Embed Size (px)
Citation preview

CANCER PAIN AND THE
MANAGEMENT
SYAFRUDDIN GAUS
DEPARTMENT OF ANESTHESIOLOGY, INTENSIVE CARE AND PAIN MANAGEMENT
FACULTY OF MEDICINE, HASANUDDIN UNIVERSITY

CPD Perioperative IDSAI, Medan Juli 2010
OBJECTIVE
Magnitude of Cancer Pain
Etiology of Cancer Pain
Pathophysiologic of Cancer Pain
Clinical Characteristic of Cancer
Pain
Evaluation of Cancer Pain
Management of Cancer Pain

CPD Perioperative IDSAI, Medan Juli 2010
MAGNITUDE OF CANCER PAIN Bonica 1985
50 % of patient of all stage reported pain > 70 % with advanced cancer
Faley 1985 50 % of patient with non metastatic cancer had significant pain 60-90 % of patient with advanced cancer reported debilitating
pain WHO 1986
70 % of patient with advanced cancer has pain 3,5 million people suffering from cancer pain with or without
satisfactory treatment every day Paice, 2006
20-75% have pain at first diagnosis 23- 100% report pain in advance stage

CPD Perioperative IDSAI, Medan Juli 2010
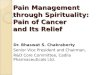
TOTAL
PAIN
SOMATIC SOURCE
ANXIETY
ANGERDEPRESSION
Non-cancer pathology
Cancer
Symptoms of debility
Side-effects of theraphy
Loss of social position
Loss of job prestige and income
Loss of role in family
Chronic fatigue and insomnia
Sense of helpessness
Disfigurement
Bureaucratic bungling
Friends who do not visit
Delay in diagnosis
Unavailable doctors
Irritability
Therapeutic failure
Fear of hospital or nursing homeWorry about familyFear of deathSpiritual unrest
Fear of pain
Family finances
Loss of dignity and bodily control
Uncertainty about future
WHO 1986

CPD Perioperative IDSAI, Medan Juli 2010
ETIOLOGY OF CANCER PAIN TUMOR-RELATED PAIN TREATMENT-RELATED PAIN DEBILITY-RELATED PAIN NON-MALIGNANT CONCURRENT
DISEASE

CPD Perioperative IDSAI, Medan Juli 2010
TREATMENT-RELATED PAIN Surgical procedures Chemotherapy
Immediate acute pain : iv infusion painPainful sequelae : arthralgia, headache,
mucositis Radiotherapy
Soft tissue injury : mucositis, proctitis, peripheral neurophaty, ets

CPD Perioperative IDSAI, Medan Juli 2010
PATHOPHYSIOLOGIC CLASSIFICATION OF CANCER PAIN NOCICEPTIVE PAIN
SOMATIC PAIN VISCERAL PAIN
NEUROPHATIC PAINNERVE COMPRESSIONDEAFFERENTATION NERVE INJURY SYMPATHETICALLY MEDIATED
PSYCHOGENIC PAIN

CPD Perioperative IDSAI, Medan Juli 2010
CLINICAL CHARACTERISTIC (1) 1. Nociceptive pain
Somatic pain : aching, stabbing, throbbing Well localized
Visceral pain : obstruction : gnawing, cramping Organ capsule : aching, sharp, throbbing Diffuse and difficult localize May referred to somatic structure

CPD Perioperative IDSAI, Medan Juli 2010
CLINICAL CHARACTERISTIC (2) 2. Neuropathic pain
Nerve compressions Burning, prickling, electric like Area innervated nerve Malignancy compression
Deafferentation nerve injury Same nerve compressions + shooting,stabbing allodynia Often loss afferent sensory function Superficial burning pain

CPD Perioperative IDSAI, Medan Juli 2010
CLINICAL CHARACTERISTIC (3)
Sympathetically mediated Cutaneous vasodilatation, increased skin
temperature, abnormal sweating, tropic cahanges and allodynia
Nondermatomal pattern pain Diagnostic sympathetic block
3. Psychogenic pain- after pathology pain generating excluded
- can contribute but pure psychogenic etiology is rare

