Embed Size (px)
Citation preview
LARYNGEAL CARCINOMA- MANAGEMENT
Dr Vikas
MANAGEMENT OF LARYNGEAL CANCERS
Multidisciplinary teams
Minimum team defined by British Association of Otolaryngologist,-
head and neck surgeon is an otolaryngologist, a
radiotherapist/oncologist, nurse, speech and swallowing therapist
CARCINOMA IN SITU
Is replacement of the full depth of epithelium by malignant cells,
without those transgressing the basement epithelium
Tis should be regarded as part of the continuum of early laryngeal
cancer and managed as T1 carcinoma
High possibilities of recurrent disease suggests holding back use of
radiotherapy for those leisions where resection would lead to
significant functional defecits and use of surgical technique wherever
possible
GLOTTIC CANCER
Carcinoma in situ
Trans oral endoscopic CO2 laser
Microlaryngoscopic cord stripping
Regular follow up is essential
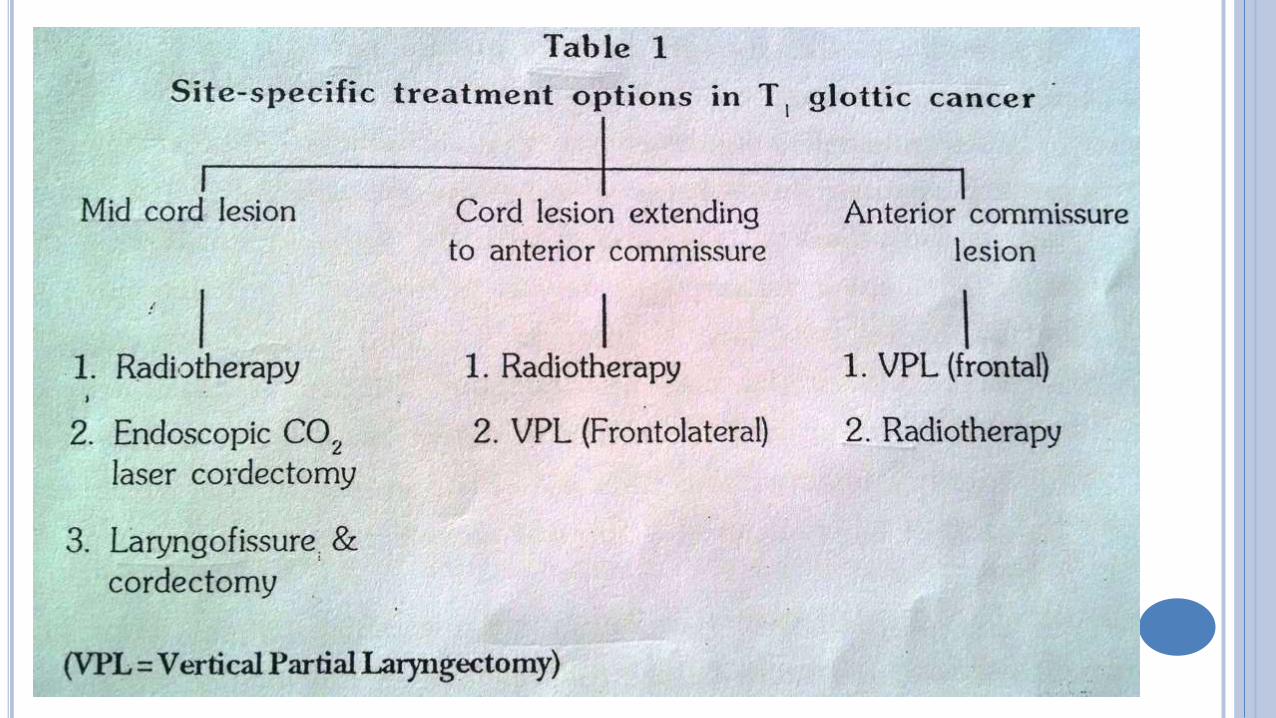
Glottic T1NO
Narrow field Radiotherapy
Voice conservation surgery
Type of surgery depends upon location of lesion within glottis
Mid cord lesion
Trans oral Endoscopic cordectomy/ CO2 laser cordectomy
>90% cure rates
Good voice quality
Very short treatment period
Tracheostomy is avoided
Laryngofissure with cordectomy-
>90% cure rates
slightly inferior voice quality
Temporary tracheostomy is required
Cord lesion extending to the anterior commissure-
Radiation therapy
Vertical frontolateral laryngectomy
Endoscopic CO2 laser excison (experience required)
Pure anterior commissure lesion
May cause early cartilage invasion ( absence of inner perichondrium)
May involve base of epiglottis or cricothyroid membrane without
causing cord fixity.
T3/T4 lesion may clinically be Under staged as T1/T2 lesion
Cure rates will be drastically compromised with radiotherapy
Surgery is preferred modality.
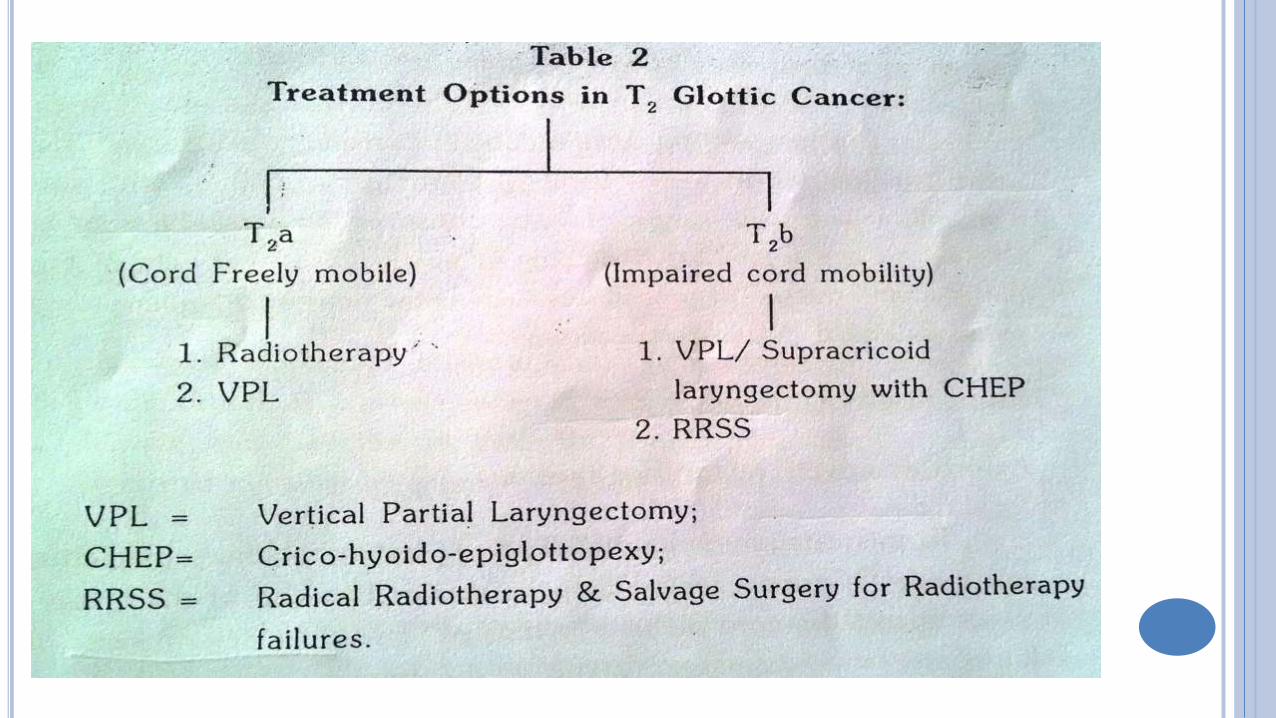
GLOTTIC T2 N0
Includes –
Superficial tumors where vocal cords are freely mobile but the suface
extension is beyond glottis( T2a)
Infiltrative tumors causing impaired cord mobility(T2b)
For T2a lesions Radiotherapy should be Treatment of choice
Voice is near normal
Regular follow up is required
Salvage surgery on failure of radiotherapy
T2b lesions being more infiltrative
Best Treated with VPL or supracricoid laryngectomy with CHEP.
Voice remains hoarse
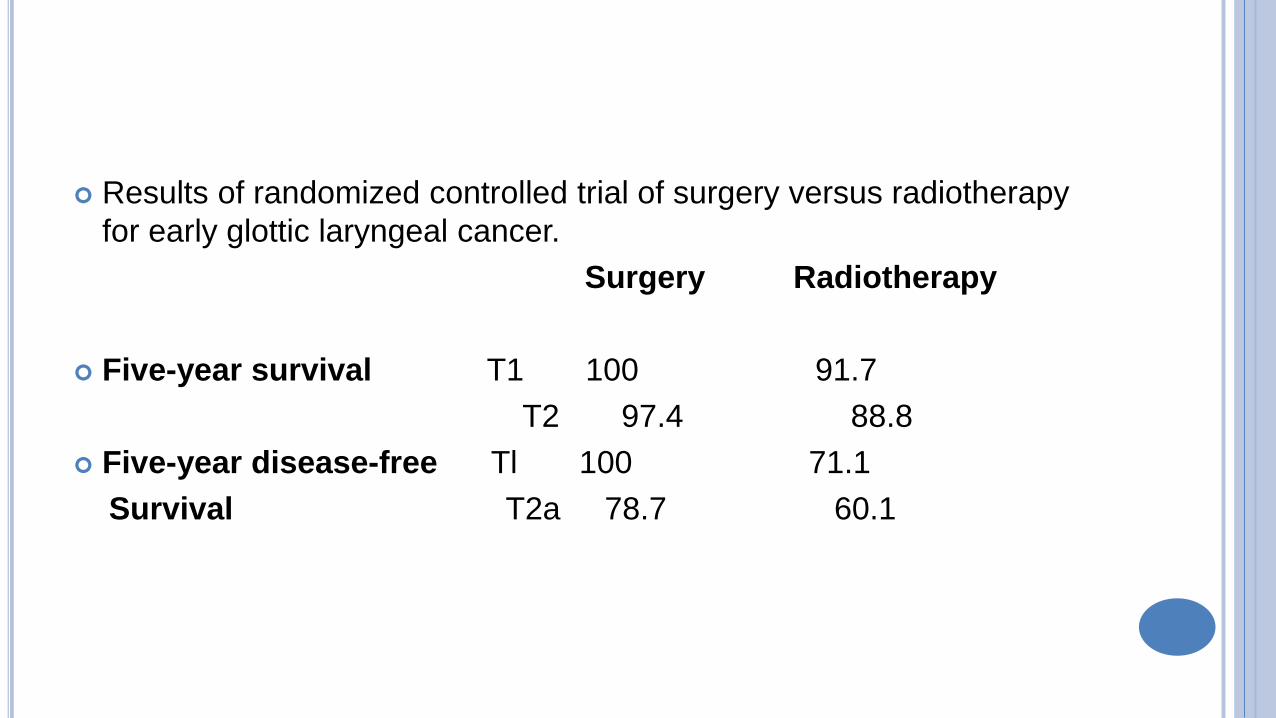
Results of randomized controlled trial of surgery versus radiotherapy
for early glottic laryngeal cancer.
Surgery Radiotherapy
Five-year survival T1 100 91.7
T2 97.4 88.8
Five-year disease-free Tl 100 71.1
Survival T2a 78.7 60.1
GLOTTIC T3, T4
Fixation of vocal cord is grave prognostic sign
Results with surgery are far superior to those with surgery alone.
Alternative is radical radiotherapy with surgery reserved for salvage of
radiotherapy failures.
Strict follow up is required
Detection of recurrences
Harwood et al, registered a surgical salvage rate of 60%
In india due to extremely poor follow up total laryngectomy is
preferred.
