Embed Size (px)
Citation preview
BONE SCAN IN ORTOHPAEDICSUMESH YADAV
DEFINITION
• A bone scan is a test that detects areas of increased or decreased bone activity by injecting a certain radiopharmaceutical ie. Tc-99m MDP.
• A/K/A Radionuclide bone scan or Bone scintigraphy
BONE SCAN
ADVANTAGES• Whole-body evaluation in one
test/ same rad exposure.
• Low radiation exposure• Sensitive evaluation
DISADVANTAGES• Needs radiopharms & gamma camera not widely available• Radiation exists• Low specificity• COST…….
Radiopharmaceutical (“Tracer”)
• The most widely used is Tc-99m labeled diphosphonates;
• Tc-99m Methylene diphosphonate (Tc-99m MDP)
• Tc-99m Medronate
Tc-99m MDP
Phosphonates concentrate in the mineral phase of bone: nearly two-thirds in hydroxyapatite crystals and one third in calcium phosphate
PATHOPHYSIOLOGY• Two major factors control accumulation of
phosphonates in bone, 1) blood flow , 2)extraction efficiency, which in turn depend on capillary permeability, acid-base balance, parathyroid hormone levels, etc.
• Maximum bone accumulation is reached 1 h after injection and the level remains practically constant up to 72 h.
• The peak of activity through the kidneys is reached after approximately 20 min. Within 1 h, with normal renal function, more than 30% of the unbound complex has undergone glomerular filtration andwithin 6 h, 60%.
• Tc-99m MDP uptake depends on osteoblast and osteoclast activity.• Increased uptake - osteoblastic activity present• Decreased uptake - pure lytic lesion ,
osteoclast activity

Technique of Bone Scan
Preparation: None• Injection of Tc-99m 20-25mCi IV, good hydrationafterwards & frequentvoiding• Wait for about 3 hrs to startimaging, avoidcontamination• Empty bladder prior toscanning• Change the cloth andremove things likely causeartifact.
• Can be performed as:– a) Limited bone scintigraphy or spot views
(planar images of a selected portion of the skeleton)
– b) Whole-body bone scintigraphy (planar images of the entire skeleton in anterior and posterior views)
– c) SPECT (single photon emission computed tomography- image of a portion of the skeleton)
– d) Multiphase bone scintigraphy (immediate and delayed images to study blood flow)
IMAGING ACQUISITION
Clinical indications
Oncological indications• Primary tumours (e.g. Ewing’s sarcoma,
osteosarcoma)• Staging, evaluation of response to therapy and
follow up of primary bone tumors• Secondary tumours (metastases)– Staging and follow-up of neoplastic diseases– Distribution of osteoblastic activity prior to
radiometabolic therapy
Non-neoplastic diseases
Whenever there is an increase in blood flow to a lesion or there is an alteration in osteoblastic activity.– Stress and/or occult fractures.– Trauma – Musculoskeletal inflammation and infection– Bone viability (grafts, infarcts, osteonecrosis).– Metabolic bone disease.– Arthritis– Complications of hardware/prosthetic joint replacement, loose
or infected joint prosthesis.– Heterotopic ossification.– Complex regional pain syndrome (CRPS)– Other bone disease, such as Paget disease, Langerhans cell
histiocytosis, or fibrous dysplasia.– Congenital or developmental anomalies.
