupted teeth and retained rootsWhere there is some irregularity of the shape ofthe bone or because of painful symptoms in anapparently normal region, a radiographshould be taken of the area. This may disclose aroot or unerupted tooth or even a dental cyst.
A root or unerrupted tooth that is deep, com-pletely invested in bone and shows no evidenceof pathological change need not necessarily beremoved as undue loss of alveolar bone wouldresult. Preservation of residual bone andfavourable ridge contour is of far greaterimportance than removal of an entity simplybecause it has been discovered. The patientshould, of course, be informed of the findingsand the decision.
Where a tooth or root is only partly in boneand is in contact with overlying soft tissue, thenremoval is advised, taking into account suchfactors as the age and medical status of thepatient, etc.
Sharp bony ridgesThis condition may occur on the crest of thelower ridge in the anterior region (Fig. 4) ormay manifest as sharp mylohyoid ridges. It canbe painful for the patient owing to forces gener-ated during chewing displacing this, or evenfibrous mucosa, onto the bony spicules. Surgi-cal smoothing of such a ridge may produce tem-porary relief, but it must be appreciated thatcontinuing resorption may cause the conditionto recur. A conservative approach to overcom-
PRACTICEprosthetics
Fig. 3 The classicsigns of erythema,swelling andulceration are clearwhere over-extension hasoccurred in the (left)post dam area
Fig. 4 Occlusal view of mandibularridge. The anterioraspect of the ridge isclearly a knife-edgeprofile

422 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 8, APRIL 22 2000
ing the problem is recommended, at least in thefirst instance. This will include relief of the mas-ter cast (eg 1 mm tin foil over the relevant areaof the ridge crest of the cast) and reduction ofthe load applied to the tissue by decreasing thesize of the occlusal table or, in appropriate cases,increasing the freeway space. Where the overly-ing mucosa is displaceable, a special impressiontechnique (Fig 12a-c, Part 4) should be used.
Enlarged tuberositiesEnlarged tuberosities may be bony or fibrous innature, and it is important to discriminatebetween these by means of radiographs if it isnecessary to provide treatment. The size of thetuberosities may be such that it is impossible toinsert a fully extended denture flange eitherbecause of the size of undercut (the dentureflange prevents movement of the coronoidprocess) or the tuberosity contacts the oppos-ing retromolar pad (Fig. 5). In the experience ofthe authors, enlarged tuberosities are rarelysubjected to the surgeon’s knife or drill.
As a good rule of thumb, however, if the interarch space cannot accommodate 2 mm of den-ture base (1 mm for the upper denture and onefor the lower denture) then surgery will berequired.
Where the tuberosity enlargement is bony innature and contains an extension of the maxil-lary sinus, surgical reduction is not an easyoption. In this case the undercuts must beblocked out during denture fabrication and/ora specific path of insertion of the denture mustbe selected.
Where there is adequate bone present andwhere mobile large fibrous tuberosities impingeinto the lower ridge, surgery to produce a firm,stable base might be undertaken.
Tori and other bony prominencesBony prominences may be present in the formof maxillary or mandibular tori, prominentmaxillary midline suture or anterior nasalspine or as an exostosis in some less commonsite. The common problem resulting fromthese structures relates to the generally thinmucosal covering, relative to the overall
denture supporting tissues. This can cause dis-comfort and/or instability of a denture unlessadequate and accurate relief is provided in thedenture. The relief area must be no deeper orextensive than the case in hand requires, or lossof retention of the denture may result. If theextent of the bony prominence is ill-defined,the assistance of a disclosing paste will berequired to outline the area to be relieved.
Occasionally, an exostosis or torus may be solarge and/or undercut as to prevent dentureinsertion, or cause the baseplate to excessivelyencroach on the available space in the oral cav-ity. Particular examples are:
• Maxillary torus: If this extends onto the postdam area and peripheral seal is significantlyreduced, surgery will be required.
• Mandibular tori: If these are large enough tosignificantly reduce the width of the tonguespace anteriorly, surgery will be required.
In these circumstances, surgical modificationof the bony contour will need to be considered.
Rehabilitation devices (transitionalprostheses)This is a term that is used to describe thoseappliances which are used either as primarydevices, to prepare a patient for prosthodontictreatment, or as an adjunct to surgical pre-prosthetic procedures.
The most commonly used of these include:
• Conditioning appliances to desensitisepatients who suffer from gagging
• Pivots used to assess tolerance to verticaldimension increase
• Pivots used as a diagnostic appliance forpatients having a history of intolerance to alower denture
• Stents for use following surgery to the border tissues
• Transitional prostheses for patients withexceedingly worn prostheses.
Conditioning appliancesA conditioning appliance, or training plate, maybe provided for home use for a patient who suf-fers from nausea or gagging when wearing adenture.1 The most common causes of gaggingare looseness/rocking of the denture, excessivethickness of the posterior border of the upperdenture (particularly when it is placed forwardof the vibrating line), or a narrow arch formthat forces the lingual cusps of the upper poste-rior teeth to impinge on the dorsum of thetongue. There can also be a strong behav-ioural/psychological aspect to this problem,and as an approach to developing the necessaryconfidence in the sufferer to feel motivated toovercome the problem, a training plate can behelpful. The training plate must be fullyextended and properly tapered in thickness at
PRACTICEprosthetics
Fig. 5 Bulboustuberosities presentproblems ofplanning forretention and forinter-ridge space

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 8, APRIL 22 2000 423
the posterior border that must be providedwith a carefully formed post dam. A finger gripmay be provided so that the patient can controlinsertion and removal of the device (Fig. 6).
Additionally, psychological assessment mightbe appropriate for some patients, in associationwith some adaptational/self-controlling mea-sures such as auto-hypnosis and controlledbreathing (see Part 2).11,12
Occlusal pivot appliancesWhere excessive freeway space is present withexisting dentures, it is not advisable to increasethe denture height beyond some 3 mm at a timeunless the tolerance of the patient to a greaterincrease is first determined. This can beachieved by the use of occlusal pivots.2
Occlusal pivots consist of two flat-surfacedpillars of acrylic resin placed bilaterally in thesecond premolar and first molar region of thelower denture. These planes must contact theopposing teeth of the upper denture bilaterallyand evenly. Pivots can also be used where agross error in the retruded contact position(RCP) of occlusion is present, to increase thestability of the denture bases and thus reducetrauma to the underlying tissues.
Pivots are made using thin tin foil placed on apaste of self-polymerising polymer (methylmethacrylate) (PMMA) added to the occlusalsurfaces of the second premolar/first molarregion of the lower denture. The denture isseated in the mouth and the patient instructedto close gently into RCP. Closure must ceasewhen bilateral contact is made to prevent dis-placement of the acrylic dough. The denture isthen removed from the mouth and the PMMAcured, after which the occlusal contacts are con-firmed as simultaneously bilateral and at therequired occlusal vertical dimension.
The tin foil is then removed and the occlusalpivots are polished with the occlusal surfacesmade flat.
Given the increased trend towards potentiallitigation, there is merit in considering adapt-ing this technique by applying the pivots to a‘copy’ denture, to ensure that the patient’soriginal denture remains intact, in case theoutcome of this treatment does not prove to besuccessful.
Other applications for pivotsIf a patient has never successfully managed acomplete lower denture, or is unable to providea reproducible RCP, occlusal pivots may behelpfully prescribed initially in the replacementdenture. In such cases, denture production pro-ceeds conventionally up to the trial denturestage, after which the lower posterior teeth areremoved and replaced by wax pivots. These areconverted to PMMA pivots during processing(Fig. 7).
As with the pivots described earlier, care must
be taken to ensure that occlusal contact on theflat planes is bilateral and even.
In review visits, occlusal adjustments can bemade and pressure relief provided as necessary,until comfort and a reproducible RCP isachieved. When this occurs, an occlusal regis-tration can then be obtained and the posteriorteeth added.
StentsWhere border tissues have been subjected tosurgery, such as for muscle attachment reposi-tioning, frenal tissue excision, or a sulcus deep-ening procedure, a stent will be required to beused during the healing phase. The stent ismade prior to surgery and is inserted immedi-ately at the operation. If this sequence is not fol-lowed, there is likely to be a marked loss ofsulcus depth rendering denture base extensionand consequent compromise to retention andstability of the denture.
The stent must be of the form and requiredextent of a denture base. It is essential that theperiphery of the device is highly polished, ofrounded form having a minimum thickness of2mm.
‘Stents’ are also recommended, in the form ofa surgical template, in dental implant surgery.When the wax try-in has confirmed the posi-tion of the teeth on the implant-supportedprostheses, the try-in is duplicated in translu-cent PMMA and this surgical template is modi-fied lingual to the anterior teeth to give an
PRACTICEprosthetics
Fig. 7 Completelower dentureprocessed in the form of lower pivot prosthesis
Fig. 6 Training platewhich may be used inthe treatment of apatient with aretching problem

Fig. 8 Example oftranslucent stentused prior to theplacement of dentalimplants. Note theremoval of basematerial, lingual tothe suggestedanterior toothposition, to facilitateplacement of thebone drill andsubsequent implants
424 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 8, APRIL 22 2000
indication to the placement of the implants(Fig. 8).
Although most general dental practitionersmight not be normally expected to make suchprostheses, they should be aware of the fact thatthey may be requested to make one by an oralsurgeon, to whom they have referred a patient.These stents for either soft tissue managementor implant placement, should be planned bythe clinician providing the restorative careprior to surgery.
PRACTICEprosthetics
1 Basker R M, Davenport J C, TomlinH R. Prosthetic Treatment of theEdentulous Patient. p184-185.London: Macmillan Press Limited.
2 Watt D M, MacGregor A R. Designingcomplete dentures. 2nd ed. p96-98.Bristol: Wright, 1982.
Helpful Hints1 Attempt to restore soft tissues to
appropriate level of health prior tocommencing replacement dentures.
2 If hard tissue enlargement is such thatinter-arch space will not permitplacement of minimal denture bases,or if tongue space is constrained, pre-prosthetic surgery will usually beindicated.
3 Occlusal pivot appliance therapy isuseful where patients have worndentures over a lengthy period.Although the technique is simple,there is merit, for medico-legalreasons, in copying the existingdenture and modifying the copy as atransitional denture — the existingdenture is thus unaltered and can assuch be returned to the patient if asuccessful outcome is not achieved.

484 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000
PRACTICEprosthetics
Impression makingJ. F. McCord,1 and A. A. Grant,2
Following on from the diagnostic andpreparatory phases of treatment, the
impression visits provide the clinician with theopportunity to confirm the diagnosis of oralconditions and, of equal importance, to deter-mine the likely degree of patient compliance tothe treatment.
According to the Oxford English Dictionary,an impression is an imprint produced by ‘thepressure of one thing upon or into the surfaceof another’. This implies an active role and not apassive role and the clinician should considerthat impressions are made, not taken.
With this philosophical principle established,impression making for complete dentures maybe categorised as follows:
Primary impressions• Conventional techniques• Template techniques
Definitive impressions• Conventional techniques• Selective pressure techniques• Functional techniques• Reline and rebase techniques (including
secondary template impressions).
In this chapter, considerable emphasis is placedon impression techniques, as recent studiesindicate that flawed impressions account for themajority of denture problems.1 Two principalpoints to mention here are especially relevant.Lower impressions tend to be ‘short’ of theretromolar pads and do not accurately recordthe functional forms of the floor of the mouthand the retromylohyoid fossae. These deficien-cies tend to result in an unstable denture. The
importance of recording the form of the floor ofthe mouth in relation to the mylohyoid muscleand the retromylohyoid fossae cannot beunderstated.
Primary impressionsRecent guidelines from the British Society forthe Study of Prosthetic Dentistry (BSSPD) statethat the requirements of the primary impres-sions are that they should accurately record clin-ical relevant landmarks of the edentulousmouth without excessive tissue distortion.2 Thisimplies that, by definition, the resultant impres-sion is overextended. These guidelines also rec-ommend the practice of using rigid stock trays,modified as necessary to ‘fit the form of the den-ture-bearing area’. Table 1 lists the anatomicalfeatures that should be recorded.
A list of techniques will now be presented, tofacilitate choice for the practitioner.
The basic function of primary impressionsfor complete dentures is to outline support. Asecondary function is to provide the basis of aprimary cast on which a customised or ‘special’tray is made.
Trays for primary impressionsA large variety of trays is available for selec-tion; some trays are metallic and have fixedhandles, some are plastic with fixed or attach-able handles. Although any tray could be used,consistently successful results tend to be pro-duced when rigid trays of appropriate exten-sion are used, especially when recordingimpressions of the mandibular arch (Fig. 1).
Trays for primary impressions tend to beselected from a supply of ‘stock’ trays which aredesigned to cover a broad range of arch forms
4
Maxillary arch Mandibular arch
i) Residual ridges, tuberosities i) Residual ridges and retromolar and hamular notches. pads.
ii) Labial and buccal sulci. Muscle ii) Labial and buccal sulci, muscle attachments and fraena. attachments labial to ridge
iii) Hard palate and the functional and fraena.area between hard and soft iii) Lingual sulcus, lingual fraenum,palate. mylohyoid ridge and
retromylohyoid arch.
Table 1 Salient anatomical features of denture bearing areas
In this section, theclinical and technicalaspects ofconventionalimpression makingare discussed andillustrated. In addition,examples of selectivepressure impressiontechniques andfunctional techniquesare presented.
In this part, we willdiscuss:• Rationale and practice of
primary impressions• Planning of ‘special’ trays• Rationale and practice of
definitive techniques• Further examples of good
practice concerning teamwork
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 188: 484–492

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000 485
PRACTICEprosthetics
and sizes. The clinician should examine theedentulous mouth and assess the length andwidth of the arch to be restored. When assessingthe stock trays for size, the clinician is advised toplace the distal portion of the tray just distal tothe posterior landmarks of the tuberosities inthe upper arch, and onto the retromolar pads ofthe lower. This enables the clinician to visualisethe width of tray required to record the func-tional width of the sulcus ie the tray shouldextend 5 mm beyond the external surface of theresidual ridge.
By keeping the posterior aspect of the tray inplace and rotating the anterior portion of thetray towards the labial sulcus, the clinician candetermine if the tray is of an appropriate length.
Care taken at this stage will ensure that over-large trays are avoided — this will reducepatient discomfort and reduce the likelihood ofthe incorporation of tissue folds at this stage.Under-sized trays will result in problems for thetechnician making the customised trays onundersized primary casts (Fig. 2). In conse-quence, the clinician will experience problemsas undersized primary impressions commonlyresult in the production of inadequate defini-tive impressions and these may result in sup-port and/or stability problems in the processeddenture.
Selection of impression materials A variety of materials may be used to recordimpressions for complete dentures (Table 2).
These materials differ in their ability to dis-place soft tissues and many clinicians hold fixedviews regarding the clinical effectiveness of eachmaterial. These arguments are possibly lessvalid in the case of maxillary impressions,where an experienced clinician may obtainacceptable results with a well selected tray andmany of these materials. Figure 3 illustrates anacceptable primary impression using animpression compound and a rigid stock tray —this result should be achievable by all practi-tioners.
Care is required, however, in the lower arch,as a poorly chosen tray and a conventional irre-versible hydrocolloid impression material maynot give the acceptable result obtained withmore viscous materials.
Impression techniqueConventional techniqueWe would urge that clinicians reject the philos-ophy that ‘it’s only the first impression’, as poorprimary casts do not provide a good basis forcustomised trays, nor do they earn the clinicianthe respect of the technician.
When the stock tray of appropriate size hasbeen selected, there is merit in practising inser-tion of the tray; ideally the clinician should bepositioned to one side and behind the patient.In addition to confirming that the tray is suit-
able for size, it allows the clinician to educatethe patient on how to control his breathingduring the recording of the impression.
When the upper tray has been loaded withthe impression material, and the upper lipeverted, the tray is held inferior and anterior tothe incisive papilla. The tray is inserted upwardsand backwards to fill, first of all, the labial sul-cus, then the left and right sulci before thepalatal area is pressed into position. The clini-cian may have to change the operating hand toensure the impression material records theright and left sulci.
With lower impressions, the clinician standsto one side in front of the patient, the tray isheld over the lower ridge and the loaded traydepressed, the labial, right and left sulci in turnbeing everted to permit the impression materialto fill the functional width of the sulci.
Fig. 2 This slideillustrates one of theproblems faced by atechnician when anunderextendedimpression has beenmade of theposterior lingualpouch (arrowed)
Fig. 3 Well-formedimpression of(lower) lingualsulcus area
Fig. 1 An example ofrigid, appropriatelyextended trays forprimary impressions.The benefits of trays of this form,especially in theretromylohyoid area, have beenendorsed by BSSPDguidelines

486 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000
PRACTICEprosthetics
Figure 4 illustrates two impressions, using atwo-phase hydrocolloid™ (Acudent Researchand Development Co. Inc., 85 Industrial Way,Buellton, California 93427, USA), each ofwhich clearly records the denture-bearing area.The gel of the thinner phase is syringed into thesulci and the viscous phase is located onto thetray. In each case, the denture-bearing area isoutlined in indelible pencil onto the completedimpression; this is to assist the technician whenthe customised tray is to be made. Impressionsshould be disinfected, in conformance to localhealth and safety guidelines, before being cast.
Before dispatching the primary impressions,or the primary casts if the dentist or his dentalnurse has cast the impressions, the clinicianshould indicate to the technician the require-ments of each customised tray, eg spacing, pres-ence of handles, etc. In the case of customisedtrays for complete dentures, we recommend
that the technician does not perforate the trays,as this inhibits the determination of a periph-eral seal (vide infra).
Template techniqueThere are occasions when either the patientwishes to have a copy made of his dentures, orthe dentist elects to replicate the form of thepolished surfaces of the dentures to help thepatient’s adaptation to the new dentures. Sev-eral clinical techniques have been advocated3–5
and they share the philosophy of fabricating amould which contains the denture to be repli-cated (the template). The material investing thedenture to be copied may be irreversible hydro-colloid or silicone rubber of putty consistency.When the denture is removed, wax or autopoly-merising resin is poured into the mould to fillthe occlusal aspects of the mould. Acrylic resinis then poured into the closed mould via inletsto fill the denture base and the replica dentureprepared before definitive impressions (Fig. 5).
Definitive impressionsAccording to the BSSPD guidelines, defini-tive impressions ‘should record the entirefunctional denture-bearing area to ensuremaximum support, retention and stabilityfor the denture during use’.
The primary purpose of definitive impres-sions, therefore, is to record accurately the tis-sues of the denture-bearing areas, in addition torecording the functional width and depth of thesulci. As has been discussed previously, there is a
Impression material
Impression compound
Tracing stick (greenstick)
Compound/greenstick admix
Irreversible hydrocolloid
Modified hydrocolloid ie two-phase system
Polyvinylsiloxanes
Polyethers
Polysulphides
Plaster of Paris
Zinc-oxide eugenol
Consistency
Viscous Medium Light
*
*
*
* * * *
* * *
*
* *
*
*
Type of tray recommended
Metal or plastic stock
Customised resin
Customised resin
Stock or customised
Metal or plastic stock
Stock for putty, Customised for medium or light phases
Customised
Customised
Customised
Customised
Impression type- Primary (1˚) or Secondary (2˚)
1° (upper and lower)
2°; 'customises' customised tray
2° (lower)
1° or 2° (upper mainly)
1° (upper and lower)
1° if putty2° for medium- and light-bodied phases
2°
2°
2° (upper)
2° (lower mainly)
Table 2 A range of materials in common usage for impressions for complete dentures (reversible hydrocolloids are omitted because of problems of cross-infection)
Fig. 4 Two well-formed impressionsusing a twin-phasehydrocolloid material

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000 487
PRACTICEprosthetics
need for the clinician to determine what type ofimpression technique is appropriate for eachpatient as, clearly, the condition of the tissues ofthe denture-bearing areas and the peri-denturetissues must influence the impression techniqueselected. The recording of the definitive impres-sion is the keystone of the denture-prescribingprocess and the practitioner should select theappropriate technique carefully.
To avoid confusion, we shall describe a stan-dard ‘conventional’ impression technique forupper and lower definitive impressions. In theinterests of completeness, we shall also describea variety of other techniques which may begrouped into the following three groups:
• Selective pressure• Functional• Reline and rebase impressions (including
secondary template impressions).
Trays for definitive impressionsPrimary casts are generally poured in dentalstone and should, by virtue of the primaryfunction of primary impressions, be slightlyoverextended. Depending on the presence,amount and position of undercuts the clinicianshould outline how much spacing is requiredbetween the tray and the primary cast, eg 3 mmspacing is recommended for irreversible hydro-colloids where large undercuts are present.
While most clinicians leave the selection ofthe tray material to the laboratory, the clinicianshould advise the technician on the form of thetray. Mention has been made already of the rea-son for not perforating customised trays forcomplete dentures prior to establishing aperipheral seal. Similarly, in order that the formof upper and lower labial sulci are not overex-tended, there is merit in having stub handlesthat will not distort the lips (Fig. 6).
Conventional impression• After disinfection of the trays, and subse-
quent rinsing in water, check that each trayis adequately extended antero-posteriorlyand bucco-lingually. If the trays interferewith the function of the peri-denture softtissues, instability of the completed denturewill occur if overextension is not relieved.The extent of the overextension may bedetermined by pressure-relief paste.Underextension may be corrected byadding tracing compound or a similarmaterial (Fig. 7).
• Apply tracing compound to the posterioraspect of the upper tray to produce a poste-rior seal. The tracing compound shouldextend uninterrupted from one border ofthe tray to the other. This allows the creationof a post dam, facilitates location of the trayposteriorly and, finally, serves as a spacer forthe impression material. In the lower tray,the compound should be added to displace
the retro-molar pad sufficient to give a pos-terior seal.
• Add the tracing compound to increase thefunctional width of one buccal periphery(the impression material will record thefunctional depth). When completed, theother buccal periphery is recorded (Fig. 8). Ifrequired, the labial periphery may bemoulded, although this is usually not neces-sary as much less resorption tends to occurin the depth of the labial sulcus. The lowertray is similarly modified.
• At this stage, the fully customised traysshould exhibit good retention, a matter ofconfidence for both clinician and patient.Also at this stage, perforation of the uppertray may be done at the chairside, to enhanceretention of, eg irreversible hydrocolloidand/or to prevent the occurrence of air bubbles being present in the palatal vault.
Fig. 6 stub handleswill not distort thelower lip; anydistortion is likely toalter sulcular formof the definitiveimpression
Fig. 7 Addition oftracing compound toa lower trayconsidered to beunderextendeddistally andposteriorly
Fig. 5 Copy denturepoured prior tomodification of boththe impressionsurface and theocclusal surface