SUPRA GLOTTIC CANCER
Mobile cords and No cartilage invasion-
Chief determinants of choice of therapy are-
Status of cervical lymph nodes
Age
Pulmonary status
Subsite within supraglottis
.
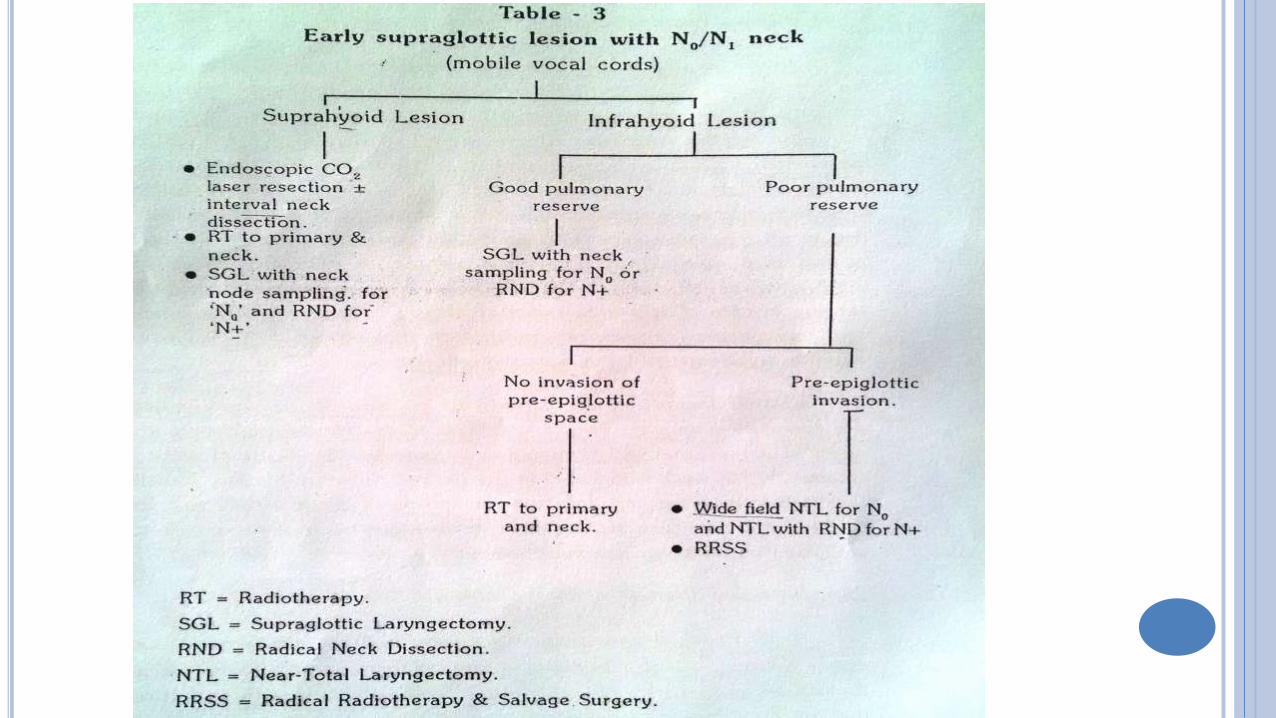
Minimal or no neck disease N0/ N1
Lesion of infrahyoid epiglottis
Surgery claims superior cure rates in comparison to radiotherapy
If pulmonary status is poor radiotherapy is preferred (no involvement of pre-
epiglottic space on CT/MRI )
Involvement of pre-epiglottic space- near total laryngectomy is preferred.
Lesions of suprahyoid epiglottis
Generally exophytic
Unlikely to involve pre-epiglottic space
Respond well to radiotherapy
Neck is included in radiation field
Small localized lesions best resected endoscopically with CO2 laser
Neck dissection may be carried out after 2 weeks if required.
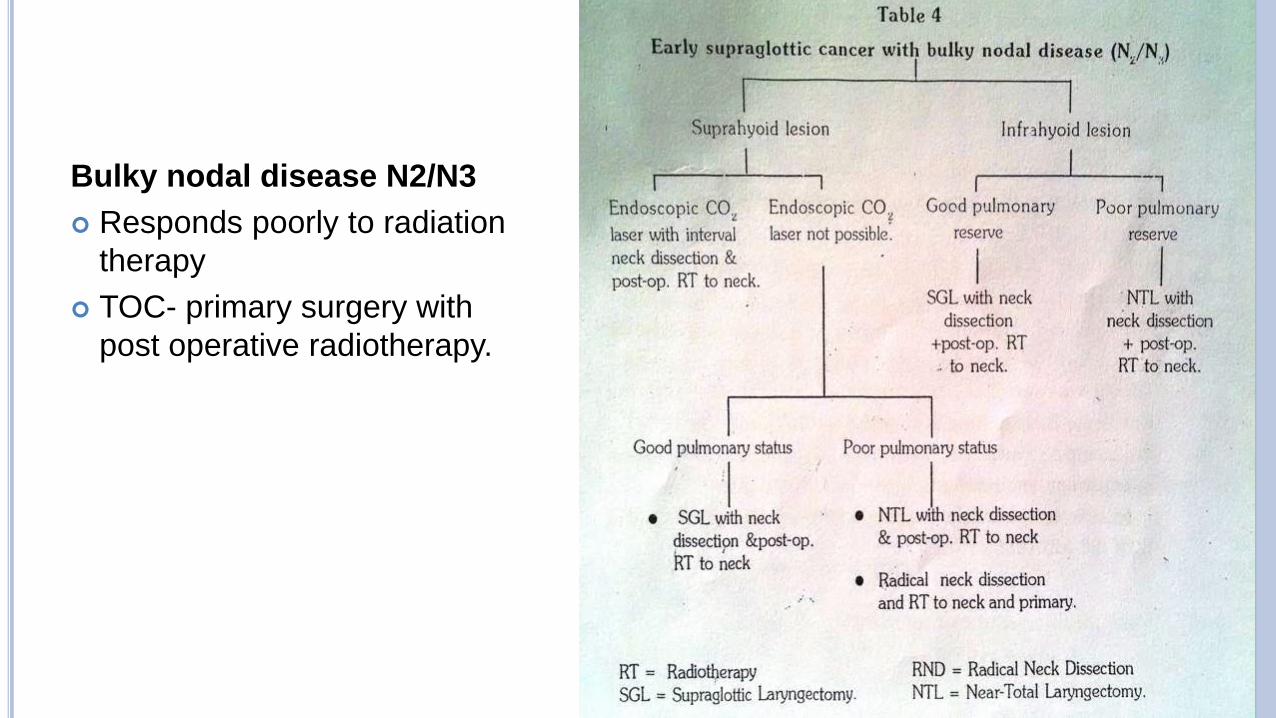
Bulky nodal disease N2/N3
Responds poorly to radiation
therapy
TOC- primary surgery with
post operative radiotherapy.
VOCAL CORD FIXITY / CARTILAGE INVASION
Total or Near total laryngectomy is indicated.
SURGERY
Advantages:
1.Treatment in single sitting
2.Minimal absence from employment
3.Certainty of removal of specimen & ability to assess margin surgically
4.Allows further laryngeal surgery or radiotherapy in case of recurrence
Disadvantages
Affect voice quality
Access sometimes difficult
Requires general anaesthesia & may need repeated operations for
which patient may not be fit
RADIATION –ADVANTAGES
Functional preservation.
Patient's preference
No Post Operative complication
Deals effectively with the microscopic invasion into the adjacent
lymphatic and venous channels
DISADVANTAGES
Ineffective at the necrotic centre of tumor so ineffective against large
bulky tumors
Relatively ineffective against Radio resistant tumors
Post radiation reactions
Morbidity
TRANSORAL LASER SURGERY
INCLUSIONAL CRITERIA
Complete endoscopic visualization of the carcinoma
Tumor extension to the contralateral VC < 3mm
Absence of arytenoid involvement (except vocal process)
Subglottic extension < 5mm
Supraglottic extension no further than lateral extension of ventricle
Mobile vocal folds
No cartilage involvement
ADVANTAGES
Good voice quality
Good swallowing
Lower complications rates
Lower costs
Shorter hospitalization
Tracheostomy and NG tubes not routinely required
OPERATIVE CONSIDERATIONS
Increased difficulty in identification of recurrent carcinoma in irradiated tissue leads to routine use of frozen section
All margins to be confirmed by permanent section post-op.
Strict follow-up with fibroscopic examination and serial imaging allowing early detection of recurrence
The use of CO2 laser excision after radiation failure does not preclude its use for persistent or multiple recurrent disease
OUTCOMES
In 40% of cases more than one laser-assisted surgery was
required
Local control rate was 51-87% (Mean 65%)
Subsequent total laryngectomy was necessary in 25%
Overall control rate including those requiring total
laryngectomy was 80-100% (Mean 83%)
Complications
Complication rates are <5% and from most to least common include:
Granuloma formation
Laryngeal edema
Laryngeal stenosis
Chondronecrosis
PARTIAL LARYNGECTOMY
Aim
Is to perform oncological clearance of tumour with as much
preservation of normal voicing and swallowing as possible
Emphasis should be given to
Survival is more important than voice
Partial laryngectomies require experience and training
Patient must have good pulmonary reserve
More radical PL should be avoided in patients who have been
previously irradiated
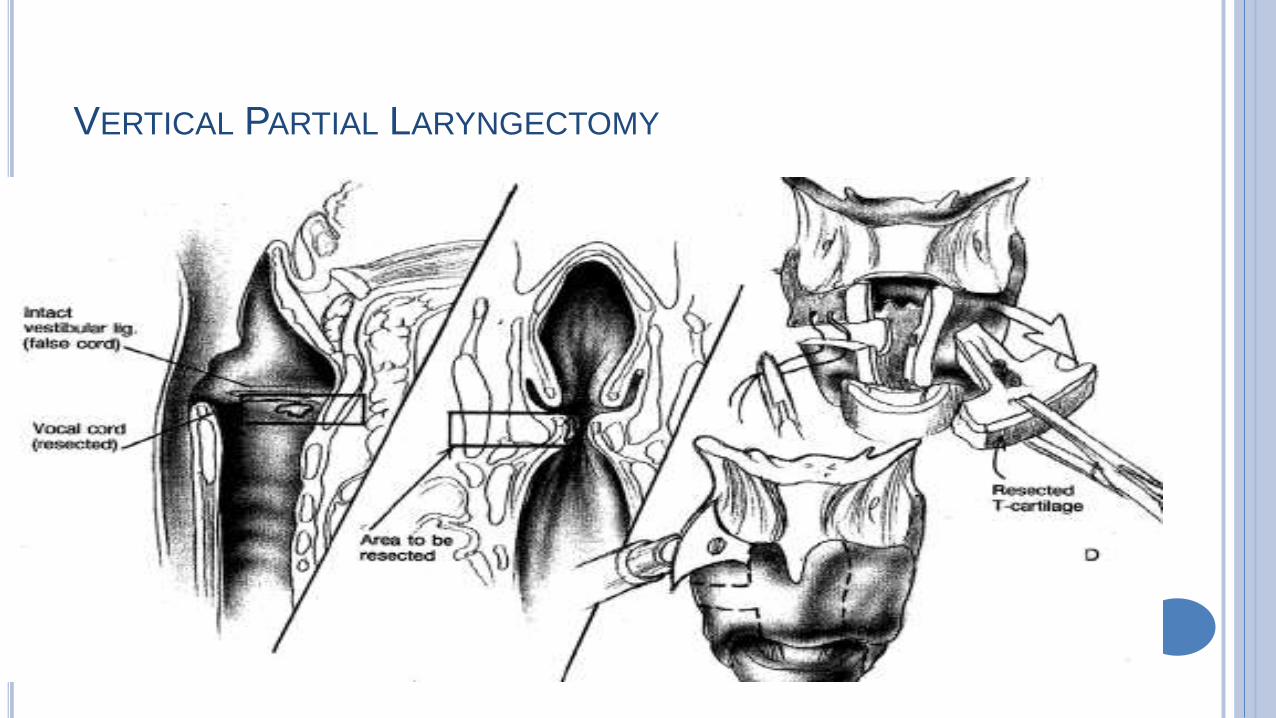
VERTICAL PARTIAL LARYNGECTOMY
Cordectomy- resection of the entire cord up to the vocal process of the
arytenoid, may be achieved by an open approach via a laryngofissure
Frontolateral laryngectomy- extends cordectomy to take in that part of the
thyroid cartilage into which the anterior commissure inserts
Anterior frontal laryngectomy- removes this region together with part of
both cords
Hemilaryngectomy-removes a vertical block of larynx to include one cord
(occasionally including arytenoid) and the anterior two-thirds of the ipsilateral thyroid
cartilage.