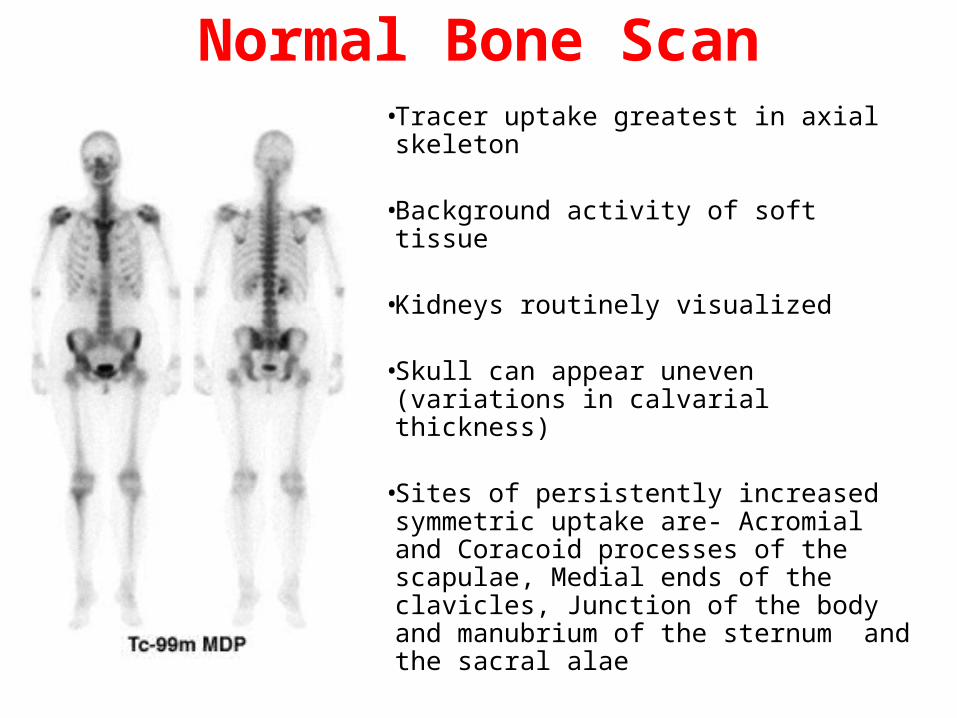
Normal Bone Scan• Tracer uptake greatest in axial
skeleton
• Background activity of soft tissue
• Kidneys routinely visualized
• Skull can appear uneven (variations in calvarial thickness)
• Sites of persistently increased symmetric uptake are- Acromial and Coracoid processes of the scapulae, Medial ends of the clavicles, Junction of the body and manubrium of the sternum and the sacral alae
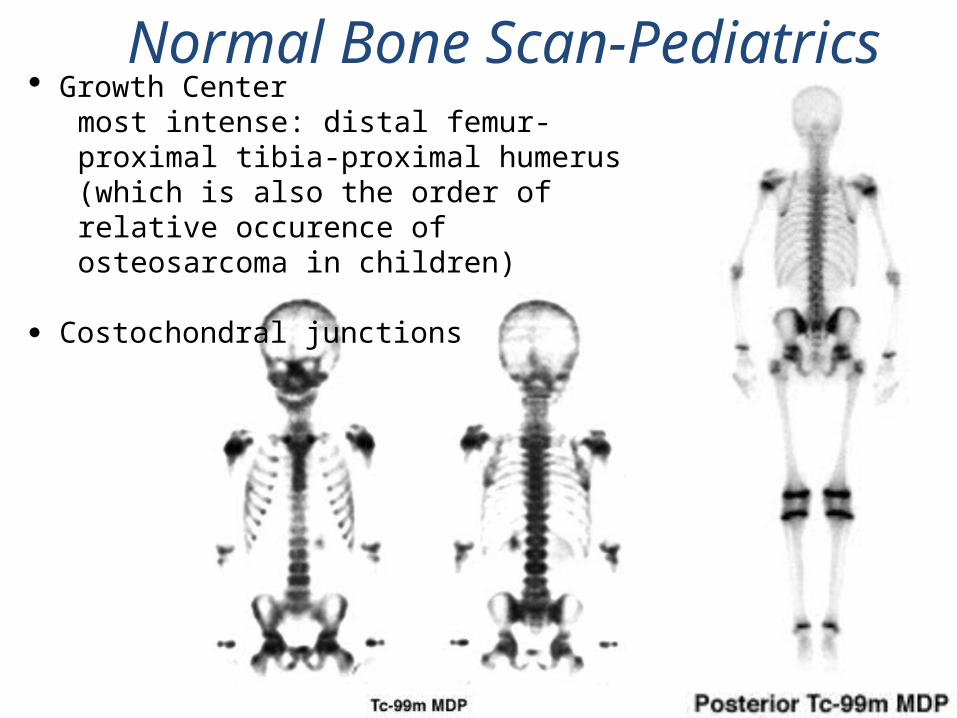
Normal Bone Scan-Pediatrics· Growth Center
most intense: distal femur-proximal tibia-proximal humerus (which is also the order of relative occurence of osteosarcoma in children)
Costochondral junctions
ABNORMAL BONE SCANS