488 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000
PRACTICEprosthetics
• Add a small amount of soft tracing com-pound or suitable material to the special traysin the region of the upper and lower caninesand gently place into the mouth. These, as forthe posterior placement, will serve as a spacerand prevent the incorporation of supportproblems by avoiding undue and uneven dis-placement of the impression material (Fig. 8).
• Depending on the nature of the ridges andthe preference of the clinician, a variety ofmaterials may be selected (Table 2). It is ourcontention that the critical components ofthis technique are that a stable and retentiveperipheral seal will be established and thatappropriate spacing is incorporated; thechoice of material, within reason, is of sec-ondary importance.
• Following loading of the tray with the mate-rial, we recommend an impression tech-nique similar to that described for theprimary impression.
• When each impression has been removedfrom the mouth, and checked for accuracyand form, it should be subjected to anappropriate disinfection procedure, eghypochlorite, 1,000 ppm available chlorine.
• Before sending the definitive impressionsto be cast, the clinician should carefullyindicate the extent of the peripheral roll tobe preserved on the master cast (Fig. 9).Given the emphasis placed on creation ofthe peripheral seal, it would not be desir-able to lose this because of faulty mastercast preparation.
Selective pressure impression techniquesIn these techniques, three of which aredescribed, there is a need to modify the impres-sion procedures because of perceived supportproblems, eg displaceable upper anterior(flabby) ridge, fibrous (unemployed) posteriormandibular ridge or flat (atrophic) mandibularridge covered with atrophic mucosa. Whileother support problems may be overcome byappropriate relief of the master cast, these con-ditions are best overcome by modified impres-sion techniques. Several variations of theseimpression techniques occur and we haveattempted to standardise them.
We recommend that the adaptation of thecustomised trays should be as for a conven-tional technique and that only after the periph-eral moulding has been completed should themodifications to the trays/techniques occur.The three common clinical conditions requir-ing selective impression techniques are:
• Displaceable (flabby) anterior maxillary ridge• Fibrous (unemployed) posterior mandibu-
lar ridge• Flat (atrophic) mandibular ridge covered
with atrophic mucosa.
(i) Displaceable (flabby) anterior maxillary ridge(see Part 3 Fig. 2)After ensuring that the peripheral moulding orcustomising has resulted in a peripheral seal, animpression of the whole maxilla is taken usingeither zinc-oxide-eugenol (ZOE) or a medium-bodied polyvinyl siloxane (PVS) impressionmaterial. The former is not recommended in apatient with a dry mouth, as it tends to irritatethe mucosa.
On setting, the impression is removed fromthe mouth and the extent of the displaceable tis-sue is drawn on the impression surface. Thisarea, and the equivalent area of the tray, are thenremoved, using a scalpel and acrylic bur(Fig. 10a) — insertion of this modified impres-sion and tray will demonstrate that the tray is nolonger retentive.
Holding the modified tray and impression insitu, use a low-viscosity material (Plaster ofParis if ZOE was used, light-bodied PVS if amedium-bodied one was used) and paint orsyringe these onto the displaceable tissue torecord them in a minimally-displaced position.On setting, it should be apparent that a periph-eral seal has been re-established.
This completed impression (Fig. 10b) shouldthen be marked and disinfected as for a conven-tionally created impression before dispatch tothe laboratory.
(ii) Fibrous (unemployed) posterior mandibular ridgeThis condition may be recognised by the pres-ence of a thin, mobile thread-like ridge which isessentially fibrous in nature (Fig. 11).
Fig. 8 Tracingcompound added toeffect a peripheralseal. Note that somecompound has beenadded on the areasrelating to the ridgeof the canine areas to act as anteriorspacers
Fig. 9 Definitiveimpression with well-defined area for theplacement of cardingwax prior to boxingthe impression,thereby preservingthe functional widthand depth of the sulci

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000 489
PRACTICEprosthetics
The technique is shown in Figure 12a–c.• When the customised tray has been ade-
quately checked for peripheral extension, itis loaded with tracing compound (green-stick) and an impression of the denture-bearing area recorded.
• Using the heated spoon-end of a Le Croncarver or a similar instrument, remove thegreenstick relating to the crestal tissues andperforate the tray in this region. Downwardfinger pressure of the modified impression,in the mouth, should elicit no discomfort.
• Inject some light-bodied PVS onto the buc-cal and lingual shelves of the greenstick and
gently insert the impression. Excess materialwill be extruded through the perforations,and the fibrous ridge will assume a restingcentral position, having been subjected toeven buccal and lingual pressures.
The impression is now treated as for a conven-tionally made impression.
(iii) Flat (atrophic) mandibular ridge covered withatrophic mucosa (Fig. 13)These ridges equate to Atwood’s ridge orders vand vi and may be complicated by folds ofatrophic and/or non-keratinised tissue lying on
Fig. 11 View of fibrous posterior mandibular ridge. Thisridge as such is not useful for support
Fig. 12 a–c Staged sequence of techniques:a) Preliminary stage using tracing compound; b) Crestalarea cleared of tracing compound - tray perforated oncrestal area; c) Definitive impression using light-bodiedpolyvinyl siloxane
a
b c
Fig. 10 a) Displaceable area removed from special tray. In this case, a medium-bondedPVS impression was used. b) Completed impression. Here a light bodied PVSimpression material was syringed onto the displaceable tissue
a b

490 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000
PRACTICEprosthetics
the ridge. McCord and Tyson described thistechnique which is specific for this clinical situ-ation.6 The philosophy is that a viscous admixof impression compound and tracing com-pound removes any soft tissue folds andsmoothes them over the mandibular bone; thisreduces the potential for discomfort arisingfrom the ‘atrophic sandwich’, ie the creasedmucosa lying between the denture base and themandibular bone.
The impression medium here is an admix of3 parts by weight of (red) impression com-pound to 7 parts by weight of greenstick; theadmix is created by placing the constituentsinto hot water and kneading with vaselined,gloved fingers.
Using a standard impression technique, thelower impression is recorded. The workingtime of this admix is 1–2 minutes and thisenables the clinician to mould the peri-tray
tissues to give good peripheral moulding(Fig. 14).
On removal, this impression is chilled inwater and then re-inserted. The operatorpresses on the stub handles of the tray on thepremolar region and reciprocates with his orher thumbs on the inferior body of themandible; ideally, discomfort will be felt by thepatient in the area pressurised by the operator'sthumbs!
Any discomfort in the denture-bearing areamay be treated by adjusting the offending areaof the impression with a heated wax knife andre-inserting as required until no further dis-comfort is felt. Alternatively, the clinician couldindicate where relief is required on the mastercast. This technique gives the clinician a reliableguide to the load-bearing potential of thepatient’s denture bearing area when making thedefinitive impression.
Functional impressionsThese techniques may be used where problemsof stability exist, either because of poor muscleadaptation and/or imbalance or because ofproblems of available denture space. They mayalso be useful in patients who have recently suf-fered from a stroke.
Two variations are commonly used for func-tional impressions.
(i) Local areas of modificationOn occasion, dentures may exhibit looseness,not arising primarily from retention problemsbut because of localised areas of poor functionaladaptation. In these cases, the application of athin mix of a chairside resilient lining material(eg Visco-Gel, Dentsply Limited Surrey UK)may be used. The mixed material is added to thefitting surface of the denture and the patient isinstructed to wear the denture for one hour.After one hour of functional moulding the den-ture is then removed from the mouth (Fig. 15)and the conventional relining process com-pleted.
(ii) Problems associated with denture space/neutralzoneThis technique is well documented and hasbeen referred to as the neutral zone techniqueor anthropoidal pouch technique. We prefer touse the term denture form impression tech-nique. It is designed for patients with poortrack records of (lower) denture stability, a largetongue or other anatomical anomaly.
The clinical stages are standard up to andincluding the registration visit. After this, theupper denture is set up conventionally to theprescribed occlusal vertical dimension (OVD).Opposing the upper set-up is a resin base withthree vertical stops joined by a wire bent in asinusoidal manner (Fig. 16). The stops mustcontact the upper teeth at the selected OVD.
Fig. 13 View ofatrophic mandibularridge suitable foradmix impressionmaterial
Fig. 14 Definitiveimpression
Fig. 15 Functionalimpression using achairside resilientlining material

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000 491
PRACTICEprosthetics
Polyvinylsiloxane putty is added to the con-ventional fitting surface and also to the buccaland lingual aspects of the lower base which hasbeen coated with the requisite adhesive, andplaced in the patient's mouth. Following this,the upper try-in is inserted and the patientasked to close to the OVD, swallow and carryout closed mouth exercises. These exercises pro-vide an indication of where inward-directedforces from the buccinator muscles are equalledor ‘neutralised’ by outwardly-directed lingualforces ie the zone of minimal conflict (Fig. 17).
The disinfected functional impression andupper try-in are sent to the laboratory and plas-ter or laboratory-putty keys made of the func-tional impression (Fig. 18). Into these keys waxis poured to give a functional form to the pol-ished surfaces and occlusal form of the lowerdenture. The technician is then required to fab-ricate the lower try-in and, subsequently thelower denture, to match the functional tem-plate — this will necessitate appropriate cus-tomising of the occlusal table width andpossibly its length.
This procedure is clinically and laboratorytechnique-sensitive and competence in thistechnique must be shared by clinicians andtechnicians if a successful outcome is to beachieved.
Reline and rebase techniques (includingsecondary template impressions)Irrespective of whether a conventional relineimpression is being taken, or a secondaryimpression for the template technique, they areboth definitive impressions and must be
accorded the same degree of attention as stan-dard impression techniques.
The denture, or replica, to be relined shouldbe modified peripherally to ensure that theperipheral seal has been established.
Undercuts are removed from the impressionsurface of the denture, to ensure that the mastercast is not damaged on removal of the denture(Fig. 19).
Zinc oxide eugenol impression material wasgenerally used here although clinicians nowprefer to use polyether, polysulphide orpolyvinylsiloxane. Before recording the defini-tive impression, there is merit in placing tracingcompound as spacing on the denture in theregion corresponding to the ridges of thecanine areas (see conventional impression tech-niques). However, care must be taken to ensurethat no unplanned increase on OVD is inadver-tently incorporated.
In the case of the maxillary impression, there
Fig. 16 Suggestedform of lower 'rim'for denture formimpression technique
Fig. 17 Completedfunctional impression ofdenture form — recorded inPVS putty
Fig. 18 Plaster of Paris diesor stents of impression ofdenture form. These enablean exact wax form to bepoured
Helpful Hints1 Carefully survey the denture-bearing
area and select a stock tray ofappropriate extension. Determinewhich form of definitive impression isindicated, on the basis of the natureof the supporting tissues/patient’sfunctional requirements.
2 Practise the insertion of the tray toenable a) the patient to be aware ofwhat is required in impressionmaking and b) the clinician to beconfident of his technique.
3 Ensure the technician is aware of therequirements for each tray (egspacing, handles, lack ofperforations, etc).
4 Use the impression material thatworks best in your hands.
5 If the impression material is absentover the tissue surface of the tray, asupport problem will be introducedto the completed denture.
6 Ensure that areas that will requirerelief are marked on the definitiveimpression using an indelible pencil.

492 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 9, MAY 13 2000
PRACTICEprosthetics
is also merit in perforating the palate in the mid-line of the rugae to prevent any possibility ofimperfections in the impression, eg air bubbles.
Although this chapter has described impres-sion techniques for a variety of clinical condi-tions, it has also stressed the importance ofgood communications with the laboratory.Good rapport between the dentist and techni-cian will ensure quality of all stages in the pre-scription of dentures.
Conventional techniques, however, do littleto inform the technician on the customising ofupper record rims. In one system, theSwissedent system (vide infra), this is addressedand shall be discussed briefly in the next chap-ter because the principles involved are soundlybased.
Fig. 19 Photograph of a poor reline impression.In addition to the faulty form of the palate(caused by folding of excess material) theundercut tuberosity areas were not relieved —presumably the impression material wasattached to the patient’s tissues.
1 Basker R M, Davenport J, Tomlin HR. Prosthetic treatment of theedentulous patient. 3rd ed. pp88-93,London: Macmillan, 1992.
2 Guides to Standards in ProstheticDentistry —- Complete and PartialDentures. Guidelines in Prosthetic andImplant Dentistry. Ogden A. (ed) pp7-11, 1996; London: QuintessencePublishing Company Limited.
3 Davenport J, Heath J R. The copydenture technique. Br Dent J 1983;155: 162-163.
4 Duthie W, Yemm R. An alternativemethod for recording the occlusionof the edentulous patient duringconstruction of replacement dentures.J Oral Rehab 1985; 2: 161-171.
5 Murray I D, Wolland A W. Simpledenture copying using the Murray-Wolland duplicating box system.Dent Tech 1986; 39: 4-8.
6 McCord, J.F., Tyson, K.W. Aconservative prosthodontic optionfor the treatment of edentulouspatients with atrophic (flat)mandibular ridges. Br Dent J 1997;182: 469-472.

PRACTICEprosthetics
BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000 529
Registration: Stage I —Creatingand outlining the form of theupper dentureJ. F. McCord,1 and A. A. Grant,2
The clinical stage following the visit wheredefinitive impressions are recorded is that
clinical visit often referred to as ‘the bite’ orocclusal registration stage. While most practi-tioners and indeed most patients might per-ceive the raison d'être of this clinical episode tobe about intermaxillary registration solely, weconsider that the three component parts of thisclinical stage merit separate consideration. Thethree component parts are:
• Creating and outlining the form of the upperdenture
• Recording of intermaxillary relations• Selection of teeth.
This chapter will present a step-by-step accountof how the clinician may develop and customisethe upper rim to create a (replacement) pros-thesis which conforms to the facial contoursand dental/peri-denture constraints, while tak-ing cognisance of the patient’s age and dentureexpectations.
Succeeding chapters will address the record-
ing of intermaxillary relations and tooth selec-tion respectively.
In clinical practice, dentists receive upperwax rims that are duly moulded into the formof the upper denture at the chairside. The pre-cise form of the upper wax rim or blockdepends, essentially, on how the technicianswere taught. In essence, considerable variationprobably exists among technicians with regardsto the positioning of the labial face of the rim.The consequence of this is that it is often a mat-ter of chance that wax has to be removed oradded to the upper rim. In an attempt to saveclinical time, and at the same time render theupper rims more appropriate in form for eachpatient, two techniques have evolved: the bio-metric technique and the Swissedent tech-nique. Both will be described for interestedpractitioners and their technicians, as they bothhave the advantage, in theory, of saving chair-side time.
Watt and MacGregor outlined the principlesof ‘biometric’ guidelines to help compensate
Table 1 Average values of maxillary labial/buccal bone loss following tooth extraction. The values on the right hand column indicate by how much the labial/buccal faces of maxillary rim are built out from the LGM remnants
Tooth position Average horizontal bone loss
Incisor 6.5 mmCanine 8.5 mmPremolar 10.5 mmMolar 12.5 mm
5
Fig. 1 Photograph ofan edentulousmaxilla. The cord-likestructure wasreferred to as theremnant of thelingual gingivalmargins
In this section, weaddress how tocustomise the upperrim (aesthetic basecontrol) to create theform of thereplacement completeupper denture. Theuse of the facebow isalso described.
In this part, we willdiscuss:• Philosophies of restora-
tion of the ‘dental bulge’ • Technical aspects of rim
preparation • Clinical stages of
determining the form of the upper rim
• The facebow transferrecord.
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 188: 529–536

530 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000
for facial changes following tooth loss, predom-inantly in the maxilla.1 In essence, they advo-cated that the replacement upper teeth beplaced in mean pre-extraction positions; theseaverages were determined over a 30-monthperiod in a group of patients rendered edentu-lous. The ‘fixed’ points of reference taken formeasurements were the remnants of the lingualgingival margin (LGM) (Fig. 1). Average valuesfor maxillary teeth of replacement dentures areshown on Table 1.
The biometric principle The biometric principle has much merit in thatit helps to compensate for post-extraction boneloss by placement of the denture teeth in per-ceived pre-extraction positions. A furtheradvantage of placement of the maxillary (den-ture) teeth labial/buccal to the residual ridge isthat this promotes lower denture stability. Theplacement of the upper posterior teeth buccalto the maxillary ridge, in addition to compen-sating for the resorption pattern of the maxilla,also means that their palatal cusps may beplaced over the mandibular ridge crest. In prac-tice, the palatal cusps will therefore occlude intothe central fossae of the lower posterior teeth,thereby directing occlusal forces onto the resid-ual ridge. In addition, this placement of thelower teeth over the lower ridge tends to avoidconstriction of tongue space. Perhaps the prin-cipal deficiency of the biometric principle is
that it does not necessarily customise the den-ture form for each patient, nor does it cater forbiological ageing. A second problem with thisphilosophy is that anatomical features not dis-similar to the remnants of the lingual gingivalmargin have been observed in patients suffer-ing from anodontia.
Another technique which helps customisethe upper rim is described in the Swissedenttechnique.2 This technique, which was referredto in the previous chapter, relies on close andunambiguous communication between theclinician and the technician. It uses two distinctmeasurements for each patient in order that theupper rim (termed the aesthetic control base[ACB]) may be customised for each patient.These two measurements are related to thepatient’s facial form and are taken immediatelyafter the definitive impressions have beenrecorded and are dispatched along with theseimpressions to the laboratory.
The first measurement is taken via what iscalled the papillameter (Fig. 2). The proceduresto be followed for the papillameter reading areas follows:
• Place the papillameter inside the patient'supper lip and let it rest on the incisivepapilla.
• Add addition-cured polyvinyl siloxane(PVS) putty to the papillameter and mouldthe upper lip to restore the vermilion border.In younger patients, the philtrum may berestored but this may not be possible in olderpatients (Fig. 3a).
• Determine how much of the upper incisorwill be shown under the upper resting liplength (vide infra).
• Level the PVS at the incisal level and recordthe reading from the graduated scale on thepapillameter (Fig. 3b).
• The customised papillameter is sent to thelaboratory and this enables the technician tohave sufficient information to prepare anupper rim that provides upper lip support.Patient information, eg from photographsor via dentures favoured by the patient may
PRACTICEprosthetics
Fig. 2 The papillameter is asimple gauge with a step onits inner aspect; this step restson the incisive papilla and thegraduated column restsbetween the labial aspect ofthe ridge and the lip. Thegraduation commences at thelevel of the incisive papilla andthe clinician determines wherethe incisal tips of the maxillaryincisors will lie in relation tothe resting lip level andrecords the readingappropriately from thegraduated scale.
Fig. 3 a) Papillameter in situ with PVS putty used to restore the form of the upper lip; b) The incisal point is indicated on the papillameter ‘Plimsoll-line’.
a b

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000 531
also be used to help determine the upper lipform which is well perceived by the patient.Equally, the Alma Gauge3 (Fig. 4) may beused to produce an upper rim (ACB) withequivalent dimensions, labially, to previousor current dentures that are considered ade-quate. In essence, the Alma Gauge comprisesa graduated table and a spring-loadedpointer that is also graduated. The denturebeing ‘templated’ is placed on the graduatedtable and the pointer placed in the impres-sion surface of the denture in the middle ofthe area occupied by the incisive papilla. Thedistance from the pointer to the incisal tip ofthe central incisors may be read off the (horizontal) graduated scale on the table.The vertical distance from the pointer tip tothe incisal tips is then read off the graduatedscale, giving a three-dimensional readingfrom the incisive papilla to the incisal tips ofthe central incisors.
The second measurement concerns the anteriorwidth of the upper rim and for this a calliper-like device called an alameter is used. Thealameter’s usage is based on a reasonable clini-cal guideline, namely that the width (ie hori-zontal distance) between the alar cartilages in asmiling patient is broadly speaking comparableto that of the canine tips (Fig. 5). This readingenables the technician to evaluate the width ofthe upper rim, assuming that there is symmetryabout the palatal midline.
Preparation of the upper rim Upper rims comprise bases and rims. Thebases may be made of wax, thermoplastic
resin or of (poly) methylmethracylate(PMMA) while the rims are generally madeof wax. Table 2 lists some of the materials,which may be used as bases for recordingrims, with indications of effectiveness. Ingeneral, bases for occlusal rims/aestheticcontrol should be:
• Well adapted and conform closely to themaster cast
• Stable, on the cast and in situ• Free of voids or surface projections on the
impression surface• No more than 1 mm thick over the residual
ridge to prevent the base interfering with theplacement of the denture teeth
• 2 mm thick in the post dam area of the max-illary denture (and 2 mm thick in the lingualflange of the mandibular denture) to impartrigidity
• Easily removed from the cast• Smooth and rounded so as to reproduce the
contours of the master cast• Constructed in materials that are dimen-
sionally stable at oral temperature.
As wax bases do not provide stability per se,their usage is not encouraged. Thermoplasticresins tend to be brittle and, as they lack theversatility of PMMA, they no longer enjoywidespread usage in clinical or laboratorypractice.
Depending on the preference of the clinicianand/or the technician, bases may be made ofauto-polymerised PMMA, light-cured PMMAor processed PMMA; all provide adequatepotential stability although they vary in their
PRACTICEprosthetics
Table 2 Common materials used as bases for record rims
Classification of base Material Advantages Disadvantages'Temporary' a. Thermoplastic resin Cheap,easy to adapt to cast, Brittle, may fracture in bases easy to adapt to post dam on clinical use.
master cast b. Auto-polymerised Cheap, technicians familiar Acceptable material but PMMA with usage handling problems possible c. Light-cured PMMA Easy to make tray, Problems of adherence of
quick technique wax to base, polishingmore difficult than b (above).
d. Vacuum-formed (PVA) Fast, quite cheap, not messy Requires thermal vacuum machine e. Baseplate wax Cheap, easy to adapt Easily distorted
'Permanent' a. Processed resin Rigid, accurate and stable Destroys master cast, bases bases — become part of good clinical and technical
final denture techniques required b. Cast alloys Bases are rigid, stable and Cost more than other types,
eg gold, should have accurate fit especially gold alloys. cobalt-chromium Sound impression techniques
required, especially in post damarea. NB a conventional wax try-in should be performed first to establish the plannedpositions of the denture teeth.
Fig. 4 The Alma Gauge whichmay be used to record thehorizontal and verticalrelationships of the incisivepapilla landmark on thedenture to the incisal points
Fig. 5 Facial view of dentatesubject indicating therelationship between thecanine tips and the alarcartilages