Removal of:
One vocal fold - from anterior commissure to vocal process
½ of opposite vocal fold may also be removed if involved
Ipsilateral false vocal cord
Ventricle
Paraglottic space (and overlying thyroid cartilage)
CONTRAINDICATIONS
Large T3 or any T4 lesion
Intrarytenoid or cricoarytenoid joint involvement
Bilateral arytenoid cartilage involvement or bilaterally diminished vocal cord mobility
Thyroid cartilage penetration
Supraglottic extension exceeding 10mm at the anterior commissure or 5mm at the vocal process of the arytenoid
Poor pulmonary function
OPERATIVE CONSIDERATIONS
The use of intraoperative frozen sections is imperative for maximal local control
All margins should be confirmed with permanent section postoperatively
In the event of failure of salvage VPL total laryngectomy remains an option and this will not ultimately affect local control. 8
The use of bipedicled flaps of strap muscles to replace excised intralarygeal soft tissue may facilitate post-op rehabilitation 13
Outcomes
Meta-analysis showed:
Local control rate 50-100% (mean 78%)
Approximately 15% of patients require completion laryngectomy for
second recurrence
Complications
Early - generally tracheostomy relatedInfection Aspiration and dysphonia
Late
AspirationChondritisLaryngeal stenosis (Must rule out local recurrence) Severe hoarseness Granulation tissueTumor recurrence
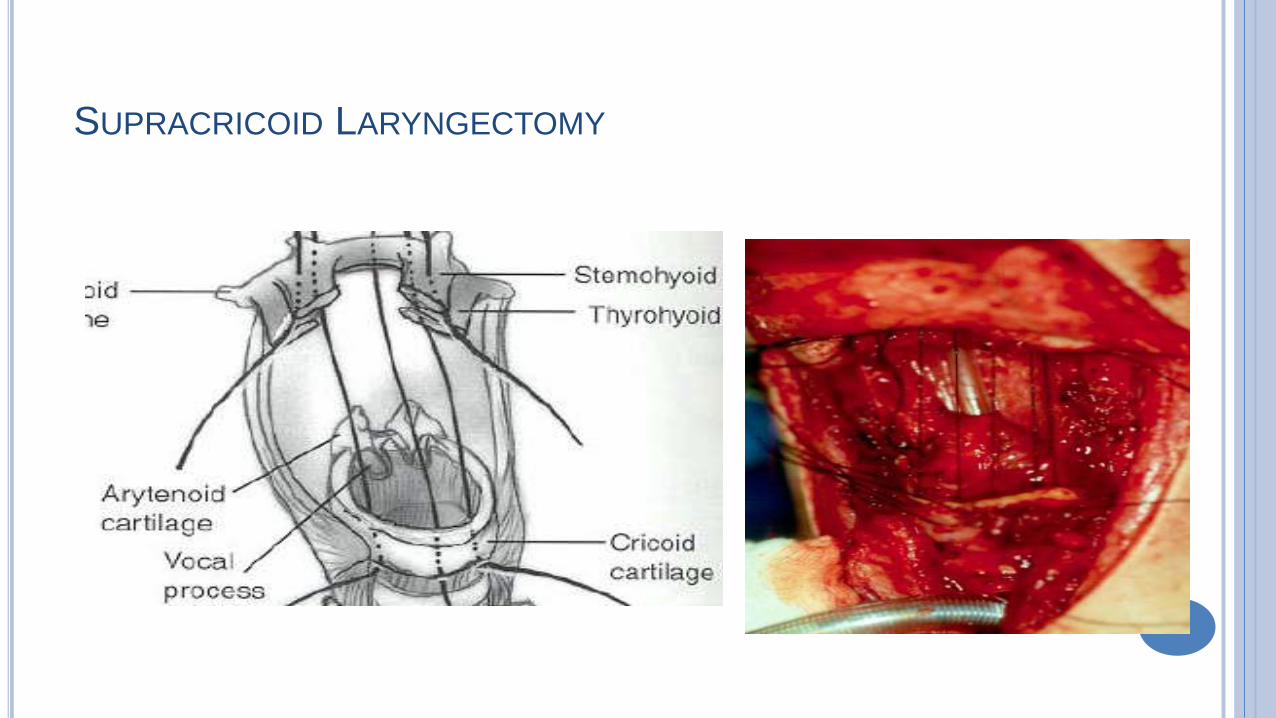
SUPRACRICOID LARYNGECTOMY
Removal of:Entire thyroid cartilageBilateral true and false vocal cordsVentriclesParaglottic and Preepiglottic spacesEpiglottisHyoid boneOne arytenoid (may spare both if not involved)
- At least one arytenoid must be spared to preserve phonation and sphincter functions
SUPRACRICOID LARYNGECTOMY
CONTRAINDICATIONS
Infiltration of both aryntenoid cartilages
Infiltration of cricoarytenoid joint or inter-arytenoid region
Subglottic extension >1cm below the vocal fold
Extension to the glossoepiglottic valecula
Major preepiglottic space invasion
Hyoid bone invasion
Invasion of outer perchondrium of thyroid cartilage
Extra-laryngeal spread
COMPLICATIONS
Swallowing disorders are the most common in the short term
Voice quality is hoarse, rough, breathy but with acceptable
intelligibility.
Aspiration Pneumonia is the most frequent complication (17.5%)
Neo-laryngeal edema
OUTCOMES
Disease-free survival 84.5%
Of the 15.5% failure of SCL, 66.7% successfully treated with Total
laryngectomy
3 year survival rate of 80 -100%
5 year survival rate of 69.4 -100%
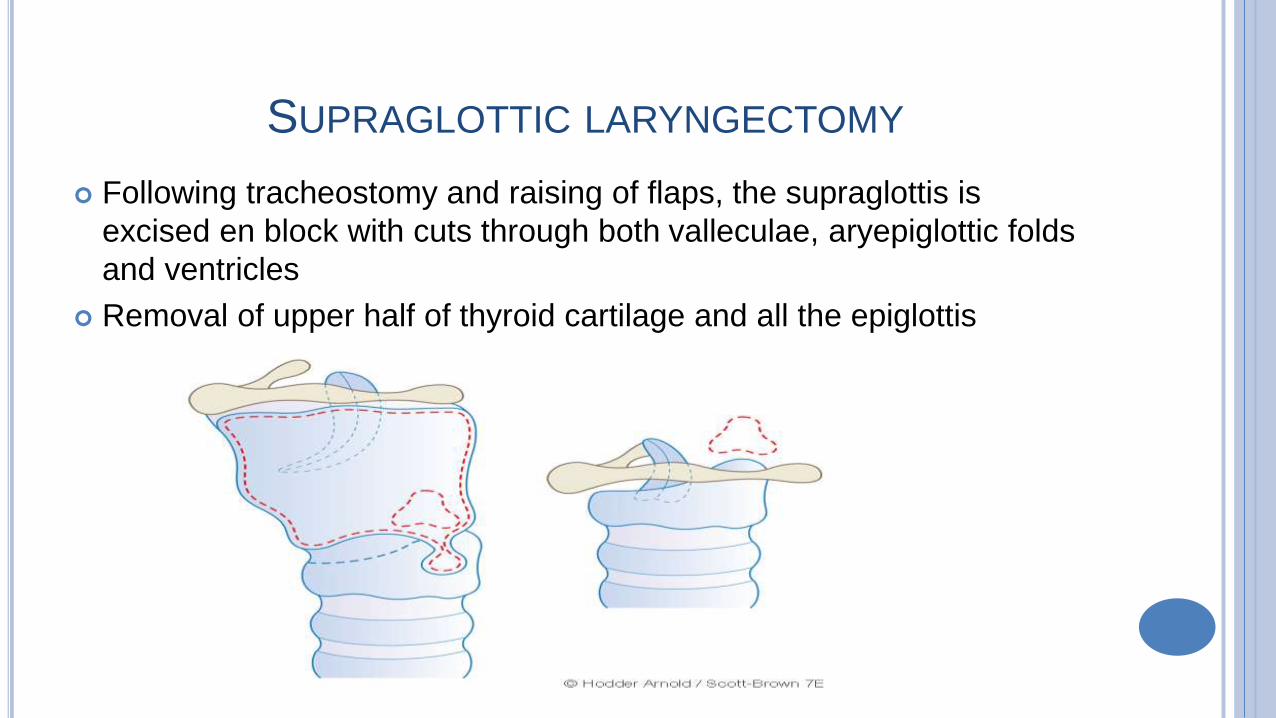
SUPRAGLOTTIC LARYNGECTOMY
Following tracheostomy and raising of flaps, the supraglottis is
excised en block with cuts through both valleculae, aryepiglottic folds
and ventricles
Removal of upper half of thyroid cartilage and all the epiglottis
SUBTOTAL LARYNGECTOMY
Operation popularised by Biller & Lawson
Three- quarter laryngectomy combining supraglottic laryngectomy with
vertical hemilaryngectomy on the side of the tumour
Indication
Supraglottic cancer which involve an arytenoid &/or vocal cord on one
side only
Tumour should be no longer than 2cm in maximum diameter
Should not extend in subglottis
NEAR- TOTAL LARYNGECTOMY
Described by Pearson
Technically complex procedure to create a physiological voice shunt
based on mobile arytenoid
No significant gains over total larygectomy
TOTAL LARYNGECTOMY
Mainstay of treatment for advanced laryngeal cancer
Fistly performed by Billroth in 1870
Curative as well as palliative.
The current 5 yr. survival rate of patients following total Laryngectomy
is about 80%
CHEMOTHERAPY
Palliative
Adjunctive
Chemoradiation
Surgery followed or preceded by
Chemoradiation
MANAGEMENT OF THE NECK
Main predictor of survival in squamous cell carcinoma is the presence,
number and extracapsular spread of lymph node metastases
N0
Elective neck dissection is commonly performed for management of
node negative T2-4 supraglottic cancer
Risk (Shah et a1.)--
Supraglottic -16-43%
Transglottic – 11-52%
Subglottic – 19-65%
Elective neck irradiation
N+ NECK IN LARYNGEAL CANCER
N1
modified neck dissection is procedure of choice
N2a or N2b
Choice of either MRND or RND followed by postoperative
radiotherapy or chemotherapy
N3
Whether or not to operate depends upon
staging of disease
presence or absence of fixation & what node is fixed to
experience of surgeon
need of patient
VOICE REHABILITATION FOLLOWING
LARYNGECTOMY
INTRODUCTION
TEP (Tracheo-oesophageal puncture) is considered gold standard
among various voice rehabilitation procedures
A good percentage of patients undergoing total Laryngectomy regain
esophageal voice
FUNCTIONAL ALTERATIONS FOLLOWING TOTAL
LARYNGECTOMY
Loss of speech.
Changes in normal swallowing mechanism
Changes in the pattern of respiration
Tracheostome problems;
Problems with loss of glottal occlusion, e.g. lifting;
Problems with airway diversion, e.g. loss of olfaction;
Body image/psychological/social problems.
