Embed Size (px)
Citation preview
Effiong E. Akang
Consultant Pathologist
University College Hospital
Ibadan, NIGERIA
BRAIN CUT UP FOR THE GENERAL PATHOLOGIST

INTRODUCTION
•CNS examination is an essential part of every full autopsy•Brain-only autopsy not ideal, but may be indicated in a few cases•Many general pathologists regard CNS examination to be adaunting task (unnecessarily so).•While neuropathologists conduct extremely detailed CNSexaminations, the same is true of other sub specialists. Forexample, cardiac pathologists may take up to 70 sections of theheart.•Yet every self respecting pathologist undertakes a fairly thoroughexamination of the heart in the average autopsy. Why not thebrain?

PREPARATION FOR BRAIN CUT UP
•CNS examination begins with thorough review of pertinentclinical findings (history, examination, investigations includingneuroimaging, management and clinical course)•CNS involvement occurs in majority of systemic illnesses;however, primary CNS disorders are relatively uncommon. Evenso, there is an impressive list of numerous primary CNSconditions•Review clinical findings and cut brain in presence of managingclinical team and certified brain aficionados (adult/paediatricneurologist, neurosurgeon, neuroradiologist, psychiatrist) so asto obtain maximal benefit

CLINICAL HISTORY
43 year old male•Headache- 5 days (sudden onset, throbbing, generalised)•Seizures- 4 days (began with twisting of mouth and up rolling of eyesand spread to become generalised tonic-clonic); 5 episodes•Vomiting- 4 days (effortless); 8 episodes•No photophobia, phonophobia or slurring of speech. No previoushead trauma, no fever, no weight loss, no limb weakness•Motor-cycle accident 3 years previously, but no neurological sequelae•Smoked marijuana and drank alcohol heavily until 5 years previously•Not a known diabetic, hypertensive or asthmatic. No family history ofsimilar illness. No other significant medical, social or drug history

PHYSICAL EXAMINATIONYoung male, drowsy, not pale, anicteric, not cyanosed, afebrile, mildlydehydrated, no palpable lymph nodes, no pedal oedema.Glasgow Coma score- 14/15. Pupils equal bilaterally, muscle tone andpower normal globally. Reflexes normal, plantar response flexorbilaterally, no neck stiffness, Kernig/Brudzinski signs negative.Pulse rate 100b/m, regular, normal volume. BP- 110/80 mmHg, HS 1and 2, no murmur.Respiratory rate 18/min, trachea central, percussion notes resonant,breath sounds vesicular.Abdomen flat, moved with respiration, no tenderness, no palpableorganomegaly.Provisional diagnosis- ?Intracranial space occupying lesion, to rule out(1) Benign intracranial hypertension, (2) Viral encephalitis

INVESTIGATIONS
Random blood glucose- 187.2mg/dl (normal 45-90 mg/dl),
PCV- 39% (normal 40-54%)
Full blood count- neutrophilia and lymphopenia
Urinalysis- haematuria ++
Retroviral screening- non-reactive
CT/MRI was not available

MANAGEMENT AND CLINICAL COURSE
He was placed on intravenous mannitol 250ml over 30 minutes,followed by intravenous Normal saline 1L 8hrly.Following review by the unit senior registrar (at 9.15 pm on14/10/14) an assessment of Adult onset seizure disorder?Intracranial space occupying lesion was made and the patientwas administered 40 mg of diazepam into each pint for the firstlitre of normal saline, Tab carbamazepam 200 mg bd, IVdiazepam 5 – 10 mg for break through seizures prn.The patient deteriorated and died 11 hours after admission

CNS AUTOPSY EXAMINATION-1- Exposure of the brain
Make full thickness ear-to-ear incisionof scalp and reflect skin flaps anteriorlyand posteriorly to expose skull boneUse manual or electrical saw(adult/older children) to remove skullcap.In neonates and infants prior to fusionof skull sutures and closure offontanelles, scissors can be used tooutline and reflect four flaps (frontalbone, occipital bone and 2 temporalbone flaps (modified Beneke method)
Waters BL, 2009. Handbook of autopsy practice