532 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000
levels of tissue-fit. In theoretical terms, how-ever, the processed bases tend to be superior.4
Technical aspects of rim preparationUnless the clinician has cast the definitiveimpression and has scored the master cast todefine the post dam (Fig. 6a), the rim will notexhibit a clinically-meaningful peripheral seal.This may be achieved by the technician reliev-ing the master cast in 1 mm wax, but stoppingthis relief 2 mm short of the vibrating line,thereby incorporating a form of post daminherent in the denture base. The clinicianmust be aware however that this would not
conform to the anatomy of the tissues compris-ing the patient’s post dam (Fig. 6b). It would,however, provide an acceptable peripheral sealas long as the functional width and depth of thesulci were faithfully restored in wax.
Using the papillameter and alameter read-ings, the anterior aspect of the rim may be cus-tomised, in wax, to permit early visualisation ofthe aesthetic form of the upper denture. Thealameter reading further helps the techniciancustomise the rim by establishing the (horizon-tal) inter-canine distance customised for eachpatient.
The posterior aspect of the rim is also madeof wax and resembles conventional record rims(Fig. 7).
Clinical stages in determining the form of theupper rimThere are eight clinical stages, these aredescribed below:
• Before immersing the rim in disinfectantmaterial, in keeping with conventionalinfection control procedures, and prior toinserting the rim into the mouth, the clini-cian should ensure that the rim is welladapted to the master cast. Alternating fin-ger pressure on each side of the rim should
PRACTICEprosthetics
a b
Fig. 6 a) The master cast has been modified by theclinician to create a post dam. Note the extension into thebuccal sulci; b) Light-cured base with ‘post dam’incorporated by stopping the wax spacer short of theposterior limit of the base.
Fig. 7 Occlusal viewof upper rim(aesthetic controlbase)
Fig. 8 The form of the lip at the height of the labial sulcushas been distorted. This will affect the position of theresting lip length by raising the lip inappropriately
Fig. 9 Appropriate lip support has restored the vermilionborder; the philtrum, however, has not been restored

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000 533
not elicit a rocking of the rim on thecast.
• When the rim has been inserted into themouth and the clinician has ensured stabilityof the rim, the first clinical step is to ensurethat the infra-nasal tissues are harmoniouswith the soft tissues of the middle third ofthe face. Failure to do this may affect theform and length of the upper lip (Fig. 8), byraising the lip inappropriately.
• Confirm that the upper lip is adequatelysupported. This should result in restorationof the vermilion border and may result inrestoration of the philtrum although, as hasbeen mentioned, this may not always bedesirable or possible (Fig. 9). Some clinicalguidelines recommend that the verticalnaso-labial angle should be 90°, althoughrecent research casts doubt on the validity ofthis guideline.5
• When the upper lip has been restored appro-priately for the patient, it is then practical forthe clinician to determine the position of theincisal point relative to the resting lip. Whilesome textbooks recommend that the incisallevel of the upper rim is 2 mm inferior to theresting upper lip, the clinician should tem-per this by deciding what is appropriate foreach patient. Younger patients may reason-ably be expected to show 4–5 mm of toothbeneath the resting lip, especially if thepatient had a Class 2 division 1 profile. Incontrast, a 70-year-old patient might be bestsuited by having the incisal point level withthe resting lip, or possibly 1 mm above this(Fig. 10). Antero-posterior verification ofthe placement of the incisal point may beachieved by asking the patient to say a wordcontaining a fricative consonant (labioden-tal sound) eg ‘fish’; in general terms, theincisal point should correspond to the ver-milion border of the lower lip.6
• The next step in this clinical exercise is todetermine the upper anterior plane. Giventhe position of the incisal point, the plane ofthe upper six anterior teeth is usefully deter-mined by making it parallel to the inter-pupillary line. This may be done using aFox’s occlusal plane guide (Fig. 11) or anydevice giving a horizontal plane eg a woodenspatula.
When this has been performed, there is merit indetermining the position of the mid points of theupper canine teeth. One useful way to recordthis is to use a photograph of the patient whenthe patient was dentate. A clear, face-on photo-graph is required for this and, regrettably, theseare not always available. Using the pupils as sta-ble reference points, the clinician may determinethe relative position of the upper canine teethusing the ratio shown in Table 3.
This simple mathematical model, using dif-ferent terms, is often used in endodontics to
determine the working length of a root canal. A second useful technique is to extend dental
floss from the inner canthus of the eye, via thelateral border of the alar cartilage (with thepatient smiling) onto the incisal edge of theupper rim (Fig. 12).
Using the canine points on the upper rim asreference points, the right and left posteriorplanes are formed. The accepted guideline isthat this plane is parallel to the line drawn fromthe inferior border of the alar cartilage to a
PRACTICEprosthetics
Fig. 11 A reasonableguideline for theupper incisal plane is parallel to the inter-pupillary line
Fig 12 The use ofdental floss todetermine theposition, on the ACB,of the mid-point ofthe canines
Fig 10 This slide of asmiling dentateseptuagenarianillustrates the fact thatthe upper centralincisors would belevel with, or justabove, the upperresting lip
Table 3 Ratio to help determine inter-canine width
Actual interpupillary distance Photographic interpupillary distance
Actual intercanine tip distance Photographic intercanine distance=

534 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000
position two-thirds of the way up the tragus(Fig. 13).
Again using the mark on the rim correspond-ing to the canine tips as a reference point, thebuccal form of the upper rim may be mouldedby reducing the inferior borders of the poste-rior rims by 3° to 5°. This procedure createswhat are known as the buccal corridors and cre-ates a more natural smile (Fig. 14).
Before completing the customising of theupper rim, the following should be scribedclearly on the anterior aspect of the rim (Fig. 15):
• Centre line• High smile line• Canine points.
The significance of these points will be madeclear in Part 7.
With the upper rim in situ, ask the patient tosmile; the upper rim should appear to be paral-lel to the lower lip line when smiling (Fig. 16).
The posterior border of the upper dentureshould displace the mucosa overlying theaponeurosis of tensor palatii at the junctionbetween the hard and soft palates. As the detailsof the displaceability of the tissues of the postdam are known only to the clinician, it is thesole responsibility of the clinician to scribe the
appropriate extent and depth of the post damusing eg a Le Cron carver or similar instrument(see Fig. 6a); if not done so prior to this stage,the clinician should ensure that he/she scribesthe post dam appropriately.
Depending on the occlusal and stabilityrequirements of the patient, the clinician mayconsider it necessary to use a facebow to trans-fer the relationship of the upper rim to an arbi-trary hinge axis. Although it must be concededthat it may not always always be strictly neces-sary to use a facebow in all complete upper den-ture cases, we are now of the opinion that wecannot think of a valid reason not to use a face-bow in the prescription of complete dentures.We firmly believe, however, that cliniciansshould consider the use of a facebow especiallywhen a complete upper denture is opposed by anatural dentition or an implant-supportedoverdenture.
As the authors use a Gothic-arch tracingdevice (Fig. 12, Part 6) to record intermaxillaryrelations, we use a facebow transfer at this stage.For those practitioners who use upper andlower rims, the facebow transfer should takeplace after the lower rim has been adjusted tovertical, antero-posterior and coronal require-ments.
PRACTICEprosthetics
Fig. 16 The occlusal surfaces of the ACB should be parallelto the smile line
Fig. 15 Upper rim/ACB indicating dental landmarks
Fig. 14 Creation of buccal corridors on the upper ACB —the incorporation of these will create a more natural andmore aesthetic smile. In this slide, the buccal corridor onthe patient’s right has been incorporated
Fig. 13 Fox’s plane used to help assess the orientation ofthe posterior occlusal plane. Note that, in this case, theplane dips posteriorly — this would result in occlusalproblems

Fig. 19 Facebowfork in situ in ACB
BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000 535
The facebow transfer recordThe facebow transfer, in this context, is used totransfer the relationship of the maxillary planeto the intercondylar axis on the patient. Onceestablished, this relationship is transferred tothe articulator in order that the casts of theedentulous maxilla assume the same relation-ship to the articulator’s intercondylar axis. Forcomplete denture work, a hinge axis facebow isnot required and a simple facebow using anarbitrary axis will suffice.
In essence, a facebow is a calliper-like instru-ment used to record the spatial relationship ofthe maxillary arch to the temporomandibularjoints and then transfer this relationship to anarticulator; it orientates the (maxillary) dentalcast in the same relationship to the opening axisof the articulator. Customarily the anatomicreferences are the mandibular condyles’ trans-verse axis and one other selected anteriorpoint.7
In essence, a facebow consists of three com-ponents, a facebow fork, an anterior locatorand a U-bow used to locate the condyles (thetwo posterior determinants).
As was mentioned earlier, the principal pur-pose of the facebow is to record the relationshipof the patient’s maxillary plane to the patient'stransverse condylar axis and then transfer thatrelationship to the articulator. To transfer thatplane, therefore, three points must be trans-ferred. In practice, two are located posteriorly,to record the arbitrary transverse axis, and oneanterior landmark (Fig. 17a and b).
We recommend the use of a facebow transferrecord simply because this ensures that theplane of the upper complete denture will bebetter aligned to the condyles and thus to themandibular arch during mandibular move-ments. This is particularly important whencomplete upper dentures are opposed by a nat-ural dentition (or a natural dentition plus alower partial denture) as displacing forces onthe upper denture may be profound. Withoutthe facebow transfer, technicians tend to set upthe upper rim parallel to the worktop; most
patients do not walk around with their maxil-lary planes parallel to worktops. Clearly if thepatient only exhibits vertical chewing move-ments, facebow transfers are not strictly neces-sary and because of this not all dental schools inthe past taught their usage, although this prac-tice would appear to be changing.
There is a range of facebows available, and theauthors are not aware of any evidence statingthat one is better than another; we believe thatpractitioners should be encouraged to use thesystem with which they are familiar and whichis compatible with the articulator used by thelaboratory/clinician.
The system demonstrated here is the Denarsystem and the reader will note that the
PRACTICEprosthetics
Fig 17 Two of the three points used to transfer themaxillary plane. a) E, External Acoustic Meatus; b) N, Nasion
a b
Fig. 18 Denarfacebow plus forks

536 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 10, MAY 27 2000
posterior points are ear pieces and the anteriorpoint is located 46 mm superior to the anteriorrim of the ACB.8 This measurement is arbitraryand is, conveniently, the mid point between theupper and lower arms of the articulator, hencethere should be space in the articulator toaccommodate both casts.
In all types of transfer bow, for edentulouspatients, the bite fork of choice is an edentulousfacebow that should not therefore alter theform of the occlusal and incisal edges of theACB (Fig. 18). This means that for practitionersusing the conventional upper and lower waxrim technique, this means that the edentulousfacebow may be used.
This step completed, the clinician may nowprogress to recording the appropriate inter-maxillary relations.
PRACTICEprosthetics
1 Watt D M, MacGregor A R. DesigningComplete Dentures 2nd Ed. pp 2-31,Bristol: Wright, 1986.
2 McCord J F, Gill M, Lee C, RichmondR. Creating Better Dentures. J Inst BrSurg Tech In Print.
3 Grant A A, Heath J R, McCord J F.Complete Prosthodontics: ProblemsDiagnosis and Management pp52-53.London: Mosby Wolfe, 1994.
4 Morris H F. Recording Bases andOcclusal Rims in Essentials ofComplete Denture Prosthodontics 2ndEd. Winkler (ed) pp 123-136, StLouis: Mosby, 1988.
5 Brunton P A, McCord J F. An analysisof nasolabial angles and theirrelevance to tooth position in theedentulous patient. Eur J ProsthodontRest Dent 1993; 2: 53-56.
6 McCord J F, Firestone H, Grant A A.Phonetic determinants of toothplacement in complete dentures.Quint Int, 1994; 25: 341-345.
7 The Academy of Prosthodontics.Glossary of Prosthodontic Terms. JProsthet Dent, 1994; 71: 72.
8 Denar Slidematic Facebow Instructionmanual Teledyne Water Pik FortCollins Colorado USA.
Helpful Hints1. Ensure rims are stable a) on master
cast b) in situ2. Ensure the master cast is scored
appropriately in the post dam regionand that areas requiring relief areidentified on the master cast (clinician’sresponsibility) or that relief has beenplaced (usually technician’s task).
3. Ensure upper labial lip form isappropriate -— this will influence thelocation of the incisal point.
4. Check that the occlusal edges are inaccordance with prosthodonticguidelines.
5. Consider the use of a facebow —technicians normally tend to set upcomplete maxillary dentures with theocclusal plane parallel to theworkbench; not all patient’s occlusalplanes are parallel to the horizontal!

PRACTICEprosthetics
BRITISH DENTAL JOURNAL, VOLUME 188, NO. 11, JUNE 10 2000 601
Registration: Stage II —intermaxillary relationsJ. F. McCord,1 and A. A. Grant,2
Recording the jaw relations is a veryimportant procedure in the production
of complete dentures. An error at this stagecan result in dentures that are uncomfort-able, or unwearable, and may even have thepotential to produce lasting damage to manyelements of the stomatognathic system.
The intermaxillary relations are, of course,three-dimensional. In order to simplify therecording of jaw relations it is established prac-tice, based on extensive clinical practice andcurrent physiological knowledge, to considerthree elements. The first of these is in the verti-cal plane to establish the amount of jaw separa-tion, while the second and third relate to thehorizontal plane (which is concerned with theanteroposterior relations) and the coronalplane when one considers the lateral relationsof the jaw.
The vertical relationshipIndividuals who have their natural dentitiondemonstrate a space between the occlusal sur-faces of the teeth of the opposing jaws whenthey are at rest and with the head upright. Thisspace, the freeway space (FWS) or interocclusaldistance, is determined by a balance betweenthe elevator and depressor muscles attached tothe mandible, and the ‘elastic’ nature of the sur-rounding soft tissue in a natural dentition. It isusually measured indirectly by noting the dif-ference between the resting vertical dimension(RVD) of the face using, for example, a Willisgauge, and subtracting from this the verticaldimension of occlusion (OVD) with the teethin occlusion (Fig. 1).
A similar set of circumstances is consideredto exist in the edentulous patient — although
the RVD may differ from that which pertainedwhen natural teeth were present. It is nowknown that the RVD is not a stable positionthroughout life for a given individual.
However, the RVD may be considered as a factor when determining as to whether a patientwill be able to tolerate wearing dentures withoutintra-oral tissue damage occurring. RVD shouldalso be taken into account as an importantaspect of the appearance of the denture-wear-ing patient. For these reasons it is the startingpoint from which the OVD is estimated.1
Because of the role played by the ‘elastic’properties of the soft tissue environment of themouth, the importance of developing the formof the upper denture as described in Part 5 isemphasised. This must be done prior to deter-mining the RVD for the edentulous patient.The weight of the soft tissues attached to themandible plays a very important role in theRVD as does the position of the head. Tiltingthe head backwards pulls the mandible awayfrom the maxilla, and a forward inclinationpushes the mandible and attached structurescloser to the maxilla.
Resting vertical dimension (RVD) measurement Many methods have been advocated for themeasurement of the RVD. These include vari-ous facial measurements, swallowing methods,biting force measurements, phonetic methods,tactile methods and electromyographic mea-surements.
We recommend a combination of some ofthe above for a simplified clinical determina-tion of RVD.
Two measuring points are required in themidline of the face — one related to the nose,
6
Fig. 1 The differencebetween RVD andOVD
In this section, variousmethods of recordingof intermaxillaryrelations arediscussed, as is thedetermination ofappropriate occlusalvertical dimension.Consideration is alsogiven to choice ofarticulator.
In this part, we willdiscuss:• How to determine FWS • How to relate the
mandible to the maxillaat an appropriate OVDin RCP
• How to record other intermaxillary relations
• A range of articulators
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 188: 601–606

602 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 11, JUNE 10 2000
and one to the chin. These points must be onsites of minimal influence from the muscles offacial expression to avoid skin movement, andshould be chosen only after careful observationof the patient seated normally in the dentalchair with the head erect. The measurement ismade with the patient in a relaxed and comfort-able position, while wearing the previouslydeveloped upper base and rim. A Willis bitegauge may be used for the measurement, as itincorporates a suitable scale (Fig. 2) or a pair ofdividers and an additional scale can be used.
It may be helpful if the patient moistens thelips with his or her tongue and brings them intolight contact prior to recording the measure-ment. Asking the patient to swallow and relaxthe jaws is also a useful method. Verification ofthe measured value can be attempted by askingthe patient to say the letter ‘m’ and to hold thefacial expression whilst the measurement ismade. The general appearance of the patient'sface and its proportions should also be takeninto account. Careful observation to guardagainst unwanted skin movement should bemaintained during the recording of measure-ments.
In conventional techniques, once the RVDhas been established, the upper and lower basesand rims are placed in the mouth after theupper rim has been moulded (see Part 5). Thelower rim is reduced in height (usually — oradded to if undersized), until it contacts evenlythe upper rim at a vertical dimension of occlu-sion some 2–4 mm less than the establishedRVD. This provides for a freeway space of2–4 mm, and establishes the OVD.
In establishing the height of the lower rim,the relative height of both the upper andlower rims should be considered. As a practi-cal consideration, an element of reasonablebalance between the two rims is desirable.Excessive height of the lower rim can have theeffect of ‘walling in’ the tongue causing aresultant unstable lower denture. On theother hand, deficient depth of the lower rimcan result in poor aesthetics and, further, mayresult in tongue biting. Conventional wis-dom, however, would indicate that the
occlusal plane should be below the dorsum ofthe tongue at rest.
Errors in OVDProvision of an appropriate OVD is importantbecause of the consequences which can stemfrom an over- or under- estimation of thisvalue.
Excessive OVD may result in increased risk oftrauma to the tissues underlying the dentures asthe absence of a freeway space effectively causescontinuous clenching of the teeth. Painfulmucosa over the denture bearing areas andmuscle soreness, particularly associated withthe masseter muscle, may become evident. Theteeth are liable to contact (causing clicking)during speech and other speech problemscaused by difficulty in bringing the lips together(eg ‘p’, ‘b’ and ‘m’ sounds) may occur. Poor aes-thetics may be apparent and there is a possibil-ity of temporomandibular joint dysfunctiondeveloping (Fig. 3).
Where there is an under-estimation of OVD,lack of support of the angles of the mouth(causing dribbling and possibly angular cheili-tis) may be apparent. Masticatory efficiencymay be reduced and poor aesthetics, because ofa lack of adequate support of the lips and cheeksmay be seen. Chin protrusion on closure of thejaws may also occur (Fig. 4).
Care at this stage is required, and, further-more, it must not be assumed that the valueselected is immutable, as the generally quotedvalue for the freeway space (FWS) is an averageone and, as such, it should be appreciated thatsome patients may require a larger, or smaller,value. For example, where atrophic mucosaexists in a middle-aged adult an increased FWSmight prevent/reduce trauma to the residualmandibular tissues (Fig. 5).2
There are several accepted tests which can beapplied to verify the established OVD. How-ever, occlusal rims are so different from theform of teeth to be used that it is very difficult toapply tests for suitability of the chosen value atthis stage. Further checks on the establishedOVD will need to be made at a later stage ofdenture production — the trial stage — andwill be dealt with in Part 8.
Registering the intermaxillary relationsThe generally agreed position for recordingthe antero-posterior position of the mandiblerelative to the maxilla is that of the retrudedcontact position (RCP). The reasons for thisare first that it is a reproducible position inthe edentulous patient. Secondly, abnormalcontact between opposing dentures when setup in other than the retruded relationshipresults in denture instability. Next, the appa-ratus used for reproducing relevant jaw move-ments (the articulator) operates from theretruded position, and abnormal temporo-
PRACTICEprosthetics
Fig. 3 Excessive OVD results in the orbicularis oris musclegroup straining to effect a seal
Fig. 2 Willis bitegauge, and a similarinstrument, both withan integrated scale,may be used tomeasure RVD andOVD
Fig. 4 Insufficient OVD mayresult in an ageing effect of thepatients

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 11, JUNE 10 2000 603
mandibular joint activity may result frompatients attempting to accommodate incor-rect occlusal relations.3
Following adjustment of the occlusal rims tothe selected OVD, the rims should be insertedinto the mouth and the patient persuaded toclose gently with the mandible in the retrudedjaw relationship. The word ‘bite’ should not beused, as this suggests to the patient that forcefulclosure is required and will result in a mandibu-lar position that is protrusive .
A number of methods have been suggestedto assist the patient to achieve retrusion of themandible. Some patients have the capacity torelax the muscles attached to the mandible sothat the operator can readily move themandible up and down as it rotates about thecondyles. In those circumstances, themandible is in the retruded position, and canbe guided there during the registration proce-dure. Other patients are able to retrude themandible when the tongue is curled back inthe roof of the mouth to feel the posterior border of the upper base, or a shallow ridge ofwax placed on the palatal area of the base posterior to the first molar region.
In our opinion, the most positive and suc-cessful method is by means of the Gothic-arch(or arrowhead) tracing method, as it readilyidentifies the most retruded position of themandible relative to the maxilla from which lat-eral excursions can be made.
Methods of registrationRecording the retruded contact position (RCP)requires upper and lower rims to be fixed inposition with the mandible in its most retrudedposition and with the jaws separated by theestablished OVD.
A variety of methods for securing a record ofthe retruded jaw relations (RJR) have been usedwith varying degrees of success.
These include:
• Wax squash bite (and its predecessor, the T-block system) (Table 1)
• Wax rims or ‘Manchester’ blocks (Table 1)• Intra-oral tracing (Gothic-arch tracing)
(Table 1)• Extra-oral tracing.
Wax squash biteThe wax squash bite involves placing a horse-shoe shaped roll of softened wax between theupper and lower rims and having the patientclose the jaws together. The lower rim is firstreduced in height to provide space for the wax.Results using this method are uncertainbecause of the lack of control of the verticaldimension, the common difficulty of obtainingmandibular retrusion, and the fact that therecord takes no account of mandibular move-ments other than the final act of closure (Fig.6). In addition, if the wax wafer is not uni-
formly softened throughout its length, anunstable relationship with the underlying tis-sues is recorded. An earlier version of thismethod was the T-block method, in which a T-shaped wax form was used instead of the sim-pler horseshoe form (Fig. 7). The ‘horizontal’portion was placed between the rims while the‘vertical’ part that protruded anteriorly wasintended to be moulded to provide a form ofcontouring of the labial aspects of the rims.This method fell into disuse because of the arbi-trary nature of the moulding procedure thatalso induced the patient to assume non-RCPposturing of the jaw, as well as having the samedefects as those mentioned above.
PRACTICEprosthetics
Table 1 Summary of relative efficiency of registration techniques for complete dentures
Method Comments
Squash bite Poor control over OVD, no control of mandibular movements, or of stability of bases, uncertainty of RCP.
Wax rims including Good control of OVD, good base stability if PMMA used. Manchester bases Uncertainty of RCP, good occlusion development with
facebow mounting.Intra-oral tracing Good control of OVD, good base stability, good control of
RCP and other mandibular activity. Excellent occlusion and articulation development with facebow mounting.
NB If, after any of the three techniques have been used, the casts are approximated and examined and the heels are found to contact, then this gypsum contact should be removed prior to articulation otherwise a posterior bite will be incorporated into the set-up and will be evident at the trial insertion.
Fig. 6 Typicalexample of squashbite — insufficientdefinitions ofdenture geometryand form areprescribed
Fig. 5 Atrophicmucosa: an efficientmasticatoryapparatus with anoptimal FWS mightresult in trauma tothe mandibular ridge—- intentionalincrease in FWSmight reduce traumato the denture-bearing tissues of themandibular denture