REQUIREMENTS FOR NORMAL PHONATION
Active respiratory support
Adequate glottic closure
Normal mucosal covering of vocal cord
Adequate vocal cord length and tension control
Components of phonation
e
Lung (Bellows)
Larynx (Vibrator)
Articulators (Lips,
tongue, teeth)
METHODS OF SPEECH FOLLOWING LARYNGECTOMY
Esophageal speech
Electro larynx
TEP (Tracheo-oesophageal puncture)
ESOPHAGEAL SPEECH
All pts. Develop some degree of esophageal speech following
Laryngectomy
All alaryngeal speech modalities are compared with this modality
Till 1970’s this was the gold standard for all other post Laryngectomy
speech rehabilitation procedures
ESOPHAGEAL SPEECH - PHYSIOLOGY
Air is swallowed into cervical esophagus
This swallowed air is expelled out causing vibrations of pharyngeal
mucosa
These vibrations along with articulations of tongue cause speech to
occur
The exact vibrating portion of pharynx is the pharyngo-oesophageal
segment
The vibrating muscles and mucosa of cervical oesophagus and
hypopharynx cause speech
ESOPHAGEAL SPEECH – PE SEGMENT
This segment is made up of musculature and mucosa of lower
cervical area (C5-C7 segments).
Vibration of this segment causes speech in pts. Without larynx
Cricopharyngeal area is important
Cricopharyngeal spasm in these pts. Can lead to failure in developing
esophageal speech
Cricopharyngeal myotomy may help these pts. in developing
esophageal speech
PUMPING AIR INTO CERVICAL OESOPHAGUS
Injection method
Inhalational method
INJECTION METHOD
Enough positive pressure is built inside oral cavity to force air into
cervical oesophagus
Lip closure and tongue elevation against palate causes increase
intraoral pressure
Air is injected into the cervical oesophagus by voluntary swallowing
This method is also known as tongue pumping / glossopharyngeal
press / glossopharyngeal closure
INHALATIONAL METHOD
Uses the negative pressure used in normal breathing to allow air to
enter cervical oesophagus
Air pressure in the cervical oesophagus below Cricopharyngeal
sphincter is the same negative pressure as that of thoracic cavity
Pts. learn how to relax Cricopharyngeal sphincter during inspiration
allowing air to flow into cervical oesophagus as it enters the lungs
Pts. are encouraged to consume carbonated drinks which facilitates
air entry into cervical oesophagus helping in generation of esophageal
speech
ESOPHAGEAL SPEECH - ADVANTAGES
Patient’s hands are free
No additional surgery / prosthesis needed. Hence no extra cost for
the pt.
Pts. Get easily adapted to esophageal voice
ESOPHAGEAL SPEECH - DISADVANTAGES
Nearly 40% of pts fail to develop esophageal speech
Quality of voice generated is rather poor
Pt. may not be able to continuously speak using esophageal voice
without interruption. They will be able to speak only in short bursts
Significant training is necessary
Loudness / pitch control is difficult
Fundamental frequency of esophageal speech is 65 Hz which is lower
than that of male and female frequencies
CAUSES FOR FAILURE
Presence of cricopharyngeal spasm
Presence of reflux esophagitis
Abnormalities involving PE segment – like thinning of muscle wall in
that area
Denervation of muscle in the PE segment
Poorly motivated patient
ELECTROLARYNX
These are battery operated vibrating devices
It is held in the submandibular region
Muscle contraction and changes in facial muscle tension causes
rudiments of speech
Initial training to use this equipment should begin even before surgery
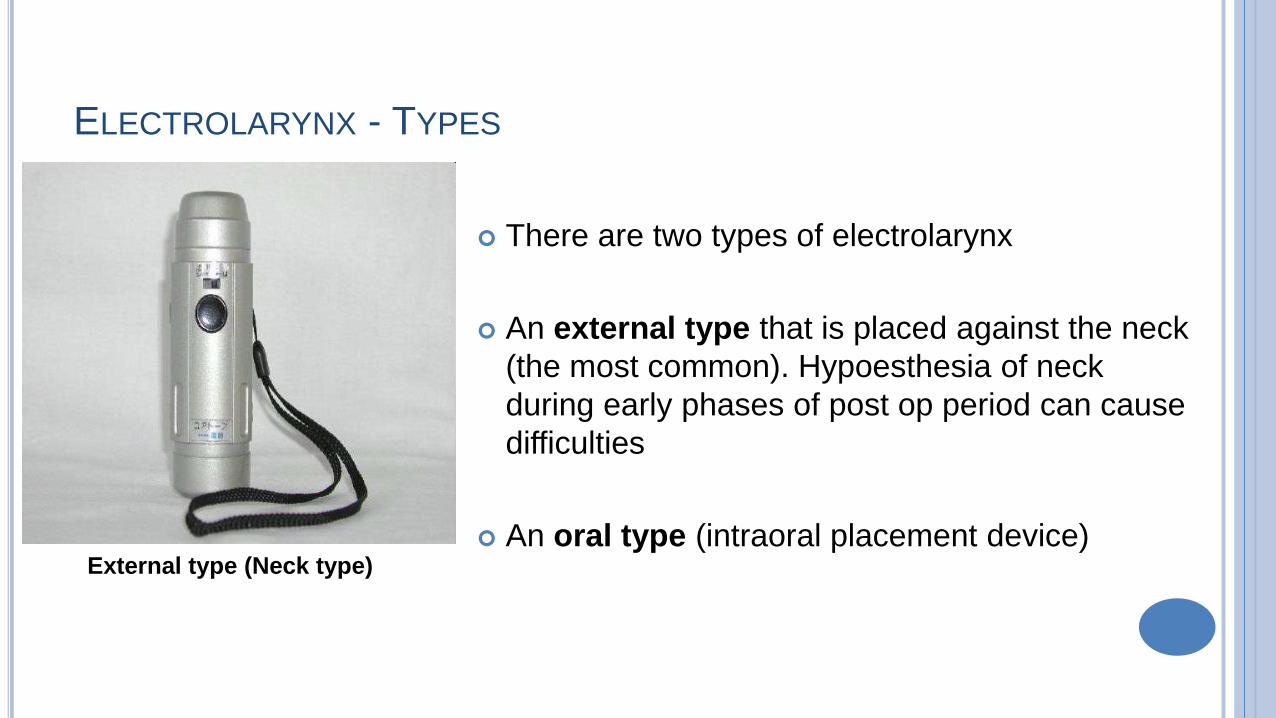
ELECTROLARYNX - TYPES
There are two types of electrolarynx
An external type that is placed against the neck
(the most common). Hypoesthesia of neck
during early phases of post op period can cause
difficulties
An oral type (intraoral placement device)External type (Neck type)
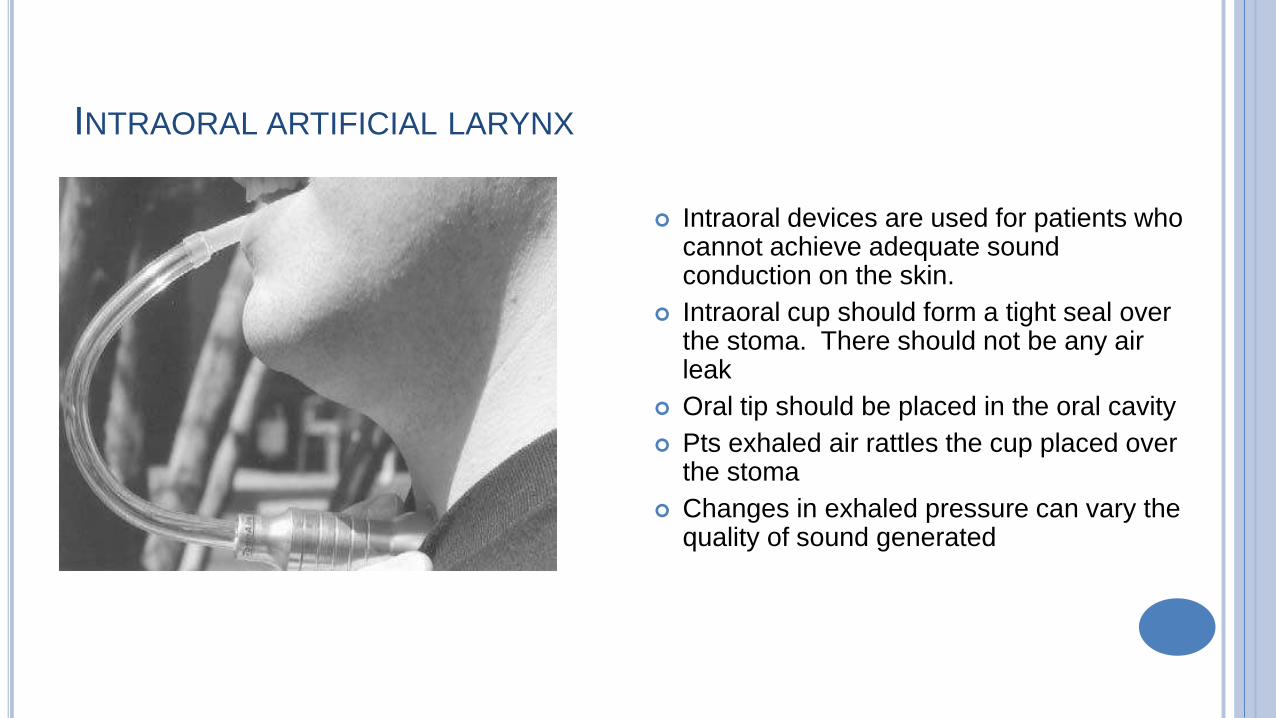
INTRAORAL ARTIFICIAL LARYNX
Intraoral devices are used for patients who cannot achieve adequate sound conduction on the skin.
Intraoral cup should form a tight seal over the stoma. There should not be any air leak
Oral tip should be placed in the oral cavity
Pts exhaled air rattles the cup placed over the stoma
Changes in exhaled pressure can vary the quality of sound generated
ELECTROLARYNX - ADVANTAGES
Can be easily learnt
Immediate communication is possible
Additional surgery is avoided
Can be used as a interim measure till the patient masters the
technique of esophageal speech or gets a TEP inserted
ELECTROLARYNX - DISADVANTAGES
The main disadvantages include the mechanical, monotonous and
robot-like sound quality.
Expensive to maintain
The necessity to use a hand to operate the controls and dependence
on batteries.