CNS AUTOPSY EXAMINATION-2A- Removal of the adult brain
Reflect dura over cerebral hemispheres
Gently lift up frontal poles and sever cranial nerves
beginning from optic to hypoglossal nerves
Transect distal brainstem/spinal cord as low as
possible and then lift out brain
CNS AUTOPSY EXAMINATION-2B- Removal of the infant brain
Reflect the dura over the cerebral hemispheresa) In cases of suspected birth trauma, remove the
hemispheres one at a time, using gravity to aid brainremoval. This way the falx cerebri and dural venoussinuses can be examined in situ. Subsequently, thebrainstem and cerebellum are removed as a block
b) In other cases remove the brain exactly as for the adultbrain, again using gravity to aid removal

CNS AUTOPSY EXAMINATION-2C- Brain smears
Prior to immersion in formalin smears may beobtained in cases of•Cerebral malaria (wet imprint)•Bacterial infections (Gram stain)•Superficial extra-axial tumours (Giemsa/Pap stain)

CNS AUTOPSY EXAMINATION-3- Sectioning the brain
The brain is usually examined after fixation in buffered10% formalin for 1-2 weeks. If there is significantintracranial haemorrhage, change the fixative after first 24hours to achieve better fixationIn forensic autopsies, or in a few selected cases where afull autopsy fails to reveal any significant changes outsidethe CNS, brain may be sectioned freshIn either case, weight of the brain must be recordedimmediately after removal from the cranial cavity

CNS AUTOPSY EXAMINATION-3- Sectioning the brain
Brain examination begins with inspection- examine for symmetry of the hemispheres; gyri and sulci; leptomeninges; brainstem and cerebellum; vessels of circle of Willis; any other focal lesions

CNS AUTOPSY EXAMINATION-3- Sectioning the brain
Transect brainstem and cerebellumMake serial sections beginning from frontal lobes to occipital lobes at 1cm intervalsArrange slices serially as you proceed

CNS AUTOPSY EXAMINATION-3- Sectioning the brain
The brain weighs 1250 gm (normal = 1100-1450gm), it appears dusky in colour and there is generalised congestion of the leptomeninges. The right hemisphere is bigger than the left hemisphere, showing narrowing of sulci and flattening of gyri, overlying a right frontal lobe mass lesion.

CNS AUTOPSY EXAMINATION-3- Sectioning the brain
Coronal sections of cerebral hemispheres show a right frontal lobe encapsulated abscess measuring 2.8 x 2.5 x 2.5 cm. There is softening and yellowish discolouration of the surrounding white matter, with blurring of grey-white matter differentiation. There is herniation of the right cingulate gyrus and effacement of the anterior horn of the right lateral ventricle with deviation of the septum pellucidum to the contralateral side.

CNS AUTOPSY EXAMINATION-3- Sectioning the brain
Transverse sections of brain stem and sections of the cerebellum appear grossly normal and show no focal lesion
CNS AUTOPSY EXAMINATION-3- Sectioning the brain- CONSULTATION
In cases requiring neuropathological consultation (immunohistochemistry and molecular studies for neurodegenerative or metabolic disorders) perform autopsy within 24 hours of death. Details will vary based on specific requirements of consultant neuropathologist
• Bisect fresh brain and preserve one half (snap freeze with liquid nitrogen and store at -800C). Ship in dry ice. Fix second half for 1-2 weeks in buffered 10% formalin and section as described above. Alternatively ship both halves.
• Fix fresh intact brain in buffered 10% formalin and at the time of brain cut up preserve one half uncut and ship by courier service. The second half is sectioned as described above. Alternatively ship intact fixed brain in 10% formalin by courier service

CNS AUTOPSY EXAMINATION-4- Removal of the spinal cord
POSTERIOR APPROACH• Midline incision over spinous
processes, resect muscle, bilateral laminectomy
• Useful for neck injuries, carniocervical instability, posterior neural tube defects
• Cons- leakage of embalming fluids, limited dissection of spinal nerve roots
ANTERIOR APPROACH• Cut lateral processes, bilaterally from
upper thoracic to sacral spines. Make transverse cuts through proximal and distal vertebral bodies. Spinal cord delivered by Kernohan’s method
• Useful for removal of spinal cord and peripheral nerves in continuity, more rapid and convenient
• Cons- likelihood of spinal cord damage