604 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 11, JUNE 10 2000
Wax rimsThe conventional method that has a higherdegree of success also involves the use of waxinterposed between the rims to secure a regis-tration. When the upper rim (aesthetic controlbase [ACB]) has been formed, and prescribedto suit the patient, the lower rim is placed in themouth and trimmed until it contacts the upperrim evenly in RCP, at the selected OVD (Fig. 8).This is done by selectively removing points offirst contact. These large wax rims may poseproblems in inexperienced hands. Even inexperienced hands it is not always easy to detectpremature contacts along the lengths of therims bilaterally.
For these reasons, a simplified lower rim hasbeen developed in the University Dental Hospi-tal of Manchester. It contains several elements
incorporated to ensure that the carefully estab-lished OVD is maintained, and that the basesare maintained in stable relationship to theunderlying tissues during the procedure. Thelower base has attached to it two pillars of waxwhich are situated in the region of the 2nd pre-molar/1st molar teeth positions (Fig. 9a and b).When the contacts, bilaterally, are even at theselected OVD, the rims may be sealed with reg-istration paste or other such medium as regu-larly used.
This method using pillars attached to thelower base — which we call the Manchesterblock method — provides control over theOVD, ensures a stable relationship between thebases and the underlying tissues, and also pro-vides a record that can be simply returned tothe mouth to verify its accuracy. To obtain afunctional impression of the labial componentof the lower arch, carding wax, Plaster of Parisor PVS putty may be attached to the labialaspect of the rim and a closed-mouth impres-sion used to determine the anterior denture-spaced form.
However, the drawbacks of this procedurecomprise uncertainty of achieving the mostretruded mandibular position, as well as a lackof information on eccentric mandibular move-ments.
Intra-oral tracingOur preferred method of obtaining a consistentposition of retrusion together with recognitionof mandibular movement other than the finalpoint of closure, is by means of an intra-oraltracing — often referred to as a Gothic-archtracing. This method is based on rotation aboutthe condyles when lateral mandibular excur-sions are made. When the mandible moves tothe left from a central position, it rotates aboutthe left condyle, and similarly, a right lateralmovement causes rotation about the rightcondyle. Between each lateral excursion, thecondyles assume their most retruded position(Fig. 10).
This technique uses two pieces of apparatus,
PRACTICEprosthetics
Fig. 7 T-blockprecursor to thesquash bite andpopular at the onsetof the NHS
Fig. 8 Conventionalupper and lower rims
Fig. 9 a) ‘Manchester’ rims — to simplify complete denture registration technique; b) Addition of carding wax tothe labial segment of the lower rim can help create a functional modelling of the denture space anteriorly
a b

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 11, JUNE 10 2000 605
one for each arch, both mounted on rigid sta-ble bases, usually made of light-cured poly-methylmethracylate (PMMA). The upperapparatus comprises a metallic plate that spansthe maxillary arch. The lower has a bar con-taining an adjustable central-bearing screw(1mm thread) mounted on wax or compound‘pivots’ added to a light-cured PMMA base(Fig. 11). The lower plate lies over the most sta-ble pivotal areas of the arch. The adjustablecentral-bearing screw is made to contact theupper plate at right angles and at the selectedOVD. The bases are adjusted so that no contactbetween them can occur and the patient canmake lateral mandibular excursions with con-tact of the central-bearing pin on the upperplate only. The patient is requested to swallow,to indicate a ‘central’ (RCP) position, thenasked to make three protrusive movementsbefore returning to RCP. From RCP the patientis asked to make three left lateral excursionsand then to return to RCP. Finally, the patientis asked to perform three right lateral excur-sions before returning to RCP. The patientshould then be familiar with the two pieces ofapparatus and the practitioner can then pro-ceed to record the tracing. This is done by coat-ing the upper plate with, eg ink from a felttipped pen and then asking the patient to repli-cate the protrusive and lateral movements. Thealternate lateral jaw movements scribe on theupper plate two arcs of rotation which intersectin a position corresponding to RCP. Clearly, itis from this point that an intersection (arrow-head) with the protrusive movement is alsotraced (Fig. 12a). To validate this position aperforated perspex cover slip is positionedwith the perforation over the arrowhead andwaxed in place. The patient is then asked toswallow and confirmation of RCP is achievedby the central bearing screw engaging the per-foration (Fig. 12b).
This fixed registration records the verticaland antero-posterior intermaxillary relations.To record the coronal relationship, Plaster ofParis or PVS putty is then placed between the
bases and the central-bearing screws to ensurean unambiguous relationship (Fig. 12c).
Extra-oral tracingThe extra-oral tracing is somewhat similar tothat of the intra-oral, except that the tracingapparatus is attached to plates that protrudebetween the lips. It is not considered to be asaccurate as that of the intra-oral method foredentulous patients because the protrusion ofthe recording apparatus is so far forward of thepivotal area that tilting and/or deflection of thebases is likely.4 In addition, as this technique isnot universally taught worldwide, it will not bedescribed further.
Further considerationsWhen these three-dimensional intermaxillaryregistrations have been completed, they will besent to the laboratory along with the ACB andfacebow transfer to be articulated. While teethhave still to be selected (see Part 7) it is appro-priate to consider briefly, the types of articula-tor on which the casts are to be mounted, as theproper adjustment of these may require addi-tional records.
Articulators for complete denturesThe usage of articulators to enhance clinicalpractice has been the subject of a recent review5
and thus we shall confine our discussion to sim-ple basic points.
PRACTICEprosthetics
Fig. 11 Apparatus for measuring Gothic arch tracing. a) Upper base plate; b) Lower base, barand central-bearing screw
Fig. 10 Line drawing of occlusalview of mandibleand arcs ofmovement about the condyles
ba

606 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 11, JUNE 10 2000
Articulators in common use for the produc-tion of complete dentures comprise (Fig. 13):
• Simple hinge (plane line)• Moveable, fixed condylar path• Semi-adjustable.
The simple hinge articulator allows the con-struction only of a centric occlusion, whereasthe fixed condylar path instrument allows someapproximate lateral and protrusive occlusion tobe developed. The semi-adjustable articulatorallows the establishment of more accurate orcustomised lateral and protrusive as well as cen-tric occlusion.
Few simple hinge articulators have provisionfor accepting a facebow record so that this fur-ther limits their usefulness. Both the fixedcondylar and the semi-adjustable types willaccept facebow records, and, in addition, themore adjustable instruments accept protrusiveand lateral interocclusal records to allow fullbenefit of their capability. Facebows improve theaccuracy of occlusal development of these artic-ulators. Facebows were discussed in Part 6.
With the maxillary cast mounted via a
facebow transfer and the mandibular arch relatedto the maxillary arch via the gothic arch tracing,the development of satisfactory eccentric (lateraland protrusive) occlusion and articulation is pos-sible. In addition, small changes (2–3 mm) in thevertical dimension may be achieved on the artic-ulator, should this be required, without the needfor a new registration.
PRACTICEprosthetics
Fig. 12 a) Typical Gothic arch or arrowhead tracing of the mandibularmovementsb) Perspex locator placed over the arrowhead point to confirmreproducibility of RCPc) PVS putty moulded between the upper and lower bases to provide acoronal relationship
Fig. 13 a) Simple hinge articulator. b) Moveable fixed condylar paths articulator. c) Semi-adjustable articulator
ba
c
a b c
1 Zarb G A, Bolender C L, Hickey J L,Carlsson G E. Boucher’sProsthodontic Treatment 10th ed. pp272-281. St Louis: Mosby, 1990.
2 Gonzalez J B. Preventing and TreatingAbused Tissue in Essentials ofComplete Prosthodontics 2nd ed.Winkler S (ed) pp81-87. St Louis:Mosby, 1988.
3 Grant A A, Johnson W. Introductionto Removable Denture Prosthodontics2nd ed. pp61-67. ChurchillLivingstone, 1992.
4 Zarb G A, Bolender C L, Hickey J L,Carlsson G E. ProsthodonticTreatment 10th ed. pp283-295. StLouis: Mosby, 1990.
5 Cabot L B. Using articulators toenhance clinical practice. Br Dent J1997; 184: 272-276.
Helpful Hints1 Determine what freeway space is
appropriate for each patient.2 Confirm RCP is reproducible.3 Ensure the completed intermaxillary
records are sealed together and areunambiguous.

660 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 12, JUNE 24 2000
PRACTICEprosthetics
As has been mentioned in Part 1, in theUnited Kingdom the dental surgeon is the
sole agent licensed to prescribe and co-ordinatethe functional and aesthetic requirements foreach patient’s replacement teeth. In the deci-sion-making required for the selection ofreplacement (denture) teeth for edentulouspatients, the dental surgeon should show aknowledge of physiological and biological fac-tors pertinent to each patient. These factorsshould be co-ordinated with aesthetic factorsapplicable to each patient, taking notice ofpatient perceptions of appearance.
Dental literature is replete with anecdotal ref-erences to aesthetic aspects of complete dentureconstruction but this is an imprecise area, com-bining ‘scientific’ and ‘artistic’ principles. The‘scientific’ principles are based on reasonablylimited longitudinal studies that, ultimately,may not necessarily cater for the needs of eachindividual patient, while the ‘artistic’ compo-nent is a paradigm of clinician’s skill, technicianflair and patient acceptance. The integration ofthese principles has led to a variety of guidelinesto help the dental surgeon in the selection of(replacement) denture teeth. Unfortunately, onthe evidence of prescriptions sent to dental lab-oratories, it is clear that these well-intendedguidelines are often cast aside.1,2 It would seem,in general terms, that many clinicians fail torecord any selection of tooth mould and/orshade and thereby abdicate the responsibility ofselection of the shades and moulds to the dentaltechnician. Equally, most clinicians spend per-haps one or two minutes over the selection ofshades for six anterior fixed restorations but afraction of that time for complete denture teeth.
Such lack of any consideration of the bodyimage of the edentulous individual mirrors thestatus of complete denture prosthodontics indentistry; for the sake of the edentulous popula-tion, and our profession, this must not beallowed to continue.
The purpose of this section is to simplify thetask of selection of teeth by dividing the processinto four separate stages:
• Selection of upper anterior teeth• Selection of lower anterior teeth• Selection of posterior teeth types and
moulds• Selection of shade(s) of the anterior and pos-
terior teeth.
Selection of upper anterior teeth Using pre-extraction recordsIf patients have pre-extraction records (eg pho-tographs or casts) then the surgeon’s task issimplified, although the clinician should alwaystemper photographic evidence to accommo-date for biologically/chronologically-inducedage-changes. For example, the amount of cen-tral incisor tooth showing with the upper lip atrest in a 25-year-old tends to be considerablygreater than that of a person in late middle ageor older. Equally, the clinician should take intoaccount other dental-related changes such asphysiological wear of teeth and facial changesevident from the photograph (Fig. 1). Photo-graphic features and/or peculiarities of loweranterior teeth and posterior teeth may also bedetermined. For this a good, clear photographis required.
The use of photographs is to be strongly rec-ommended. Particularly useful are those of a
Registration: Stage III — selection of teethJ. F. McCord,1 and A. A. Grant,2
7
Fig. 1 Twophotographs to showsubtle facial anddental changes whichcan occur from lateyouth to middle age
In this section,particular attention isdrawn to guidelineson the selection ofteeth for completedentures. Factorsinfluencing selection ofteeth are discussedand presented intabular form for easyguidance.
In this part, we willdiscuss:• How to select appropri-
ate moulds of anteriorteeth
• How to select appropri-ate moulds of posteriorteeth
• Factors influencing shadeof teeth
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 188: 660–666

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 12, JUNE 24 2000 661
PRACTICEprosthetics
patient that were taken when the subjects wasdentate or wore dentures which were admiredby the patient. The photographs should realisti-cally show head-on facial views of the patientsmiling; failure to do this may not reveal anysign of the anterior teeth. Such views shouldenable the clinician to see and to measure care-fully the ratio of the patient’s horizontal inter-canine distance, and relate that to theinterpupillary distance in the photograph. Inthe clinic, the clinician may then measure thepatient’s interpupillary distance and it shouldbe possible to establish the horizontal width ofthe upper six anterior teeth (Fig. 2).
Other guidelines to the selection of replace-ment upper anterior teeth are itemised inTable 1.
In most cases, however, no adequate pho-tographs or other pre-extraction records areavailable and the clinician has to decide howbest to select the teeth that will satisfy aestheticand functional parameters. It is at this stage thatguidelines relating to anterior tooth position-ing may be used and these guidelines are cen-tred on the fact that the (six) upper anteriorteeth should:
• Appropriately support the upper lip• Occupy that area of the upper anterior arch
bordered by the corners of the mouth• Allow for individualisation where indicated,
eg rotation, imbrication or spacing.
It should be stressed that the patient may well
be entirely satisfied with the teeth on their pre-sent (or perhaps an earlier favoured) dentureand there is much sense in repeating the pre-scription of existing moulds.
We would argue that to achieve this, the clin-ician should select the teeth on the basis ofmeasurements and decisions made with theupper rim still in place, in order that functionaland aesthetic parameters may be assessed (seePart 5).
With the upper rim in place and the lipappropriately supported (see Fig. 8, Part 5) andthe incisal point determined, the patientshould be asked to smile. By marking the out-line of the high smile line on the upper rim, theclinician is assisting the decision making fortooth moulds (Fig. 3). Another critical point isto determine the position of the canine teeth.Earlier reference has been made to the use ofpre-extraction records. Where these are notpresent, some authorities advocate using theposition of the corners of the mouth, at rest.Another method, used by the authors, is to askthe patient to smile and to extend a line from
Fig. 2 (below) Template toassist in formulating the(horizontal) width of the uppersix anterior teeth
Table 1 Guidelines to the selection and position of upper anterior teeth* indicates that photographs of appropriate quality are used Nature of guideline Frontal view Sagittal view Coronal view Other
Pre-extraction Photograph Photograph Photograph (unlikely) Extracted teeth*Relate canine Cast of arch points to pupils Radiograph (unlikely)
*Relate canine points to Relative with similar inter-alar width (smiling) appearance
*Relate six anterior *Relate six anterior teeth to smile line teeth to smile lineCast of arch Cast of archRadiograph RadiographRelative of similar Relative with facial appearance similar appearance
.Post-extraction Central incisors restore Vertical naso-labial
philtrum if possible angleCentral incisors restore vermillion borderIncisal points and smile Amount of tooth line determine height of showing below lip at tooth (age-related) rest (age-related)Position of canine pointsRelate to inter-alar width (smiling)Relate to pupils (require pre-extraction photograph)Relation of upper rim to Relation of upper rim smile line to smile line
FIg. 2 Formula for calculating horizontal width
Width of upper six anterior teeth(photograph)
Interpupillary width(photograph)
Width of upper six anterior teeth
Interpupillary width(actual)
=

662 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 12, JUNE 24 2000
PRACTICEprosthetics
the inner canthus of the eye via the lateral bor-der of the alar cartilage and extend that ontothe upper rim. This may be done with a ruler orby the use of dental floss (Fig. 4). This equates,in a high proportion of cases, to the position ofthe tip of the upper canine teeth.3 If a flexibleruler was laid from one canine point to anotheron the upper rim (aesthetic control base [ACB]),the length of the ‘aesthetic anterior arc’ could beread off; this reading is the second criticaldimension required to prescribe tooth moulds(Fig. 5). Prior to scrutinising mould charts, how-ever, it is of critical importance that the cliniciandetermines how the patient desires the tootharrangement to look. If the patient wishes spac-ing, then clearly that would require teeth of asmaller width to be used. The converse is truewhere imbrication or crowding is desired. Theimportance of the two measurements is appar-ent when one examines most tooth mouldcharts. Figure 6 illustrates typical measurementsassociated with all anterior teeth, although in theinterests of fairness, fictitious mould names havebeen incorporated to avoid apparent favouringof any one mould. It can be seen that there arethree values allocated per mould:
1. The combined widths of all six anteriorteeth, ie from distal of canine to distal of the
contralateral canine (in mm). NB This isapproximately the circumference of theupper rim from one canine point to theother plus 8–10 mm.
2. The height of the central incisors from theincisal edge to the highest point on the labialface of the tooth corresponding to the high-est point of the crown (in mm).
3. The width of the central incisors.
While the third value is of use in the prescrip-tion of removable partial dentures, we do notsee any obvious value in the determination oftooth moulds for replacement complete den-tures other than ensuring that replicatedmoulds are copied faithfully.
Armed with these two measurements,which may be read off the record rim, theclinician should be able to select from thosemoulds that lie within 1 mm of the selectedintercanine distance. Similarly, an awarenessof dental ageing changes is required when theheight of the central incisors is being consid-ered. The distance measured from the recordrim is from the incisal tip to the high smileline. Most prosthodontic textbooks recom-mend that the highest point on the labialaspect of the crown lies 1 mm above this;clearly for middle-aged and older patients,modification of the central incisors will berequired (ie remove the translucent tip of theincisal edge) to reflect the age of the patient(Fig. 7). In order to customise the anteriorteeth to reflect the age of the patient, the clin-ician will usually select longer centralincisors than would be expected, to permitincisal grinding. On the other hand, somepatients may not show much of their teethwhen they smile. This may be a cultivatedhabit, for socio-psychological reasons, a con-sequence of tooth wear and a long upper lip,or perhaps simply a feature peculiar to thesepatients. This may be clear from a good pho-tograph of the patient smiling. It may also be
Fig. 5 Flexible ruler used tomeasure the (labial)circumference of the arc fromone canine tip to the other. Astooth mould charts for anteriorteeth give dimensions from thedistal of one canine to theother, 8–10 mm should beadded to the abovemeasurement, to cater for thedistal ‘half’ of each canine
Fig. 3 The scribing ofthe high smile line onthe ACB helps theclinician to determinethe height of thecentral incisor tooth.Care should be takento compensate fortooth wear
Fig. 4 Dental floss used to givean acceptable guideline forthe position of the canine tipon the ACB
Fig. 6 Tooth mould chartindicating dimensions of severalmoulds

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 12, JUNE 24 2000 663
PRACTICEprosthetics
apparent at the time of preparation of theupper rim (ACB).
The clinician is, at all times, advised to con-sult with the patient regarding the patient’swishes and expectations on tooth selection, toavoid, or at worst to minimise, any potentialproblems of acceptance of the replacementdenture at a later date.
Clinical experience, however, indicates thateven when these two measurements are fol-lowed, other factors are brought into play tofinalise anterior tooth selection. Williams, in1907, suggested that the frontal appearance ofthe face from the (normal) hairline to the chincould be used as a guideline to the inverseshape of the central incisor (Fig. 8).4 Sometooth manufacturers, in an attempt to assistclinicians to select appropriate tooth moulds,suggest that the labial shape of the anteriortooth reflects the shape of the (edentulous)maxillary arch. Neither of these has any scien-tific credence, indeed the latter takes noaccount of trauma or unusual post-extractionchanges.
We recommend that clinicians shouldassess the facial profile in a three-dimensionalway. This involves incorporating frontal andlateral views plus that taken from behind thepatient looking down the face, to determinean overall view of the dento-facial profile.Patients from each of the skeletal classifica-tions may be identified and this can help theclinician select a tooth mould which is inaccordance with the profile of the appropri-ately supported lip (Fig. 9) on the basis ofclinical experience of facial forms.
Selection of lower anterior teethAs has already been referred to, pre-extractionrecords may be used to ensure appropriatetooth selection and, indeed, the anterior formof the trial dentures.
When these are not available, referral may bemade to manufacturers’ mould charts to equatethe lower anterior teeth to the selected upperanterior teeth. Or the practitioner may opt tocreate a functionally-generated profile of thelower denture space5 (sometimes called theneutral-zone impression technique), identifythe position of the lower canines (via the angleof the mouth) and then measure the canine-canine distance. As tooth moulds for loweranterior teeth have the equivalent three mea-surements to upper anterior teeth, the clinicianmay choose for the mould that is appropriatefor each patient, taking age, facial form andpatient perceptions into account.
Selection of posterior teeth types andmouldsIt is probably accurate to state that this portionof the prescription form is least considered byclinicians, the choice of posteriors being often
made by technicians who tend not to have seenthe patient. This is a remarkable state of affairswhen one considers that complete dentures aresupposedly prescribed primarily to restorefunction and secondarily to restore facialappearance.
As this series is intended for interested gen-eral dental practitioners and not for special-ists, there will be no section on the geometryof occlusion, as that will be covered in stan-dard prosthodontic textbooks. It is pertinent,however, to discuss, albeit briefly, types of pos-terior teeth.
According to Lang posterior tooth mouldsare of four types:6
1. Anatomic2. Non-anatomic3. Zero-degree teeth4. Cuspless teeth.
According to the Glossary of ProsthodonticTerms, the following definitions apply to eachtype:7
Fig. 7 Photograph ofunprepared upperright central incisorfrom a mould (A). Themodified tooth (B)has been adjusted tosuit the patient bygrinding away theincisal translucency.The clinician shouldcompensate for thisin selecting the mould
Fig. 8 Williams’guideline to toothselection by relatingupper central incisorform to frontalappearance of theface has no scientificcredence
Fig. 9 With a well-formed upper rim(ACB) in situ, the clinician can interpreta skeletal form which may suggest anappropriate incisor arrangement. Inthis case, with the ACB, the v-shapedform of the maxilla is clear to see,suggestion of a Class II division Iappearance