Difficult while speaking over telephone
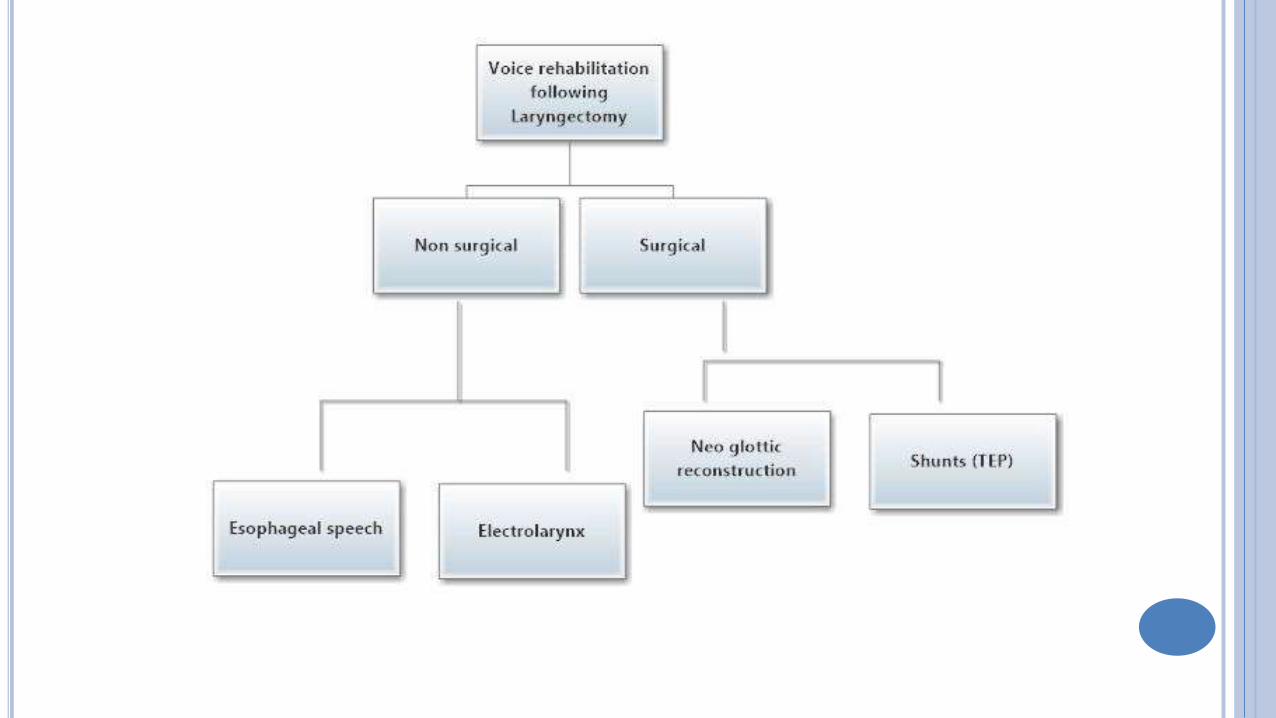
TYPES OF VOICE RESTORATION SURGERIES
Neoglottic reconstruction
Shunt technique
NEOGLOTTIC PROCEDURE
Trachea hyoidopexy
This can restore voice function in alaryngeal patients
Abandoned due to increased incidence of complications like
aspiration
SHUNT TECHNIQUE
Developed by Guttmann in 1930
Involves creation of shunt between trachea and esophagus
Lots of modifications of this procedure is available, Basic aim is to
divert air from trachea into the esophagus
TYPES OF SHUNTS
High trachea-esophageal shunt (Barton)
Low trachea-esophageal shunt (Stafferi)
TEP shunts (Guttmann)
CAUSES OF FAILURE OF SHUNT PROCEDURE
Aspiration through the fistula
Closure of the fistula
To avoid these problems prosthesis was introduced
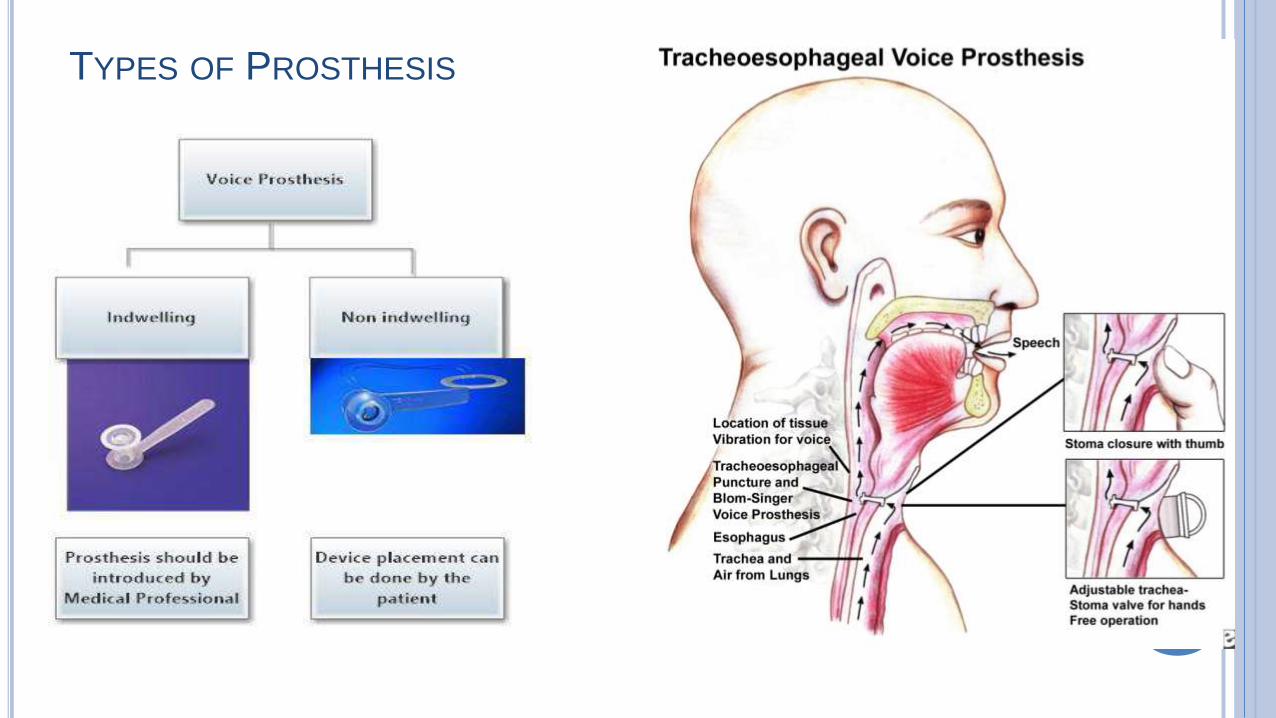
TYPES OF PROSTHESIS
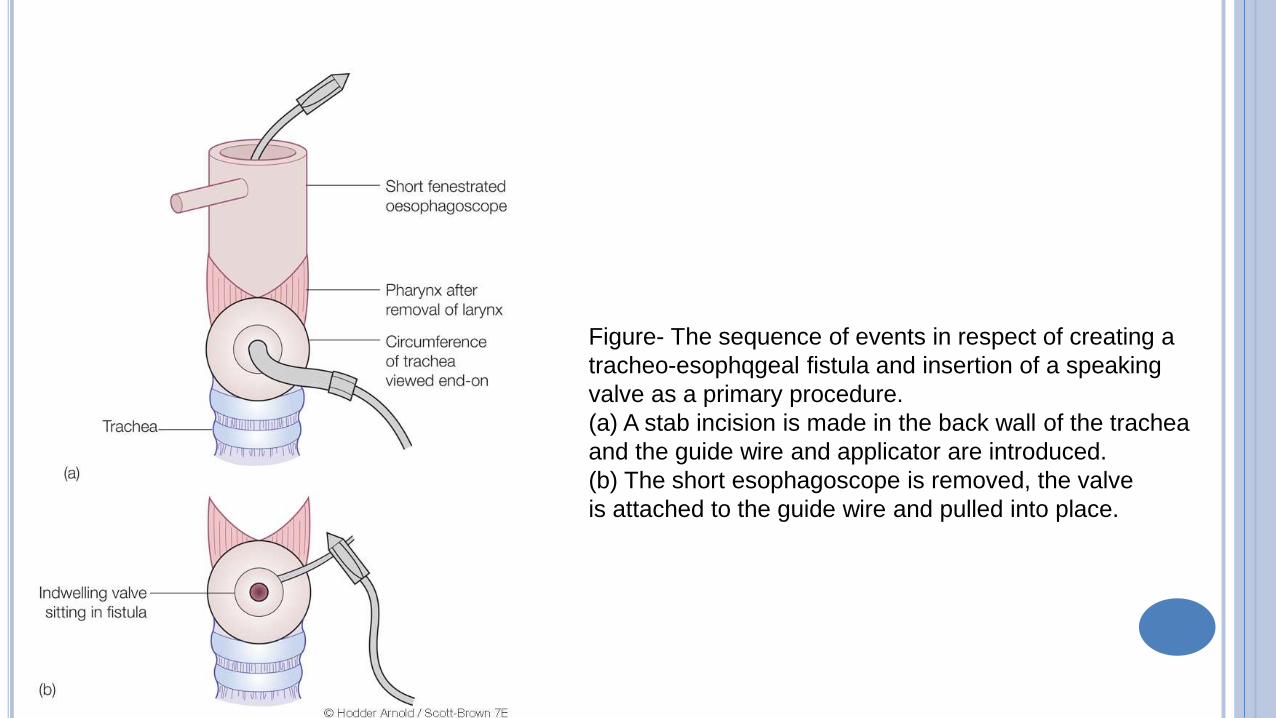
Figure- The sequence of events in respect of creating a
tracheo-esophqgeal fistula and insertion of a speaking
valve as a primary procedure.
(a) A stab incision is made in the back wall of the trachea
and the guide wire and applicator are introduced.
(b) The short esophagoscope is removed, the valve
is attached to the guide wire and pulled into place.
TEP
Was first introduced by Blom and Singer in 1979
One way silicone valve is introduced via the fistula
This valve served as one way conduit for air into esophagus while
preventing aspiration
This prosthesis has two flanges, one enters the esophagus while the
other rests in the trachea. It fits snugly into the trachea-esophageal
wound
Indwelling prosthesis have more rigid flanges when compared to that
of non indwelling ones
A medallion ring is attached to the non indwelling prosthesis to
prevent aspiration
TYPES OF TEP
Primary TEP – Performed during total laryngectomy
Secondary TEP – Performed 6 months after surgery
ANATOMICAL STRUCTURES TEP
TEP is performed in midline (Less bleeding)
Structures that are penetrated during TEP- membranous posterior
wall of trachea, esophagus and its 3 muscle layers and esophageal
mucosa
Interconnecting tissue in the trachea-esophageal space
ADVANTAGES OF TEP
Can be performed after laryngectomy / irradiation / chemotherapy /
neck dissection
Fistula can be used for esophago-gastric feeding during immediate
PO period
Easily reversible
Speech develops faster than esophageal speech
High success rate
Closely resembles laryngeal speech
Speech is intelligible
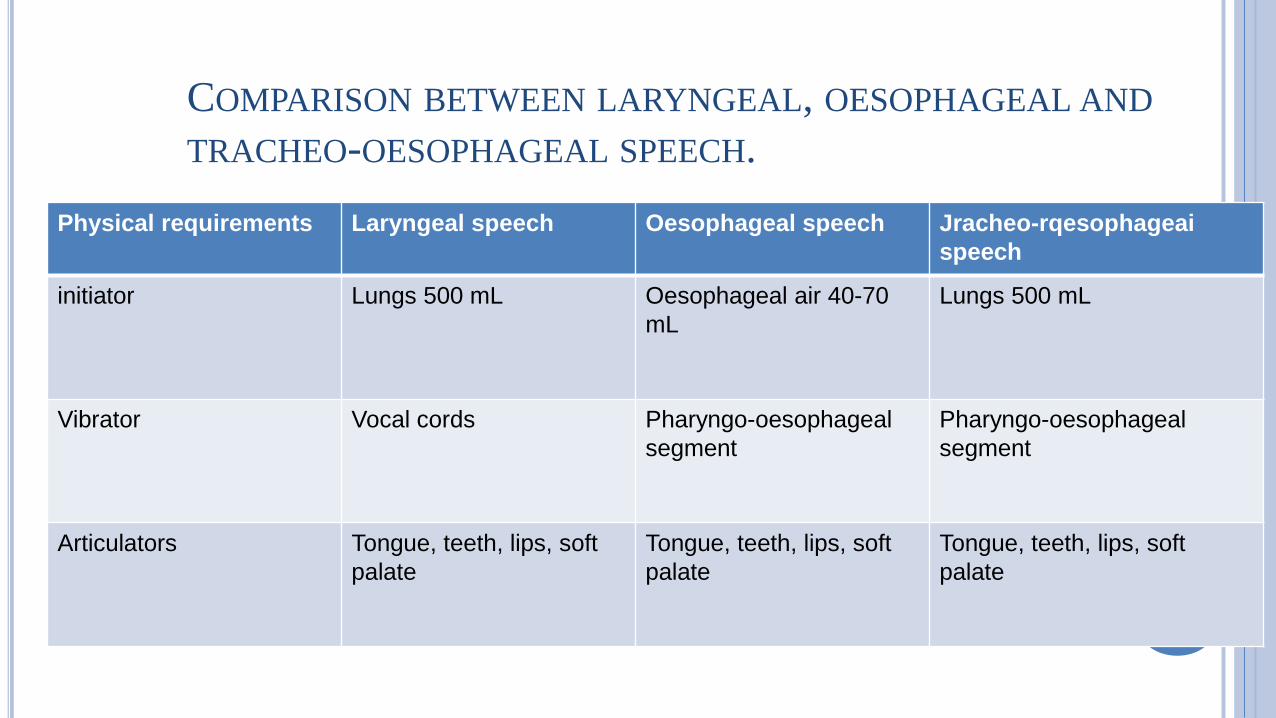
COMPARISON BETWEEN LARYNGEAL, OESOPHAGEAL AND
TRACHEO-OESOPHAGEAL SPEECH.
