Embed Size (px)
DESCRIPTION
By Ms. Kostiuk from Microbiology department
Citation preview

DiphtheriaDiphtheriaTuberculosisTuberculosis

Diphtheria is acute human infectious disease caused by toxigenic Corynebacterium diphtheriae, transmitted by airborne droplets, manifesting in local fibrinous inflammation of mucous membrane of nasopharynx and trachea, and common intoxication, cardiovascular, nervous, urogenital system injury

Species of Corinebacterium Species of Corinebacterium genusgenus
C.C. diphtheriaediphtheriae C.C. xerosis, xerosis, species that normally lives in the eye, species that normally lives in the eye,
skin, and mucous membranes and is an occasional skin, and mucous membranes and is an occasional opportunist is eye and postoperative infections.opportunist is eye and postoperative infections.
C.C. pseudodiphtheriticum pseudodiphtheriticum (hofmannii)(hofmannii), , a a normal inhabitant of the human nasopharynx, can normal inhabitant of the human nasopharynx, can colonize natural and artificial heart valves. colonize natural and artificial heart valves.

Features of Corynebacterium Features of Corynebacterium diphtheriae diphtheriae
Gram-positive rods of variable sizeGram-positive rods of variable size Club-shaped/slender rod (with swell on the one end)Club-shaped/slender rod (with swell on the one end) Pleomorphic, can develop filamentous formsPleomorphic, can develop filamentous forms Nonmotile Nonmotile Arranged in palisades or in V-, X- or L-shaped formationArranged in palisades or in V-, X- or L-shaped formation Older cells are filled with volutin granules that consist of Older cells are filled with volutin granules that consist of
polyphosphate. The granules stain metachoromaticallypolyphosphate. The granules stain metachoromatically Aerobic and facultative anaerobicAerobic and facultative anaerobic Require special media for cultivation Require special media for cultivation (encriched with blood,serum or egg). Scanty (encriched with blood,serum or egg). Scanty growth in ordinary mediagrowth in ordinary media

Morphology ofMorphology of С. С.diphtheriaediphtheriae
Methylene blue stain Neisser’s stain
Metachromatically stained volutin inclusionsMetachromatically stained volutin inclusions

Cultivation of C. diphtheriaeCultivation of C. diphtheriae
Loeffler’s mediaLoeffler’s media with solidified with solidified serumserum
Blood agar Blood agar Tellurite agar.Tellurite agar. Contains a Contains a
potassium tellurite that is potassium tellurite that is reduced to elemental tellurium reduced to elemental tellurium within C.diphtheriae. The within C.diphtheriae. The typical gray-black color of the typical gray-black color of the colony is diagnostic criterion colony is diagnostic criterion

Catalase Catalase Glucose Glucose Sucrose Sucrose Maltose Maltose Nitrate Nitrate reduc-reduc-tion tion
Urease Urease Gelatin Gelatin hydrosyhydrosysis sis
++ ++ -- ++ ++ -- --
Biochemical activity of Biochemical activity of C.diphtheriaeC.diphtheriae

Biotypes of C.diphtheriaeBiotypes of C.diphtheriae
Gravis Gravis Mitis Mitis Intermedius Intermedius Belphanti Belphanti

Differentiation criterions for Differentiation criterions for C.diphtheriae biotypesC.diphtheriae biotypes
Feature Feature Gravis Gravis Mitis Mitis
Growth on solid Growth on solid media media
R colonies R colonies S coloniesS colonies
Growth in broth Growth in broth Surface pellicle and Surface pellicle and granular depositgranular deposit
Diffuse Diffuse turbidity turbidity
Fermentation of Fermentation of glycogenglycogen
Yes Yes No No
Fermentation of Fermentation of starchstarch
Yes Yes No No
Hemolysis Hemolysis No No Yes Yes
Toxigenicity Toxigenicity More strains are More strains are toxigenic toxigenic
Less strains Less strains are toxigenic are toxigenic