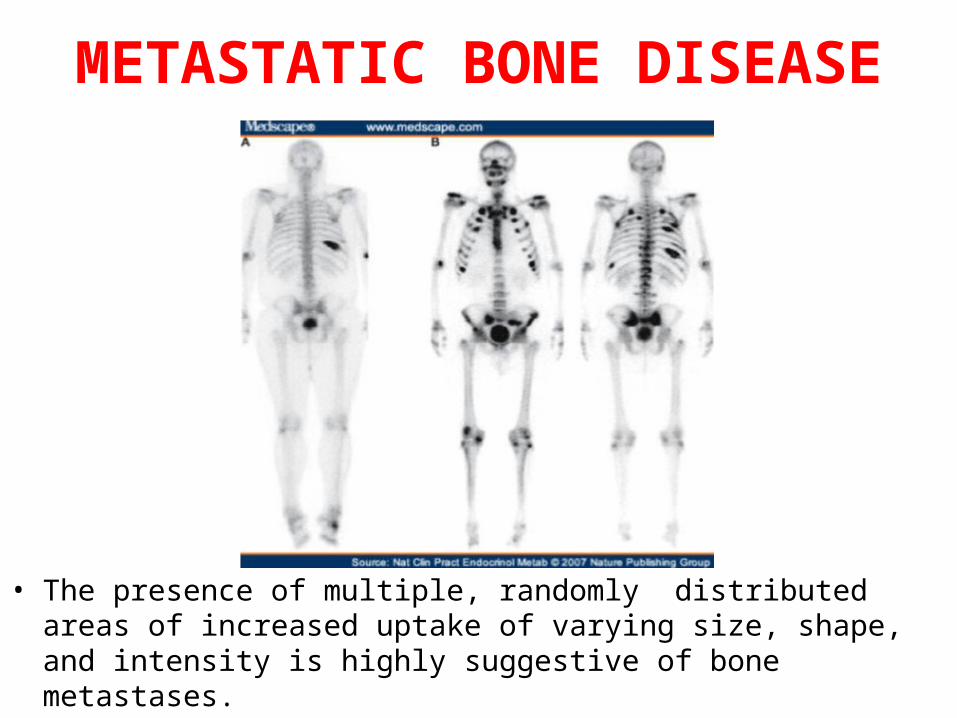
METASTATIC BONE DISEASE
• The presence of multiple, randomly distributed areas of increased uptake of varying size, shape, and intensity is highly suggestive of bone metastases.
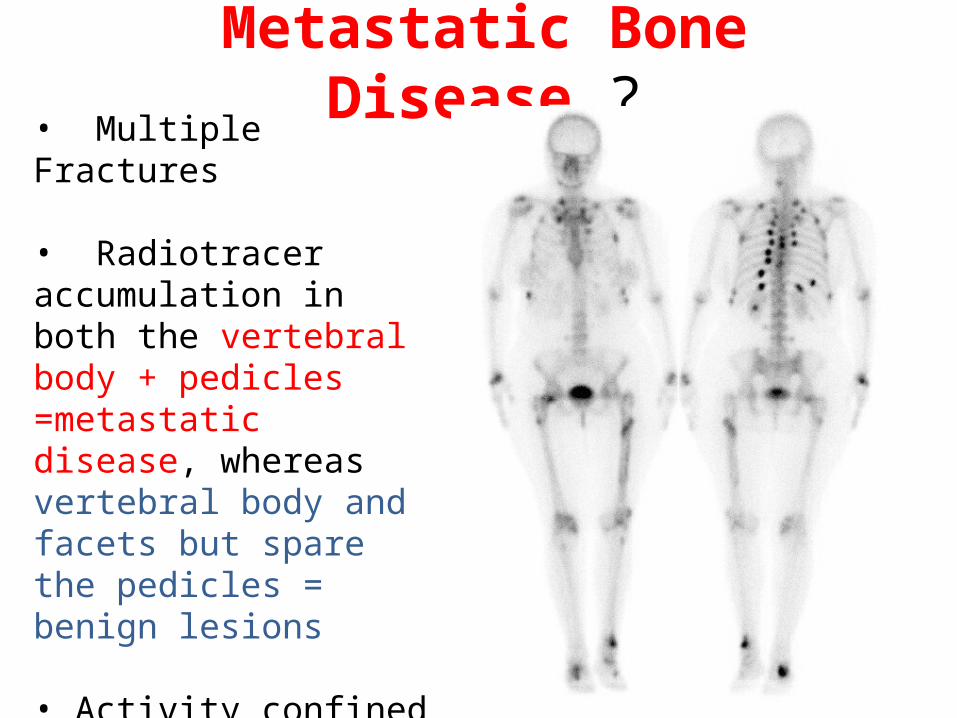
Metastatic Bone Disease ?• Multiple Fractures
• Radiotracer accumulation in both the vertebral body + pedicles =metastatic disease, whereasvertebral body and facets but spare the pedicles = benign lesions
• Activity confined to the vertebral body can be due to tumor, trauma, or infection
Flare phenomenon
• Seen in patients who are responding to treatment, reflects healing of the bone lesions and has been described as the “flare” phenomenon.