Physical requirements Laryngeal speech Oesophageal speech Jracheo-rqesophageai
speech
initiator Lungs 500 mL Oesophageal air 40-70
mL
Lungs 500 mL
Vibrator Vocal cords Pharyngo-oesophageal
segment
Pharyngo-oesophageal
segment
Articulators Tongue, teeth, lips, soft
palate
Tongue, teeth, lips, soft
palate
Tongue, teeth, lips, soft
palate
DISADVANTAGES OF TEP
Pt should manually cover the stoma during voicing
Good pulmonary reserve is a must
Additional surgical procedure is needed to introduce it
Posterior esophageal wall can be breached
Catheter can pass through the posterior wall
TEP – PATIENT SELECTION
Motivated patient
Patient with stable mind
Patient who has understood the anatomy & physiology of the process
Patient should not be an alcoholic
Good hand dexterity
Good visual acuity
Positive esophageal air insufflation test
Patient should not have pharyngeal stricture / stenosis
Stoma should be of adequate depth and diameter
Intact trachea-esophageal wall
CONTRAINDICATIONS OF TEP
Extensive surgery involving pharynx, larynx with separation of
trachea-esophageal wall
Inadequate psychological preparation
Patient with doubtful ability to cope up with prosthesis
Impaired hand dexterity
Suspected difficulty during PO irradiation
PRIMARY - TEP
Hamaker first performed in 1985
Primary TEP should be attempted where ever possible
In this procedure puncture is performed immediately after
laryngectomy and prosthesis is inserted
Primary tracheo-oesophageal puncture is now accepted as the
optimal method for voice rehabilitation.
Prosthesis of sufficient length should be used
ADVANTAGES OF PRIMARY TEP
Risk of separation of trachea – esophageal wall is minimized
Tracheo – esophageal wall is stabilized to some extent by the
prosthesis
Flanges of prosthesis protects trachea from aspiration
Stomal irritation is less
Patient becomes familiar with prosthesis immediately following
surgery
Post op irradiation is not a contraindication
PRIMARY TEP - PROCEDURE
Because of exposure following laryngectomy it is easy to perform
Ideally performed before pharyngeal closure
Puncture is performed through pharyngotomy defect
Ryles tube can be introduced via the fistula to provide gastric feeding
in the post op period
SECONDARY TEP
Usually performed 6 weeks following laryngectomy
This allows pt time to develop esophageal speech
Area of fistula is identified using rigid esophagoscope
Prosthesis can be inserted immediatly
MODIFIED SECONDARY TEP PROCEDURE
Performed under local anesthesia
Patient placed in recumbent position with mild extension of neck with
a shoulder roll
Tracheostomy tube is removed
12 0’ clock position of tracheostoma visualized and infiltrated using
2% xylocaine with 1 in 100,000 adrenaline