С.С.diphtheriae biotypes cultural diphtheriae biotypes cultural properties properties
GravisGravis forms large colonies R-form (rough surface, with uneven edge)
MitisMitis forms small colonies S-form (smooth surface, with flat edge)

Virulence factors ofVirulence factors of C. C. ddiphtheriaeiphtheriae
ExotoxinExotoxin (diphtheritoxin). It consist of 2 fragments:
• B - for binding to the target cells• A – active part that inactivates the elongation inactivates the elongation
factor in the ribosomes and thereby stops factor in the ribosomes and thereby stops protein synthesisprotein synthesis
Enzymes: catalase, dehydroginase, DNAses, neuraminidase, hyaluronidase
Cord-factor (in microcapsule) – toxic effect on mitochondria
Surface lipids – antiphagocytic factor

C. C. ddiphtheriaeiphtheriae exotoxin exotoxin
Diphtheritoxin affects the body on two levels: Local. The toxin causes inflammation, fever, sore throat,
nausea, severe swelling in the neck. It necrotizes cells in the site of bacteria attachment and
causes formation of pseudomembranepseudomembrane. This film consist of solidified fibrous exudate cells, fluid that develops in the pharynx, and bacilli.
If membrane forms into the larynx and trachea, it can cause airway abstruction (mechanical asphyxiation).
Systemic (toxemia). Toxin is carried by the blood to certain target organs, primarily the heart, nerves and kidneys.
It causes myocarditis accompanied by arrhythmias and circulatory collapse, recurrent laryngeal nerve palsy.

The clinical appearance in The clinical appearance in diphtheria infectiondiphtheria infection
Inflammation of the pharynx and tonsils marked by a pleudomembrane and swelling over the entire area.

Toxigenisity of C.diphtheriaToxigenisity of C.diphtheria
The toxigenisity of C.diphtheria is connected with bacteriophage.
The DNA that codes for diphtheria toxin is part of the genetic material of a temperate bacteriophage. During the lysogenic phase of viral growth, the DNA if this virus integrates into the bacterial chromosome and the toxin is synthesized.
C.Diphtheria cells that are not lysogenized by this phage do not produce exotoxin and are nonpathogenic.

Laboratory diagnosis Laboratory diagnosis
Bacteriological methodBacteriological method.. Isolating of pure culture Isolating of pure culture and and demonstrating toxin productiondemonstrating toxin production
Microscopy Microscopy of smears of the throat swab that are of smears of the throat swab that are stained by Gram method and methylene blue stained by Gram method and methylene blue (only presumptive diagnosis because possible (only presumptive diagnosis because possible presence of nontoxigenic corynebacteria and presence of nontoxigenic corynebacteria and other pleomorphic gram-positive rods)other pleomorphic gram-positive rods)
Gen diagnosis – PCR analysisGen diagnosis – PCR analysis

Tests for toxicity of Tests for toxicity of C.diphtheriaeC.diphtheriae
In vitro:In vitro:• Immunoprecipitation test in the agarImmunoprecipitation test in the agar• Immunoenzyme reaction Immunoenzyme reaction • PCR testPCR test
In vivo:In vivo:• Biological probe on the guinea pigs and Biological probe on the guinea pigs and
rabbits rabbits

Immunoprecipitation test for Immunoprecipitation test for diphtheria toxindiphtheria toxin
1
2
3
4
5

Biologic test for toxin Biologic test for toxin detectiondetection

Treatment Treatment
Antitoxin Antitoxin Antimicrobial drugs – antibiotics from the Antimicrobial drugs – antibiotics from the
penicillin or erythromycin familypenicillin or erythromycin family

Prevention Prevention
Immunization with diphtheria toxoid. Immunization with diphtheria toxoid.
Usually given as a combination of diphtheria Usually given as a combination of diphtheria toxoid, tetanus toxoid, and inactivated pertussis toxoid, tetanus toxoid, and inactivated pertussis bacilli)bacilli)
Toxoid is preparedToxoid is prepared by treating the exotoxin with by treating the exotoxin with formaldehyde during 4 to 6 weeks at temperature formaldehyde during 4 to 6 weeks at temperature 373700C.C.
Immunization does not preventImmunization does not prevent nasopharyngeal nasopharyngeal carriage of the microorganisms carriage of the microorganisms