• Usually observed within 3 months after initiation of treatment and is often associated radiographically with the sclerotic changes that indicate healing.
• Continued increase in the number and intensity of lesions beyond 6 months is usually indicative of disease progression
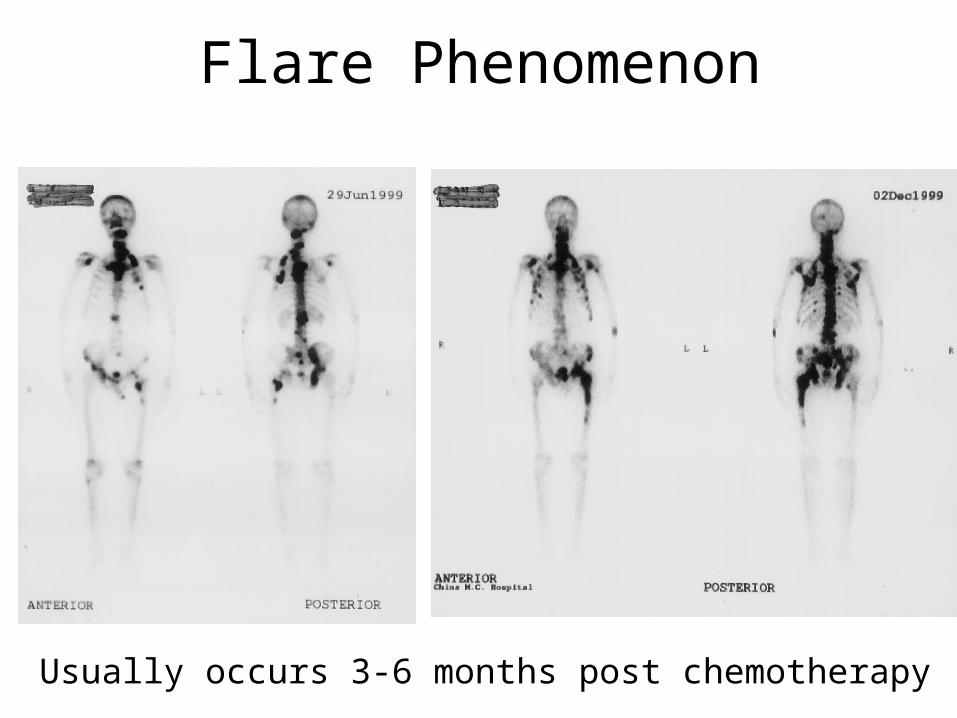
Flare Phenomenon
Usually occurs 3-6 months post chemotherapy
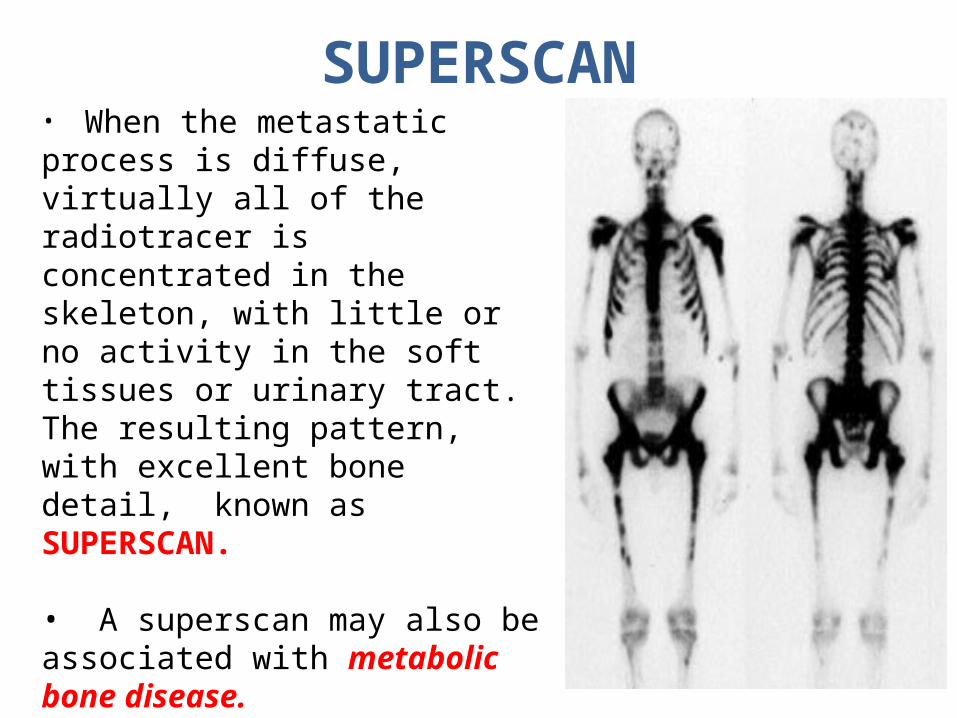
SUPERSCAN• When the metastatic process is diffuse, virtually all of the radiotracer is concentrated in the skeleton, with little or no activity in the soft tissues or urinary tract. The resulting pattern, with excellent bone detail, known as SUPERSCAN.