664 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 12, JUNE 24 2000
PRACTICEprosthetics
1. Anatomic: teeth that have cuspal inclina-tions greater than 0° and tend to replicateocclusal anatomy. Such teeth may have cus-pal angles set to 20°, 30°, 33° or 45°.
2. Non-anatomic: teeth designed in accor-dance with mechanical principles ratherthan from the anatomic standpoint.
3. Zero-degree teeth: posterior teeth that have0° cuspal angles.
4. Cuspless teeth: teeth designed without cus-pal prominence on the occlusal surface ieinverted cusp teeth.
We would suggest, in the interests of clarity,that three types of posterior tooth form be con-sidered, namely teeth with cusps, teeth withoutcusps and teeth which exhibit both characteris-tics (hybrid moulds). Such teeth typically haveupper teeth with cuspal angles of 20° with mod-ified buccal cusps and lower non-anatomicteeth which have been rendered essentially cus-pless (Fig. 10a–c).
The decision the clinician has to make shouldbe determined out of the needs of the patient.In essence, three factors have to be considered,namely occlusal factors, stability factors andaesthetic factors (Table 2).
Occlusal factorsIf the patient only performs vertical mandibu-lar movements then it is possible that cusplessteeth will suffice. If, however, the patient per-forms ruminatory mandibular movements(watch the patient eat a biscuit or a piece of carrot), then teeth with cusps will be requiredfor balanced articulation (and thus stable den-tures). Examination of current dentures mayassist in the diagnosis (Fig. 11). For example, if
Fig. 10 a) Posteriorteeth which havecusps b) Posteriorteeth which arecuspless c) Hybridmould ie teeth whichare modified toobtain the benefitsof a) and b)
Table 2 List of factors influencing selection of posterior tooth form
Type of Tooth Occlusal factors Stability factors Aesthetic factorsTeeth with cusps
Teeth without cusps
Hybrid teeth The presence of cusps, even modified cusps, can facilitate balanced articulation with reduced chance of cuspal locking
Balanced occlusion Possible, but may require grinding to prevent slide from RCP to ICPBalanced articulation Cusps are required to obtain a truly balanced occlusion, but technician's skills and time are implicit, as is sound registration technique
If no slide present, stability possibleCan be problematic with flat lower ridges and in implant-borne cases
Tend to look better as they appear natural, as long as teeth of appropriate length are selected
Balanced occlusion Possible and these teeth generally take less laboratory time to set upBalanced articulation A truly balanced articulation is not possible with these teeth
Absence of cusps in the upper posterior teeth means balanced articulation is not possible
Have a worn (attrited) appearance
Balanced occlusion Possible some grinding may be necessaryBalanced articulation Possible if concepts such as lingualised occlusion are used, ie the maxillary palatal cusps are intended to maintain contact with their antagonists
Can look natural
a
b
c

BRITISH DENTAL JOURNAL, VOLUME 188, NO. 12, JUNE 24 2000 665
PRACTICEprosthetics
the dentures have occlusal surfaces that areevenly worn (ie flat), this is usually suggestive ofvertical (chopping) mandibular movements,whereas much greater wear of the maxillarybuccal cusps especially, is suggestive of rumina-tory mandibular movements.
Stability factorsIn addition to stability engendered out of mus-cle balance and occlusal balance in all borderpositions, cusps that tend to lock or cause trip-ping can aggravate the stability of dentures.This is particularly pronounced in flat, atrophicmandibular ridges. Some schools of thoughtautomatically prescribe cuspless teeth in suchcases; clearly if balanced articulation isrequired, cuspless teeth are, in such cases, illog-ical. Another factor to consider is the width ofthe posterior teeth. If the posterior teeth are toobroad, they could present to the tongue whatamounts to lingual undercuts and the presenceof these could lead to a major cause of instabil-ity (Fig. 12).
Thought should also be given to the numberof posterior teeth. There are few clinical situa-tions where there is sufficient mesio-distal lengthto incorporate two molars and two premolarswithout compromising stability (see Part 10 ondiagnosis of faults); common options are to dropoff either one premolar or one molar.
Aesthetic factorsThese factors are ones that can only be deter-mined by the patient and are a good example ofthe value of informed consent; the patientshould be informed of the options and allowedto decide on the appearance of posterior teethas well as anterior teeth.
Selection of colour and shade of teethAs this book is intended to serve as a clinical aidfor general dental practitioners, no attempt willbe made to detail the fundamentals of thecolour scheme.
While great care is often spent by dental prac-titioners over the selection of teeth of appropri-ate colours and shades, eg six anterior crowns,conventional wisdom would suggest that this isnot the case where the selection of teeth forcomplete dentures is concerned.
Nevertheless, practitioners should take intoaccount four qualities when selecting dentureteeth.
1. Hue: This is a specific colour resulting fromlight of a particular wavelength acting on theretina. The hue is an indication of a specificcolour, eg blue, green, reddish yellow. Someauthorities suggest that the hue of teethshould harmonise with the hue of thepatient’s face/natural hair. Others, however,quote studies that cast doubt on this philos-ophy.8
2. Saturation (chroma): This represents theamount of colour per unit area, eg a toothmay appear greyer than another tooth. Thehue of both teeth could be equal or one toothcould contain a higher saturation of the greythan the other.
3. Brilliance (value): This equates to the light-ness or darkness of a tooth. Variations inbrilliance are affected by dilution of thecolour (ie the hue) by black or white. It is theratio of white or black on teeth to the naturalhue which determines the lightness or dark-ness of teeth.
4. Translucency: This property enables light topass through a body without giving any dis-tinguishing image.
The careful selection of colours and shades ofteeth is therefore verging on the artistic inter-pretation of the clinician and the patient. Thepatient may have very strong views on the shadeof their replacement dentures and it may be aclinical advantage to have two options availablein shade guides. One is the standard shade guidewhich is calibrated in shades A, B, C and D. The second option is ranged from the lightest
Fig. 11 This patient clearly undertakes a range of bordermovements and should be provided with balancedarticulation
Fig. 12 The occlusal tables on this lower denture are toolarge. First of all, the excessive width of the molars ispresenting lingual undercuts which will de-stabilise thedenture. In addition, the presence of the second molar onthe inclined plane of the ramus will induce a protrusivemovement

666 BRITISH DENTAL JOURNAL, VOLUME 188, NO. 12, JUNE 24 2000
PRACTICEprosthetics
shade C to the darkest shade (Fig. 13a and b).We would emphasise a careful and deliberateconsultation with patients regarding shades ofteeth, taking into account age (teeth tend tobecome darker with age although this is notalways absolute), patient preference and, withguarded reservation, skin colour. The selectionmay also be varied, eg there is often justificationin having canine teeth slightly darker thanincisors (Fig. 14).
When all of these details have been recordedon the laboratory (prescription) card, the rimsmay be dispatched to the laboratory for finaldentures to be made.
ba
Fig. 13 Vita shade guide: a) arranged according to colour; b) according to lightness
1 Basker R M, Ogden A R, Ralph J P.Complete denture prescription — anaudit of performance. Br Dent J 1993;174: 278-284.
2 Barsby M J, Hellyer R P, Schwarz WD. The qualitative assessment ofcomplete dentures produced bycommercial dental laboratories. BrDent J 1995; 179: 51-57.
3 Grant A A, Johnson W. Introductionto Removable Denture Prosthodontics2nd ed. pp 88-89. London: Churchill-Livingstone, 1992.
4 Williams J L. A new classification ofhuman tooth forms with specialreference to a new system of artificialteeth. Dent Cosmos 1914; 56: 627-628.
5 McCord J F, Grant A A, Quayle A A.Treatment options for the edentulousmandible. Eur J Prosthodontics RestDent 1992; 1: 19-23.
6 Lang B R. Complete DentureOcclusion. Dent Clin N Amer 1996;40: 85-101.
7 American Academy ofProsthodontics. Glossary ofProsthodontic Terms. J Prosthet Dent1994; 71: 56-107.
8 Landa L S. Anterior tooth selectionand guidelines for complete dentureaesthetics In Winkler S (ed).Essentials of Complete DentureProsthodontics 2nd ed. St.Louis:Mosby 1988, 202-216.
Helpful Hints1 Listen to the patient’s views.
2 Use photographs/favoured dentures ifpossible.
3 Use the aesthetic central base to assistin the delineation of the maxillary‘anterior aesthetic arc’.
4 Select lower anterior teeth to comple-ment the upper anteriors.
5 Select posterior teeth using aestheticand functional criteria.
Fig. 14 View ofnatural incisors. Notethere is no realharmony betweenthe hue of the faceand that of the teeth.The canines,however, are darkerthan the incisors

4 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 1, JULY 8 2000
PRACTICEprosthetics
Trial dentures, insertion ofprocessed dentures and reviewof complete denturesJ. F. McCord,1 and A. A. Grant,2
This chapter will be divided into three sec-tions: one devoted to clinical aspects of the
delivery of trial dentures, another to the deliv-ery of the processed dentures, and the third sec-tion will deal with the review appointment.
Trial insertion of complete denturesBy definition, a trial denture is the arrangementof teeth in wax, for trial, prior to completion ofthe denture.1
By convention, this stage typically occupies oneclinical visit, unless the trial denture has errorswhich are of clinical and/or technical origin! The temporal constraints of prosthodon-tic practice under NHS Regulations have oftenperceived this visit to be transient by nature. Wewould seek to redress this scenario and offer thesuggestion that two trial visits may be consideredas being both sensible and practical.
In the same way that the trial visit is oftenlabelled a dress rehearsal, the analogy to ourthespian counterparts is worth closer investiga-tion. The role of a dress rehearsal for a theatrecompany is threefold. First of all, it enablesactors to verify that they are all word-perfect.Secondly, it enables the wardrobe manager toconfirm that the costumes and props are appro-priate, both from a point of fit and also for veri-fying the temporal continuity of the costumesto the historical period reflected in the play.Finally, it enables the director to establish thatall lighting changes and stage scenery areacceptable.
It is therefore perhaps appropriate to specifythe role of the trial denture stage(s). Again,three aspects must be considered.
• The functional and aesthetic acceptability ofthe dentures, according to the dentist (den-tist’s role).
• The functional and aesthetic acceptability ofthe dentures, according to the patient(patient’s role).
• The competence of the technical delivery(technician’s role).
These components are summarised in Table 1.
The dentist’s roleOn receipt of the articulated trial dentures, theclinician should perform more than a cursoryexamination of them prior to their placementin the mouth. The first stage is to ensure thatthe maxillary and mandibular trial dentures arewell adapted to the respective master casts andthat both bases are stable. The technician isresponsible for ensuring the accuracy of fit ofbases to casts while the ultimate responsibilityfor the accuracy of reproduction of the oral tis-sues rests with the clinician who recorded thedefinitive impression.
The next stage is to remove the mandibulartrial denture from the articulator and to assessthe relationship of the maxillary posterior teethto the mandibular ridge. As a general guide to(lower) complete denture stability, the palatalcusps of the maxillary premolar and molar
8
Fig. 1 Relationship ofmaxillary palatalcusps to themandibular ridge. Itis recommended thatthese cusps areplaced over thelower ridge crest andthus occlude with thecentral fossae of themandibular posteriorteeth
In this section,checklists aredescribed to assist thepractitioner inverifying theacceptability/non-acceptability ofcomplete dentures attrial insertion andinsertion visits. Therelative roles ofclinician, technicianand patient arediscussed.
In this part, we willdiscuss:• The integral aspects of
the trial denture visit• The integral aspects of
the insertion visit• What to do at the
review appointments
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 189: 4–8

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 1, JULY 8 2000 5
PRACTICEprosthetics
teeth should lie over the mandibular ridge(Fig. 1).
With the mandibular denture still off thearticulated mandibular casts, there is muchmerit in assessing the position of the poste-rior teeth by holding a straight-edged instru-ment on the ridge-section of the mandibulardenture (Fig. 2); the central fossae of thelower posterior teeth should overlie thestraight edge (this represents the zone occu-pied by the palatal cusps of the maxillary posterior teeth in retruded contact position[RCP]).
When both trial dentures have beenremoved from the articulator, the clinicianshould inspect the intermaxillary space toensure no unplanned increase or decrease indimension has occurred. If an intra-oral trac-ing method was used, the intermaxillaryspace may be verified by examining the cen-tral-bearing apparatus that should still be inthe work tray. This provides a good guide tothe distances between the upper and lowerridges. The clinician should also examine thecasts to ensure that no laboratory-induceddefects have been induced on the denture-bearing areas.
If both dentures are replaced on their respec-tive casts, the clinician may then examine theocclusal relationships of both dentures, toestablish that balanced occlusion is present and,if requested, that balanced articulation has beenrealised.
With the patient present, and followinginfection control procedures,2 the mandibulardenture may be inserted in the patient’s mouth.There are several reasons why there is merit ininserting the mandibular denture first.
• If the maxillary denture is inserted first, thetwo buccinator muscles are, ideally, restoredto their functional width and subsequentinsertion of the mandibular denture maystretch the oral commissures; this may be asource of discomfort for many long-termedentulous patients.
• If the maxillary denture is inserted first,insertion of the mandibular trial denturemay dislodge the upper denture and thismay alarm the patient unnecessarily.
• The verification of a stable denture base and,further, of a peripheral seal in a lower den-ture is a source of relief and a confidencebuilder for patients who have a history oflower denture problems.
• The patient may be shown how to use thetongue to control or ‘weigh down’ themandibular denture. Careful instruction, atthis stage may assist the patient to establishgood circum-denture muscle balance whichwill enhance denture stability (Fig. 3).
When the mandibular denture has beeninserted, it should be checked for stability. If the
Table 1 Summary of components for trial denture assessment
Personal responsibilities Factors to be considered
Dentist’s role • Ensure that the trial dentures fit the master casts and that the bases are stable.• Verify the vertical, sagittal and coronal intermaxillary relations.• Verify the stability of the bases in the mouth. • Verify the selection of anterior and posterior teeth, their colour and that the occlusal planes are correct.• Verify that speech is lucid.• Verify that the waxwork is aesthetic and functional.
Patient’s role • To record their wishes and expectations.• Informed consent agreed and that the patient approves of any alteration in form from the previous dentures.• The patient, and any accompanying person, should agree on the acceptability of the trial dentures and that the patient is happy to proceed to completion.
Technician’s role • To have replicated the registration records faithfully.• To place teeth according to prosthodontic norms.• To provide stable bases.• To ensure that balanced occlusion/articulation is provided, according to the prescription by the clinician. • To have articulated casts appropriately and to have set condylar angles to any prescription given.• To ensure waxwork is complementary to the age and personality of the patient.
Fig. 2 A wax knifeis placed over the‘ridge space’ of atrial denture to helprelate the accurateplacement of themandibularposterior teeth

6 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 1, JULY 8 2000
PRACTICEprosthetics
base is stable on the master cast and unstable inthe mouth, the possibility of a faulty definitiveimpression must be considered; if this is thecase, a new definitive impression is indicated.
The extension of the mandibular denturebase should also be assessed, bucco-labiallyand lingually. Over-extension should beremoved and under-extension corrected; if thelatter is a consequence of lack of extension intothe master cast, the deficiency may be resolvedby addition. If, however, the master cast isunder-extended, problems of support and sta-bility may arise (see Part 10), and a new defini-tive impression is indicated — the importanceof educating the patient on how to control thelower denture has already been referred to.These factors should, of course, have beenidentified and corrected at the registrationstage, but the thoroughness of double-check-ing at this stage should reduce post-insertionproblems.
The maxillary trial denture is then assessedfor stability and for over-/under-extension.The same guidelines for under-/over-extensionof the lower denture base apply for the upperdenture.
When both trial dentures are in the mouth,the following four aspects of the dentures maybe assessed in turn.
• Occlusal relations.• Occlusal planes.• Appearance of teeth and gums (gingival
matrix).• Speech — should not be adversely affected
by dentures.
Occlusal relationsAs has been pointed out in Part 6, there arethree intermaxillary relations to consider.These are the vertical, antero-posterior or sagit-tal and coronal intermaxillary relations.
The vertical relation is the occlusal verticaldimension (OVD) and the clinician shouldensure that this has been reproduced faithfullyfrom the registration sent to the technician.Figure 1, Part 6 illustrates how resting verticaldimension (RVD) and OVD may be measuredto determine if the FWS is appropriate and the
significance of this cannot be understated. Aswill be detailed later, vertical relations may alsobe assessed phonetically.
The sagittal or antero-posterior relation, atthe established OVD should, in the completedenture patient, incorporate the retruded con-tact position (RCP) which is coincident withintercuspal position (ICP).3
The coronal relation relates the mandibulararch to the maxillary arch in a relationship gen-erally observed from the frontal aspect.
The minimal requirement of all completedentures is that all posterior teeth of bothdentures (including canines) meet simultane-ously and evenly in RCP. If balanced articula-tion is required, this should also be present inright and left working and protrusive move-ments. Verification of balanced articulation atthe trial denture stage is recommended butshould be done cautiously as the teeth are setin wax and may be dislodged if the patient isover-vigorous — even in the absence ofocclusal interferences.
If the occlusal relation on the articulator isnot matched in the mouth, especially RCP, theclinician should consider re-registering theocclusion. Only if there is a slight slide fromRCP to ICP (ie less than 0.5 mm) can the clini-cian justify not re-registering the intermaxillaryrelationships.
If the occlusal relations are acceptable, theclinician should then confirm the acceptabilityof the occlusal planes.
Occlusal planesIn this category, four planes may be considered,namely the incisal plane, left and right posteriorocclusal planes and the plane of the mandibularteeth.
Incisal plane: The inter-pupillary line is anacceptable guideline for this plane and the clin-ician, and the patient, should confirm itsacceptability.
Right and left occlusal planes: Standardguidelines for these planes are that they shouldbe parallel to the alar-tragus line and instru-ments such as Fox’s occlusal plane guide maybe used to confirm these planes (the right maynot equal the left). Inappropriately formedplanes may result in occlusal errors that mayresult in pathognomonic signs and symptoms(see Part 10).
Plane of the mandibular teeth: Ideally, theresting tongue should overlie the lingualaspects of the lower teeth and this may bedemonstrated to good effect at the trial denturestage to augment (lower) denture stability videsupra.
Appearance of teeth and gums (gingival matrix)This aspect of the trial denture visit(s) is of con-siderable importance to the patient and theacceptance of the dentures by the patient
Fig. 3 The lower trial denture iscontrolled by thecircum-denturemusculature toenhance stability andimprove patientconfidence

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 1, JULY 8 2000 7
PRACTICEprosthetics
reflects the acceptability of tooth positioning,tooth selection and colour selection by the clin-ician plus the technical competence of the tech-nician. Given the complexity of occlusal andaesthetic factors, we recommend that two trialvisits, as a minimum, be allocated. This is especially valid when patients have a history ofdenture-related problems or where difficultiesare anticipated.
It is easy to be confused, if not discouraged,when there is a need to adjust twelve or four-teen teeth per denture. There is, therefore,merit in asking the technician to set-up only thesix anterior teeth in each denture for an initialtrial insertion. The appearance of only six teethper denture may be seen, altered and agreedupon easily. In addition the vertical and antero-posterior intermaxillary relations of the trialdentures can be verified (Fig. 4).
When the form and arrangement of theupper and lower anterior teeth have beenagreed upon, the second trial denture visitcould be arranged, at which the posteriorteeth are positioned and occlusal relationscould be checked.
It must not be overlooked, however, that thetechnician’s skills lie not only with tooth place-ment and angulation; in addition to these fac-tors related to appearance is the contour of thewaxwork equivalent to the gingival architec-ture. Here, the interdental papillae should beconvex, the papillary lengths varied and the tis-sue heights formed appropriately to create anatural appearance (Fig. 4).
SpeechSpeech is an important function that in generaloften receives scant attention from the dentalprofession. Most dentists are aware of theimportance of clarity of sibilant sounds, in par-ticular the test for the ‘closest’ speaking space, ieask the patient to say ‘Mississippi’.
Other phonetic tests which may be usedrelate to other consonant sounds, namely frica-tives or labio-dental sounds (eg ‘f ’ or ‘v’). Byasking a patient to say a sentence such as ‘fishand vinegar’ the clinician can determine if thefricative sounds are clear and this will help ver-ify the appropriate placement of the upper cen-tral incisors antero-posteriorly.
When all of these tests have been performedby the clinician, we would recommend that theclinician leave the patient for a short time withtheir trial dentures, preferably in the companyof a friend. Then allow the patient to converseand, in general, acclimatise to the proposedform of the replacement denture. Thereafterany additional modifications may be made tothe dentures.
When the patient and the clinician are bothsatisfied with the trial dentures, the denturesmay be sent for processing. Prior to returningthe trial dentures to the laboratory for process-
ing, thought should also be given to determin-ing the shade of the denture base. This may betranslucent in the palate, pink or veined or maybe modified to conform to the gingivae of thepatient.
The patient’s roleThe successful provision of replacement den-tures owes much to patient co-operation andadaptation. Neither of these factors can bedefined with clarity nor can they be easily quan-tified. For this reason, patient consent to form
and appearance is paramount. As has beenmentioned previously, we recommend that twotrial denture visits be arranged, partly to facili-tate any alterations to be performed at chairsideby the clinician but also, of equal importance,to enable the patient to adjust and to consent tothe form and appearance of the replacementdentures.
The technician’s roleAlthough Part 9 will address technical consid-erations in the prescription of complete den-tures, it is important to stress the importanceof close, unambiguous communicationsbetween clinicians and technicians. The aimsand objectives of a quality complete dentureservice should be common to both parties ifthe patient is to have any chance of adaptingto replacement dentures. For these reasons,casts of acceptable quality require thatimpressions of acceptable quality are deliv-ered. Similarly, technicians who spend a con-siderable time placing teeth in wax rims andthen contouring the wax are understandablyaggrieved when a reset is demanded because‘the bite is wrong’. The role of the technician isclearly that of a skilled team member who iswholly reliant on the clinician performingmaximally.
Insertion of processed denturesIn essence, the clinical procedures of this stagemirror those of the trial denture stage, theexception being, hopefully, that the patienttakes the replacement dentures home. Sometechnicians process dentures on the master
Fig. 4 Six upper andlower teeth havebeen set up for thefirst trial visit. Thisallows the clinicianto determine that theocclusal parametersare acceptable andthat the patient andthe clinician mayjudge theappearance of theanterior set-up