CPD Perioperative IDSAI, Medan Juli 2010
SEVERITY-BASED CLASSIFICATION OF CANCER PAIN REFLECT
TUMOR SIZELOCATIONEXTENT TISSUE DESTRUCTIONMECHANISM OF PAIN
PAIN INTENSITY USED TO GUIDE ANALGESIC THERAPY

CPD Perioperative IDSAI, Medan Juli 2010
EVALUATION OF CANCER PAIN MEDICAL HISTORY PAIN HISTORY PAIN ASSESSMENT :
LOCATION CHARACTER SEVERITY ONSET DURATION TEMPORAL PATTERN RELIEVING AND EXACERBATION FACTOR ASSOCIATED SYMPTOMS PREVIOUS ANALGESIC THERAPY SPECIFIC CANCER TREATMENT

CPD Perioperative IDSAI, Medan Juli 2010
THE WHO CANCER PAIN STEP LADDER ORIGINALLY INTRODUCED IN 1986
SIMPLETHREE STEPWIDELY AVAILABLE AND INEXPENSIVE
ANALGESIC GLOBALLY DISTRIBUTED AND
CURRENTLY CONSIDERED AS STANDARD FOR MANAGEMENT CANCER PAIN

CPD Perioperative IDSAI, Medan Juli 2010

CPD Perioperative IDSAI, Medan Juli 2010
OPIOID Mainstay of cancer pain Multiple routes
EnteralParenteral ( iv, sc )Spinal deliveryTransdermalTransmucosal
Several formulation : sustained release eg. MS Contin, Kadian,
Avinza. Rapid release : not available in Indonesia

CPD Perioperative IDSAI, Medan Juli 2010
OPIOIDS COMPARATIVE
Opioid Half live Equipotent IV dose ( mg/kg)
Equipotent PO dose ( mg/kg )
Duration ( hr )
MorphineFentanyl
PethidineAlfentanylSufentanylCodeine Oxycodone
2-4 hrs1 – 7 min
3 – 4 hrs1.4 min1.4 min3 hrs2 – 6 hrs
0.10.001
10.050.00011.2N/A
0.3 – 0.50.001-0.005 transmucosal1.5 – 2N/AN/A20.1
3-50.75 – 1
2 – 30.514 - 6 4 – 6

CPD Perioperative IDSAI, Medan Juli 2010
MORPHINE Least lipid soluble Metabolites M6G and M3G ( longer half
lifes ) M6G more potent than morphine M3G ( no analgesic effect ) role in
tolerance Slow release ( controlled release or
sustained release ) use for chronic and cancer pain
Slow onset, prolonged duration fast titration its impossible

CPD Perioperative IDSAI, Medan Juli 2010
FENTANYL AND ITS ANALOGS Highly lipid soluble synthetic opioid Rapid onset and short duration Metabolite inactive (safe for renal
impairment) Suitable for transdermal administration

CPD Perioperative IDSAI, Medan Juli 2010
PETHIDINE Synthetized as a potential substitute for
atropine ( atropine like effect ) Weak affinity for NMDA receptor Pethidine superior in renal and biliary
colic but evidenced show that all opioids are equally effective
Metabolite is norphetidine ( normeperidine ) with long half-life ( 15-20 hrs ) analgesia ( µ receptors ) but neurotoxicity ( CNS excitation : anxiety, mood changes, tremors, twitching, myoclonic , convulsion )

CPD Perioperative IDSAI, Medan Juli 2010
NORPETHIDINE TOXICITY Treatment
Discontinue pethidine Substitue to alternative opioidSymptomatic treatment DO NOT administer naloxone
Suggest Dose limit : 1000 mg in first 24 hrs and 600-
700 mg/day thereafter, Reduced in elderlyShould be avoided in renal impairment