• A superscan may also be associated with metabolic bone disease. Unlike in metastatic disease, however, the uptake in metabolic bone disease is more uniform in appearance and extends into the distal appendicular skeleton.
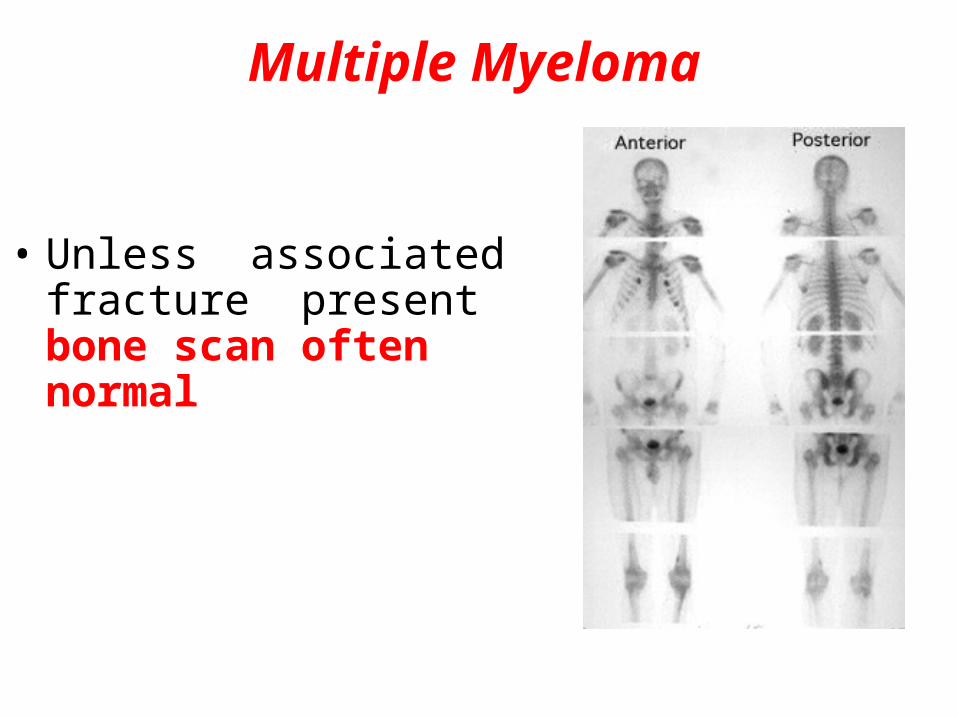
Multiple Myeloma
• Unless associated fracture present bone scan often normal
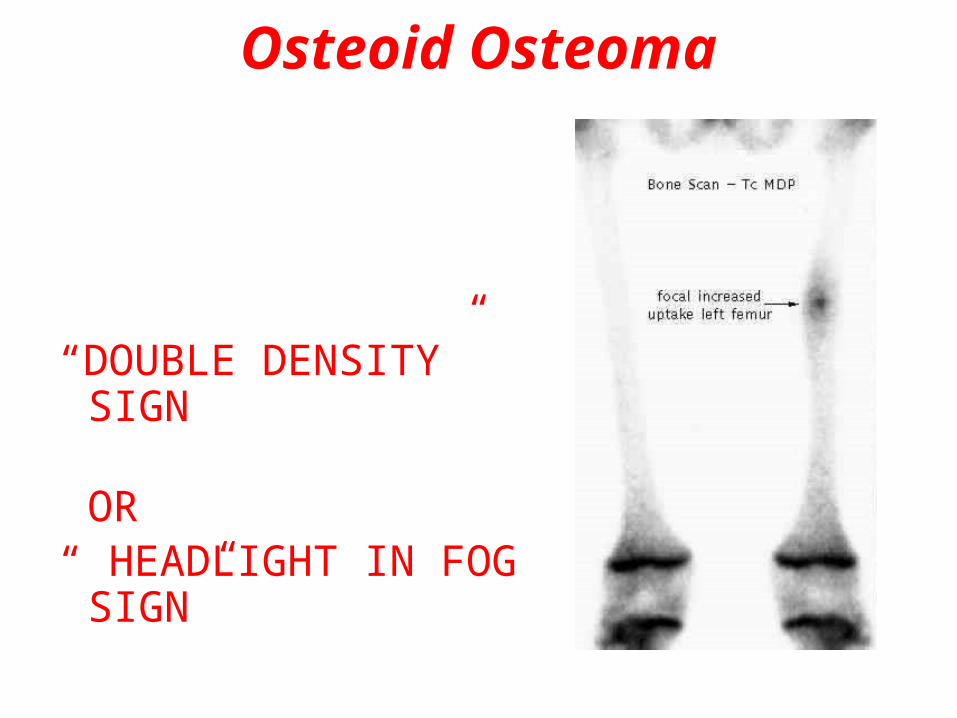
Osteoid Osteoma