CNS AUTOPSY EXAMINATION-5- Provisional anatomical diagnosis
1. Chronic pyelonephritis
2. Right frontal lobe cerebral abscess
3. Haemorrhagic gastritis
4. Pulmonary oedema

CNS AUTOPSY EXAMINATION-6- Clinicopathological correlation
Adult onset seizures with raised intracranial pressure
Brain abscess
Use of intravenous mannitol instead of high dose corticosteroids accelerated patient’s demise

SELECTED CASES- 1• 17 year female with
ante mortem FNA diagnosis of NHL
• Post-mortem revealed large cell NHL with involvement of ovaries, kidney, pancreas, intestines, thyroid, scalp, skull and dura
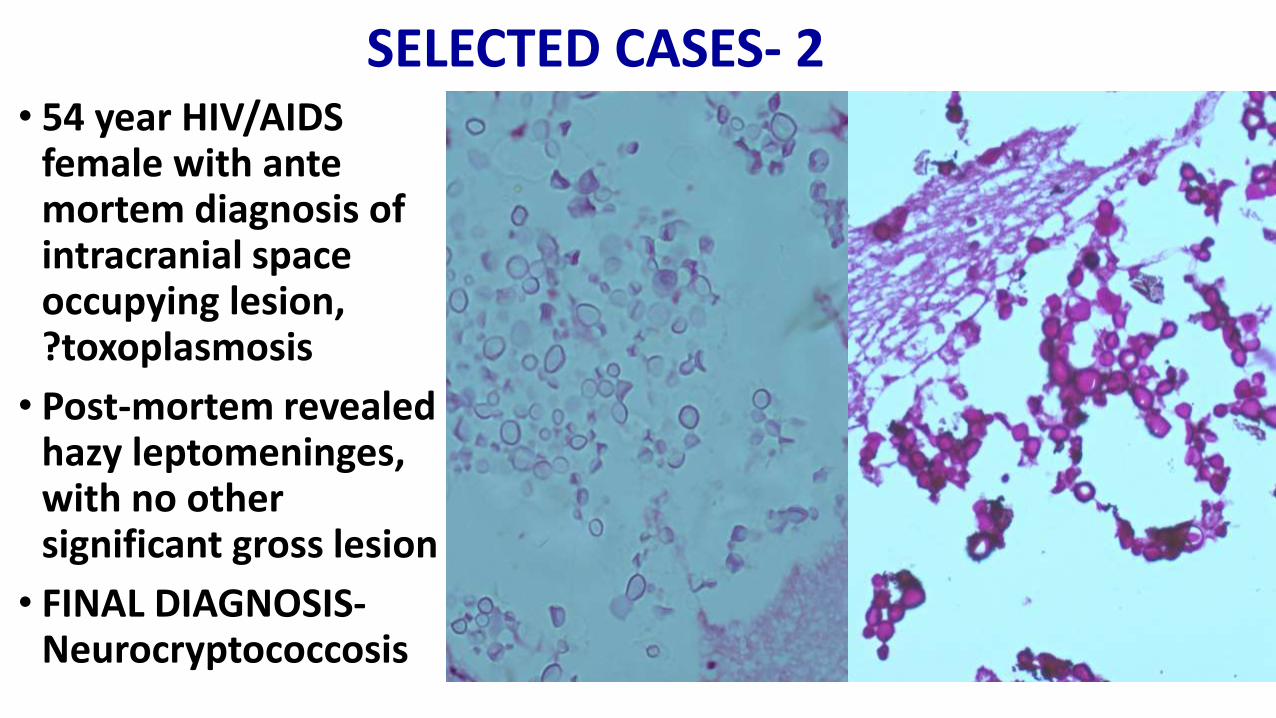
SELECTED CASES- 2• 54 year HIV/AIDS
female with ante mortem diagnosis of intracranial space occupying lesion, ?toxoplasmosis
• Post-mortem revealed hazy leptomeninges, with no other significant gross lesion
• FINAL DIAGNOSIS-Neurocryptococcosis
SUMMARY
• CNS examination is an essential part of every full autopsy
• Should be preceded by review of clinical findings and in presence of managing clinical team and neuro specialists
• Brain and spinal cord examination should be systematic and detailed
• Clinicopathological correlation with clinical and other autopsy findings is vital

Thanks for listening!