Yanker’s suction tube is inserted into the oral cavity till it hitches
against 12-0 clock position of tracheostome
This area is incised using 11 blade and widened using curved artery
forceps
Blom singer prosthesis is then introduced through this fistula
12 – 0 CLOCK POSITION OF TRACHEOSTOMA
YANKER’S SUCTION TUBE INSERTED
TEP - INCISION
TEP - WIDENED
PROSTHESIS INTRODUCED
PROSTHESIS USED IN TEP
Blom-Singer prosthesis
Panje button
Gronningen button
Provox prosthesis
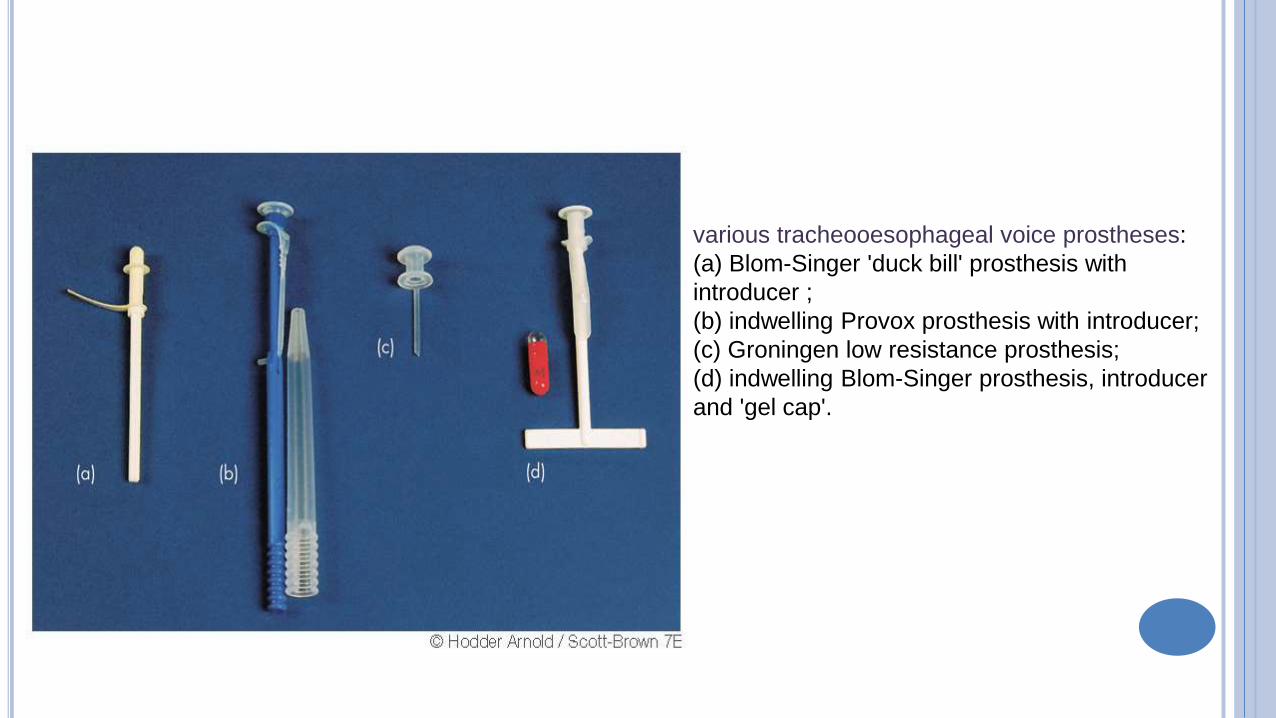
various tracheooesophageal voice prostheses:
(a) Blom-Singer 'duck bill' prosthesis with
introducer ;
(b) indwelling Provox prosthesis with introducer;
(c) Groningen low resistance prosthesis;
(d) indwelling Blom-Singer prosthesis, introducer
and 'gel cap'.
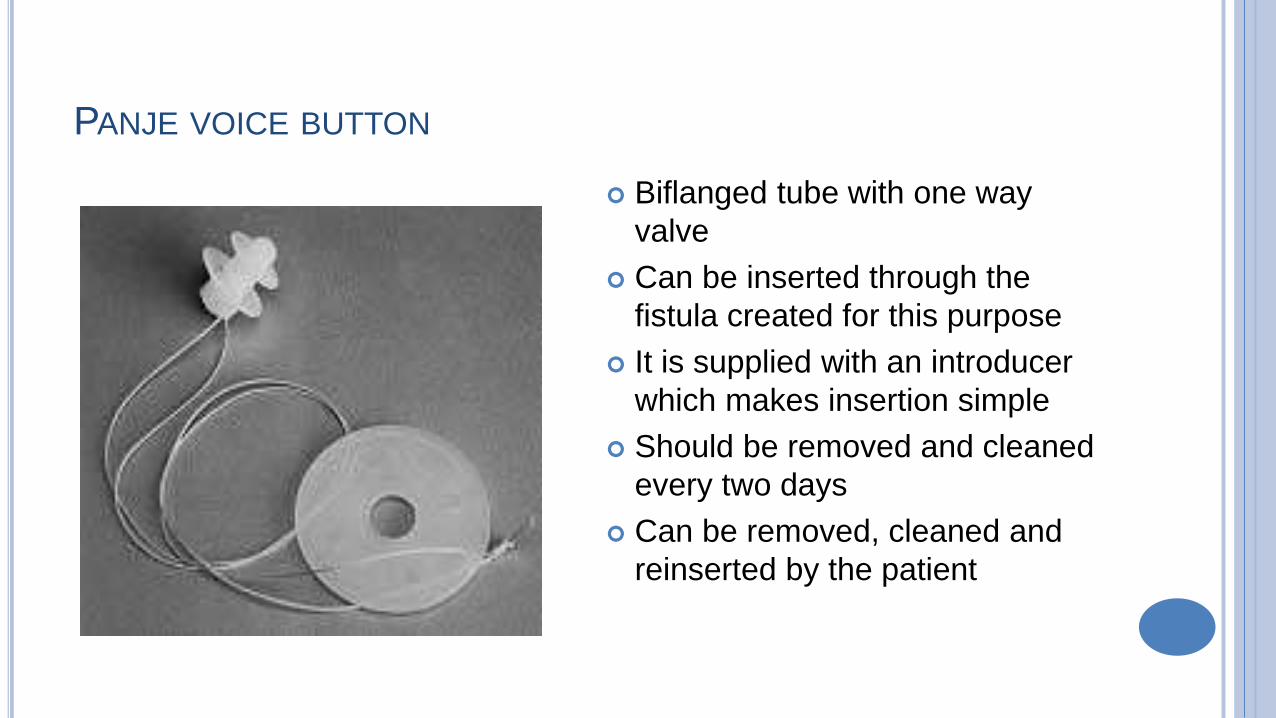
PANJE VOICE BUTTON
Biflanged tube with one way
valve
Can be inserted through the
fistula created for this purpose
It is supplied with an introducer
which makes insertion simple
Should be removed and cleaned
every two days
Can be removed, cleaned and
reinserted by the patient
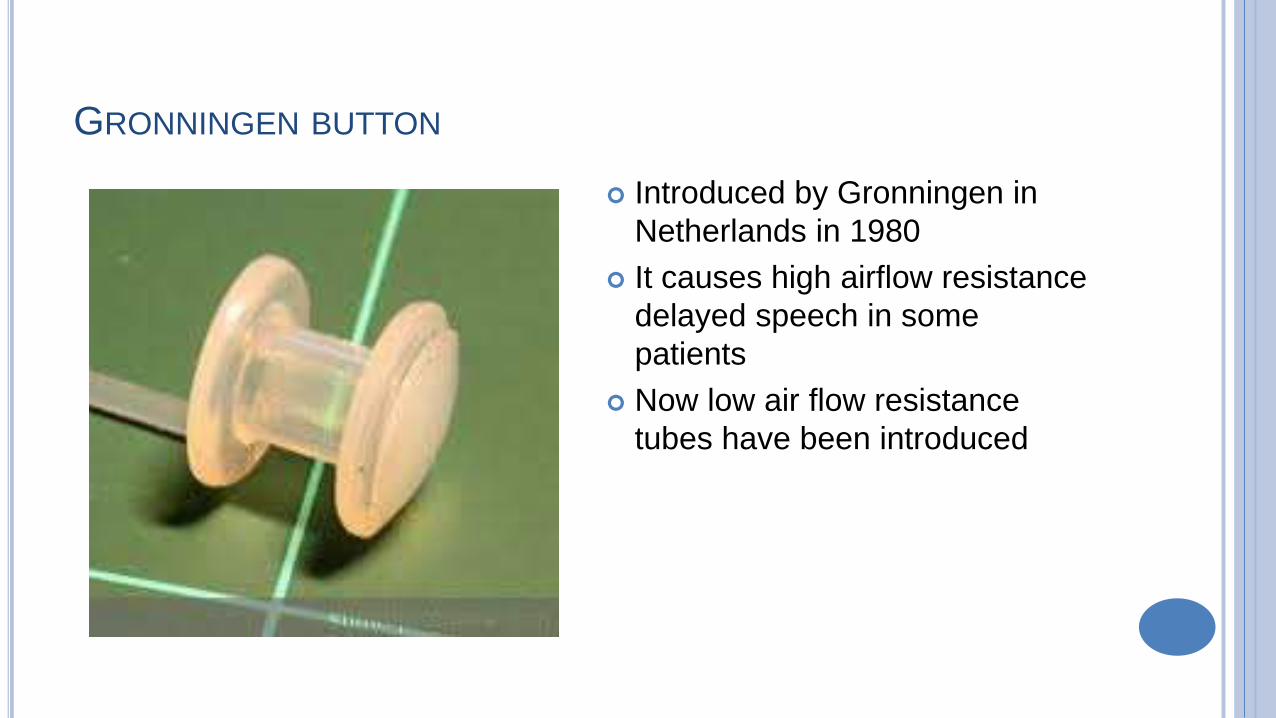
GRONNINGEN BUTTON
Introduced by Gronningen in
Netherlands in 1980
It causes high airflow resistance
delayed speech in some
patients
Now low air flow resistance
tubes have been introduced
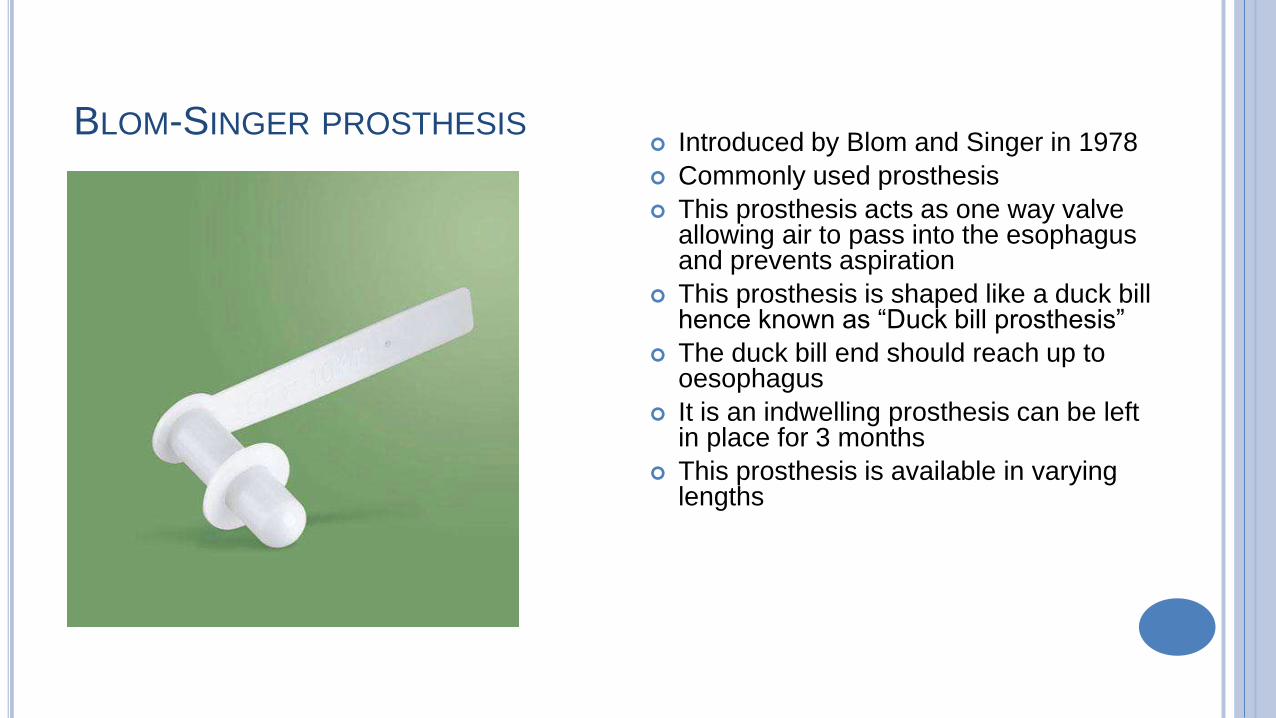
BLOM-SINGER PROSTHESIS Introduced by Blom and Singer in 1978
Commonly used prosthesis
This prosthesis acts as one way valve allowing air to pass into the esophagus and prevents aspiration
This prosthesis is shaped like a duck bill hence known as “Duck bill prosthesis”
The duck bill end should reach up to oesophagus
It is an indwelling prosthesis can be left in place for 3 months
This prosthesis is available in varying lengths
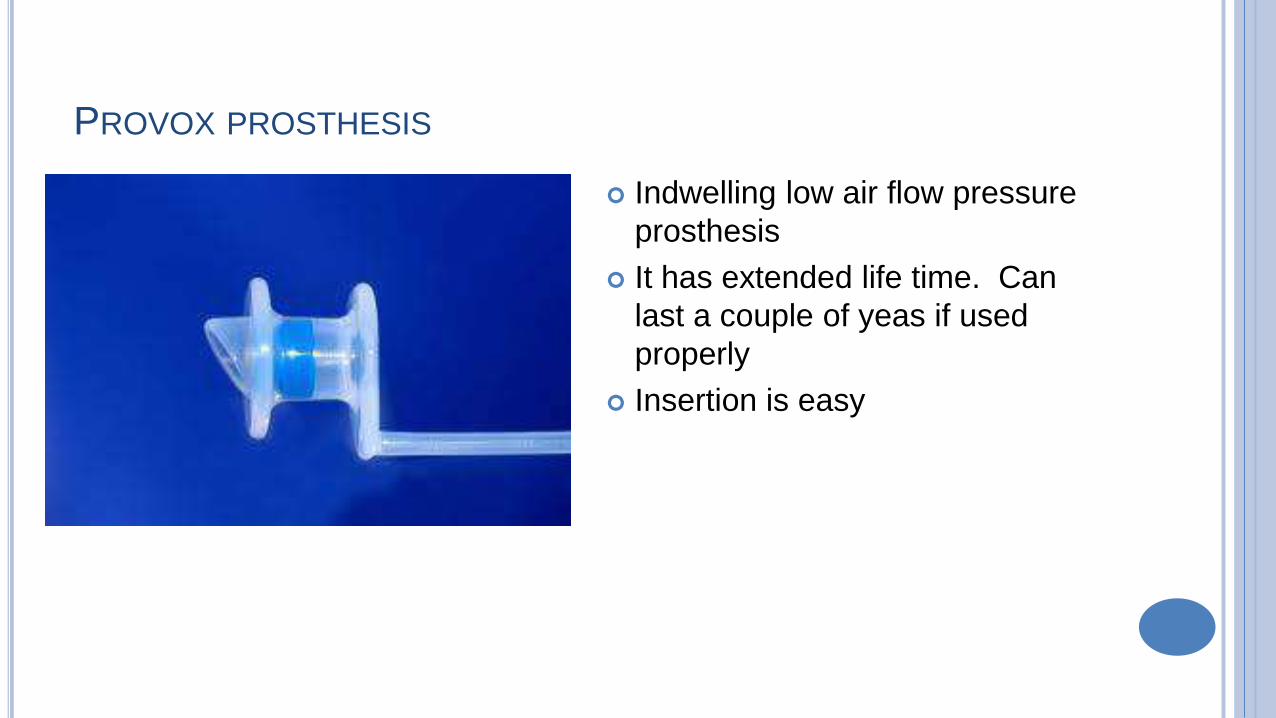
PROVOX PROSTHESIS
Indwelling low air flow pressure
prosthesis
It has extended life time. Can
last a couple of yeas if used
properly
Insertion is easy
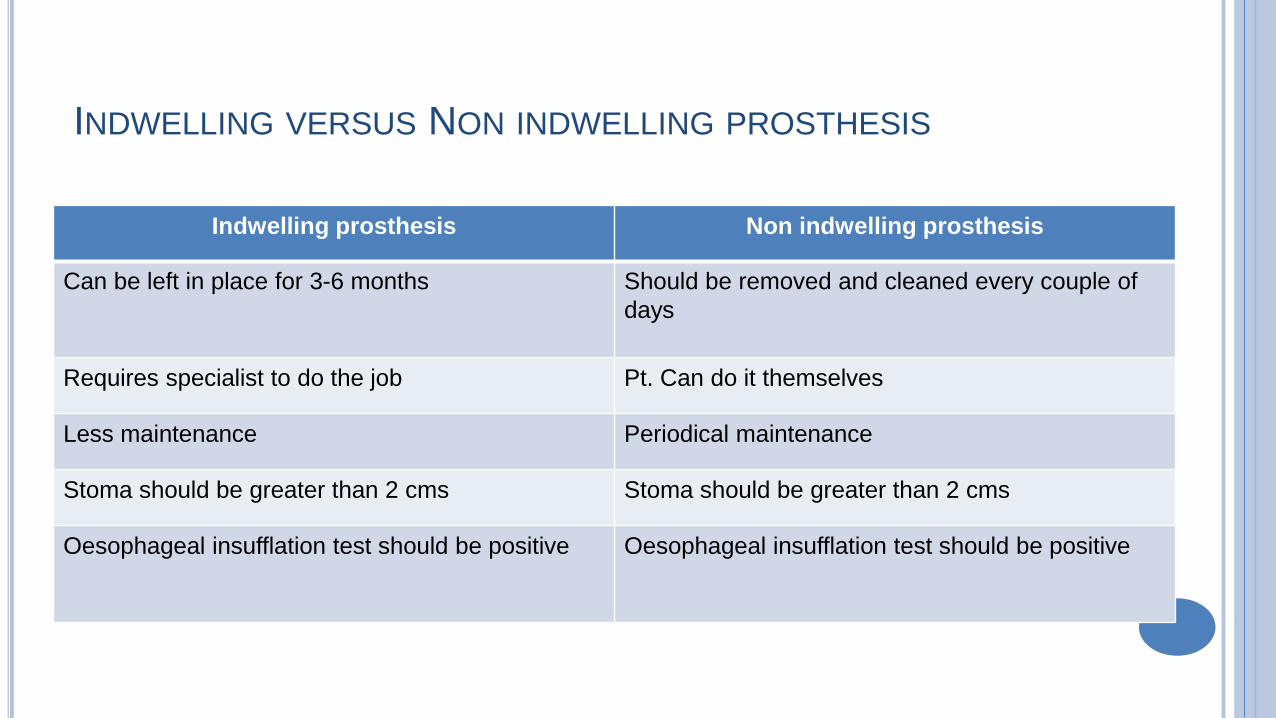
INDWELLING VERSUS NON INDWELLING PROSTHESIS
Indwelling prosthesis Non indwelling prosthesis
Can be left in place for 3-6 months Should be removed and cleaned every couple of
days
Requires specialist to do the job Pt. Can do it themselves
Less maintenance Periodical maintenance
Stoma should be greater than 2 cms Stoma should be greater than 2 cms
Oesophageal insufflation test should be positive Oesophageal insufflation test should be positive
PROBLEMS WITH TEP INSERTION
Leak through the prosthesis
Leak around the prosthesis
Immediate aphonia / dysphonia
Hypertonicity problems
Delayed speech
OESOPHAGEAL INSUFFLATION TEST
Should be performed before TEP
Assesses cricopharyngeal muscle response to esophageal distention