The incidence and fatality rates for The incidence and fatality rates for diphtheria in the USAdiphtheria in the USA

TuberculosisTuberculosis is a chronic bacterial infection is a chronic bacterial infection of the lungs (and often other body organs) of the lungs (and often other body organs) characterized by slight fever, weight loss, characterized by slight fever, weight loss, sweating at night, and chronic cough sweating at night, and chronic cough productive of blood-streaked sputumproductive of blood-streaked sputum

Classification of mycobacteria Classification of mycobacteria that are agents of tuberculosisthat are agents of tuberculosis
Порядок Порядок ActinomycetalesActinomycetales Family Family MycobacteriaceaeMycobacteriaceae
• Genus MycobacteriumGenus Mycobacterium Species that are human pathogensSpecies that are human pathogens::
• Mycobacterium tuberculosis (humanMycobacterium tuberculosis (human,, 92 %) 92 %)• Mycobacterium bovisMycobacterium bovis ( (cowcow, 5 %), 5 %)• Mycobacterium africanumMycobacterium africanum (3 %) (3 %)• M. avium (M. avium (causes tuberculosis in causes tuberculosis in
immunocompromised humans, in AIDS immunocompromised humans, in AIDS patientspatients - - 15-14 %);15-14 %);

Properties of Mycobacterium Properties of Mycobacterium tuberculosistuberculosis
Pleomorphic long, thin rods with a tendency to Pleomorphic long, thin rods with a tendency to be filamentous or branching.be filamentous or branching.
Do not form capsules, flagella, or sporesDo not form capsules, flagella, or spores They are stained poorly by the dyes used in They are stained poorly by the dyes used in
Gram’s stainGram’s stain Obligate aerobeObligate aerobe Resistant to acids and alkalia, to various Resistant to acids and alkalia, to various
germicides, to dehydration germicides, to dehydration Slowly growing bacilliSlowly growing bacilli Cell wall consists of 60% lipids and contains Cell wall consists of 60% lipids and contains
several complex lipids: several complex lipids: Mycolic acids (long-chain fatty acids), which Mycolic acids (long-chain fatty acids), which
contribute to the organism’s acid-fastnesscontribute to the organism’s acid-fastness Wax DWax D Phosphatides Phosphatides

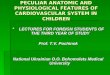
M.Tuberculosis in sputum M.Tuberculosis in sputum
Red acid-fast bacilli against acid-susceptible blue cells.
M.Tuberculosis bacilli are frequently localized intracellularly
Ziehl-Neelsen stained specimen

Cultivation of Cultivation of M.tuberculosisM.tuberculosis
M.tuberculosis forms non-pigmented R-colonies M.tuberculosis forms non-pigmented R-colonies Laboratory media for M.tuberculosis cultivation Laboratory media for M.tuberculosis cultivation
(Lowenstein-Jensen media) contains complex (Lowenstein-Jensen media) contains complex nutrients (eg, egg yolk, potato) and dyes (eg, nutrients (eg, egg yolk, potato) and dyes (eg, malachite green). The dyes inhibit the unwanted malachite green). The dyes inhibit the unwanted rapidly growing normal flora that interfere with rapidly growing normal flora that interfere with the isolation of M.tuberculosisthe isolation of M.tuberculosis

Virulence factors of Virulence factors of M.tuberculosisM.tuberculosis
Cord factorCord factor ( (trehalose dimycolatetrehalose dimycolate) – ) – destruction of cell mitochondriadestruction of cell mitochondria,, inhibition of inhibition of leukocyte migrationleukocyte migration
Lipids and phosphatidesLipids and phosphatides – – toxic effect for toxic effect for cellscells
Resistance to digestionResistance to digestion in macrophages and in macrophages and intracellular multiplicationintracellular multiplication
Protein, combined with waxes, (tuberculin) Protein, combined with waxes, (tuberculin) elicits delayed hypersensitivity elicits delayed hypersensitivity
Do not produceDo not produce exotoxins and exotoxins and have nohave no endotoxin endotoxin