“DOUBLE DENSITY” SIGN OR“ HEADLIGHT IN FOG SIGN”
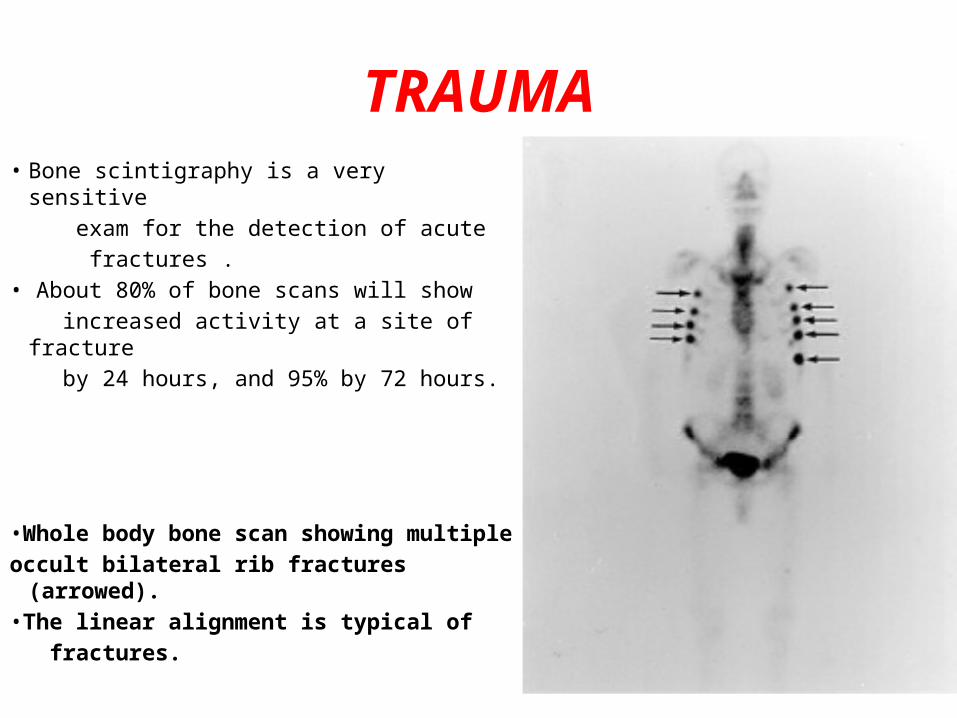
TRAUMA• Bone scintigraphy is a very sensitive exam for the detection of acute fractures .• About 80% of bone scans will show increased activity at a site of fracture by 24 hours, and 95% by 72 hours.
•Whole body bone scan showing multipleoccult bilateral rib fractures (arrowed).•The linear alignment is typical of fractures.