8 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 1, JULY 8 2000
PRACTICEprosthetics
casts and return the polished, processed den-tures to the clinician in a plastic bag or someother receptacle. Many quality laboratories,however, practice a more ideal technique ofhaving the dentures processed on duplicatedmaster casts, so that the dentures are returnedon casts and on the articulator.
The advantage of some articulator systems, ofwhich the Denar system is a good example, isthat the laboratory work may be sent on themounting platforms and the technician andthe dentist may retain their own articulators,yet both may be confident of the accuracy ofthe mounting.
The benefits of each surgery having a goodarticulator cannot be over-emphasised, as itenables the clinician to thoroughly examinethe trial dentures and processed denturescomprehensively before they are inserted intothe patient’s mouth. Assuming that the abovepractices are followed, the suggested sequenceof events required at the delivery stage are asfollows:
1. With the processed dentures on the articu-lated casts, verify that the dentures are inbalanced occlusion, and that the incisalguidance post is in contact with the incisalguidance platform. If the post is off theplatform, an occlusal error/disturbancehas occurred and this should be identified,using articulating paper, and the prema-ture contacts should be ground to enablethe post to contact the platform.
2. Check working, balancing and protrusiveocclusions. Again the post should remainin contact with the platform during thesemovements. A different colour of articulat-ing paper is recommended for each excur-sion. Prematurities should be removedonly after they have been identified via thearticulating paper. Polish the occlusal sur-faces that have been ground.
3. Remove the dentures from the casts andensure there are no sharp ridges or acrylicpearls on the ‘impression’ surface of thedenture.
4. After appropriate infection control, placethe lower denture in the mouth and assessthat no over-extensions occur along theperiphery of the denture. Gently press onthe occlusal surfaces of the lower premolarteeth and ensure no support problems areevident at this stage.
5. Position the upper denture and ensure thatno over-extensions are present along theperiphery. Similarly, ensure no supportproblems exist at that stage by pressinggently on the occlusal surfaces of the pre-molar teeth.
6. Confirm the occlusal relationships areacceptable, as per stages 1 and 2.
7. Confirm appropriate freeway space exists.8. The patient then be re-instructed how to
use the tongue to control the lower den-ture.
9. We further recommend that, at this stage,the patient should be instructed to bite onthe tip of a cotton wool roll (or a carrot)between the first premolar and canineteeth of the upper and lower dentures on apreferred biting side. Instruct the patient tokeep a grasp of the roll (unless this ispainful) and then pull the cotton wool rollaway from the patient. Pain indicates eitherthat a support problem exists or that thedenture base is unstable. As the lattershould have been excluded before, the sup-port problem may be located via pressure-relief paste and the denture base relievedappropriately (see Part 10). An acceptableocclusal result is perceived to have beenobtained if the cotton wool roll breaks. Theobject of this exercise is to instruct thepatient how to bite (ie teach the patient to‘caninise’ to incise).
10. Finally, let the patient inspect the denturesin a mirror and assess speech by asking thepatient to repeat their address, etc.
Review proceduresThe topic of dentist-organised reviews is proneto variation. It is our practice to arrange areview 4 days after insertion and a secondreview 1 week after that. Depending on factorsas diverse as status of denture-bearing tissues,patient perceptions, etc, patients may requestfurther ‘views’. The procedures for dealing withdenture problems will be dealt with in Part 10.
Epidemiological data would support theannual review of complete denture wearers toscreen for any pathological changes in the oraltissues or associated denture-related problems.
Helpful Hints1. Closely scrutinise the trial dentures on
the articulated casts — do they equateto what you prescribed, and are thetrial dentures well adapted to the casts?
2. Confirm that the position of the anteriorand posterior teeth is acceptable.
3. Place the lower denture in the mouthbefore the upper when assessing bothdentures as a dental unit.
4. The planned usage of two trial visitshas much merit. The first concentrateson verifying OVD, RCP andappearance. The second confirmsposterior planes, mandibularmovements and a refinement ofappearance.
1 Nairn R I, Shapiro M M J. ProstheticDentistry Glossary in Guidelines InProsthetic and Implant Dentistry,1996. London: QuintessencePublishing Co., pp29-97.
2 Control of Cross-Infection inDentistry. BDA Advisory Services.
3 Guidelines to Standards in ProstheticDentistry — Complete and PartialDentures In Ogden A (ed )Guidelines in Prosthetic and ImplantDentistry 1996. London:Quintessence Publishing Co. Ltd, pp7-16.

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 2, JULY 22 2000 71
Technical aspects of completedenture constructionJ. F. McCord,1 and A. A. Grant,2
On several occasions throughout this series,mention has been made of the need to
establish, and maintain, a good working rela-tionship between the clinician and the techni-cian. In order that this relationship may beprosthodontically productive, respect has to beearned from both these members of the den-ture team. This requires that consistency ofquality should be the aim for all stages of com-plete denture construction and by clinician andtechnician alike.
With the above in mind, this section seeks tohighlight, on a chronologically sequential basis,the technical involvement with each clinicalvisit. To avoid repetition for each stage, it will beassumed standard practice for all work to bedisinfected in the surgery and in the laboratorybefore commencement of each stage.
Primary impression visitThe primary aim of this visit is to record, in stocktrays, the denture-bearing areas of each arch.According to the Guides to Standards in Pros-thetic Dentistry,1 there are basic requirementsrequired for primary impressions, and these arelisted in Table 1. In addition to these, it is recom-mended that the clinician, if not casting theimpressions, will indicate the extent of the den-ture-bearing area. An indication, on the pre-scription form of the spacing for and design ofthe special tray(s) is also required, as the techni-cian cannot tell from a stone cast the relative dis-placeability of tissues and, in consequence,where relief is required.
Technician’s objectivesFigure 1 illustrates a good quality primary(plaster) cast that has faithfully reproduced all
of the requirements listed in Table 1. The iden-tification of the outline of the peripheralextension of the special tray, scribed on thecast by the clinician, enables the technician toconstruct a special tray to the itemisedinstructions of the clinician. An example of agood quality light-cured special tray is shownin Figure 6, Part 4 — this tray had a 2 mmspacing overlying the cast.
Definitive impression visitThe aim of this visit is to record the denture-bearing tissues, at the appropriate degree of tissue displacement, in addition to recordingthe functional width and depth of the sulci. Inthis way, support, retention and some of theaspects of stability are addressed.
Technician’s objectivesThe definitive impressions are cast in stone or75% stone-plaster mix (in the interests ofstrength) and these function as master casts. Aswas referred to in Part 4, the clinician shouldscribe, on the definitive impression, the posi-tion of the post-dam and also the plannedpreservation of the peripheral roll (see Fig. 9,Part 4).
By boxing out the land area relevant to thepreserved peripheral roll, the technician shouldpresent a quality cast that only requires that theclinician inscribe the extent of the post dam.
Equally, it may be that some areas of the castmay require to have tin foil added to producerelief areas, or some areas, eg undercuts, may beblocked out using plaster (Fig. 2).
The responsibility for the selection of thematerial to form the base of the upper andlower rims rests with the clinician. Table 2,
9
Table 1 Minimal requirements of areas to be recorded in primary impressions for complete dentures
Maxillary arch Mandibular arch
Residual ridge including the full extentof the tuberosities and hamular notch
Residual ridge, including the full extent of theretromolar pads
Functional depth of labial and buccalsulci, including fraenae and muscleattachments
Functional depth of labial and buccal sulci, including fraenae, muscle attachments and external oblique ridges
The hard palate and its junction with the soft palate
The lingual sulci, lingual fraenum, mylohyoid ridges and retro-mylohyoid areas
This article deals withtechnical aspects ofcomplete dentures aswell as the importanceof good communicationbetween the clinicianand the technician. Theobjectives fortechnicians for eachcomponent arediscussed.
In this part, we willdiscuss:• Technical objectives in
the preparation of a castfor tray construction.
• Technical objectives ofrim preparation.
• Aspects of tooth placement.
• The importance of good dentist-technician communication
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 189: 71–74
PRACTICEprosthetics

72 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 2, JULY 22 2000
Part 5 lists the materials which may be used asbases and most technicians should have theskills to make well-adapted bases (which willimpart stability at the next clinical stage) in allof the above materials.
When the master cast has been completed tothe needs of the patient, the technician has toproduce record rims or upper rim/aestheticcontrol base (ACB) and central-bearing appa-ratus to the clinician’s instructions.
Anecdotally speaking, this aspect of the clini-cian-technician interface is the weak link of theprescription process as the technician often hasno way of knowing where to place the labial faceof the upper rim, nor does he or she know theheight of the labial face of the rim.
It is entirely probable that a combination ofdiverse teaching philosophies concerning theplacement of maxillary teeth on replacementdentures (and thus the form of the upper rim)among both clinical and technological teachinginstitutions has contributed to confusion onhow technicians should make the upperrim/ACB. Copy denture techniques, the Almagauge or the use of devices such as the alameterand the papillameter (Part 5) have assisted inhelping the technician to customise an upperrim/ACB that should not require too muchaddition/removal of wax.
While the same thoughts apply for thelower conventional record rim, the simplifi-cation of the ‘Manchester rim’ or the con-struction of the central-bearing apparatusreduces the potential for confusion overdimensional parameters .
It is the objective of the technician to fabri-cate all of the component pieces for the third
clinical visit and to ensure that they are well-adapted, stable and finished to a high quality.Failure to have any piece of apparatus fit thecast is the fault of the technician; the converse isalso true, namely that if the base fits the cast,but not the relevant arch, the fault often lieswith the clinician.
Third clinical visitThe aims of this visit are threefold:
• To determine the form of the upper dentureand to provide clear guidelines for the place-ment of the teeth. This may or may notinvolve a facebow transfer, depending on thepreference of the clinician.
• To relate the mandibular arch to the maxil-lary arch in a reproducible three-dimen-sional prescription.
• To select teeth of appropriate mould andshade.
Technician’s objectivesOn receipt of the completed prescription fromthe clinician, the technician has to relate theupper cast to the articulator, the nature ofwhich should ideally be selected by the clini-cian. For simplicity, a Denar facebow hasbeen used throughout this section. The tech-nician transfers the upper rim/ACB to thearticulator via a transfer jig (Fig. 3). In thisway, the relationship of the maxillary plane tothe patient’s condylar axis is transferred to thearticulator, forming an equivalent relation-ship to the articulator’s condylar axis. Prior tomounting the upper cast onto the articulator,the technician should ensure that indexgrooves are placed on the base of the cast (Fig.4). This facilitates the process termed split-casting which enables casts to be remountedaccurately onto the articulator post-process-ing. In this way, any processing-inducedocclusal errors may be eliminated. To elimi-nate errors, the gypsum product should bemixed with water containing a food colouringand an anti-expansion agent. The formerenables good colour contrast between themaster cast and the mounting medium whilethe latter substantially reduces any small,potential errors which might arise in themounting of casts.
An alternative option to the use of indexinggrooves is the use of magnets to locate the caststo the articulator.
The second task for the technician is to mountthe lower cast on the articulator in the referenceestablished by the clinician. Again for reasons ofestablished technological procedure, the lowerbase should have index grooving placed.
When the upper and lower casts are articu-lated, the technician uses the teeth of selectedshade and mould and arranges the upper teethas follows.
PRACTICEprosthetics
Fig. 1 Typical example of agood quality primary castclearly demonstrating theprimary and secondary supportareas of the mandibulardenture-bearing area. Bydefinition, it is over-extended inorder that the extent of thespecial tray may be tracedappropriately (indicated)
Fig. 2 1mm tin foilrelief has been placedover a torus palatinusand the incisivepapilla to reduceproblems of supportpost-insertion

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 2, JULY 22 2000 73
• To the form of the labial surface of theupper rim/ACB.
• The posterior teeth are positioned such thattheir palatal cusps overlay the lower ridge(Fig. 5).
• Antero-posterior and palato-buccal com-pensating curves commence at the upperfirst molar teeth.
Lower teeth are set up with the necks of the ante-rior teeth over the lower ridge and the centralfossae of the posterior teeth overlying the lowerridge. Particulars of tooth positioning and set-ting up may be found in standard textbooks ofdental technology or of prosthodontics.
In addition to skilled placement of the den-ture teeth in wax, the technician has the respon-sibility of combining form and function,ensuring that balanced occlusion exists inretruded contact position (RCP) in every case,and balanced articulation when so requested bythe clinician.
In addition to embedding teeth in wax torestore dental appearance and function, thetechnician should then mould the wax repre-senting the gingival architecture appropri-ately. Clearly if the clinician gives noinformation to the technician, then the tech-nician can only guess the desired characteri-sation of the gingivae — photographs areexceedingly useful.
As was mentioned in Part 8, we recommendthat two trial visits are organised, The first visit,with the six upper and six lower anterior teethset-up enables verification of occlusal verticaldimension (OVD), RCP and the acceptabilityof both bases from those aspects relating tocomfort, stability and the appearance of theanterior teeth. With these important aspectsestablished, we would argue that it is easier, forboth clinician and technician, to concentrateon details relating to the form of the teeth andalso the gingivae. In essence, the technicianshould ensure that the gingival architecture sat-isfies four criteria.
1. It should be convex antero-posteriorly andsupero-inferiorly, to indicate a healthyappearance, at the same time ensuring ahygienic, self-cleaning form.
2. It should have an harmonious arrangementof heights of the gingivae; ideally the crescentof the gingivae is highest in the middle of theupper central incisors, drops for the lateralincisors and rises again for the uppercanines. The height of the gingival crescentsfor the upper first premolar teeth should beapproximately identical to those of theupper canines.
3. The interdental papillae should demonstratea natural pattern, ideally being longestbetween the upper central incisor teeth. Theabove three aspects are shown clearly inFigure 6.
4. The technician should use dental floss toremove excess wax interdentally. At the trialdenture stage, this merely reflects on lack ofattention to detail by the technician; if un-noticed, it can result in dentures with pooraesthetic quality (Fig. 7).
Trial denture visitsThere are four main aims of this visit:
• To verify that the appearance of the denturesis satisfactory.
• To verify that the occlusal requirements havebeen achieved.
• To confirm that speech has not beenadversely affected by the form of the replace-ment dentures.
• To decide on any requirements for the den-ture base eg veined acrylic, translucentacrylic on the palate, staining, placement ofrestorations, etc.
When these checks have been performed, andclinician and patient are satisfied with the formand function of the trial dentures, the techni-cian may proceed to process the dentures.
PRACTICEprosthetics
Fig. 4 Grooves onthe cast facilitateremoval andremount via the split-cast system. Asimilar mechanism isachieved via the useof magnets to retainand locate casts
Fig. 3 Denartransfer jig relatesthe bite-forkassembly to thearticulator
Fig. 5 The use of atranslucent mountingtable enables thetechnician to assessthe relationship ofthe maxillary palatalcusps to themandibular residualridge. The anteriordark linecorresponds to theoutline of the upperrim. The areascorresponding to themid-incisal point andthe canine pointshave been marked

74 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 2, JULY 22 2000
Technician’s objectivesPrior to preparation for processing, the tootharrangement is rechecked to ensure no damageoccurred in transit from the clinician, and thatno tooth is loose. Similarly, the waxwork in rela-tion to the teeth is checked to ensure that eachtooth is securely sealed in place (this is anotherbenefit of the use of convex interdental papillae).
The waxwork relating to the polished sur-faces is also checked to ensure it is well adaptedto maintain the peripheral roll.
The occlusion and teeth are double checkedto ensure no alteration has occurred to theocclusion — this should be done immediatelybefore investing as small changes might occur ifsizeable alterations were made to the waxwork.
On the assumption that the denture base ispolymethylmethracylate (PMMA) and that theclinician has instructed the technician on thespecifics of the polymer, the technician willinvest the (dis-articulated) casts in the lowerhalves of dental flasks.
The other halves of the flasks are then used to‘hood’ the teeth to be used in the denture, and
the bulk of stone investing these teeth isintended to minimise tooth movement duringpacking and processing of the dentures.
In essence, the process of converting wax trialdentures into completed dentures comprisestwo stages and these involve removal of waxand replacing the wax with polymerdough/putty which is processed under pres-sure. The wax elimination procedure uses hotwater to soften and remove the wax. Thereafterthe technician has the option of using one oftwo techniques to process the PMMA.
The first process involves placement of thePMMA dough manually into the flasks, effect-ing a trial closure and then clamping the flasksunder pressure and controlled temperaturewater bath for the appropriate curing cycle.
The second procedure involves injectionmoulding of pre-packaged dough/putty, underpressure into the flasks and the dentures arethen processed conventionally. The pre-pack-aged dough has the advantage that the techni-cian need not handle the unprocessedmonomer, a factor with health and safetyimplications. The injecting equipment is quiteexpensive, but there are claims (as yet unsub-stantiated) that the level of residual monomerin the processed dentures is less than with con-ventional methods of processing.
Following deflasking, and preliminaryrefinement of any flashes on the dentures, thedentures and their bases are re-articulated andthe occlusion scrutinised to see that:
• The incisal pin is still on the table;• Balanced occlusion is still present in RCP;• Balanced articulation, if requested is still
present on the articulator.
The dentures are then removed from the castsand the dentures trimmed, pumiced and pol-ished to a high standard (Fig. 8).
Note: The high polish should not be appliedto the denture teeth as this will create an unnat-ural appearance.
At this stage, the technician should have com-pleted his involvement in the treatment con-tract — unless problems dictate otherwise.These problems will be discussed in Part 10.
PRACTICEprosthetics
Fig. 6 Good gingival form hasbeen created here
Helpful Hints1. Establish a good working relationship
with your technician.2. Clarify your design philosophies of
casts, special trays, etc.3. Take time to detail the prescription for
each denture — it ensures that thedetail required may be confirmed.
4. Encourage the delivery of trial dentureson articulators — this encouragesattention to detail for aesthetic andfunctional aspects.
1 Guides to Standards in ProstheticDentistry. In A Ogden ed Guidelinesin Prosthetic and Implant Dentistry.London: Quintessence Publishing CoLtd, pp5-16.
Fig. 7 Poor gingival form andcareless wax control hasresulted in a less than aestheticresult
Fig. 8 Well processedand polishedcomplete dentures

128 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 3, AUGUST 12 2000
PRACTICEprosthetics
Identification of completedenture problems: a summaryJ. F. McCord,1 and A. A. Grant,2
There is, inevitably, the potential for problemsto arise subsequent to the insertion of com-
plete dentures. These problems may be transientand may be essentially disregarded by the patientor they may be serious enough to result in thepatient being unable to tolerate the dentures.
Factors causing problems may be grouped,essentially into four causes.
• Adverse intra-oral anatomical factors egatrophic mucosa.
• Clinical factors eg poor denture stability.• Technical factors eg failure to preserve the
10
Symptoms/clinical findings
Related to impression surfaceDiscrete painful areas
Pain on insertion and removal, possibly inflamed mucosa on side(s) of ridges
Areas painful to pressure
Over-extension of lingual flange. Painful mylohyoid ridge; denture lifts on tongue protrusion; painful to swallow
Generalised pain over denture-supporting area
Lack of relief for frena or muscle attachments; pinching of tissue between denture base and retromolar pad or tuberosity. Sore throat, difficulty in swallowing
Cause
Pearls or sharp ridges of acrylic on the fitting surface arising from deficiency in laboratory finishing
Denture not relieved in region of undercuts
Pressure areas resulting eg from faultyimpressions, damage to working cast, warpage of denture base. Consider also residual pathology (eg retained root), lack of relief for active frena, non-displaceable mucosa over bony prominence (eg torus)
Over-extended lower impression: instructions to laboratory not clear or non-existent
Under-extended denture base - may be the result of over-adjustment to the periphery, or impression surface. Check for adequacy of FWS
Peripheral over-extension resulting from impression stage and/or design error. Palatal soreness as post dam too deep
Treatment
Locate with finger, or snagging dry cotton wool fibres. Use disclosing material to assist locality toease denture
Use disclosing material to adjust in region of’wipe off’. Exercise care as excessive removal may reduce retention. Also clinician should only insert denture and then remove it - the patient should not occlude as this may confuse an occlusal fault with support problems
Use disclosing material to accurately locate area to be relieved. If severe, remake may be required. Consider removal of root
Determine position and extent of over-extension using disclosing material and relieve accordingly
Extend denture to optimal available denture support area. If insufficient FWS, remake may be required
Relieve with aid of disclosing material. Care with adjustment of post dam - removal of existing seal and its replacement in greenstick prior to permanent addition may be required
Table 1 List of factors resulting in discomfort related to the impression surface of dentures
In this section, guidelines to the diagnosis ofcomplete denture problems are presented intabular form. Suggestions to the managementof these problems are listed.
In this part, we will discuss:• Factors resulting in
discomfort associatedwith dentures
• Factors resulting in looseness of the dentures
• Factors associated withproblems of adaptation
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 189: 128–134

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 3, AUGUST 12 2000 129
PRACTICEprosthetics
peripheral roll on a master cast.• Patient adaptional factors.
By far the most critical factors are the patientadaptional factors. Many patients with positivestereotypes may overcome errors of prescrip-tion. Some patients, however, are unable toadapt physically and/or psychologically to den-tures that satisfy clinical and technical prostho-dontic norms. Clearly it would be in the bestinterests of the clinician and the patient to deter-mine this at the assessment stage, and wasreferred to in Part 2.
The prescribing clinician is responsible forplanning complete dentures after diagnosingpotential problems; be they anatomical, physiological, pathological or emotional.
Once a denture-wearing problem becomesapparent, it is important that it is addressed in
a logical and systematic way. That is to say, anadequate history of the problem must beobtained and a careful examination of themouth carried out so that an accurate diagno-sis can be made, and an appropriate treatmentplan devised.
Without doubt listening to the patient (astheir difficulties are described) is the mostimportant first step in the process, and itsimportance cannot be overemphasised.
Because of the plethora of potential com-plete denture problems, this section is largelyconfined to those that are most commonlyencountered at the time of insertion ofreplacement dentures or during reviewappointments in the days and weeks afterinsertion. For a comprehensive overview ofthe diagnosis and management of completedenture problems, readers are referred to
Cause
Anterior prematurity or posterior prematurity, incisal locking, lack of balanced articulation
If no over-extension present, look for protrusive slide from RCP to ICP
If no impression surface defect, may be lack of incisal overjet causing incisal locking
Vertical dimension of occlusion more than patient can tolerate
For cheeks - likely that functional width of sulcus was not restored. For lips - poor lip support/inadequate anterior horizontal overlap
Lack of lingual overjet - teeth generally placed lingual to lower ridge
Flange on buccal aspect of tuberosity too thick and constraining coronoid process
Treatment
Determine where occlusal prematurities exist. Adjust occlusion by selective grinding. If severe error remount using facebow and new interocclusal records
Mark deflecting inclines of posterior teeth with thin articulating paper. If slide exceeds half a cusp width, re-register and reset
Reduce incisal vertical overlap. If appearance compromised, resetting the incisors may be required
If excess less than 1.5 mm, grind to provide FWS. If greater than 1.5 mm, re-register to reset dentures at new OVD
For cheek biting, restore functional width of sulcus and/or reset. For lips, grind lower incisors to provide a more appropriate incisal guidance angle
Remove lower lingual cusps, or reset teeth
Use disclosing material to accurately define area involved, relieve and repolish
Table 2 List of factors resulting in discomfort - relating to occlusal and polished surfaces of dentures
Related to occlusal surfacesPain on eating in presence of occlusal imbalance (no support problems)
Pain lingual to lower anterior ridge
Pain and/or inflammation on labial aspect of lower ridge
Pain about periphery of dentures possibly accompanied by pain in masseter and posterior temporalis muscles (classically pain increases as the day progresses)
Cheek and or lip biting
Tongue biting
Related to polished surfacesPain at posterior aspect of upper denture on opening
Symptoms/clinical findings