CPD Perioperative IDSAI, Medan Juli 2010
TRAMADOL Centrally acting synthetic analgesia µ receptors activity ( by main metabolite
M1 ( O-desmethyl-tramadol )) Inhibit reuptake NE and serotonine (5HT )
in nerve terminal Advantages of equianalgesic dose opioid
Less sedation Less repiratory depression Less constipation Nausea and vomiting similar Not a controlled drug

CPD Perioperative IDSAI, Medan Juli 2010
Epilepsy was relatively contra indication Seizure have been reported but
probably similar with other opioid Accumulation M1 in renal failure can
cause respiratory depression Total daily dose : 600 mg

CPD Perioperative IDSAI, Medan Juli 2010
CODEINE Naturally alkaloid like morphine Metabolized in liver by CYP 2D6
converted to morphine (2-10%) analgesic effect of Codeine
( ineffective prodrug of morphine ) Usually for mild to moderate pain Combine with non-opioid agents like
acetominophen or aspirin increased analgesic efficacy but also decreased opioid relate adverse effect

CPD Perioperative IDSAI, Medan Juli 2010
EQUIANALGESIC DOSES OPIOIDS
Oral dose ( mg )
Opioid Parenteral iv/sc/im( mg )
400 Meperidine 100
100 Tramadol 100
200 Codeine 130
30 Morphine 10
- Fentanyl 0.15 – 0.20
- Sufentanyl 0.02
Morphine 50 mg PO in 24 hrs = fentanyl patch 25 mcg/hr

CPD Perioperative IDSAI, Medan Juli 2010
PARACETAMOL Analgesic antipyretic Used in all steps in Stepladder WHO Recommend dose 4000 mg/d Dose adjustment in hepatic dysfunction

CPD Perioperative IDSAI, Medan Juli 2010
NSAIDS Analgesic, antipyretic and anti-
inflammatory Nonselective agents and selective COX-
2 inhibitors Effective component in multimodal
therapy Carefully selected patients due to
adverse effect COX-2 inhibitors proveide protection
adverse effect but concern in Cardiovascular effect

CPD Perioperative IDSAI, Medan Juli 2010
ADJUVANT ANALGESICS Antidepressant
Inhibition NE and serotonin reuptake For neurophatic pain Delays onset day to week Mood elevating and sleep enhancing effect Adverse effect on cardiac , glaucoma n prostatic Amitriptyline, Nortryptiline and Despiramine
Anticonvulsant For neurophatic pain eg. Chemotherapy Na channel blocker : Carbamazepine and
clonazepam Gabapentin : Ca Channel and can act as NMDA
antagonist . 900 – 3600 mg/d

CPD Perioperative IDSAI, Medan Juli 2010
ADJUVANT ANALGESIC Corticosteroids
Inhibit prostaglandin synthesis and reduce edema
For neuropathic pain syndromeBone pain , malignant intestinal obstructionDexamethasone 12 – 24 mg once daily
NMDA antagonistBind EAA glutamat For severe neuropathic painRoutine use limited due to cognitive
changes

CPD Perioperative IDSAI, Medan Juli 2010
ADJUVANT ANALGESIC Local anesthetic
Inhibiting ions across neural membrane Relieving neuropathic painOrally, topically, intravenously,
subcutaneously, spinallyFor Intractable neuropathic pain :
Lidocaine intravenous 1 – 2 mg/kg ( max 500 mg ) over 1 hour then 1 -2 mg/kg/h continuous infusion

CPD Perioperative IDSAI, Medan Juli 2010
OTHER TECHNIQUE FOR CANCER PAIN Nerve block Sympathetic nerve block Myofacial trigger point Neurolytic block : celiac plexus block Epidural or intratechal drugs

CPD Perioperative IDSAI, Medan Juli 2010
NONPHARMACOLOGIC THERAPIES Physical therapy
TENSAccupunctureCounterirritation
Psychological approachDepression and anxiety most oftenCognitive intervention : relaxation

CPD Perioperative IDSAI, Medan Juli 2010
Thank You