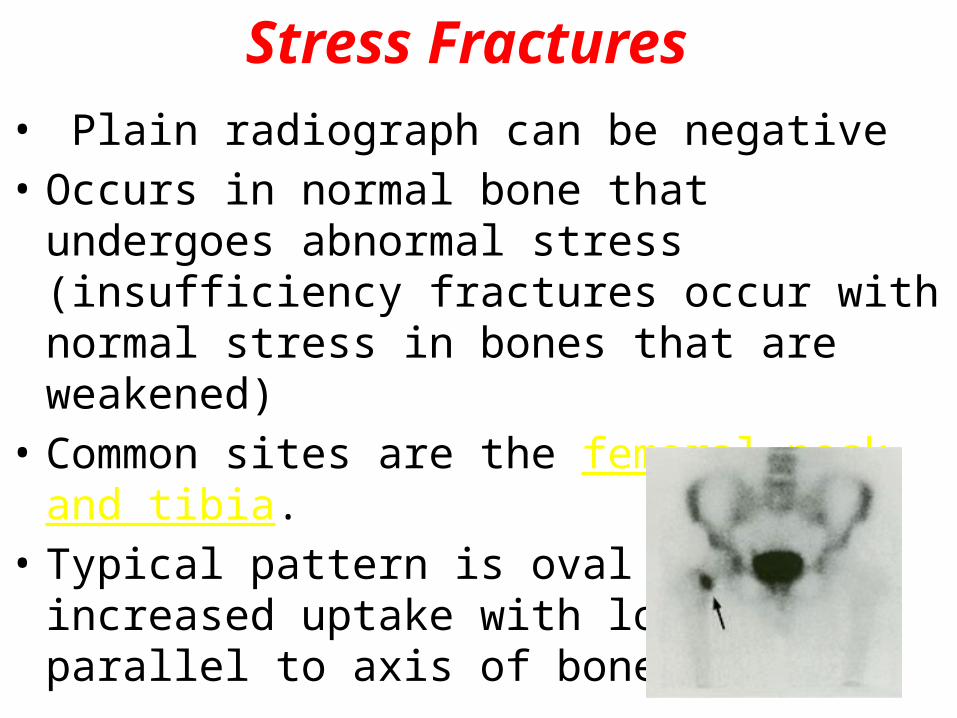
Stress Fractures• Plain radiograph can be negative• Occurs in normal bone that undergoes abnormal
stress (insufficiency fractures occur with normal stress in bones that are weakened)
• Common sites are the femoral neck and tibia. • Typical pattern is oval area of increased uptake with
long axis parallel to axis of bone
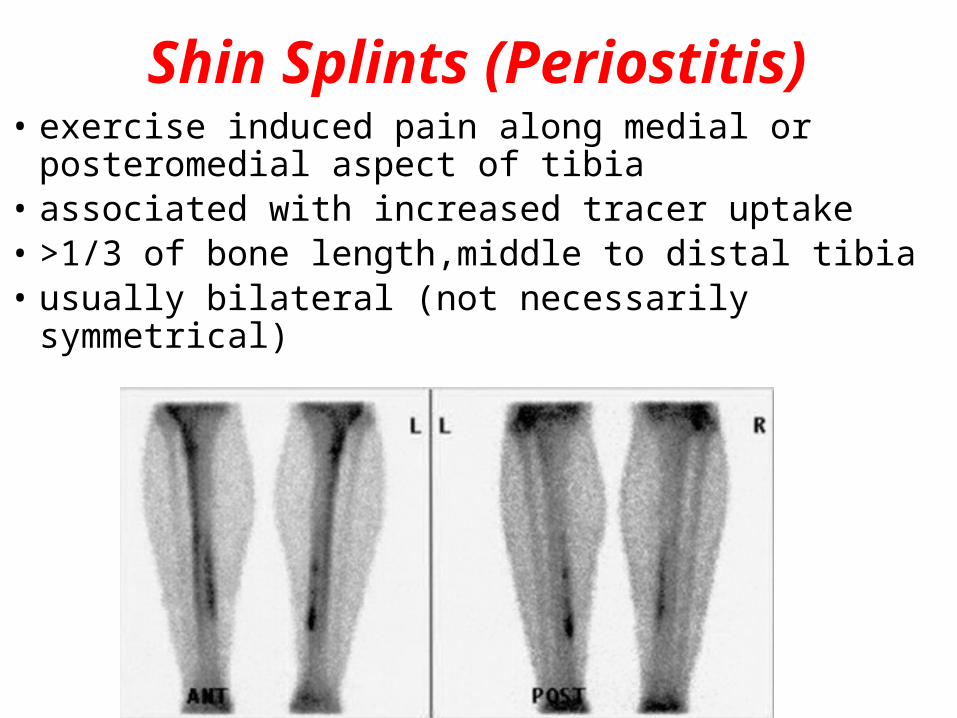
Shin Splints (Periostitis)• exercise induced pain along medial or
posteromedial aspect of tibia• associated with increased tracer uptake• >1/3 of bone length,middle to distal tibia• usually bilateral (not necessarily symmetrical)
Bone Infarction/AVN • Appearance depends on time course – In acute phase of vascular compromise, no
radiotracer is delivered to the bone tissue. So the affected part of the bone appears as a photopenic defect.