130 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 3, AUGUST 12 2000
PRACTICEprosthetics
standard prosthodontic texts.Problems reported by patients shortly after
provision of replacement dentures include dis-comfort, looseness or general problems in relation to adaptation. Some of these prob-lems/difficulties may have a very large numberof possible causes, and, indeed, can be multi-factorial in origin. For simplicity the problemswill be discussed in the order they tend tooccur most frequently.
In the following tables, a list of causes andsuitable forms of treatment to address the prob-lems are summarised.
Discomfort associated with denturesMany patients experience some discomfort fora period of up to a few days following receipt ofnew or replacement dentures. The great major-ity of patients achieve comfortable co-exis-tence with their appliances following a shortperiod of adjustment to the new conditions.This can be greatly assisted by a careful,detailed explanation of any difficulties that theoperator might anticipate.
For some, however, especially where poten-tial problems were not identified at examina-tion or at the time of insertion, the consequent
Cause
Burning mouth syndrome often seen in middle-aged or elderly females. Denture faults must be excluded, also general organic and pyschogenic factors
Vitamin B12/folate deficiency
Xerostomia, commonly side effect of prescribed drugs
May have neurological or psychological aspects. Possibly drug related
Herpes simplex or Herpes zoster virus. History and distribution of lesions to confirm
TMJ pain dysfunction syndrome may be related to rapid change on OVD (either gross increase or decrease) on production of new denture. May have psychological aspects, occasionally part of general joint disease
Rare symptoms may relate to higher residual monomer content of acrylic
Denture-related stomatitis. Often has a frictional element due to ill-fitting denture plus opportunistic candidal infection. Occasionally related to iron or folate deficiency
Treatment
Correction of any denture faults, may require multivitamin/nutrition advice and treatment. Possibly antidepressant therapy. Refer to Consultant in Oral Medicine
Refer for medical treatment
Where some saliva flow is present, sugar-free citrus lozenges may help. Where there is an obvious paucity of saliva, artificial saliva may be considered
Difficult to manage. Treatment may be required to include occlusal adjustment and/or occlusal pivots
Dentures merely coincidental to the condition. May be useful to suggest preventive remedy (eg acyclovir) for some sufferers
If denture faults present, careful correction required with special care to registration andvertical dimension
If excess residual monomer detected, rebase denture using controlled heat cure cycle. May need to consider remaking denture using polycarbonate resin
Best to leave denture out until condition clears,then remake. If not possible, correct denture faults, eg using occlusal pivots, regularly supervised and replaced tissue conditioners prior to remake. If angular cheilitis present, combinations of antifungal and antibacterial agents (eg miconazole) useful
Table 3 List of factors resulting in discomfort - factors with possible systemic associations. Some of these
Burning sensation over upper denture supporting tissues, but may involve other intra-oral tissues, eg tongue.
Beefy red tongue, possibly glossodynia
Frictional lesions related to dentures, mucosa may adhere to probing finger, may be complaint of dry mouth
Tongue thrusting. Empty mouth ’chewing’. Often seen in elderly patients
Presence of herpetiform ulcers in mouth
Painful ’click’ related to TMJ on opening and/or closing mouth and/or tenderness of muscles of mastication
Patient complains of allergy to denture material
Painless erythema of mucosa related to support of (usually) upper denture, may be accompanied by angular cheilitis
Symptoms/clinical findings
conditions may occur several months post insertion

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 3, AUGUST 12 2000 131
PRACTICEprosthetics
discomfort can be prolonged.In addition, discomfort may arise some time
after apparently successful prosthodontic pro-vision as a result of intra-oral or systemicchanges or of denture wear or damage. Discomfort is most frequently — but notexclusively — associated with the lower den-ture supporting area.
The Tables (Tables 1, 2 and 3) summarisecommonly experienced sources of discom-fort, and means of addressing the causative factors.
Looseness of dentures Looseness of dentures (Tables 4, 5 and 6) ismore commonly associated with the lower den-ture, and may be referred to by patients as theirdenture ‘rocking’, ‘falling’ (complete upper) or‘rising’ (complete lower), ‘shifting’ or some-times that they ‘feel too big’.
In simple terms, retention and stability ofcomplete dentures may be likened to a simplebalance ie on one side retaining forces and onthe other displacing forces. If the latter exceedthe former, instability/looseness will arise. It
Cause
Border under-extension in depth
Border under-extension in width. Often a particular problem in disto-buccal aspects of upper periphery which may be displaced by buccinator on mouth opening.
Posterior border of upper denture
Consequence of ageing process; scleroderma, submucous fibrous
Deficient impression. Damaged cast. Warped denture. Over-adjustment of impression surface. Residual ridge resorption.Undercut ridge. Excessive relief chamber. Change in fluid content of supporting tissues
Medication by many commonly prescribed drugs, irridation of head and neck region, salivary gland disease
Basic shape of denture incorrect,lower molars too lingual; occlusal plane too high: upper molars buccal to ridge and buccal flange not wide enough to accommodate this; lingual flange of lower convex. Patient of advanced biological age, infirm
Treatment
Add softened tracing compound to relevant border, mould digitally and by functional movements by patient. Replace compound with acrylic resin. As a temporary measure a chairside reline material may be used as described above
Check border is correctly sited on fixed tissue at junction with mobile tissue of soft palate. Trace thin string of softened tracing compound along impression surface of posterior border and seat denture firmlyin mouth. Replace compound with acrylic resin. For temporary solution, use butymethacrylate resin as above
Mould denture borders incrementally using softened tracing-compound as functional movements are performed - aim to slightly under-extend depth and width of denture periphery. Repeated treatment may be required as inelasticity progresses
Reline if design parameters of denture satisfactory, otherwise remake as required. Ensure that areas of heavy contact between denture andtissues are relieved prior to impression making. Where change in tissue fluid distribution is suspected check medication (eg diuretics) posture (eg heart failure) lack of recovery of tissues from effects of old denture prior to working impressions being obtained. Stabilise fluid content of tissues and use minimal pressure impression method
Design dentures to maximise retention and minimise displacing forces. Prescribe artificial saliva where appropriate
Correct design faults by, eg removal of lingual cusps of posterior teeth.Flatten polished lingual surface of lower from occlusal surface to periphery, fill sulci to optimal width. May require remake to optimal design. Use information from successful previous denture if available. Denture adhesives may be deemed to be necessary
Table 4 List of factors resulting in looseness of dentures - arising from decreased retention forces
Lack of peripheral seal
Inelasticity of cheek tissues
Air beneath impression surface. Denture may rock under finger pressure. May see gap between periphery of flange and ridge. Occlusal error subsequent to warpage
Xerostomia Reduces ability to form a suitable seal
Neuromuscular control Essential for successful denture wearing: speech and eating difficulties occur
Symptoms/clinical findings

132 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 3, AUGUST 12 2000
PRACTICEprosthetics
must be stressed, however, that the fulcrum isthe patient, or rather the patient’s ability toadapt to dentures — this is less easy to antici-pate. This is illustrated in Figure 1, which is aline drawing of factors influencing completedenture stability.
Problems relating to an inability to adaptto denturesThere are a variety of symptoms which may befunctionally-related (ie eating associated prob-
Cause
If buccal to tuberosities, denture displaces on mouth opening, or cheek soreness occurs. Thickened lingual flange enables tongue to lift denture; thick upper and lower labial flanges may produce displacement during muscle activity
Design error
Poor/inappropriate impression technique especially in posterior lingual pouch area
Molars on lower denture lingual to ridge, optimum triangular shape of dentures absent
Posterior occlusal table too broad, causing tongue trapping
Thick lingual flanges encroaching on tongue space, causing lifting. Excess lip pressure to lower anterior aspect - teeth anterior to ridge, thick peripheryExcess pressure from upper lip to upper denture arising from teeth too labially sited to acute naso-labial angle; or failure to adequately seat denture during relining impression procedure
Treatment
Slightly under-extend denture flangeand accurately mould softened tracing compound. Check borders of record rims and trial dentures at the appropriate stages. Deep post dam to be cautiously reduced and denture worn sparingly until inflammation clears
Reduce over-extension. Use disclosing material to determine what is excessive
Reline if all other design parameters satisfactory, otherwise remake. Ensure denture is removed from mouth 90 mins prior to impression
Remove lingual cusps and lingual surface from relevant area, repolish.If triangular form not restored, resetteeth or remake denturesNarrow posterior teeth and/or remove most distal teeth from dentures. Reshape lingual polished surfaceThin lower labial flange, ensure optimal extension to retromolar pads to resist displacement, reset anterior teeth if necessaryUsually requires remaking denture
Table 5 List of factors resulting in looseness of dentures: arising from increased displacing forces
Denture bordersOver-extension in depthSlow rise of lower denture when mouth half open, line of inflammation at reflection of sulcal tissues; ulceration in sulcal region. Deep post dam on upper base may cause pain, ulceration
Overextension in widthCheeks appear plumped out. In lower, the buccal flange may be palpated lateral to external oblique ridge
Poor fit to supporting tissueRecoil of displaced tissue lifts denture
Denture not in optimal space
Symptoms/clinical findings
Retaining forces Displacing forces
Patient’s ability to controldentures can increase apexof fulcrum and stability
Fig. 1 Factors influencing complete denture stability

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 3, AUGUST 12 2000 133
PRACTICEprosthetics
lems, speech etc), psychologically-related ormay relate to patience. Clearly there is a need todiagnose the former at the planning stage oftreatment and to avoid the latter by virture of trial denture visits which focus on the functional and aesthetic components of the compete dentures.
Some of the psychologically-related prob-lems may be recognised at an early stage buteven if psychological assessments are taken, notall are infallible.
A brief list of factors affecting adaptation todentures including their causes and modes oftreament are listed in Table 7.
SummaryThis chapter has attempted to summarise in atabular form a list of factors that are commonlyfound at recall visits. The tables themselves are self-explanatory and serve as a ‘useful tip’ list.
For more detailed lists, readers are referred tostandard prosthodontic text.
Cause
Uneven tooth contact causingttilting of dentures and prevents even seating of loosened appliances
ICP and RCP not coincident - disrupts border seal and prevents accurate reseating
Lack of freedom in ICP(occlusal-locking) dentures will shift on supporting tissues for those patients with poor control of mandibular movements
Excessive vertical overlap ofanterior teeth. Lack of balance and anterior tooth contact may cause tilting, soreness in lower ridgeLast mandibular molars placed too far posteriorly and lie over retromolar pad or ascending part of ramus. Occlusal contact on this ’inclined plane’ causes denture to slip forwardOcclusal plane/s not orientated appropriately and masticatory forces tend to move dentures over supporting tissues
Masticatory forces tend to cause denture to sink into and tilt towards supportingtissues
Denture rocks over prominence which may be covered with inflamed tissue
Does not adapt to impression surface of denture reducing support and retention factors
Use of excessive amounts of fixative, or self-applied reline material, or even cotton wool, to attempt to relieve contact with supporting tissues
Treatment
Adjust occlusion until even initial contact in RCP obtained. If gaps between teeth exceeds 1.5 mm reset teeth or remakedentures. For gaps less than 1.5 mm it may still be necessary, in the interest of accurate diagnosis, to remount the dentures, as a patient’s mouth may be too tender to permit chairside adjustment.Adjust occlusion for coincident ICP/RCP contact. If error is greater than half widthof cusp, all teeth on at least one denture need resetting.Remount dentures on adjustable articulator and adjust area of occlusal contact. Allow 1.5 mm of anterior movement from RCP. May use cuspless teeth where appropriate
Reduce height of lower anteriors. Aesthetic problems may necessitate resetting of teeth
Remove most posterior teeth from denture
Usually requires teeth to be reset or dentures to be remade
Reline after removal of acrylic from impression surface until no contact with displaceable tissue, provide many vent holes, low viscosity impression material, maximise posterior border seal
Remove acrylic from impression surface where disclosing material shows excessive loading of supporting tissues. Do not create excessive relief or loss of retention may result
Reline dentures to obtain optimal border extensions in depth and width, use low viscosity impression material
Eliminate the cause of pain
Table 6 List of factors resulting in looseness of dentures - arising from increased displacing forces - occlusal and anatomical factors
Occlusal errors
Ulceration labial to lower ridge
Fibrous displaceable ridge
Bony prominence covered by thin mucosa (eg tori)
Non-resilient soft tissue
Pain avoidance mechanisms
Symptoms/ clinical findings

134 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 3, AUGUST 12 2000
PRACTICEprosthetics
Cause
May be lack of skill with new dentures, excessive OVD, occlusal interference, loose dentures, or poor perception of patient to denture wearing
Unstable dentures. Check that retentive forces are maximised and displacing forces minimised and all available support has been used
Broad posterior occlusal surfaces which replaced narrow teeth on previous denture. Non anatomical type teeth used where cusped teeth previously used
Lack of OVD, so that mandibular elevator muscles cannot work efficiently
Excessive OVD
Cause may not be obvious. May be unfamiliarity - check that problem not present with old dentures
May be loose dentures, thick distal border of upper denture: lingual placement of upper posterior teeth or low occlusal plane causing contact with dorsal aspect of tongue
Patient failed to comment at trial stage, or has subsequently been swayed by family or friends. Perhaps the change from the old denture to the replacement denture is too sudden/severe
Level of occlusal plane unacceptable, teeth placed on upper anterior ridge and no/poor lip support
Labial fullness and anterior tooth position may be inaccurate. OVD may be inadequate
Patient’s skin colour not taken into account in determining colour of base material
Treatment
Where unfamiliarity present, reassurance and persistence recommended. Address specific faults or remake as required
Construct dentures to maximise retention and minimise displacing forces
Where non-anatomical teeth used, careful explanation of rationale is required, may be possible to reshape teeth. Routine use of narrow tooth moulds recommended.
May increase up to 1.5 mm by relining but if deficiency is greater, remake denture
Can remove up to 1.5 mm from occlusal plane by grinding, but if more is required, remake dentures
Check for vertical dimension accuracy, and that vertical incisor overlap not excessive. Palatal contour should not allow excessive tongue contact or air leakage -assess using disclosing paste over denture palate while sound is made. NB It is recommended that the patient’s speech is assessed at trial insertion visit
Construct dentures to maximise retention and minimise displacing forces. Use ’condition’ appliance eg fully extended base for home use. Psychological assessment if indicated
Accurate assessment of patient’s aesthetic requirements. Ample time for patient comments at trial stage. Use any available evidence to assist - photographs, previous dentures. Consider template prosthesis
Accurate prescription to laboratory via optimally adjusted occlusal rim
Adjust tooth position as appropriate.If OVD problem, re-register jaw relations
Remake using suitable base material
Table 7 List of denture problems associated with problems of adaptation
Noise on eating/speakingMay be apparent on first insertionor may appear as resorption causes dentures to loosen
Eating difficultiesDentures move over supporting tissues
’Blunt teeth’
’Jaws close too far’
’Cannot open mouth wide enoughfor food’. May be speech problems and facial pain especially over masseter region
Speech problemsUncommon, but presence is of great concern to patient. May affect sibilant (eg s), bilabial (eg p,b), labiodental (eg f.v)
GaggingMay be volunteered by patient prior to treatment, or apparent at commencement of treatment or on insertion of denture
AppearanceComplaints may arise from patient or relatives. Common complaints include: shade of teeth too light ordark; mould too big/small; arrangement too even or irregular or lacking diastema
Too much visibility of teeth
Creases at corners of mouth
Colour of denture base material ’unnatural’
Symptoms/clinical findings

186 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000
PRACTICEprosthetics
Specific clinical problem areasJ. F. McCord,1 and A. A. Grant,2
In this section, specific clinical problem areas,which involve aspects over and above con-
ventional complete dentures, will be discussed.The six areas to be discussed are:
• Conventional immediate complete dentures• Copy (template) dentures• Relines and rebases• Overdentures (complete) • Implant-retained/supported complete
dentures• Combination syndrome.
In addition to having to satisfy prosthodonticnorms for conventional complete dentures,all six areas require distinct planning proce-dures, which relate to both technical and clin-ical procedures, yet they tend to sharecommon problems, particularly with regardsto retention and stability of complete den-tures. The six categories are summarised andreaders are referred to standard textbooks formore comprehensive descriptions.
Conventional immediate completedenturesAccording to Nimmo and Winkler, an immedi-ate denture may be defined as ‘a complete orremovable partial denture constructed forinsertion immediately following the removal ofnatural teeth’.1 Such dentures were once pro-vided on a regular basis in dental practice, espe-cially in the post World War II era. For a varietyof reasons, one of which is improved dentalhealth education, this treatment regime is nowless regularly provided.
In the interests of simplicity, and to avoidrepetition for the remainder of this chapter, theterm immediate denture will be intended tomean an immediate complete denture.
In theory, immediate dentures may bedefined as interim or conventional. In the for-mer, an existing (partial) prosthesis is con-verted into a complete denture. In the latter,conventional wisdom recommends that pos-terior teeth distal to the first premolar teethare extracted, the ridges allowed to heal for2–3 months and the anterior teeth subse-quently extracted and a conventional imme-diate denture inserted.
Table 1 lists the potential categorisation ofimmediate dentures and also of overdentures.There are obvious similarities between the two
from planning and technological points of viewbut the latter offers greater patient benefits(vide infra).
Transitional immediate complete denturesIn this category, a patient who is currentlywearing a satisfactory removable partial den-ture is rendered edentulous and the teeth tobe replaced are added to the denture. Addi-tional base material, to effect maximal cover-age of the denture-bearing area, is alsoprovided. This is the philosophy behindtraining dentures and is the rationale behindthe prescription of, eg Kennedy I type den-tures in older patients for whom the progno-sis of the remaining teeth is poor. After aperiod of time to enable, it is hoped, neuro-muscular control of the training denture, animpression is taken with the training denturein situ. The resultant master cast is thenmodified by removal of the remaining teeth(see conventional immediate complete den-tures) and the transitional dentureprocessed. Figures 1–3 show the clinicalstages in the transformation of the partialdenture to the transitional complete imme-diate denture.
Conventional immediate complete denturesAlthough a range of clinical scenarios are possi-ble, the most common clinical situation, and theone to be described is where the posterior teethhave been extracted and the anterior teethremain. There is much merit in retaining, if pos-sible, the four first premolar teeth to provide areasonable and unambiguous occlusal stop inretruded contact position (RCP), and this pro-vides an acceptable assessment of occlusal vertical dimension (OVD). The techniquedescribed here may be used if the premolar teethare present or not.
Stage 1The teeth to be removed are assessed clinicallyand radiographically, and an assessment of thelevels of the alveolar bone made. Primaryimpressions are made using, eg a combinationof impression compound and irreversiblehydrocolloid (Fig. 4).
NB Although trays do exist for partially-den-tate patients, we recommend, nevertheless, thecombination of a viscous material (for the sad-
11In this final article ofthe series, the clinicaland technical aspectsof a range of similarforms of immediateprosthesis arediscussed. Similarly,copy denture andreline/rebaseprocedures aredetailed.
In this part, we will discuss:• Conventional overden-
tures • Implant supported
complete dentures• Copy dentures• Relines and rebases
and construction andcombination syndrome
1*Head of the Unit of Prosthodontics,2Emeritus Professor of RestorativeDentistry, University Dental Hospital ofManchester, Higher Cambridge Street, Manchester M15 6FH*Correspondence to: Prof. J. F. McCordemail: [email protected] PAPER
© British Dental Journal2000; 189: 186–193

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000 187
PRACTICEprosthetics
dle areas) and a less viscous impression mater-ial for the areas where teeth are retained, as thephilosophies for primary impressions outlinedin Part 4 apply here.
It is also worth mentioning here thatpatients ought to be informed of the fact thatimmediate dentures represent a useful solu-tion to the advent of edentulousness. Thesedentures may require several chairside relines
during the first 3 months after insertion ofthe immediate denture(s) and will require tobe replaced some time after that (although,some patients have coped with immediatedentures for many years). The medico-legalimplications of this important piece of infor-mation should not be overlooked and Figure5 shows a patient information leaflet regard-ing complete dentures.
Fig. 1 Occlusal view of remaining teeth and present lowerpartial denture
Fig. 2 Occlusal view of remaining teeth and edentulous saddles
Fig. 3 Pick up impression showing current denture andremaining teeth. It is a simple matter for the technician to addthe remaining teeth to the present denture
Fig. 4 Stock tray modified with impression compound in thesaddle area and overall irreversible hydrocolloid impressionmaterial
Type of Transitional
Conventional • Previous partial denture used and immediate converted to a complete denture. • After an appropriate period, a
conventional replacement (definitive) denture is made.
Overdenture • Previous partial denture used and converted to a complete
denture. • After an appropriate period, a definitive replacement overdenture is made.
Immediate
• Posterior teeth removed, and after a set time, the remaining teeth are extracted and the complete immediate denture is inserted.• After an appropriate period, a conventional replacement (definitive) denture is made.
• Posterior teeth removed, and after a set time, the teeth selected as overdenture abutments are prepared to receive the overdenture and the complete immediate denture is inserted.• After an appropriate period, a definitive replacement overdenture is made
Definitive
• Not an accurate description here, as, by definition, conventional immediate dentures cease to be so on insertion, owing to the nature of extractions and subsequent resorptive processes.
• In this category, the dentures receive some or most of their support and perhaps retention and some stability via either i. abutment roots +/– precision attachments ii. implants + precision attachments
Table 1 Theoretical categories of immediate dentures and overdentures
denture