Cord formation in infected Cord formation in infected tissuetissue
Red-stained M.tuberculosis and blue macrophages

PathogenesisPathogenesis
TransmissionTransmission
By respiratory aerosol By respiratory aerosol By food (nonpasterised By food (nonpasterised
milk)milk) By contactBy contact Vertical - from the Vertical - from the
mother to the fetusmother to the fetus ((rarelyrarely))
Infectious doseInfectious dose is around is around 10 cells10 cells
Natural reservoirNatural reservoir:: M.tuberculosis – M.tuberculosis –
humanshumans M.bovis – animals M.bovis – animals
(cow)(cow)
Initial site of Initial site of infectioninfection is the is the lung (commonly)lung (commonly)

Tubercle formation Primary tubercolosis.
The bacilli in lung are phagocytosed by macrophages and multiply intracellulary. After 2 weeks, delayed hypersensitivity to the TB develop.
Macrophages fuse together to form large multinucleated cells. Lymphocytes and macrophages then wall off the infected area from the surrounding tissue. The localized collection of inflamatory cells is called a granuloma (tubercle).
In most cases, growth of the TB is halted by granuloma formation.
Serondary reactivation tuberculosis. Live bacilli can remain dormant and become reactivated weeks, months, or years later. They multiplies, spreads into the bronchial tube and upper respiratory tract.

Forms of extrapulmonary Forms of extrapulmonary tuberculosistuberculosis
Tuberculosis of kidney and urinary tract Tuberculosis of kidney and urinary tract Tuberculosis of genital organs Tuberculosis of genital organs Tuberculosis of bones and jointsTuberculosis of bones and joints Tuberculosis of eyes Tuberculosis of eyes Tuberculosis of intestineTuberculosis of intestine Tuberculosis of regional lymph nodes Tuberculosis of regional lymph nodes Tuberculosis of skin Tuberculosis of skin Tubercular meningitis Tubercular meningitis

Immunity and prevention Immunity and prevention
BCG vaccineBCG vaccine contains a strain of alive contains a strain of alive attenuated M.bovis (bacilli Calmette-Guerin or attenuated M.bovis (bacilli Calmette-Guerin or BCG)BCG)
Success rate of vaccination is around 80% in Success rate of vaccination is around 80% in children and to 50% in adults.children and to 50% in adults.
The length of protection is 5 to 15 years. The length of protection is 5 to 15 years.
Resistance is mediated by cellular immunity, ie, by CD4-positive T cells

Laboratory diagnosisLaboratory diagnosis BacterioscopyBacterioscopy of sputum. Acid-fast staining by Zuehl- of sputum. Acid-fast staining by Zuehl-
Neelsen method and fluorescent acid-fast staining. Neelsen method and fluorescent acid-fast staining. Sensitivity of the method is 5-10 thousands of bacilli in Sensitivity of the method is 5-10 thousands of bacilli in a milliliter of sputuma milliliter of sputum
Bacteriologic methodBacteriologic method. Isolation of bacilli on Lowenstein-. Isolation of bacilli on Lowenstein-Jensen or Middlebrook media) and its identification. Jensen or Middlebrook media) and its identification. Sputum is pretreated with acid or alkali for Sputum is pretreated with acid or alkali for contaminents inhibition. Sensitivity of the method is 20-contaminents inhibition. Sensitivity of the method is 20-100 bacilli in a ml of sputum, duration is to 6-8 weeks. 100 bacilli in a ml of sputum, duration is to 6-8 weeks.
Gen diagnosisGen diagnosis – PCR analysis. Sensitivity – 10 and more – PCR analysis. Sensitivity – 10 and more bacilli in a ml, duration – 2 hoursbacilli in a ml, duration – 2 hours
Biological methodBiological method. Infecting guinea pegs, rabbits. The . Infecting guinea pegs, rabbits. The most sensitive – 1-5 bacilli in a ml of sputummost sensitive – 1-5 bacilli in a ml of sputum
Serological diagnosisSerological diagnosis (immuno-enzyme test, indirect (immuno-enzyme test, indirect agglutination test, complement-fixation test)agglutination test, complement-fixation test)
Allergic probeAllergic probe – Mantoux test – Mantoux test