– After revascularization, exuberant osteoblastic repair manifests as intense radiotracer uptake.
– Subsequently, when repair is complete, radiotracer uptake may return to baseline levels
• Less sensitive than MRI
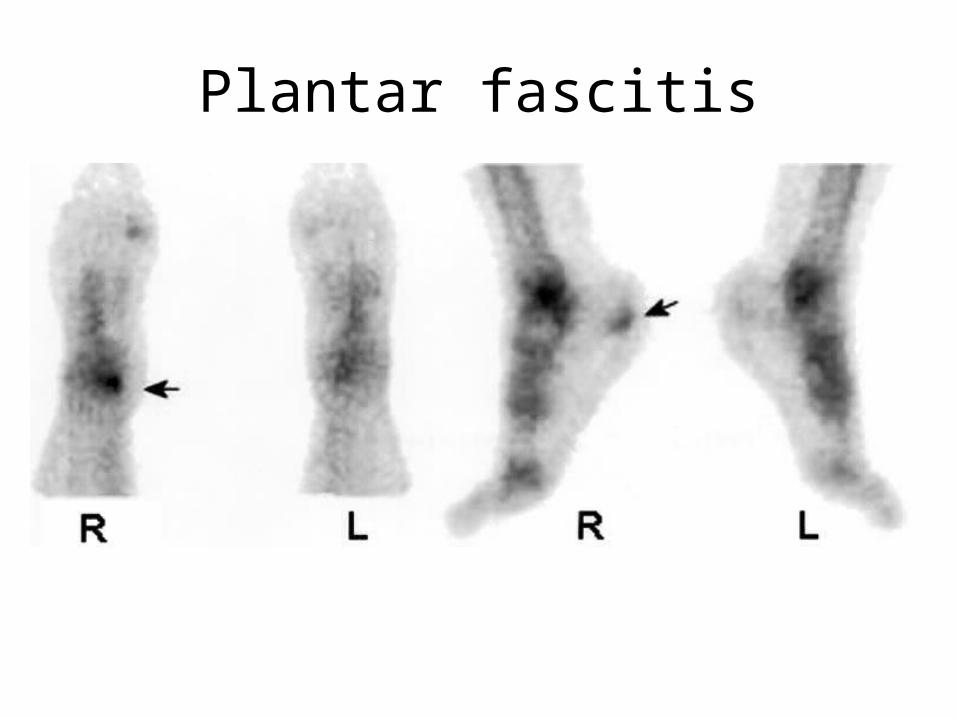
Plantar fascitis
3 PHASE BONE SCAN• 3 stages which follow IV injection of the tracer.• 1) Flow phase• 2 to 5-sec images are obtained for 60 seconds after injection• Demonstrates perfusion and characterises the blood flow to a particular area• 2) Blood pool phase• the blood-pool image is obtained 5 min after injection• demonstrated the blood pool, not the blood flow• inflammation causes capillary dilatation and increased blood flow
• If the study is going to be a triphasic bone scan, a third phase is added.
• 3) Delayed phase• the bone image is obtained 2 - 4 hours later• urinary excretion has decreased the amount of the radionuclide in soft tissue • DIFFERNTIATE OSTEOMYELITIS FROM CELLULITIS
OSTEOMYELITIS
• The classic appearance of osteomyelitis on three-phase bone scans consists of focal hyperperfusion, focal hyperemia, and focally increased bone uptake
• Phase I + Phase II with negative Phase III- Cellulitis
• All positive- OM
SOME OTHER TRACERS
• GALLIUM-67-Sensitive for detection of inflammatory process.- HOT in ABSCESS ( Vertebral OM)- LYMPHOMA- SARCOIDOSIS
• INDIUM 111-• Tagged with leucocytes.• More sensitive than Ga67 scans.• Used with Sulfur Colloid Scan – Delineate areas of
normal bone activity IN 111 labelled Leucocyte- Highlight involved region.- SO INCONGURENCE OF BOTH IS HIGHLY SUGGESTIVE
OF INFECTION
PAINFUL PROSTHESIS-LOSSENING OR INFECTION
• 3 PHASE BONE SCAN-• Focally increased uptake- Loosening• Diffuse , Uniformly distribution – Infection• Not very specific• Ga-67 SCAN-• Differntiate between pure mechanical
loosening and infection