188 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000
PRACTICEprosthetics
Stage 2A definitive impression is made. It should beemphasised that time should be taken to ensurethat the peripheries are appropriately extended.Patients who have never worn complete den-tures previously will have to endure enoughadaptational problems without having to copewith instability as a consequence of over-exten-sion. Again, the clinician should specify to thetechnician the amount of spacing required,according to the type of impression material tobe used.
Stage 3Registration of intermaxillary relations. Aswith conventional complete dentures, vertical,antero-posterior and coronal relations need tobe recorded and record rims (Fig. 6) will help
the clinician to record these relations. It may bepossible to use the remaining anterior teeth as ameans of selecting the mould and shade of theteeth for the immediate denture; in some cases,the remaining teeth may not lend themselves tocopying and a conventional method may beused to assess tooth selection (vide supra).
Stage 4 The three-dimensional inter-maxillary rela-tions are confirmed at the trial denture stage asis the shade and form of the teeth. The informa-tion above, plus details of pocket depth enablethe technician to determine where to positionthe necks of the replacement teeth. Equally, theclinician should decide whether the immediatedenture has no flange (open-faced) a shortflange (ridge-lapped) or whether a full flangecan be accommodated. The presence of largeundercuts may rule out the latter (Figs 7 and 8).In such cases, and where there is a need toattempt to restore a semblance of the interden-tal papillae, the flange may be taken to the bul-bosity of the alveolar undercut using a shortflange. Readers are referred to textbooks ofprosthodontics for details of the technical pro-cedures.
The dentures are then completed ready forinsertion following an effective cross-infectionregime prior to the required clinical proce-dures.
After the insertion of the immediate den-tures, the patient is given instructions on thecare of their dentures (see Fig. 5) and reviewedafter 24 hours and then weekly, according topatient need until the clinician prescribes areline. This may be a conventional type of relineor a ‘chairside’ reline using an auto-curingmaterial.
Copy (template) denturesAlthough impression techniques relating to thisform of treatment were outlined in Part 4, wefeel that it is appropriate to elaborate on thephilosophy of template dentures. Over 30 yearsago, Brill recognised that some patients, partic-ularly elderly patients, had problems adaptingto the (new/altered) form of replacement den-tures.3 He argued that retention of the form ofthe polished surfaces of the dentures and relin-ing/rebasing of the impression surfaces (den-ture bases) would enable the dentist to providereplacement dentures to which (older) patientsmight adapt more easily. This philosophy led tothe birth of the ‘copy’ denture technique. If allsurfaces of the complete denture were beingreplicated, this would indeed be a ‘copy’ den-ture. If only the polished surface is being repli-cated, however, then we would argue that thetechnique should be considered a templatetechnique, as the denture bases and the occlusalsurfaces are altered, only the polished surface is‘copied’. A variety of techniques was referred to
Fig. 5 Patient information leafleton immediate dentures
A great deal of care and skill has been used in the production of the denture(s) that you have received. To enable you to learn to use the denture(s) as quickly as possible and get the greatest benefit from them, you are asked to note the following advice.1. Do not remove the dentures yourself. Your dentist will remove them at your next appointment.2. If pain occurs relief may be obtained by taking two paracetamol tablets at not less than four-hourly intervals.3. Eat only soft foods at this stage and rinse the mouth lightly after meals.
Next appointmentThis appointment will normally be arranged about 24 hours following the extractions. Your dentures will be removed and any treatment necessary to improve your comfort will be carried out. You will be shown how to remove and replace the denturesand your next follow-up appointment will be arranged.
Home care 1. Eating may be difficult at first; cut your food into small pieces and take your time chewing. Avoid tough and sticky foods over the learning period.2. Remove your dentures and clean them after each meal. A soft brush with soap and cold water are satisfactory for cleaning. Alternatively, a proprietary denture cleaner may be used following the manufacturers' instructions. Rinse the mouth thoroughly with warm water before replacing the dentures.3. Wear the dentures night and day, removing them only for cleaning. (You will be advised when you can begin to leave the dentures out at night).4. Pain and soreness sometimes occur with new dentures and adjustment may be required. Arrange an appointment to see your dentist as soon as possible. Do not attempt to adjust the dentures yourself.5. We are obliged to inform you that, following tooth extraction, the bone of the jaws surrounding these teeth is resorbed (shrinks). In consequence, your dentures will become progressively looser. As a result your dentures will need to be relined and, usually after 6 months replaced by new dentures.
Figure 5 Instructions to patients receiving immediate dentures
Fig. 6 Record rims onmaster casts to recordinter-maxillary relations

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000 189
PRACTICEprosthetics
in Part 4, and practitioners should use the onethat works best for them.
There is no doubt that the template tech-nique is a sensible and effective treatment strat-egy for older patients, or those patients whobecause of neurological impairment areunlikely to develop good muscular adaptationto conventional complete dentures.
The clinical stages for template dentures are;
• At the first visit, after appropriate historyrecording and diagnosis, prior to templat-ing, primary impressions may be made. Aswas described in Part 4, the existing denturesare replicated. Given the stability ofpolyvinylsiloxane putty systems, we wouldrecommend the techniques whereby this isused, especially for practitioners who do nothave casting services on the premises.
• At a second clinical visit, impressions aremade within the replicated dentures; thisserves effectively as a relining/rebasing toimprove the fit of the denture base to thedenture-bearing tissues. The occlusal sur-faces are then modified to a new OVD andRCP if desired.
• At the third visit, the wax trial denture isassessed and if the dentures are perceived tobe satisfactory by both the clinician and thepatient, the dentures are sent to the labora-tory to be processed conventionally.
This technique has been shown to result insuccessful resolution for those clinical cases(vide supra) in which conventional prostho-dontics might not have worked. Although theconcept of template dentures is philosophi-cally simple, it nevertheless requires that theclinician exercises appropriate clinical skilland judgement.
Three areas of caution, in particular are wor-thy of consideration.
• Ensure, in the older patient especially, thatthe OVD is carefully selected. This problemhas already been referred to in Part 6.
• None of the currently described techniquesadequately caters for problems of support(eg displaceable upper ridge) and modifica-tions of impression techniques may be nec-essary to overcome these problems.
• This technique requires that the technicalsupport is proficient. If the replication of thedenture form is not thorough, the outcomeof the treatment may be jeopardised.
Relines and rebasesAlthough one technique for a ‘reline’ impres-sion was described in Part 4, this merelydescribes how to do it. We feel that thisapproach, while appropriate to a chapterdescribing impression techniques, requireselaboration, hence we have included somecomments here on the basic principles of
relining/rebasing, as we feel that this proce-dure is often mistakenly assumed to be a‘simple’ procedure that tends to be per-formed poorly.
Residual ridge resorption under denturebases is an inevitable occurrence and allpatients ought to be informed of this. As wasdescribed earlier, this resorption may be pre-
dicted to occur rapidly over the first 3 monthspost-extraction then slow down, althoughthere will inevitably be great variation amongpatients. Dentists, we feel, should be mindful ofthe need to maintain the adaptation of the den-ture bases to the selected areas of the denture-bearing area.
In order to compensate for residual ridgeresorption, the impression surfaces of the den-tures may on occasion be modified; the twoprocesses whereby this may be carried out aretermed relining and rebasing.
According to the Glossary of ProsthodonticTerms, relining describes the procedures usedto resurface the tissue (impression) surface ofthe denture with new base material,2 thus pro-ducing an accurate adaptation to the denturefoundation area.
In the same document, a rebase is describedas the laboratory process of replacing the entiredenture base of an existing prosthesis.
In essence, the process of relining is carriedout on mandibular complete dentures and theprocess of rebasing is carried out on maxillarycomplete dentures, although many practi-tioners use the term reline to mean both.
The indications and contra-indications forrelining/rebasing are listed in Table 2.
Further factors to be taken into considera-tions for relining and rebasing are:
• The OVD should be acceptable (where min-imal freeway space (FWS) is present, thiscould induce further denture-wearing prob-lems).
• There should be occlusal balance in RCP, orshould be easily achievable if not present.
• The dentures are adequately extended, ormay be easily rendered so via a chairsidereline material or tracing compound, prior
Fig. 7 This immediate denture hasbeen designed with afull labial flange

190 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000
PRACTICEprosthetics
to the recording of the impression — there islittle point in relining a denture that does notsatisfy prosthodontic norms.
The clinical and technical procedures forreplacement of the denture base of completedentures are relatively complicated and requireclinical competence — if denture bases areseverely under-extended, unattainable bal-anced occlusion exists in RCP and a gross lossin OVD has occurred, practitioners are advisedto prescribe replacement dentures.
OverdenturesAccording to Basker et al., overdentures are pros-theses constructed to gain support and retentionfrom retained roots (or dental implants).4 In thissection, the term overdentures is intended tomean complete denture overdentures.
In essence, the retention of roots tosupport/retain an overdenture has been shownto reduce residual ridge resorption, improvestability and to retain proprioception.3 For amore detailed description of overdentures,readers are recommended to standard text-books on the subject.4,5
As is described in Table 1, overdentures maybe classified as being one of three classes, transi-tional, immediate and definitive.
Transitional overdenturesAs with the immediate denture category, a par-tial denture worn by the patient is modified byaddition of teeth; the planned retention of twoor more roots facilitates adaptation to completedentures, in addition to reducing ridge resorp-tion. In all other respects, the clinical and labo-ratory stages are similar to those of transitionalimmediate dentures. In this technique, theteeth are reduced in height (to the level of thegingival margins) at the time of the insertion ofthe denture. To guard against rocking of thedenture on insertion, the clinician is advised toreduce the teeth on the master cast above thegingival margins. This will ensure that therewill be a small space between the overdentureabutment teeth and the denture; this space maybe filled in by a chairside reline material toensure stability of the transitional immediatedenture.
Immediate overdenturesThe clinical and technical stages of this type ofoverdenture are essentially similar to that ofimmediate overdentures. The clinical differ-ences are clearly that a planned number of rootsare retained and, post-decoronation, the clini-cian has to decide how best to seal-offendodontic access cavities (if endodontic pro-cedures have been carried out) or of dentinaltubules if elective endodontics has not beenperformed.
It is not established practice to place preci-sion attachments in immediate overdentures.
A second point is that, in these situations,hard tissue undercuts tend to contra-indicatefull labial flanges and most immediate overden-tures tend to have a ridge-lapped appearance(Fig. 8). In these cases, there is no real flange butthe acrylic of the denture base is extended up tothe ridge undercut. In addition to improvingthe appearance of the denture by incorporatinginterdental papillae, this technique helps masksome resultant ridge resorption.
Fig. 8 Owing to anobvious labialundercut, there hasbeen no attempt toplace a full flange andan open appearancehas been created. NB Socketing is notrecommended as itencourages aninappropriateappearance post-healing
Indications
• 3–6 months post insertion of immediate complete dentures.
• When adaptation of denture bases to the tissues of the denture-bearing areas is poor. • When, for medical or social reasons the patient is unable to attend the required number of visits for replacement dentures and no contra-indications apply. • When the patient is unable to afford replacement complete dentures and no contra-indications apply.
Contra-indications
• When an excessive amount of resorption has occurred.• When the underlying tissue is inflamed and/or hypertrophic or hyperplastic. • When the patient exhibits symptoms suggestive of TMJ problems. Accurate diagnosis and resolution of the problem are indicated first of all. • When the dentures have induced a speech problem. • When the appearance of the dentures is unsatisfactory to the patient. • When the intermaxillary relationships are unsatisfactory.
Table 2 List of indications and contraindications for relining and rebasing

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000 191
PRACTICEprosthetics
To avoid embarrassment of a social natureto the patients (and of a professional natureto clinicians) it can be reasonable practice touse denture fixative at the time of insertion ofthis overdenture type. This is especially validif the patient has never worn a denture previ-ously, as the (soft) tissues of the denture-bearing area may take some time to bedisplaced.
Definitive overdenturesAt a selected period post-extraction and de-coronation and insertion of either a transitionaloverdenture or an immediate overdenture, areplacement overdenture may be planned. Thisreplacement denture may be a straight-forwardreplacement complete denture which happensto be an overdenture; in this case, conventionaltechniques would suffice.
If, however, there is a need to improve reten-tion, the clinician may decide to use precisionattachments. The two most common precisionattachments used for overdentures are studs(Fig. 9) and bar assemblies (Fig. 10). The readeris referred to a textbook on overdentures onindications and contra-indications here, eg if abar is selected, then it tends to assume that theroots are approximately parallel.
When the clinician has determined whichtype of precision attachment is appropriate forthe patient, the treatment sequence followed isas follows:• Stage 1. Primary impressions recorded as for
the conventional denture technique. Thetechnician should be informed of the deci-sion to prescribe precision attachments andthe case planned with the laboratory beforeproceeding further.
• Stage 2. If the abutment teeth have beenendodontically-treated, then the root canalsof selected teeth (usually canine teeth) areprepared with reamers matched to impres-sion posts to give parallel-sided threadedposts. One such system is illustrated in Figure 11. Definitive impressions arerecorded, again with the same attention todetail for peripheral seal as per conventionaldentures.
• Stage 3. The appearance of the upper den-ture, intermaxillary relations and selectionof tooth moulds and shades are carried outas for conventional dentures.
• Stage 4. In addition to the trial insertion(s)for the denture(s), the clinician should verifythe accuracy of fit of the precision attach-ments. When precision attachments andtrial denture are deemed to be satisfactory,the overdentures may be processed.
• Stage 5. As the retention of teeth does signifi-cantly enhance function and retention oflower dentures particularly, extreme cautionis advised to ensure that the occlusalschemes of the dentures are in harmony with
mandibular movements, or (upper) dentureinstability may well result.
• Stage 6. As with all other denture types,review visits and recall visits are necessary.
Patients should be made aware of the need tomaintain good oral hygiene around abutments.They should also be informed that mainte-nance is required for the precision attachments;the effects of wear and tear on the precisionattachments means that tightening and/orreplacement will be inevitable at some time.
Implant-retained complete denturesAn implant is a device or substance that isplaced or implanted in the body for the purposeof restoring lost or deficient function and/or thereplacement of deficient tissue. A dentalimplant is implanted into or onto the tissues of
Fig. 10 A bar assemblyused to retain acomplete loweroverdenture
Fig. 9 Studs used to retain lowercomplete overdenture
Fig. 11 Para-post system which hasreamers, which match impressionposts

192 BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000
PRACTICEprosthetics
the jaws with the object of providing anchoragefor a fixed or removable prosthesis, or for theaugmentation or regeneration of deficient tis-sues. Clearly with such a general definition, arange of implant materials and implant typesmay be used. For the interests of this chapter, theimplant material discussed is titanium (or alloysof titanium) and the type of implant referred tois the endosseous implant. Examples showndemonstrate two types (Nobel-Biocare andFriatec) and these reflect the clinical experi-ence and preference of the authors.
Substantial data are available to indicate thevery real functional and psychological advan-tages of restoring edentulous jaws with dentalimplants,6,7 and there is no doubt that thistreatment modality is practised universally byspecialist prosthodontists and general dentalpractitioners. We would recommend that clini-
cians undertaking such treatments undergosufficient clinical training to comprehend thesurgical and prosthodontic philosophies inher-ent in well-established and creditable implantsystems.
We would further contend that the restora-tive clinician is the orchestral leader of implanttherapy as they should be involved with treat-ment planning at the onset of treatment, estab-lishing the form of the surgical template,prescribing the intermediate and definitiveprostheses and overseeing the maintenance ofthe prosthesis/es.
The prosthodontic stages inherent in implant-retained (complete) denture therapy, in additionto treatment planning stages are as follows:
• Stage 1. The clinician proceeds with the caseas for a conventional denture and, at thetrial denture stage, when satisfied with theform and function of the trial dentures,arranges the surgical stent(s) required. Onesuch stent is illustrated in Fig. 3 of Part 8.The surgeon uses this stent to help positionthe implants.
• Stage 2. Post-insertion of the implants, thepatient is advised to refrain from wearingtheir denture for 1 week. Thereafter, succes-sive resilient linings will be required toreduce trauma to the tissues overlying theimplants. Relief will also be required over thesite of the implants to reduce the potentialfor loading of the implants during thisperiod when, it is hoped, osseo-integrationis occurring.
• Stage 3. After the implants have been uncov-ered and healing caps placed on the per-mucosal abutments, impressions are taken.Figures 12 and 13 indicate two systems andtheir different (although fundamentally simi-lar) impression techniques for implant-retained complete dentures. In the particularcase shown in Figure 12, the central implantwas not utilised and subsequently covered upto allow room for the bar assembly.
In essence, the stages following this are similarto those described above for definitive overden-tures, with the exception that the abutmentsused are screwed in place.
Figure 14 is an intra-oral view of an implant-supported bar assembly in situ.
As with overdentures, the need to includemaintenance visits should always be empha-sised to the patient.
Combination syndromeReference has been made previously to the diffi-culties encountered by having to provide areplacement complete denture in one arch whilethe opposing arch contains a natural (or essen-tially natural) dentition; this challenging clinicalcombination has been termed the combinationsyndrome. Two types exist: edentulous maxilla
Fig. 13 Impression posts for a lower, implant-retained completedenture using theNobel-Biocaresystem
Fig. 12 Impressionposts for a lower,implant-retainedcomplete dentureusing the IMZ(Friatec) system
Fig. 14 Intra-oral viewof implant-supportedbar assembly

BRITISH DENTAL JOURNAL, VOLUME 189, NO. 4, AUGUST 26 2000 193
PRACTICEprosthetics
opposed by natural dentition and edentulousmandible opposed by natural dentition.
Edentulous maxilla opposed by a naturaldentition in the mandibular arch.In this situation, the displacing forces on theupper denture resulting from mandibularmovements have to be harnessed and a varietyof ways of maximising the retentive forces andreducing the displacing forces must be used.
The retaining forces are maximised by ensur-ing that a peripheral seal is present and this hasbeen described in an earlier chapter.
Displacing forces are reduced by co-ordinat-ing the maxillary teeth and maxillary plane ofocclusion to mandibular movement. These areachieved via one of the following ways:
• Using a facebow to transfer the plane of theupper arch to the condylar axis.
• Using a central-bearing screw to create anarrowhead (Gothic-arch) tracing.
• Setting the articulator condylar angles toaccord to the border tracings on the arrow-head tracing.
• Establish, carefully, at trial insertion, thatRCP is reproducible.
• That the technician ‘mills’ the occlusion tosuit the patient. This will inevitably be neces-sary, as (denture tooth) cuspal inclines willbe unlikely to equal those of the patient. Thisshould not be carried out without consider-ation of aesthetic and functional demands ofthe patient and should be carried out inadvance of the recording of definitiveimpressions of the mandibular arc.
• On occasion, the clinician may need to usethe patient to ‘mill-in’ the occlusion in thechair. A technique sometimes used by theauthors is to make a paste of carborundumpowder and toothpaste and to ask thepatient to trace out the border movementswith the denture in situ and with the teeth inocclusion.
• In our clinical experience, there hasinevitably been a need to review the patientafter 3 days and to refine the cuspal anatomyof the maxillary denture teeth.
• Clinicians should be aware of the need tomaintain and even replace dentures in theseconditions, hence patients should also be soinformed at the onset of treatment.
As with most complete denture problems,patient co-operation is essential if success is tobe achieved.
Edentulous mandible opposed by a naturaldentition in the maxillary arch.This clinical problem is even more difficult to treatthan the former and although identical techniquesare recommended in this scenario, success will bemore problematic. Even with sound prosthodon-tic impression techniques, displacing forces willinevitably overwhelm retaining forces of themandibular denture and only immense physio-logical control of the denture will create stability.In this clinical situation, implant-retained den-tures are in a class of their own as a preferred treat-ment modality.
Although other problematic clinical situationsexist, we have attempted to cover the principal situations which may be encountered in daily gen-eral dental practice and this section, in addition toPart 10 gives, it is hoped, an insight how to identifyand treat common prosthodontic problems.
Helpful Hints1. For any form of immediate denture,
always inform first-time completedenture-wearers of:a: the problems associated withmanaging complete dentures andb: the inevitable residual ridgeresorption and its sequelae.
2. Immediate complete immediatedentures or complete overdentures —the clinician should ensure that theessential principles of complete dentureprosthodontics are adhered to.
3. Where complete upper overdenturesare concerned, tissue displacement(and associated tissue fluiddisplacement) usually does not occurat the time of insertion of the dentureand a denture adhesive may berequired over the first 24–48 hours.The patient should be advised (of thispossible transient retentive aid)before the insertion-visit to avoid thepatient developing a negativestereotype towards the denturesand/or the clinician.
4. Where precision attachments areused for conventional overdenturesor implant-retained overdentures,the clinician should remember thatthey occupy space and may be bulky. The clinician is also advised to consultwith his/her technician, at thetreatment planning stage, as to thetechnical feasibility of each case.
1 Nimmo A , Winkler, S In Winkler S(ed). Essentials of Complete DentureProsthodontics (2nd. edn). St. Louis:Mosby, 1988 pp 361-374.
2 Brill N. Factors in the mechanism offull denture retention. Dent PractDent Rec 1967, 18: 9-19.
3 The Academy of Prosthodontics. TheGlossary of Prosthodontic Terms,(6th edn). J Prosthet Dent 1994; 71:41-116.
4 Basker R M, Harrison A, Ralph J P,Watson C. Overdentures in generaldental practice (3rd edn). London,BDJ pp 1-9, 1993.
5 Brewer A A, Morrow R M.Overdentures (2nd edn). St. Louis,Mosby, 1980.
6 McCord J F, Grant A A, Quayle A A.Treatment options for the edentulousmandible. Eur J Prosthodont RestDent 1992; 1: 19-23.
7 Blomberg S. In Branemark P I, ZarbG A, Carlsson G E (eds). Tissue-Integrated Prostheses, Osseo-integration in Clinical Dentistry 1985,Chicago: Quintessence PublishingCo. Chapter 9, pp165-174.
This series is available asa BDJ book — A ClinicalGuide to CompleteDenture Prosthetics byProfessor J F McCordand Dr A A Grant(ISBN 0 904 588 64 5,price £29.95) This canbe purchased fromMacmillan Direct,Brunel Road,Houndmills,Basingstoke, HantsRG21 6XSTel: 01256 302699