A fluorescent acid-fast stain of A fluorescent acid-fast stain of M.tuberculosis from sputumM.tuberculosis from sputum

Mantoux test – tuberculin skin Mantoux test – tuberculin skin testtestHypersensitivity to the tubercle bacilli is detected by injecting small amount of tuberculin or PPD (purified protein derivative) into the skin.
Results - appearance of induration and erythema in the site of injection after 48-72 hours: Negative - less than 5 mm Intermediate – 5 to 10 mm Positive – more than 10-15 mm
Interpretation: 5-10 mm – neither person is vaccinated with BCG or probably
infected (if not vaccinated) Reaction of more than 10 mm are assumed to be infected with
M.tuberculosis If negative test person is not infected and not immune and
should be vaccinated with BCG

Treatment Treatment Multiple-drug therapy is used to prevent the drug-Multiple-drug therapy is used to prevent the drug-
resistant mutants circulation. resistant mutants circulation.
Duration of treatment is 4 to 24 monthsDuration of treatment is 4 to 24 months
Treatment for most patients with pulmonary Treatment for most patients with pulmonary tuberculosis is with 3 drugs:tuberculosis is with 3 drugs:
Isoniazid Isoniazid Rifampin Rifampin Pyrazinamide Pyrazinamide For immunocompromiced patients and humans with For immunocompromiced patients and humans with
disseminated form disseminated form ethambutol or streptomycinethambutol or streptomycin is is added added
Ciprofloxacin, amikacin, cycloserine. Ciprofloxacin, amikacin, cycloserine.

Atypical mycobacteriaAtypical mycobacteria
The atypical mycobacteria are classified onto 4 groups The atypical mycobacteria are classified onto 4 groups according to their rate of growth and whether they according to their rate of growth and whether they produce pigment under certain conditionsproduce pigment under certain conditions
Photochromogens Photochromogens (M.kansasii) (M.kansasii) produce a eyllow-produce a eyllow-orange-pigmented colony only when exposed to lightorange-pigmented colony only when exposed to light
ScotochromogensScotochromogens (M.scrofulaceum) produce the (M.scrofulaceum) produce the pigment chiefly in the darkpigment chiefly in the dark
NonchromogensNonchromogens (M.avium) produce little or no (M.avium) produce little or no yellow-orange pigment in presence or absence of yellow-orange pigment in presence or absence of lightlight
Rapidly growing mycobacteriaRapidly growing mycobacteria (M.fortuitum) produce (M.fortuitum) produce colonies in less than 7 days. colonies in less than 7 days.

Cultural properties of Cultural properties of mycobacteriamycobacteria
M. tuberculosis M. kansasii(photochromogenic)
M. gordonae(scotochromogenic)

Agent of leprosy Agent of leprosy
Mycobacterium leprae is agent of leprosy.
M.leprae has not been grown in the laboratory media or in cell culture. It can be cultivated in the mouse footpad on in the armadillo.
The bacilli replicates intracellularly, typically within skin hystiocytes, endothelial cells, and nerve cells. Red acid-fast bacilli
Ziehl-Neelsen stain

Leprosy Leprosy
The incubation period averages several years (due to very slow multiplication of bacilli)
There are 2 distinct forms of leprosy – tuberculiod and lepromatous
When lepromatous form deformation of hands, nose, lips, chin.
Leprosy is a chronic, progressive disease of the skin and nerves