A catheter is placed through the nostril up to 25 cm mark. This
indicates probable site of puncture
Pt is asked to count numbers or vocalize “Ah”
INSUFFLATION TEST INTERPRETATION
Fluent voice on minimal effort – normal
Breathy voice indicating -hypotonic cricopharyngeal muscle
Hypertonic voice – “Cricopharyngeal spasm”
Spasmodic voice – “Extreme cricopharyngeal spasm”
COMMON PROBLEMS WITH TEP
Improper location of puncture
Inappropriate size of puncture
Presence of cricopharyngeal spasm
Leakage through and around the prosthesis
LOCATION OF TEP
12-0,’clock position of stoma
About 1-1.5 cms from trachea-cutaneous junction
If located superiorly pt may find it difficult to occlude
If located deep into the trachea then it becomes difficult to introduce
the prosthesis
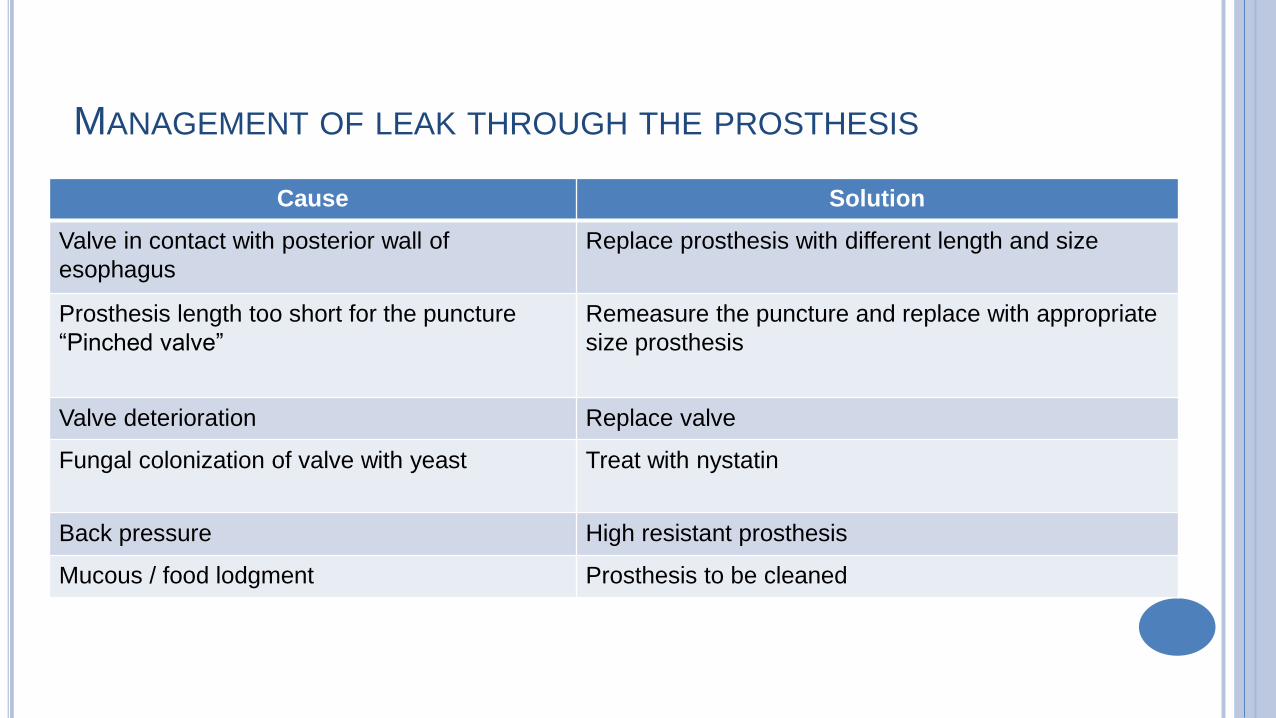
MANAGEMENT OF LEAK THROUGH THE PROSTHESIS
Cause Solution
Valve in contact with posterior wall of
esophagus
Replace prosthesis with different length and size
Prosthesis length too short for the puncture
“Pinched valve”
Remeasure the puncture and replace with appropriate
size prosthesis
Valve deterioration Replace valve
Fungal colonization of valve with yeast Treat with nystatin
Back pressure High resistant prosthesis
Mucous / food lodgment Prosthesis to be cleaned
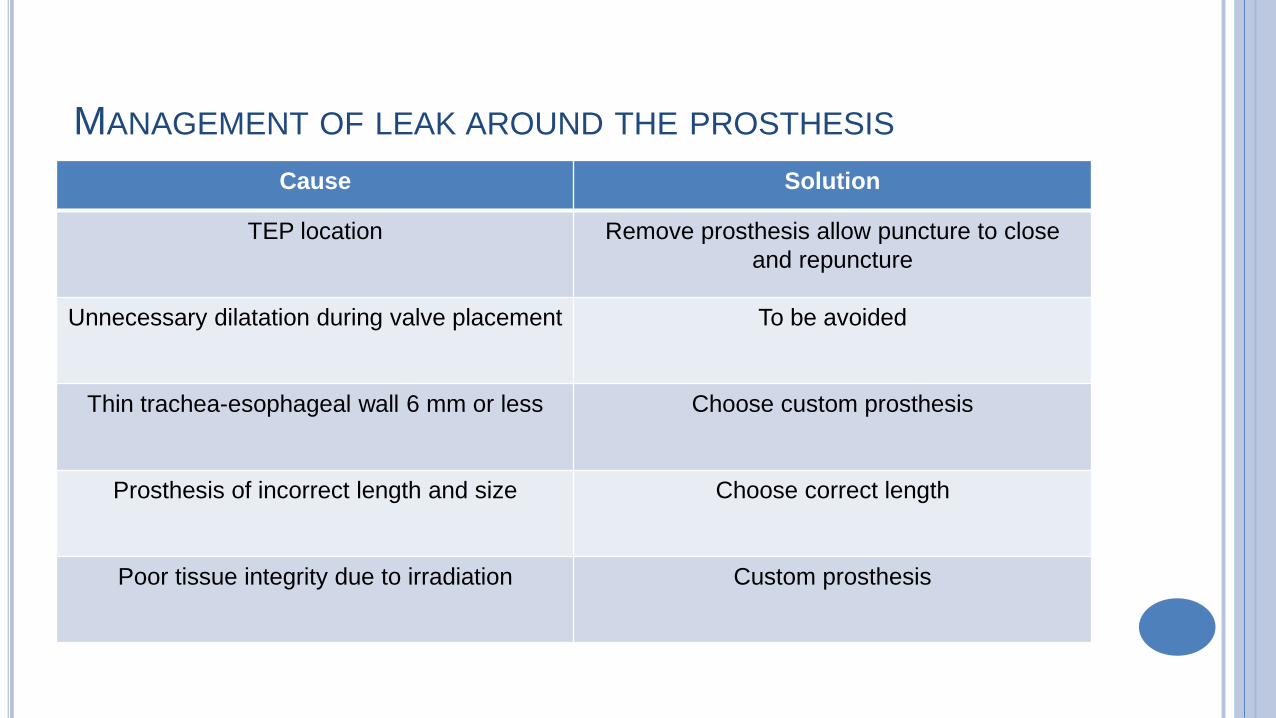
MANAGEMENT OF LEAK AROUND THE PROSTHESIS
Cause Solution
TEP location Remove prosthesis allow puncture to close
and repuncture
Unnecessary dilatation during valve placement To be avoided
Thin trachea-esophageal wall 6 mm or less Choose custom prosthesis
Prosthesis of incorrect length and size Choose correct length
Poor tissue integrity due to irradiation Custom prosthesis
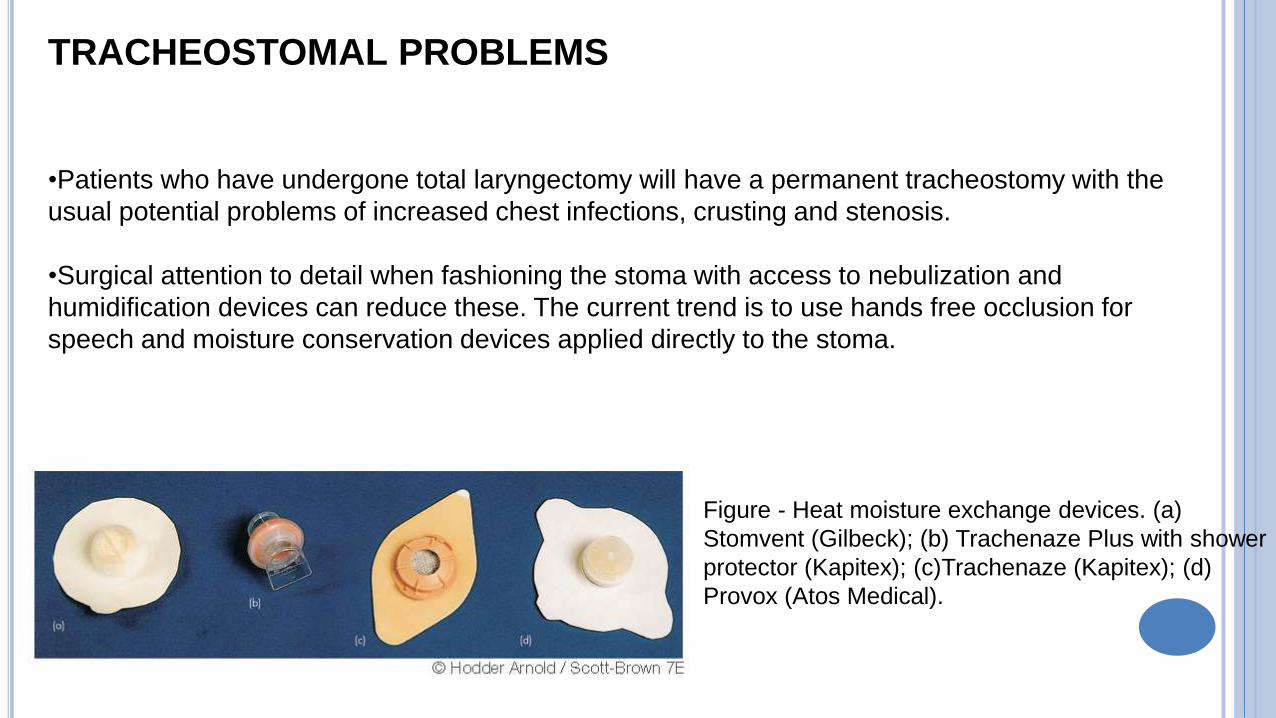
TRACHEOSTOMAL PROBLEMS
•Patients who have undergone total laryngectomy will have a permanent tracheostomy with the
usual potential problems of increased chest infections, crusting and stenosis.
•Surgical attention to detail when fashioning the stoma with access to nebulization and
humidification devices can reduce these. The current trend is to use hands free occlusion for
speech and moisture conservation devices applied directly to the stoma.
Figure - Heat moisture exchange devices. (a)
Stomvent (Gilbeck); (b) Trachenaze Plus with shower
protector (Kapitex); (c)Trachenaze (Kapitex); (d)
Provox (Atos Medical).
RECENT ADVANCES
In 1998 , Strome et al, performed the first true laryngeal transplant in
Cleveland, USA.
In 2010 UC Davis Medical Center, California performed another
successful laryngeal transplant.
Recently, Delaere et al. have developed a procedure using tracheal
autotransplantation, with vascularity provided by a radial forearm free-
flap. Thirty-six patients have been treated with reportedly excellent
results.